

Abstract
Objective
This study examined whether uncontrollable stressful life events were associated with sexual risk taking among adolescents across a 1-year period, and whether supportive friendships modified associations.
Design
Participants were 159 sexually active African American adolescents (57% male; mean age (SD) = 17.0 (1.5) years at baseline). Participants were recruited for in-person interviews through random digit dialing in one inner-city neighborhood characterized by high rates of poverty and crime relative to the surrounding city.
Main Outcome Measures
Dependent variables included substance use before sexual activity and inconsistent condom use.
Results
Among adolescents who reported low levels of supportive friendships, uncontrollable stressors were associated with greater levels of sexual risk taking over time. In contrast, uncontrollable stressors were not associated with sexual risk taking among adolescents who reported high social support from friends; risk taking was typically moderate to high among these adolescents.
Conclusion
Different processes may explain sexual risk taking among adolescents with varying levels of social support from friends. Adolescents with low support may be prone to engagement in health risk behavior as a stress response, while adolescents with high support may engage in risk behavior primarily due to peer socialization of risk.
Keywords: adolescence, African American, stressful life events, social support, sexual risk taking
The incidence of sexually transmitted infections among adolescents in the United States is increasing (Weinstock, Berman, & Cates, 2004), particularly among African Americans aged 15 to 24 years (CDC, 2006) and among youth of lower socioeconomic status (Ford et al., 2005; Newbern, Miller, Schoenbach, & Kaufman, 2004). Although African American youth aged 13 to 19 years represent only 17% of United States teenagers, they account for 69% of new HIV/AIDS cases (CDC, 2007). Rates of gonorrhea and syphilis are also disproportionately high among African American youth (CDC, 2006). African American inner-city communities, in particular, are characterized by relatively high rates of sexually transmitted infections (STD Control Section, 2007).
The primary purpose of the present study is to examine whether stressful life events are associated with greater levels of sexual risk taking among a community based sample of inner-city disadvantaged African American adolescents. We consider whether cumulative exposure to stressful life events is associated with inconsistent condom use and with sexual activity in the context of substance use. A secondary purpose of the study is to examine whether supportive friendships moderate the association between stressful life events and sexual risk taking in a manner that is consistent with the stress-buffering model of social relationships (Cohen, Gottlieb, & Underwood, 2001; Cohen & Wills, 1985) or a peer socialization of risk model (e.g., Gardener & Steinberg, 2005). Research suggests that social contexts involving peers are an important determinant of health risk behavior among adolescents (Dolcini & Adler, 1994; Gardner & Steinberg, 2005; Henrich et al., 2006). To our knowledge, the present study is the first to examine whether cumulative exposure to different life stressors is associated with sexual risk taking among adolescents, and whether supportive friendships modify these associations.
Sexual risk taking in the context of inner-city African American communities
Sexual risk taking among inner-city communities is thought to be related, in part, to living in an impoverished, unsafe environment that imposes high levels of stress and hopelessness (Bolland, 2003; Cohen et al., 2000; Ellen, Jennings, Meyers, Chung, & Taylor, 2004). Low socioeconomic status and African American ethnicity are independently associated with greater exposure to uncontrollable life stressors and perceived stress during adolescence (Brady & Matthews, 2002; Goodman, McEwen, Dolan, Schafer-Kalkhoff, & Adler, 2005). Youth living in disadvantaged neighborhoods have increased risk for exposure to community violence, criminal victimization, and discrimination based on ethnicity (Attar, Guerra, & Tolan, 1994; McLoyd, 1998; Simons, Murry, McLoyd, Lin, Cutrona, & Conger, 2002). Low income families are more likely than middle and upper income families to live in environments characterized by noise, crowding, substandard housing, and lack of routine in the home (Evans, Gonnella, Marcynyszyn, Gentile, & Salpekar, 2005). Income disparities and chaotic living conditions may increase parents’ stress and fatigue and undermine children’s ability to acquire skills for coping with stressors and managing behaviors (Evans et al., 2005; Gutman, McLoyd, & Tokoyawa, 2005). Stressful life events may increase the likelihood that adolescents make poor choices regarding behavior, especially if potentially risky behaviors provide a temporary escape from life stressors (Brady & Donenberg, 2006; Wills, Sandy, Yaeger, Cleary, & Shinar, 2001).
Links between stressful life circumstances and sexual risk taking
Research suggests that individuals may sometimes engage in sexual behavior to escape from stressors. Having sex as a means of coping with negative emotions was associated with greater increases in sexual risk behavior (e.g., sex in exchange for drugs or money) up to two years later in one study of adolescents and young adults (Cooper, Shapiro, & Powers, 1998). African American youth in this study were more likely than European American youth to report coping with negative emotions through sex, but stressful life events were not assessed. Some research has linked violence exposure to sexual risk taking (Berenson, Wiemann, & McCombs, 2001; Brady & Donenberg, 2006; Silverman, Raj, Mucci, & Hathaway, 2001; Voisin, 2005), but this research is cross-sectional and has not taken the approach of examining an array of stressors that may occur during adolescence. One study linked cumulative stressor exposure with greater likelihood of engaging in a composite of health risk behaviors including sex and substance use (He, Kramer, Houser, Chomitz, & Hacker, 2004), but this study did not examine sexual behavior separately or whether substance use and sexual behavior occurred in the same context.
Literature linking stressful life events with substance use is relevant to the present study because adolescents who engage in substance use are more likely to engage in sexual risk taking (Cooper, Peirce, & Huselid, 1994). Sexual behavior in the context of substance use, moreover, may increase the likelihood that adolescents engage in unprotected sexual intercourse (Hingson, Strunin, Berlin, & Heeren, 1990; Jemmott & Jemmott, 1993; Kingree, Braithwaite, & Woodring, 2000). The accumulation of different stressful life events (e.g., having a serious accident, parental divorce or unemployment) is associated with greater engagement in alcohol, cigarette, and marijuana use during adolescence (McCubbin, Needle, & Wilson, 1985; Wiesner & Juang, 2004; Zimmerman, Ramirez-Valles, Zapert, & Maton, 2000) and with increases in substance use over time (Wills, 1986; Wills, Sandy, Yaeger, Cleary, & Shinar, 2001; Windle, Mun, & Windle, 2005). It is unclear, however, whether cumulative exposure to stressful life events is associated with sexual behavior in the context of substance use.
How might supportive friendships modify associations between stressors and sexual risk taking?
For decades, researchers have observed that resources for support lessen the impact of stressful life circumstances on health outcomes (Cohen & Wills, 1985). The stress-buffering model of social relationships posits that social connections benefit health by providing psychological and material resources necessary to cope with stress, thereby decreasing the likelihood that individuals engage in health risk behavior as a means of coping (Cohen, 2004; Cohen, Gottlieb, & Underwood, 2001). Supportive friendships may lessen the impact of stress in different ways. For example, friends may reduce emotional distress or aid engagement in problem solving strategies. When applied to adolescent sexual risk taking, the stress-buffering model suggests that stress should be associated with greater sexual risk taking only among adolescents who have few resources for support; sexual risk taking should be relatively low among adolescents who have many resources for support, regardless of stress level.
The stress-buffering model of social relationships is based, in large part, on research among adult populations. Among adolescents, source of support may be a critical factor in determining whether support is associated with low levels of risk taking. Experimental research suggests that peers enhance adolescents’ risk taking tendencies (Gardener & Steinberg, 2005). This can be described as peer socialization of risk. Risk behavior may be pleasurable to adolescents and allow them to identify with and strengthen their ties with friends (Jessor, 1984; Sieving, Eisenberg, Pettingell, & Skay, 2006). Adolescents who are well connected with peers may also avail themselves of increased opportunities to engage in risk during unsupervised gatherings of friends. Supportive friendships may thus be associated with moderate or high levels of health risk behavior regardless of whether adolescents are experiencing stress.
Only a small body of research has examined associations between adolescent health risk behavior and supportive friendships, as opposed to focusing on other features of peer relationships (e.g., peer deviance). This literature is most consistent with the peer socialization of risk model. For example, emotional support from parents is associated with lower levels of substance use among adolescents, while emotional support from peers is associated with higher levels of substance use (Wills, Resko, Ainette, & Mendoza, 2004). McCubbin et al. (1985) found that close friendships were associated with greater alcohol use among a predominantly middle class European American sample of adolescents, independent of stressor exposure. Although studies suggest that peers engage in levels of sexual risk behavior that are similar to one another (e.g., Boyer, Tschann, & Shafer, 1999; Dolcini & Adler, 1994; Dolcini, Harper, Watson, Catania, & Ellen, 2005; Romer et al., 1994), almost no research has examined whether specific features of friendship influence sexual risk. In an exception, Henrich et al. (2006) tested for, but found no longitudinal association between supportive friendships and sexual risk behavior among a nationally representative sample of adolescents.
Two studies have examined whether supportive friendships alter associations between stressful life circumstances and health risk behavior during adolescence, and each study focused on substance use. Zimmerman et al. (2000) examined whether support moderated associations between stressful life events and alcohol and marijuana use among urban African American adolescents. They found no direct effect or interaction effect involving support. Windle (1992) found that supportive friendships and stressful life events were independently associated with greater alcohol problems among a predominantly European American sample of adolescents girls. Supportive friendships and stressful life events interacted to influence alcohol problems among boys, but the interaction was difficult to interpret.
Is sexual risk taking a stress response or part of a problem behavior syndrome?
An important conceptual issue in evaluating the association between stressful life events and risk behaviors is whether risk behaviors are a response to uncontrollable life stressors or whether they reflect an underlying tendency to engage in risk (Brady & Donenberg, 2006). The co-occurrence of different health risk behaviors among youth has been described as a problem behavior syndrome (Jessor, Donovan, & Costa, 1996). Adolescents’ experience of potentially controllable stressors (e.g., having bad grades at school, getting into trouble with the police) and engagement in sexual risk taking may reflect an underlying propensity to make poor choices. Research on the association between stressful life events and adolescent health risk behavior has generally not distinguished between those events that are uncontrollable and potentially controllable (for exceptions, see Wiesner & Juang, 2004; Wills, Yaeger, & Sandy, 2003). In addition, research has not included both types of events in the same model. The present study adjusts for adolescents’ experience of potentially controllable stressors and more directly tests the hypothesis that stressful life events increase risk for engagement in health-compromising behaviors, independent of any underlying propensity to make poor choices.
Hypotheses
Hypothesis 1
Greater accumulation of uncontrollable stressful life events will be associated with more frequent sexual activity in the context of substance use and with less frequent condom use, independent of potentially controllable life events.
Hypothesis 2
The accumulation of uncontrollable stressful life events will be associated with greater sexual risk taking only among adolescents with low levels of social support. Among adolescents with high levels of social support (intimacy with friends, instrumental aid from friends), we expect one of two possible outcomes based on theory and extant literature. If sexual risk taking is low among adolescents with high levels of social support, regardless of stress level, this outcome would be consistent with the stress-buffering model of social relationships. If sexual risk taking is high among adolescents with high levels of social support, regardless of stress level, this outcome would be consistent with the peer socialization of risk model.
Method
Recruitment and Procedure
Data from the present study are part of a larger longitudinal study examining social development and behavior among African American inner-city youth (Dolcini et al., 2005). The institutional review board (IRB) at the sponsoring institution approved all study procedures. Initial participants were recruited through random digit dialing from a specific zip code defining an inner-city neighborhood in a West Coast city to obtain a representative sample of African American adolescents aged 14 to 18. African American adolescents in this neighborhood have the highest rates of sexually transmitted infections in the surrounding city (DiClemente et al., 1996; STD Control Section, 2007).
In the initial screening, 70% of all contacted households agreed to cooperate. Participants over age 18 and parents, for those under 18, provided informed consent, and all youth under 18 assented. Of the 119 individuals recruited from the initial probability sample, 91 (76%) completed an initial interview by a gender-matched interviewer in our field office. These friendship-network “seeds” identified 333 close friends, 111 of whom were also recruited for the study. Friends qualified for participation if they were aged 14 to 21 years and from the same neighborhood as seeds or a neighborhood in close proximity. Friends of any ethnicity could participate, but most were African American. The 91 seeds and 111 friends completed a baseline interview and were invited to participate in a 1-year follow-up. Retention rate at the 1-year follow-up was 81% (163/202). Youth were reimbursed for participation.
Sample Characteristics
One hundred fifty-nine adolescents reported being sexually active at one or both of the two data collection time points. At baseline, 128 adolescents reported being sexually active during the past year (63% of 202 adolescents). At the 1-year follow up, 116 reported being sexually active during the past year (71% of 163 adolescents). Eighty-five of these adolescents were sexually active at both the baseline and follow-up assessments, while 31 became sexually active between the baseline and follow-up assessments.
Of the 159 participants who were sexually active at baseline and/or follow-up, 57% were male. Age ranged from 14 to 21 years at baseline, with a mean age of 17.0 (SD=1.5); all but 9 adolescents were between 15 and 19 years old. Eighty-eight percent of adolescents described themselves as African American, 8% were of mixed ethnicity with African American heritage, and 4% were of Asian, Latino, or European-American ethnicity.
Measures
We examined report of stressful life events and supportive friendships at baseline. Report of sexual risk taking at both baseline and follow-up assessments was examined.
Stressful life events
A 25-item measure, based on Wills and colleagues’ Negative Life Events Inventory (Wills, Vaccaro, & McNamara, 1992), assessed exposure to stress during the past year. The Negative Life Events Inventory was specifically developed for adolescents. For the present study, the lead author and two postdoctoral fellows independently rated items. Raters unanimously agreed that 11 life events were negative and beyond adolescents’ control; these items were classified as uncontrollable. One or more raters thought that 10 negative life events were potentially under adolescents’ control; these items were classified as potentially controllable (see Table 1). Four items were omitted from this study because they were not judged to be clearly negative (e.g., A new person joined your household). Life events composites were formed by tallying the number of reported events within each category. Because the inventory is an event-based measure, we did not conduct tests of internal consistency. One respondent failed to complete the measure and was excluded from analyses.
Table 1.
Percentage of adolescents reporting each negative life event during the past year at baseline.
| Uncontrollable Life Events | Potentially Controllable Life Events | ||
|---|---|---|---|
| 1. Someone in the family was arrested. | 39.2% | 1. You and your boyfriend or girlfriend broke up. | 54.1% |
| 2. Someone in the family had a serious illness. | 35.4% | 2. You got bad grades in school. | 44.6% |
| 3. Someone in the family was incarcerated or put in jail or prison | 32.3% | 3. You argued a lot with your parents. | 43.0% |
| 4. Your parents had problems with money. | 29.1% | 4. Some people stopped paying attention to you. | 39.5% |
| 5. Your parents argued a lot. | 23.9% | 5. You got disciplined from school. | 21.2% |
| 6. Someone in the family had a serious accident. | 21.7% | 6. You got into trouble with the police. | 19.6% |
| 7. Someone in the family was robbed, attacked, or shot. | 20.4% | 7. You were not accepted into a group or team in which you wanted to be a member. | 16.5% |
| 8. Someone in the family experienced damage or loss of property. | 15.8% | 8. You had trouble with your physical appearance. | 16.5% |
| 9. Someone in the family had a mental health (psychological) problem. | 15.2% | 9. You had a serious accident. | 11.4% |
| 10. Your parents separated or divorced. | 14.1% | 10. You had a serious illness. | 9.5% |
| 11. Your father or mother lost a job. | 14.0% | ||
Supportive friendships
Adolescents completed the Intimacy and Instrumental Aid subscales of the Network of Relationships Inventory (Furman & Buhrmester, 1985). We modified response categories to better fit the population. Adolescents were asked to rate items on a 5-point Likert scale ranging from 1 (not at all) to 5 (all the time). This measure does not specify a time frame for receipt of social support. We averaged the 3 items assessing intimacy with friends (I tell my close friends everything, I share my secrets and private feelings with my close friends, I talk to my close friends about things I do not want others to know) and 3 items assessing instrumental aid from friends (my close friends… teach me how to do things I do not know, help me to figure out or fix things, help me when I need to get something done). Alphas for the intimacy (α=.87) and instrumental aid (α=.63) scales were acceptable. Eight participants failed to complete the supportive friendships measure and were excluded from analyses involving these variables.
Sexual risk taking
At baseline and 1-year follow-up assessments, sexual risk taking composite variables were formed for inconsistent condom use, alcohol use before having sex, and marijuana use before having sex. Composite variables were weighted by frequency of sexual activity with each of adolescents’ three most recent partners.
Frequency of sexual activity
Adolescents estimated the number of times they had sex with each of their three most recent partners during the past year. Scores ranging from 1 to 4 were assigned for each partner based on reported frequency of sexual contact: 1-10, 11-25, 26-50, or 51+ occasions of sexual activity.
Inconsistent condom use
Participants were asked how frequently they used condoms when engaging in vaginal intercourse with each partner during the past year, using a 5-point scale: 5 (never), 4 (less than half of the time), 3 (about half of the time), 2 (more than half of the time), 1 (always). Scores for frequency of sexual contact with a specific partner (1 through 4) were multiplied by scores reflecting inconsistent condom use with that partner (1 through 5), and the resulting products were summed across partners. The resulting composite variable reflected risk for sexually transmitted infections due to inconsistent condom use. Adolescents received higher scores if they rarely used condoms, had sexual intercourse frequently, and had a greater number of partners.
Substance use prior to sexual activity
Participants were asked to rate the frequency with which they engaged in alcohol or marijuana use prior to sexual activity with each partner during the past year. They used the following 5-point scale: 1 (never), 2 (less than half of the time), 3 (about half of the time), 4 (more than half of the time), 5 (always). Frequency of substance use with a specific partner was multiplied by frequency of sexual contact with that partner, and resulting products were summed across partners. This resulted in two sexual risk taking variables at each time point: frequency of alcohol use before sex and frequency of marijuana use before sex.
Plan of Analyses
Preliminary analyses examine the distributions of and correlations between study variables, adjusting for age and gender. Mixed model linear regression analyses are used to test study hypotheses. Each model regresses an individual sexual risk taking variable (inconsistent condom use, alcohol use before sex, marijuana use before sex) on the following variables entered sequentially: (1) age and gender, (2) uncontrollable life events, (3) potentially controllable life events. Separate models test cross-sectional and longitudinal associations, resulting in six separate tests. These analyses test whether uncontrollable life events reported at baseline are associated with greater levels of sexual risk taking in both cross-sectional and longitudinal analyses. In a separate set of longitudinal analyses, baseline level of risk taking is entered on a fourth step. Adjustment for baseline level of sexual risk taking limits analyses to those 85 adolescents who were sexually active at both the baseline and 1-year follow-up assessments. This set of longitudinal analyses tests whether uncontrollable life events reported at baseline are associated with greater changes in sexual risk taking among sexually active youth during the year under study, and thus, takes into account the repeated measures design.
For the second part of the study—an examination of whether supportive friendships moderate associations between stressful life events and sexual risk taking—we perform additional analyses to include an interaction term between uncontrollable life events and one of two potential moderators (instrumental aid from friends, intimacy with friends). We present significant interaction effects in two ways. First, we show the effect of uncontrollable life events on sexual risk taking within groups of adolescents who report low or high levels of the moderator (simple effects tests within two groups determined by median split, shown in tables). Second, we present a figure depicting illustrative interactions by entering values one standard deviation above and below the mean values for uncontrollable life events and the moderator, consistent with the recommendation of Aiken and West (1991).
Mixed model linear regression analyses are performed in SPSS. Consistent with the recommendation of McCulloch and Searle (2001), we use restricted maximum likelihood estimation. Intercepts in regression models are allowed to vary randomly by friendship network (i.e., an identifier indicating the network to which a seed or friend belonged). In other words, the regression analyses account for the influence of friendship network membership on sexual risk behavior through the modeling of within-group correlation structures. All other variables are examined as fixed effects.
Results
Distribution of items used to create sexual risk taking composites
At baseline, 128 adolescents reported having one partner, 72 reported a second partner, and 43 reported a third partner during the past year. For partners 1, 2, and 3, 46%, 68%, and 57% of adolescents, respectively, reported having sex between 1 and 10 times. At the 1-year follow-up assessment, 116 adolescents reported having one partner, 67 reported a second partner, and 39 reported a third partner during the past year. For partners 1, 2, and 3, 40%, 54%, and 68% of adolescents, respectively, reported having sex between 1 and 10 times.
For partners 1, 2, and 3 at baseline, 60%, 79%, and 76% of adolescents, respectively, reported always using condoms. For partners 1, 2, and 3 at the 1-year follow-up assessment, 53%, 70%, and 81% of adolescents, respectively, reported always using condoms. At both the baseline and 1-year follow-up assessments, 60% or more of adolescents reported never using alcohol before sex and 50% or more reported never using marijuana before sex, when percentages were examined across partners 1, 2, and 3.
Distributions of and correlations between study variables, adjusting for age and gender
Table 1 presents the percentage of adolescents at baseline reporting each negative life event during the past year. Life events and supportive friendship composite variables were normally distributed, while sexual risk taking composite variables were positively skewed (see Table 2). Natural logs of sexual risk taking variables were examined in subsequent analyses. Paired sample t-tests indicated that sexual risk taking increased across the 1-year period between assessments (i.e., adolescents reported more frequent engagement in substance use prior to sexual activity and less frequent condom use over time; all p’s<.05; not shown in table).
Table 2.
Distributions of untransformed study variables and correlations, adjusting for age and gender. 1
| Mean | SD | Range | 1. | 2. | 3. | 4. | 5a. | 5b. | 6a. | 6b. | 7a. | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Uncontrollable life events | 2.6 | 2.1 | 0-10 | ||||||||||
| 2. Potentially controllable life events | 2.8 | 1.6 | 0-7 | .45 *** | |||||||||
| 3. Instrumental aid from friends | 3.5 | 0.8 | 1.7-5 | .11 | .04 | ||||||||
| 4. Intimacy with friends | 3.8 | 1.0 | 1-5 | .04 | .07 | .45 *** | |||||||
| 5. Inconsistent condom use | |||||||||||||
| a. Baseline | 5.7 | 5.7 | 0-30 | .12 | .15 | .04 | .09 | ||||||
| b. Follow-up | 6.7 | 5.6 | 0-24 | .18 * | .11 | .20 | .22 * | .42 *** | |||||
| 6. Alcohol use before sex | |||||||||||||
| a. Baseline | 4.9 | 4.6 | 0-25 | .24 ** | .14 | -.03 | .09 | .68 *** | .27 * | ||||
| b. Follow-up | 5.0 | 4.5 | 0-22 | .26 ** | .13 | .19 * | .18 | .18 | .71 *** | .40 *** | |||
| 7. Marijuana use before sex | |||||||||||||
| a. Baseline | 6.1 | 6.3 | 0-32 | .33 *** | .15 | -.06 | -.01 | .67 *** | .25 * | .87 *** | .39 *** | ||
| b. Follow-up | 6.8 | 6.7 | 0-35 | .19 * | .12 | .08 | .10 | .19 | .63 *** | .38 *** | .81 *** | .55 *** |
Baseline report of life events and supportive friendship variables are reported. Natural log transformations were performed on sexual risk behavior variables prior to analyses.
p<.05,
p<.01,
p<.001
Adolescents who reported a greater number of uncontrollable stressful life events at baseline also reported a greater number of potentially controllable life events. In addition, they reported more frequent alcohol or marijuana use before having sex at baseline and follow-up, and less frequent condom use at follow-up (see Table 2). Life events, however, were not associated with indices of social support. Sexual risk taking variables were correlated with one another within and across time points, with two important exceptions: inconsistent condom use at baseline was not associated with frequency of alcohol or marijuana use prior to having sex at the 1-year follow-up assessment. In contrast, alcohol or marijuana use prior to having sex at baseline was associated with more inconsistent condom use at the 1-year follow-up assessment. Greater instrumental aid from friends and intimacy with friends at baseline was associated with more frequent alcohol use before having sex and inconsistent condom use at follow-up, respectively.
Regressions of Sexual Risk Taking Variables on Stressful Life Events
Regressions of sexual risk taking variables on stressful life events are presented in three parts: (1) cross-sectional analyses among adolescents who were sexually active at baseline, (2) longitudinal analyses among adolescents who were sexually active at follow-up, (3) longitudinal analyses that adjusted for baseline sexual risk taking among the subset of adolescents who were sexually active at both baseline and follow-up.
Baseline analyses
Adolescents who reported a greater number of uncontrollable life events reported more frequent alcohol use and marijuana use before having sex at baseline (see Table 3, Model 1). These effects held when including potentially controllable life events as a covariate in the models (see Table 3, Model 2).
Table 3.
Regressions of sexual risk taking variables on stressful life events. 1
| Alcohol Use before Sex Est. (s.e.) | Marijuana Use before Sex Est. (s.e.) | Inconsistent condom use Est. (s.e.) | ||||
|---|---|---|---|---|---|---|
| Baseline | Follow-up | Baseline | Follow-up | Baseline | Follow-up | |
| Base Model | ||||||
| Age | .22 (.04) *** | .05 (.05) | .22 (.05) *** | .03 (.05) | .22 (.05) *** | .14 (.05) ** |
| Female Gender | .09 (.12) | .17 (.13) | .23 (.14) | .30 (.16) | -.11 (.14) | -.07 (.15) |
| Model 1 | ||||||
| Uncontrollable life events | .08 (.03) ** | .10 (.03) ** | .12 (.03) *** | .09 (.04) ** | .05 (.03) | .07 (.04) * |
| Model 2 | ||||||
| Uncontrollable life events | .08 (.03) * | .10 (.03) ** | .12 (.04) ** | .09 (.04) * | .03 (.04) | .07 (.04) |
| Potentially controllable life events | .01 (.04) | .00 (.04) | -.01 (.05) | .00 (.05) | .05 (.05) | .01 (.05) |
The base model shows the effects of age and female gender on sexual risk taking outcomes. All subsequent models include age and gender as covariates, but these effects are not shown in the table. All models adjust for potential effects of friendship network on sexual risk taking. N=127 for baseline analyses and N=115 for prospective follow-up analyses.
p<.05,
p<.01,
p<.001
Longitudinal analyses on adolescents who were sexually active at follow-up
Adolescents who reported a greater number of uncontrollable life events at baseline reported more inconsistent condom use, alcohol use before sex, and marijuana use before sex at the 1-year follow-up assessment (see Table 3, Model 1). When potentially controllable life events were included as a covariate, uncontrollable life events remained associated with more frequent alcohol use and marijuana use before having sex (see Table 3, Model 2). Thus, having a greater number of uncontrollable life stressors at baseline was associated with greater levels of substance use before sex one year later.
Longitudinal analyses on adolescents who were sexually active at both time points
When baseline level of risk taking was added as a covariate, uncontrollable life events remained associated with more frequent alcohol use before having sex among the 85 adolescents who were sexually active at both time points (Est.(s.e.)=.10 (.04), p<.05, not shown in table). Thus, having a greater number of uncontrollable life stressors at baseline was associated with greater increases in alcohol use before sex from baseline to follow-up.
Moderating Effects of Supportive Friendships
Baseline analyses
Five of the six interactions between uncontrollable life events and supportive friendships were statistically significant (see Table 4). Higher numbers of uncontrollable life events were associated with more frequent alcohol use before sex among adolescents who reported low instrumental aid from friends or low intimacy with friends. There was no association between uncontrollable life events and alcohol use before sex among adolescents who reported high support from friends. Figure 1a depicts an illustrative interaction, showing that adolescents who reported high support engaged in intermediate levels of alcohol use, regardless of stress. The significant interaction between uncontrollable life events and intimacy with friends in predicting marijuana use before sex (see Table 4) paralleled the association observed for alcohol use before sex.
Table 4.
Moderating effects of supportive friendships on associations between uncontrollable life events and sexual risk taking. 1
| Outcome: Alcohol Use before Sexual Activity Est. (s.e.) | Outcome: Marijuana Use before Sexual Activity Est. (s.e.) | Outcome: Inconsistent Condom Use Est. (s.e.) | ||||
|---|---|---|---|---|---|---|
| Baseline | Follow-up | Baseline | Follow-up | Baseline | Follow-up | |
| Instrumental aid from friends | -.06 (.08) | .15 (.08) | -.09 (.09) | .11 (.10) | .02 (.09) | .18 (.10) |
| Uncontrollable life events (ULE) | .08 (.03) * | .10 (.03) ** | .13 (.04) ** | .10 (.04) * | .03 (.04) | .08 (.04) * |
| Interaction | -.11 (.04) ** | -.13 (.04) ** | -.06 (.04) | -.07 (.05) | -.09 (.04) * | -.11 (.05) * |
| Effect of ULE in low instrumental aid group | .11 (.05) * | .15 (.04) *** | --- | --- | .06 (.05) | .14 (.04) ** |
| Effect of ULE in high instrumental aid group | .05 (.05) | -.03 (.06) | --- | --- | .03 (.06) | -.04 (.07) |
|
| ||||||
| Intimacy with friends | .09 (.07) | .15 (.07) * | .01 (.07) | .09 (.08) | .12 (.07) | .21 (.08) * |
| Uncontrollable life events (ULE) | .08 (.03) * | .09 (.04) * | .13 (.04) ** | .09 (.04) * | .03 (.04) | .07 (.04) |
| Interaction | -.10 (.03) ** | -.06 (.03) | -.07 (.03) * | -.03 (.04) | -.10 (.03) ** | -.05 (.04) |
| Effect of ULE in low intimacy group | .14 (.05) ** | --- | .18 (.05) ** | --- | .09 (.05) | --- |
| Effect of ULE in high intimacy group | -.04 (.05) | --- | .04 (.05) | --- | -.08 (.06) | --- |
Analyses are adjusted for age, gender, potentially controllable life events, and friendship network. Instrumental aid from friends and intimacy with friends were entered into separate regressions. N=119 for baseline analyses and N=109 for prospective follow-up analyses.
p<.05,
p<.01,
p<.001
Figure 1.
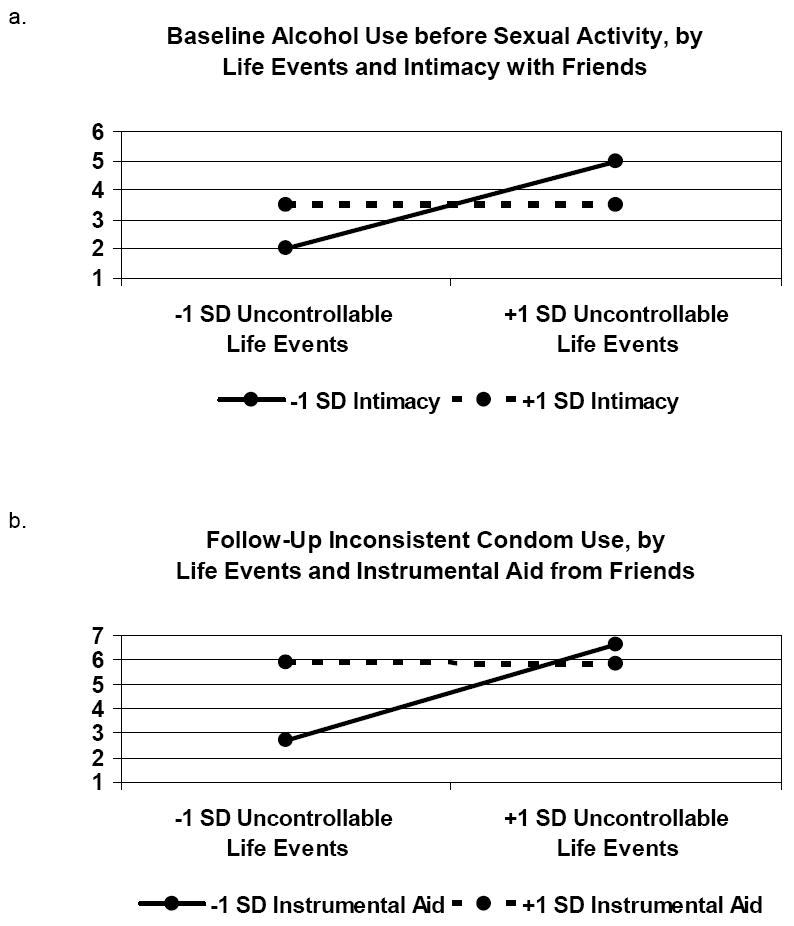
Illustrative interactions between stressful life events and supportive friendships.
Uncontrollable life events also interacted with supportive friendships to influence inconsistent condom use (see Table 4). Although the simple effects tests in this case were non-significant, graphical representation of the data (not shown) suggested that higher numbers of uncontrollable life events were associated with higher levels of inconsistent condom use only among adolescents who reported low instrumental aid from friends or low intimacy with friends. Regardless of stress, adolescents who reported high instrumental aid engaged in moderate levels of inconsistent condom use, while adolescents who reported high intimacy engaged in high levels of inconsistent condom use.
Longitudinal analyses on adolescents who were sexually active at follow-up
When sexual risk taking at the 1-year follow-up was the outcome, two of the six interactions between uncontrollable stressful life events and supportive friendships were significant (see Table 4). Higher numbers of uncontrollable life events at baseline were associated with more frequent alcohol use before sex at follow-up among adolescents who reported low instrumental aid from friends at baseline. Adolescents reporting high instrumental aid engaged in intermediate levels of alcohol use before sex at follow-up, regardless of stress. Higher numbers of uncontrollable life events were also associated with more inconsistent condom use at follow-up among adolescents who reported low instrumental aid. Among adolescents who reported high instrumental aid, level of inconsistent condom use was relatively high and was unaffected by level of uncontrollable stressors. Figure 1b illustrates this interaction.
Longitudinal analyses on adolescents who were sexually active at both time points
Baseline level of risk taking was included in longitudinal analyses to test whether uncontrollable life events and supportive friendships interacted to influence changes in sexual risk taking among the smaller sample of adolescents who were sexually active at both time points. No interaction effects were significant from this set of analyses.
Discussion
Results suggest that adolescents may engage in sexual risk taking as a response to stressful life events. Adjusting for age, gender, friendship network membership, and potentially controllable life stressors, adolescents who reported greater numbers of uncontrollable life stressors during the past year reported more frequent alcohol and marijuana use before sex at baseline and one year later, at follow-up. Among a smaller subset of adolescents who were sexually active at both time points, uncontrollable life stressors at baseline were associated with increases in frequency of alcohol use before sex over time. Research indicates that substance use prior to sexual activity may increase the likelihood that adolescents engage in unprotected sexual intercourse (Hingson et al., 1990; Jemmott & Jemmott, 1993; Kingree et al., 2000). In the present study, substance use prior to sexual activity at baseline was associated with inconsistent condom use at the follow-up assessment.
One of the most striking findings to emerge from the present study was the percentage of adolescents reporting relatively severe stressors. Our findings are consistent with other research showing that disadvantaged adolescents experience chronic, severe forms of stress (Attar et al., 1994; Evans et al., 2005; McLoyd, 1998; Simons et al., 2002). Observed links between uncontrollable stressful life events and sexual risk taking may aid in understanding why rates of sexually transmitted infections are high among lower socioeconomic status African American youth (CDC, 2006; Ford et al., 2005; Newbern et al., 2004). Protecting one’s physical health may seem relatively unimportant to adolescents who feel overwhelmed by life stressors and who may engage in risk behavior to temporarily reduce distress or escape from stressful life circumstances. Adolescents with multiple life stressors may also have a smaller repertoire of coping skills from which to choose. In support of this idea, research suggests that stress influences levels of substance use among adolescents by impairing the development of social competency skills (Fishbein et al., 2006). In the present study, adolescents who reported higher numbers of uncontrollable life events also reported higher numbers of potentially controllable life events. This is consistent with the idea that stressful life circumstances increase the likelihood that adolescents make poor choices regarding behavior.
By enhancing adolescents’ social skills and coping repertoire, interventions may broadly influence health behavior over the long term. For example, Griffin, Botvin, and Nichols (2006) found that a substance use prevention intervention, Life Skills Training, had a direct protective effect on sexual risk behavior over 10 years later. The program includes a focus on building cognitive-behavioral skills to enhance self-esteem, manage anxiety, communicate effectively, develop personal relationships, and assert one’s rights. Health protective sexual behavior may thus be fostered by social contexts that promote the development of confidence and general competence among adolescents.
Stress-buffering model of social relationships versus peer socialization of risk
Peer relationships are an important social context that may influence sexual behavior among adolescents (e.g., Dolcini, Harper, Boyer, Pollack, & Adolescent Medicine Trials Network for HIV/AIDS Interventions, 2008; Romer et al., 1994). One purpose of the present study was to test competing conceptualizations of how stressful life events might be associated with health risk behavior among adolescents who report less supportive or more supportive friendships. The stress-buffering model predicts that social relationships will protect adolescents from engaging in health risk behavior as a response to stressful life events (Cohen et al., 2001). According to the stress-buffering model, however, adolescents with many resources for support should engage in relatively low levels of health risk behavior, regardless of stress level. In contrast, a peer socialization of risk model predicts that adolescents with many resources for support from peers will engage in moderate to high levels of risk behavior, perhaps due to identification with risk taking peers or increased opportunities to engage in risk behavior during unsupervised gatherings of peers (Gardner & Steinberg, 2005; Jessor, 1984). This process may occur regardless of stress level.
Consistent with our hypothesis, the accumulation of uncontrollable stressful life events was associated with more frequent alcohol and marijuana use before sex and with more frequent failure to use condoms only among adolescents who reported low levels of supportive friendships. Patterns of sexual risk taking among adolescents who were well connected with peers appeared most consistent with a peer socialization of risk model. Adolescents with highly supportive friendships engaged in moderate to high levels of sexual risk taking regardless of stress level. These adolescents may have a similar risk behavior profile to those adolescents who engage in risk only when they experience high levels of stress and low levels of support, but the behavior of each group appears to be driven by different underlying motivations.
Some health professionals advocate delivering peer-based health promotion interventions to friendship networks in order to influence norms surrounding risk behavior (e.g., Dolcini et al., 2005; Fang, Stanton, Li, Feigelman, & Baldwin, 1998). Although youth who perceive that their peers are engaging in sexual activity are more likely to engage in sexual activity themselves (e.g., Boyer, Tschann, & Shafer, 1999; Romer et al., 1994), peer influence extends to health protective sexual behaviors as well. In the same sample of adolescents examined in this study, for example, those adolescents who knew that their peers were using condoms were more likely to protect themselves in this way one year later (Paxton, Dolcini, Harper, & Becerra-Guzman, 2008). Peer-based health-promotion interventions targeting friendship groups have been shown to increase condom use up to 6 months later (Stanton et al., 1996). Qualitative work, moreover, suggests that sexual education interventions with friends allow both male and female adolescents to feel more comfortable, reveal sensitive information, relate to each other’s experiences, and protect one another (Harper et al., 2008).
The net effect of socialization with peers may be positive
We do not wish to give the impression that close friendships during adolescence should be discouraged. If low levels of socialization with peers were health protective, sexual risk taking should have been uniformly low among the adolescents in our study who reported low levels of supportive friendships. Instead, these adolescents engaged in high levels of sexual risk taking when they experienced a greater number of stressful life events. The fact that uncontrollable stressful life events were not associated with sexual risk taking among adolescents who reported highly supportive friendships must be viewed as positive. Research has documented the beneficial effects of having supportive friendships (Berndt, 1996; Brown et al., 1997; Laursen, Furman, & Mooney, 2006). The present findings show that resiliency to stress is one of the benefits conferred by having strong social connections with peers. Resiliency to stress is especially important to adolescents living within disadvantaged environments (Allison et al., 1999; Grant et al., 2005).
Study strengths and limitations
It is both a strength and limitation of the present study that we focused on a single inner-city neighborhood. Even though other studies involving middle-class and ethnically diverse samples of adolescents have formed similar conclusions regarding stress and risk behavior (e.g., Cooper et al., 1998; Griffin et al., 2006; Wills et al., 2003), our results cannot be assumed to generalize to relatively advantaged groups of adolescents and other ethnic groups. Due to the reported sexual behavior of our sample, the generalizability of our findings is limited to heterosexual adolescents. We had low power to detect interactions between stressful life events and coping in longitudinal analyses among the smaller subset of adolescents who were sexually active at both time points. Although we relied on adolescents’ recall of their sexual behaviors and related substance use during the past year, self-report of these behaviors have been shown to be reliable (Catania, Gibson, Chitwood, & Coates, 1990; Forman & Linney, 1991).
The present study’s strengths include its community sample, longitudinal design, and initial use of random digit dialing, increasing our ability to generalize findings to similar inner-city communities of African American adolescents. We also created measures of sexual risk taking that reflected multiple dimensions that contribute to risk (i.e., frequency of substance use and inconsistent condom use weighted by frequency of sexual activity across different partners).
Directions for future research
Future studies incorporating multiple assessment points should examine whether stressful life circumstances are linked with substance use prior to sexual activity, inconsistent condom use, and contraction of sexually transmitted infections in a manner that suggests a causal chain of events. Investigating how stressful life circumstances may influence other types of substance use before sexual activity, such as stimulants, is also warranted, given how links between stimulant use and sexual risk taking have been observed among some populations (e.g., Semple, Zians, Grant, & Patterson, 2006).
Research should also investigate whether patterns of risk behavior are equally harmful regardless of motivation or whether some motivations place adolescents at particular risk for experiencing long-term negative outcomes. It is possible that adolescents who engage in health risk behavior as a means of fitting in with peers may lessen risk behavior over time as they become more comfortable in the group dynamic and as developmentally normative levels of health risk behavior decline (Silbereisen & Kracke, 1997). In contrast, adolescents who engage in risk behavior as a stress response may escalate risk behavior over time, especially if new stressors occur. Early risk behavior, particularly in the context of having low social support, might lead to the development of maladaptive patterns of coping with stress.
Future research should also further examine the stress-buffering and peer socialization of risk roles of friends during adolescence. Friends may be more likely to socialize risk if the outcome in question involves behavior that is pleasurable and socially normative during adolescence. Friends may be more likely to buffer one another from stress if outcomes involve risk taking behavior that is not pleasurable. Research should attempt to delineate when in the developmental process friends cease facilitating risk and begin to primarily serve a stress-buffering role, consistent with the literature on adults (Cohen et al., 2001; Cohen & Wills, 1985).
Conclusions
Supportive friendships may protect disadvantaged adolescents from engaging in sexual risk taking as a stress response. However, supportive friendships do not necessarily prevent adolescents from engaging in risk. Different processes may explain sexual risk taking among adolescents who have relatively low or high support from friends. Adolescents with minimal support may be prone to engagement in health risk behavior as a stress response, while those with higher levels of support may engage in risk primarily due to peer socialization. Future research should investigate multiple types of risk behavior, examine whether patterns of risk behavior are equally harmful in the long-term, regardless of motivation, and further examine the stress-buffering role that friends may serve during adolescence.
High rates of sexually transmitted infections among African American inner-city communities (STD Control Section, 2007) may be partially addressed by tailoring interventions on the basis of reported life stressors and social support. Adolescents with few resources for support may benefit from programs in which adults take an active role in providing support and teaching life skills, including adaptive strategies for coping with stress. Such programs should address the potentially high number of stressful life events that adolescents may experience and anticipate that some events involving family members (e.g., serious illness, mental health problems, incarceration) may limit adolescents’ access to adults who are ordinarily resources for support. It may be necessary to build or enhance adolescents’ familial and extra-familial support networks to promote adaptive strategies for coping with stress. Adolescents with many resources for support, particularly from friends, may benefit from peer-based health promotion programs that seek to influence norms surrounding risk behavior within friendship networks (Dolcini, Harper, Boyer, Watson, et al., 2008; Dolcini, Harper, Boyer, Pollack, et al., 2008). This may serve to offset potential peer socialization to engage in risk.
Acknowledgments
This research was funded by a grant from the National Institute of Mental Health (R01 MH57234) awarded to Dr. Dolcini while she was on faculty at the University of California, San Francisco. Part of Dr. Brady’s preparation of this manuscript was supported by the Ruth L. Kirschstein National Research Service Award (T32 MH019391). We would like to acknowledge the contributions of Susan E. Watson, Gail Bolan, Jonathon Ellen, Joseph Catania, Nancy Adler, Bradford Brown, Julie Wall, Lei Han, Jason Chang, and Torsten Neilands in conducting various aspects of this study, as well as the dedicated work of staff members. The generous support of the community, especially the youth who participated in the study and their families, was critical to the success of this project.
Footnotes
Publisher's Disclaimer: The following manuscript is the final accepted manuscript. It has not been subjected to the final copyediting, fact-checking, and proofreading required for formal publication. It is not the definitive, publisher-authenticated version. The American Psychological Association and its Council of Editors disclaim any responsibility or liabilities for errors or omissions of this manuscript version, any version derived from this manuscript by NIH, or other third parties. The published version is available at http://www.apa.org/journals/hea/
Contributor Information
Sonya S. Brady, University of Minnesota School of Public Health Division of Epidemiology & Community Health
M. Margaret Dolcini, Oregon State University College of Health & Human Sciences Department of Public Health
Gary W. Harper, DePaul University College of Liberal Arts and Sciences Department of Psychology
Lance M. Pollack, University of California, San Francisco Center for AIDS Prevention Studies
References
- Aiken LS, West SG. Multiple regression: Testing and interpreting interactions. Newbury Park, California: Sage Publications, Inc; 1991. [Google Scholar]
- Allison KW, Burton L, Marshall S, Perez-Febles A, Yarrington J, Kirsch LB, Merriwether-DeVries C. Life experiences among urban adolescents: Examining the role of context. Child Development. 1999;70:1017–1029. doi: 10.1111/1467-8624.00074. [DOI] [PubMed] [Google Scholar]
- Attar B, Guerra N, Tolan P. Neighborhood disadvantage, stressful life events, and adjustment in urban elementary-school children. Journal of Clinical Child Psychology. 1994;23:391–400. [Google Scholar]
- Berenson AB, Wiemann CM, McCombs S. Exposure to violence and associated health risk behaviors among adolescent girls. Archives of Pediatric Adolescent Medicine. 2001;155:1238–1242. doi: 10.1001/archpedi.155.11.1238. [DOI] [PubMed] [Google Scholar]
- Berndt TJ. Transitions in friendship and friends’ influence. In: Graber JA, Brooks-Gunn J, Petersen AC, editors. Transitions through adolescence: Interpersonal domains and context. Mahwah, New Jersey: Lawrence Erlbaum Associates; 1996. pp. 23–53. [Google Scholar]
- Bolland JM. Hopelessness and risk behavior among adolescents living in high-poverty inner-city neighborhoods. Journal of Adolescence. 2003;26:145–158. doi: 10.1016/s0140-1971(02)00136-7. [DOI] [PubMed] [Google Scholar]
- Boyer CB, Tschann JM, Shafer M. Predictors of risk for sexually transmitted diseases in ninth-grade urban high-school students. Journal of Adolescent Research. 1999;14:448–465. doi: 10.1177/0743558499144004. [DOI] [PubMed] [Google Scholar]
- Brady SS, Donenberg GR. Mechanisms linking violence exposure to health risk behavior in adolescence: Motivation to cope and sensation-seeking personality. Journal of the American Academy of Child and Adolescent Psychiatry. 2006;45:673–680. doi: 10.1097/01.chi.0000215328.35928.a9. [DOI] [PubMed] [Google Scholar]
- Brady SS, Matthews KA. The influence of socioeconomic status and ethnicity on adolescents’ exposure to stressful life events. Journal of Pediatric Psychology. 2002;27:575–583. doi: 10.1093/jpepsy/27.7.575. [DOI] [PubMed] [Google Scholar]
- Brown BB, Dolcini MM, Leventhal A. Transformations in peer relationships at adolescence: Implications for health-related behavior. In: Schulenberg J, Maggs JL, Hurrelmann K, editors. Health risks and developmental transitions during adolescence. New York, NY: Cambridge University Press; 1997. pp. 161–189. [Google Scholar]
- Catania JA, Gibson DR, Chitwood DD, Coates TJ. Methodological problems in AIDS behavioral research: Influences on measurement error and participation bias in studies of sexual behavior. Psychological Bulletin. 1990;108:339–362. doi: 10.1037/0033-2909.108.3.339. [DOI] [PubMed] [Google Scholar]
- Centers for Disease control and Prevention. HIV/AIDS Surveillance in Adolescents and Young Adults (through 2005) Slide Set [internet] 2007 October Available: http://www.cdc.gov/hiv/topics/surveillance/resources/slides/adolescents/index.htm.
- Centers for Disease Control and Prevention. Sexually Transmitted Disease Surveillance, 2005. Atlanta, GA: U.S Department of Health and Human Services; 2006. Nov, [Google Scholar]
- Cohen D, Spear S, Scribner R, Kissinger P, Mason K, Wildgen J. “Broken windows” and the risk of gonorrhea. American Journal of Public Health. 2000;90:230–236. doi: 10.2105/ajph.90.2.230. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cohen S. Social relationships and health. American Psychologist. 2004;59:676–684. doi: 10.1037/0003-066X.59.8.676. [DOI] [PubMed] [Google Scholar]
- Cohen S, Gottlieb BH, Underwood LG. Social relationships and health: Challenges for measurement and intervention. Advances in Mind-Body Medicine. 2001;17:129–141. [PubMed] [Google Scholar]
- Cohen S, Wills TA. Stress, social support, and the buffering hypothesis. Psychological Bulletin. 1985;98:310–357. [PubMed] [Google Scholar]
- Cooper ML, Peirce RS, Huselid RF. Substance use and sexual risk taking among black adolescents and white adolescents. Health Psychology. 1994;13:251–262. doi: 10.1037//0278-6133.13.3.251. [DOI] [PubMed] [Google Scholar]
- Cooper ML, Shapiro CM, Powers AM. Motivations for sex and risky sexual behavior among adolescents and young adults: A functional perspective. Journal of Personality and Social Psychology. 1998;75:1528–1558. doi: 10.1037//0022-3514.75.6.1528. [DOI] [PubMed] [Google Scholar]
- DiClemente RJ, Lodico M, Grinstead OA, Harper G, Rickman RL, Evans PE, Coates TJ. African American adolescents residing in high-risk urban environments do use condoms: Correlates and predictors of condom use among adolescents in public housing developments. Pediatrics. 1996;98:269–278. [PubMed] [Google Scholar]
- Dolcini MM, Adler NE. Perceived competencies, peer group affiliation, and risk behavior among early adolescents. Health Psychology. 1994;13:496–506. doi: 10.1037//0278-6133.13.6.496. [DOI] [PubMed] [Google Scholar]
- Dolcini MM, Harper GW, Boyer CB, Pollack LM. Adolescent Medicine Trials Network for HIV/AIDS Interventions. Project ÒRÉ: A friendship based intervention to prevent HIV/STIs in urban African American adolescent females. 2008 doi: 10.1177/1090198109333280. Manuscript submitted for publication. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dolcini MM, Harper GW, Boyer CB, Watson SE, Anderson M, Pollack LM, Chang JY. Preliminary findings on a brief friendship-based HIV/STI intervention for urban African American youth: Project ÒRÉ. Journal of Adolescent Health. 2008;42:629–633. doi: 10.1016/j.jadohealth.2007.11.003. [DOI] [PubMed] [Google Scholar]
- Dolcini MM, Harper GW, Watson SE, Catania JA, Ellen JM. Friends in the ‘hood: Should peer-based health promotion programs target nonschool friendship networks? Journal of Adolescent Health. 2005;36:267e6–267e15. doi: 10.1016/j.jadohealth.2004.10.003. [DOI] [PubMed] [Google Scholar]
- Ellen JM, Jennings JM, Meyers T, Chung S, Taylor R. Perceived social cohesion and prevalence of sexually transmitted diseases. Sexually Transmitted Diseases. 2004;31:117–122. doi: 10.1097/01.OLQ.0000110467.64222.61. [DOI] [PubMed] [Google Scholar]
- Evans GW, Gonnella C, Marcynyszyn LA, Gentile L, Salpekar N. The role of chaos in poverty and children’s socioemotional adjustment. Psychological Science. 2005;16:560–565. doi: 10.1111/j.0956-7976.2005.01575.x. [DOI] [PubMed] [Google Scholar]
- Fang X, Stanton B, Li X, Feigelman S, Baldwin R. Similarities in sexual activity and condom use among friends within groups before and after a risk-reduction intervention. Youth & Society. 1998;29:431–450. doi: 10.1177/0044118x98029004002. [DOI] [PubMed] [Google Scholar]
- Fishbein DH, Herman-Stahl M, Eldreth D, Paschall MJ, Hyde C, Hubal R, Hubbard S, Williams J, Ialongo N. Mediators of the stress-substance-use relationship in urban male adolescents. Prevention Science. 2006;7:113–126. doi: 10.1007/s11121-006-0027-4. [DOI] [PubMed] [Google Scholar]
- Ford CA, Pence BW, Miller WC, Resnick MD, Bearinger LH, Pettingell S, Cohen M. Predicting adolescents’ longitudinal risk for sexually transmitted infection. Archives of Pediatrics and Adolescent Medicine. 2005;159:657–664. doi: 10.1001/archpedi.159.7.657. [DOI] [PubMed] [Google Scholar]
- Forman S, Linney J. Increasing the validity of self-report data in effectiveness trials. NIDA Research Monographs. 107:235–247. [PubMed] [Google Scholar]
- Furman W, Buhrmester W. Children’s perceptions of the personal relationships in their social networks. Developmental Psychology. 1985;21:1016–1024. [Google Scholar]
- Gardner M, Steinberg L. Peer influence on risk taking, risk preference, and risky decision making in adolescence and adulthood: An experimental study. Developmental Psychology. 2005;41:625–635. doi: 10.1037/0012-1649.41.4.625. [DOI] [PubMed] [Google Scholar]
- Goodman E, McEwen BS, Dolan LM, Schafer-Kalkhoff T, Adler NE. Social disadvantage and adolescent stress. Journal of Adolescent Health. 2005;37:484–492. doi: 10.1016/j.jadohealth.2004.11.126. [DOI] [PubMed] [Google Scholar]
- Grant KE, McCormick A, Poindexter L, Simpkins T, Janda CM, Thomas KJ, Campbell A, Carleton R, Taylor J. Exposure to violence and parenting as mediators between poverty and psychological symptoms in urban African American adolescents. Journal of Adolescence. 2005;28:507–521. doi: 10.1016/j.adolescence.2004.12.001. [DOI] [PubMed] [Google Scholar]
- Griffin KW, Botvin GJ, Nichols TR. Effects of a school-based drug prevention program for adolescents on HIV risk behavior in young adulthood. Prevention Science. 2006;7:103–112. doi: 10.1007/s11121-006-0025-6. [DOI] [PubMed] [Google Scholar]
- Gutman LM, McLoyd VC, Tokoyawa T. Financial strain, neighborhood stress, parenting behaviors, and adolescent adjustment in urban African American families. Journal of Research on Adolescence. 2005;15:425–449. [Google Scholar]
- Harper GW, Dolcini MM, Benhorin S, Watson SE, Boyer CB, Anderson M. The benefits of a friendship-based HIV/STI prevention intervention for African American youth. 2008 doi: 10.1016/j.jadohealth.2007.11.003. Manuscript submitted for publication. [DOI] [PubMed] [Google Scholar]
- He K, Kramer E, Houser RF, Chomitz VR, Hacker KA. Defining and understanding healthy lifestyles choices for adolescents. Journal of Adolescent Health. 2004;35:26–33. doi: 10.1016/j.jadohealth.2003.09.004. [DOI] [PubMed] [Google Scholar]
- Henrich CC, Brookmeyer KA, Shrier LA, Shahar G. Supportive relationships and sexual risk behavior in adolescence: An ecological-transactional approach. Journal of Pediatric Psychology. 2006;31:286–297. doi: 10.1093/jpepsy/jsj024. [DOI] [PubMed] [Google Scholar]
- Hingson RW, Struinin L, Berlin BM, Heeren T. Beliefs about AIDS, use of alcohol and drugs, and unprotected sex among Massachusetts adolescents. American Journal of Public Health. 1990;80:295–299. doi: 10.2105/ajph.80.3.295. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jemmott JB, III, Jemmott LS. Alcohol and drug use during sexual activity: Predicting the HIV-risk-related behaviors of inner-city Black male adolescents. Journal of Adolescent Research. 1993;8:41–57. [Google Scholar]
- Jessor R. Adolescent development and behavioral health. In: Matarazzo JD, Weiss SM, Herd JA, Miller NE, Weiss SM, editors. Behavioral health: A handbook of health enhancement and disease prevention. New York: John Wiley & Sons, Inc; 1984. pp. 69–90. [Google Scholar]
- Jessor R, Donovan JE, Costa F. Personality, perceived life chances, and adolescent behavior. In: Hurrelmann K, Hamilton SF, editors. Social Problems and Social Contexts in Adolescence: Perspectives across Boundaries. New York: Aldine de Gruyter; 1996. pp. 219–233. [Google Scholar]
- Kingree JB, Braithwaite R, Woodring T. Unprotected sex as a function of alcohol and marijuana use among adolescent detainees. Journal of Adolescent Health. 2000;27:179–185. doi: 10.1016/s1054-139x(00)00101-4. [DOI] [PubMed] [Google Scholar]
- Laursen B, Furman W, Mooney KS. Predicting interpersonal competence and self-worth from adolescent relationships and relationship networks: Variable-centered and person-centered perspectives. Merrill-Palmer Quarterly. 2006;52:572–600. [Google Scholar]
- McCubbin HI, Needle RH, Wilson M. Adolescent health risk behaviors: Family stress and adolescent coping as critical factors. Family Relations. 1985;34:51–62. [Google Scholar]
- McCulloch CE, Searle SR. Generalized, Linear, and Mixed Models. New York: John Wiley and Sons; 2001. [Google Scholar]
- McLoyd V. Socioeconomic disadvantage and child development. American Psychologist. 1998;53:185–204. doi: 10.1037//0003-066x.53.2.185. [DOI] [PubMed] [Google Scholar]
- Newbern EC, Miller WC, Schoenbach VJ, Kaufman JS. Family socioeconomic status and self-reported sexually transmitted diseases among Black and White American adolescents. Sexually Transmitted Diseases. 2004;31:533–541. doi: 10.1097/01.olq.0000137898.17919.35. [DOI] [PubMed] [Google Scholar]
- Paxton KC, Dolcini MM, Harper GW, Becerra-Guzman N. A longitudinal examination of the impact of family and friends on sexual behaviors of African American adolescents. 2008 Manuscript in preparation. [Google Scholar]
- Romer D, Black M, Ricardo I, Feigelman S, Kaljee L, Galbraith J, Nesbit R, Hornik RC, Stanton B. Social influences on the sexual behavior of youth at risk for HIV exposure. American Journal of Public Health. 1994;84:977–985. doi: 10.2105/ajph.84.6.977. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Semple SJ, Zians J, Grant I, Patterson TL. Methamphetamine use, impulsivity, and sexual risk behavior among HIV-positive men who have sex with men. Journal of Addictive Diseases. 2006;25:105–114. doi: 10.1300/J069v25n04_10. [DOI] [PubMed] [Google Scholar]
- Silbereisen RK, Kracke B. Self-reported maturational timing and adaptation in adolescence. In: Schulenberg J, Maggs JL, Hurrelmann K, editors. Health risks and developmental transitions during adolescence. New York: Cambridge University Press; 1997. pp. 85–109. [Google Scholar]
- Sieving RE, Eisenberg ME, Pettingell S, Skay C. Friends’ influence on adolescents’ first sexual intercourse. Perspectives on Sexual and Reproductive Health. 2006;38:13–19. doi: 10.1363/psrh.38.013.06. [DOI] [PubMed] [Google Scholar]
- Silverman JG, Raj A, Mucci LA, Hathaway JE. Dating violence against adolescent girls and associated substance use, unhealthy weight control, sexual risk behavior, pregnancy, and suicidality. Journal of the American Medical Association. 2001;286:572–579. doi: 10.1001/jama.286.5.572. [DOI] [PubMed] [Google Scholar]
- Simons RL, Murry V, McLoyd V, Lin K, Cutrona C, Conger RD. Discrimination, crime, ethnic identity, and parenting as correlates of depressive symptoms among African American children: A multilevel analysis. Development and Psychopathology. 2002;14:371–393. doi: 10.1017/s0954579402002109. [DOI] [PubMed] [Google Scholar]
- Stanton BF, Li X, Ricardo I, Galbraith J, Feigelman S, Kaljee L. A randomized, controlled effectiveness trial of an AIDS prevention program for low-income African-American youths. Archives of Pediatrics & Adolescent Medicine. 1996;150:363–372. doi: 10.1001/archpedi.1996.02170290029004. [DOI] [PubMed] [Google Scholar]
- STD Control Section. San Francisco Sexually Transmitted Disease Annual Summary, 2006. San Francisco Department of Public Health; San Francisco, California: Jul, 2007. Available: http://www.sfdph.org/dph/files/reports/StudiesData/STD/SFSTDAnnlSum2006.pdf. [Google Scholar]
- Voisin DR. The relationship between violence exposure and HIV sexual risk behaviors: Does gender matter? American Journal of Orthopsychiatry. 2005;75:497–506. doi: 10.1037/0002-9432.75.4.497. [DOI] [PubMed] [Google Scholar]
- Weinstock H, Berman S, Cates W., Jr Sexually transmitted diseases among American youth: Incidence and prevalence estimates, 2000. Perspectives on Sexual and Reproductive Health. 2004;36:6–10. doi: 10.1363/psrh.36.6.04. [DOI] [PubMed] [Google Scholar]
- Wiesner M, Juang L. Brief report: Parents’ life events and substance use among German adolescent girls: Testing a family mediation model. Journal of Adolescence. 2004;27:485–489. doi: 10.1016/j.adolescence.2004.03.002. [DOI] [PubMed] [Google Scholar]
- Wills TA. Stress and coping in early adolescence: Relationships to substance use in urban school samples. Health Psychology. 1986;5:503–529. doi: 10.1037//0278-6133.5.6.503. [DOI] [PubMed] [Google Scholar]
- Wills TA, Resko JA, Ainette MG, Mendoza D. Role of parent support and peer support in adolescent substance use: A test of mediated effects. Psychology of Addictive Behaviors. 2004;18:122–134. doi: 10.1037/0893-164X.18.2.122. [DOI] [PubMed] [Google Scholar]
- Wills TA, Sandy JM, Yaeger AM, Cleary SD, Shinar O. Coping dimensions, life stress, and adolescent substance use: A latent growth analysis. Journal of Abnormal Psychology. 2001;110:309–323. doi: 10.1037//0021-843x.110.2.309. [DOI] [PubMed] [Google Scholar]
- Wills TA, Vaccaro D, McNamara G. The role of life events, family support, and competence in adolescent substance use. American Journal of Community Psychology. 1992;20:349–374. doi: 10.1007/BF00937914. [DOI] [PubMed] [Google Scholar]
- Wills TA, Yaeger AM, Sandy JM. Buffering effect of religiosity for adolescent substance use. Psychology of Addictive Behaviors. 2003;17:24–31. doi: 10.1037/0893-164x.17.1.24. [DOI] [PubMed] [Google Scholar]
- Windle M. A longitudinal study of stress buffering for adolescent problem behaviors. Developmental Psychology. 1992;28:522–530. [Google Scholar]
- Windle M, Mun EY, Windle RC. Adolescent-to-young adulthood heavy drinking trajectories and their prospective predictors. Journal of Studies on Alcohol. 2005;66:313–322. doi: 10.15288/jsa.2005.66.313. [DOI] [PubMed] [Google Scholar]
- Zimmerman MA, Ramirez-Valles J, Zapert KM, Maton KI. A longitudinal study of stress-buffering effects for urban African American male adolescent problem behaviors and mental health. Journal of Community Psychology. 2000;28:17–33. [Google Scholar]