

Abstract
The quality of the child care environment and caregiver practices can potentially have significant, lasting impact on children’s social development. This study involves the development and a small-scale efficacy trial of the Carescapes program, a video-based training program that focuses on promoting positive social development in young children attending family child care. Fifty-seven caregivers who provided child care in their homes were randomly assigned to immediate intervention or waitlist control groups. Random coefficients analyses showed significant increased use of effective behavior management practices and decreased overall children’s problem behavior for the intervention group. A mediation model demonstrated that increases in effective behavior management practices were associated with decreases in problem behavior. A medium intervention effect was found for caregiver’s monitoring and a small effect for use of positive attention. These effects declined 5 months following the intervention. Implications for future efficacy and effectiveness studies in family child care settings that involve strategies to facilitate maintenance are discussed.
Children experience the greatest rate of development during the first 5 years of their lives, and besides the family environment, child care is the setting in which this growth predominately occurs (Shonkoff & Phillips, 2000). Child care is typically the first experience young children will have with a group of other young children, and thus plausibly can facilitate positive interactions and the formation of positive relationships among children, as well as the development of socially skilled behavior in young children. Evidence supports positive influence of child care quality on social outcomes (Loeb, Fuller, Kagan, & Carrol, 2004; NICHD Early Child Care Research Network, 2001; Peisner-Feinberg & Burchinal, 1997; Phillips, McCartney, & Scarr, 1987). Yet the NICHD large-scale study of Early Child Care and Youth Development brings into question whether child care quality has a lasting positive influence on children’s social development (Belsky et al., 2007; NICHD Early Child Care Research Network, 2003, 2004). Differential findings likely depend on the child’s age when the care is provided, the way in which child care quality is defined, and what social outcomes are assessed.
Much less is known about the extent to which the quality of care in family child care settings influences children’s social development. In family child care settings, the care of children is provided in the caregiver’s home. It is difficult to articulate empirical evidence that is solely pertinent to family child care as many studies have combined data from family and center-based care, or equivocal results have been found in the studies of family child care, likely due to low sample sizes or poor research designs (Kontos, 1992). A number of more recent studies have demonstrated that training for caregivers who provide child care in their homes was related to greater quality of care giving practices. Care providers in family child care settings with higher levels of training have been found to provide higher overall quality of child care (Norris, 2001; Weaver, 2002). Both level of education and training were shown to predict quality of caregiving in child care homes (Burchinal, Howes, & Kontos, 2002) and these predictions were stronger than those of adult-child ratio and caregiver experience.
Specific caregiver practices that have been associated with higher levels of training are more frequent engagement with children (Bordin, Machida, & Varnell, 2000), less detachment from children (Burchinal et al., 2002), and a greater likelihood for planning of child activities (Kontos, Howes, & Galinski, 1996). Although these caregiver practices have been shown to promote positive social development in children in center-based child care (e.g., Dunn, 1993; McCartney, Scarr, Phillips, & Grajek, 1985; Peisner-Feinberg et al., 2001), the studies in family child care settings did not directly investigate the impact of these caregiver practices on children’s behavior. A meta-analysis of caregiver training studies confirms positive impact of caregiver training on caregiver practices in regular child care and preschools, with fewer studies and weaker effects found for children’s skills and behavior (Fukkink & Lont, 2007). These results were found to generalize to child care providers with varying levels of education.
The Importance of Facilitating Positive Social Development in Young Children
A number of social skills in young children have been identified as important to overall social competence and peer acceptance. These include effective initiation of interactive social play, effective social responses, and cooperative interactions such as offering help and sharing (Odom & Ogawa, 1992). Children who lack such social skills are likely to experience a range of social problems and difficulties, such as peer rejection and aggression from playmates (Olson, 1992). Children lacking in social competencies are also at risk for developing internalizing problems, such as social withdrawal and anxiety (Olson & Rosenblum, 1998).
Social problems first identified during the preschool years tend to be stable (Richman, Stevenson, & Graham, 1982), and are likely to increase in severity over time (Walker, 1995). Children who enter school with social behavior problems, such as oppositional behavior and aggression, are at elevated risk for continued social difficulties throughout elementary school (Campbell & Ewing, 1990; Mesman, Bongers, & Koot, 2001) and for exhibiting antisocial behavior during adolescence (Loeber, 1990; Moffitt, 1993; Patterson, Reid, & Dishion, 1992). Attending to ways in which caregivers of young children in community settings can facilitate social competencies and prevent the development and escalation of such problems is essential.
Although a few studies have investigated longitudinal effects of early childhood intervention programs on social adjustment problems in youth, these studies have mainly been conducted in more formal preschool and center-based child care settings, such as the Perry Preschool Program (Schweinhart, Berrueta-Clement, Barnett, Epstein, & Weikart, 1985) and the Abecedarian Project (Campbell, Ramey, Pungello, Sparling, & Miller-Johnson, 2002). To develop a broader reach of these effective practices, it is important to intervene in additional forms of community settings in which young children spend a substantial amount of time.
Variable Quality of Child Care in Home Settings
About 3.7 million toddlers and preschool-age children in the United States spend an average of 26 hours per week in family child care settings (Mulligan, Brimhall, West, & Chapman, 2005). Compared to center-based care, the quality of care in family child care varies greatly (Goelman & Pence, 1990). Caregivers in family child care are likely to have lower levels of education and training compared to those providing center-based care (Howes & Hamilton, 1993) and the environments are less likely to be safe and designed for age-appropriate activities (Howes, 1983). Children from low-income families are more likely to attend family child care than center-based child care (Frankel, 1994; Hofferth, Shauman, Henke, & West, 1998), which may be due to availability and affordability. Unfortunately, it is the low-income children who are likely to attend the family child care settings with the lowest quality ratings (Goelman & Pence, 1990). Thus, the young children who are at risk of developing social and behavioral problems (Brooks-Gunn, Duncan, & Aber, 1997; Dodge, Pettit, & Bates, 1994) are the ones who are more likely to spend a substantial amount of time receiving low quality child care. Improvements in the quality of family child care, particularly in the ways in which social development is nurtured and child behaviors are managed, would likely have long-term positive influence on many at-risk children.
Purpose of This Study
The purpose of this study was to develop and evaluate the efficacy of Carescapes, a video-based training program to give family child care providers strategies in facilitating children’s social development, proactive approaches for managing children’s behavior, and ways to promote positive behavior in children who exhibit frequent challenging behaviors. Video-based instruction is particularly useful in disseminating effective behavioral intervention strategies in community settings because of its efficiency and potential for wide reach. Although empirically validated programs involving teacher training, parent training, and children’s social skills training exist, few applied settings have implemented them (Carnine, 1997; Kazdin, 1991). A key reason appears to be that there are practical obstacles for implementing programs that require substantial resources. Video-based programs can offer a more efficient and affordable format for providing quality training to child care providers.
In a prior study, an instructional video-based training module on ways to set up the child care home to promote social development was developed and evaluated (Rusby, Taylor, & Marquez, 2004). This training module was delivered to caregivers in an interactive 3-hour workshop session. The content included an overview of social development, importance of social skills, and typical social skills for preschool-age children, and also demonstrated ways to promote social development by a) arrangement of physical space, b) selection of materials and toys, and c) setting schedules and routines. Overall, caregivers reported that they learned new practical information, and promising trends in improvements of the child care environment and positive behavior in children were found.
In the present study, two more training modules were developed for the Carescapes program, one on proactive approaches for managing children’s behavior and the other on understanding and dealing with problem behavior. Each of the three training modules were provided to caregivers in interactive 3-hour workshop sessions. This small-scale efficacy trial is the first evaluation of all three modules using a randomized waitlist control design. Most interventions are first evaluated in efficacy studies carried out by the developers (Flay et al., 2005). In efficacy studies, interventions are carried out in optimal conditions with highly trained interventionists and ample resources. Subsequent, experimental effectiveness studies in which interventions are carried out in community settings (e.g., schools, clinics) under natural conditions of that setting are needed to provide evidence for empirical support (Chambless & Ollendick, 2001; Flay et al., 2005). This efficacy trial is the first step in the evaluation process.
The Carescapes program was primarily expected to improve the use of proactive behavior management practices, such as monitoring and providing clear expectations and positive attention. Increases in these practices were expected to reduce children’s problem behavior in the child care homes. Secondary hypotheses were that caregivers in the intervention group would make improvements in the child care environment and that children attending child care homes in the intervention group would exhibit increased social skills.
Method
Participants
Participants were drawn from the Oregon Child Care Resource and Referral Network agencies in two counties (total population approximately 640,000). Certified and registered family child care homes were considered eligible for participation. At the time of the study, in Oregon, caregivers with child care homes licensed as a registered child care home could have 3–10 children, and were required to have a) training in infant and child CPR and first aid, b) a food handlers permit, c) training on child abuse and neglect, d) an on-site health and safety inspection, and e) 8 hours of additional child care related training every 2 years. A certified child care home could have up to 12 children (or up to 16 with prior approval) and the facility was primarily educational for children 36 months old and older. In addition to the requirements for registered child care, the provider and assistants must have 15 hours of training related to child care every year. To be eligible for the study, at least two children who were 2½ to 6 years old needed to attend the child care home. Also, caregivers had to speak and understand English and could not have participated in a previous study that involved a portion of the intervention. There were 544 eligible care providers.
To increase minority participation, random stratified sampling of participants from each ethnic and race category was originally planned in the county that had this information in their database. The goal was to invite half the sample from minority populations, but since there were fewer minority caregivers than anticipated, all eligible minority caregivers from the county were invited to participate. In the other county, ethnicity and race information of the neighborhood schools was collected (Oregon Department of Education, http://www.ode.state.or.us/sfda/reportstudents.htm) and two thirds of the child care homes invited to participate in this study were randomly selected from 7 of the 36 neighborhoods with the greatest ethnic diversity (1 with the greatest Hispanic population and 2 neighborhoods each representing the greatest percentage of each racial category—African-American, Asian/Pacific Islander, and American Indian/Alaskan Native). One third of child care homes were randomly selected from the other neighborhoods in the county.
Caregivers were found inactive if they had moved out of the area, the phone had been disconnected without new contact information, or they had shut down or planned to shut down their child care soon. During the recruitment phase, 60 caregivers were found “inactive” and 23 were ineligible for participation. Out of 188 active and eligible child care homes selected, 22 (12%) did not respond after initial contact, 96 (51%) declined participation (primarily because they were too busy), and 70 (37%) agreed to participate. Based on U.S. Census data, the median household income of the neighborhoods in which the child care homes were located did not substantially differ between care providers who consented and those who did not consent to participate (the median household income was $39,937 for consenters’ neighborhoods and $39,140 for nonconsenters). Thus, the participating sample does not appear biased regarding the economic status of the neighborhoods in which they were located. By the end of the 2-year study, 57 caregivers remained in the study (81% retention).
Participants were offered $20 for filling out baseline questionnaires, $25 for filling out postintervention questionnaires, and $25 for each workshop attended. Participating caregivers were also provided with three credit hours per workshop toward their child care professional development. All the participants were female, 73% were Caucasian, 10% were Hispanic/Latino, 4% Asian or Hawaiian/Pacific Islander, 3% American Indian, 1% African-American, and 9% were of other or unknown ethnicity/race. Other demographic information on participating caregivers collected at baseline (such as caregiver age, education, years of experience, percent of homes with one or more than one caregiver, and number of children) is presented in Table 1. There were no significant differences between the intervention and waitlist control groups on these variables.
Table 1.
Participating Caregivers and Child Care Home Demographics
| Total Sample | Intervention | Waitlist Control | |
|---|---|---|---|
| Sample Size | 63 | 33 | 30 |
| Caregiver Age | |||
| 1. 18–21 years old | 0% | 0% | 0% |
| 2. 22–29 | 17% | 18% | 13% |
| 3. 30–39 | 32% | 30% | 36% |
| 4. 40–49 | 26% | 27% | 26% |
| 5. 50 and older | 25% | 24% | 26% |
| Mean | 3.59 | 3.55 | 3.63 |
| Caregiver Education | |||
| 1. High school or GED | 29% | 33% | 22% |
| 2. Some college | 43% | 36% | 52% |
| 3. AA degree | 6% | 3% | 10% |
| 4. BA/BS | 14% | 18% | 10% |
| 5. Some graduate school | 8% | 9% | 6% |
| Mean | 2.26 | 2.35 | 2.15 |
| Total number of adults providing care | |||
| 1. One | 73% | 74% | 70% |
| 2. More than one | 27% | 26% | 30% |
| Mean | 1.28 | 1.26 | 1.30 |
| Mean years of experience | 9.3 | 9.5 | 8.9 |
| Mean total number of children | 8.7 | 8.7 | 8.7 |
Note. All mean differences between intervention and waitlist control groups were not statistically significant.
Individual children were not participants in this study. Parents were informed about the evaluation study and the site visit assessments of the child care home, ways in which the child care provider promotes social development, and overall, what children do.
Research Design and Procedures
Baseline questionnaires completed by the primary caregiver were collected prior to randomization of child care providers into intervention and waitlist control conditions. In cases where there were more than one caregiver, the caregiver who provided the most care to children was considered the “primary” caregiver who participated in the study. All caregivers at each child care home (not just the “primary”) were invited to the intervention or waitlist workshops. Approximately 1 month after the intervention group participated in the last of three workshops, all participating caregivers completed the questionnaire again (post).
Assessments also involved three site visits per phase in which research assistants conducted observations and completed ratings of caregiver practices and overall child behavior. On average the three assessment times within each phase (pre and post) were about 9 weeks apart (Figure 1 shows the design and assessment timeline). The collection of postdata began 4 weeks after the intervention group completed the third workshop, so the last assessment data point (T6) occurred an average of 22 weeks (or about 5 months) post intervention. During the first presite visit (T1) and the first postsite visit (T4) assessors completed a rating on the child care environment of each child care home. Random reliability checks were assigned on 18% of the site visits, in which two research assistants visited the site to collect observation data. By baseline data collection, 65 caregivers continued participation in the study and 100% completed the baseline questionnaires. The first site visit assessments were completed on 98% of participating child care homes in baseline, the second on 94%, and the third on 92%. By the end of the baseline observation phase, 63 caregivers were participating (two caregivers dropped out of the study because they were closing down their child care business).
Figure 1.

Design and assessment timing. Caregiver questionnaire and Childcare Ecology Checklist was collected at T1 and T4.
After the preintervention assessment data were collected, family child care sites were randomly assigned to participate in the intervention workshops immediately or after completion of the posttest assessments (33 child care homes were assigned to immediate intervention and 30 to waitlist control condition). Random assignment to condition controls for causally relevant variables (Rubin, 1974) and reduces the likelihood that something other than the intervention would account for observed differences between conditions at the conclusion of the study. The intervention workshops were about 2 weeks apart. After each workshop, participating caregivers filled out a feedback form on the usefulness of the workshop and barriers to implementation of the practices learned. The beginning of the postdata collection began about 1 month after the third intervention workshop.
Intervention
The development of the Carescapes intervention content was drawn from research from the early intervention field and included studies in preschools and child care. The research base for the content of each intervention module is described below.
Module 1: Setting up to support social development
This training module demonstrated how to enrich the child care experience by organizing the child care space into activity areas, providing a variety of toys and materials, and offering a variety of activities that promote positive social interactions and socially skilled behavior. This training module also showed how to effectively lead children through transitions between activities. Having an enriched and organized child care environment is critical for promoting social engagement and preventing problem behavior (Hilton, 1987; McEvoy, Fox, & Rosenberg, 1991; Nordquist & Twardosz, 1990; Twardosz & Risley, 1982) and helps prepare children for school (Love et al., 2003). When caregivers plan and organize experiences and routines that are manageable and predictable for young children, the emotional demands of the daily experiences are reduced, enabling the child to focus on learning new skills (National Research Council & Institute of Medicine, 2002), including important social skills. Greater details about the content and research base for this module is reported in Rusby et al. (2004).
Module 2: Proactive approaches for managing children’s behavior
The content of the second training module focused on proactive behavior management practices. This module included (a) building a positive relationship with children, (b) developing and teaching clear rules and expectations, (c) getting and maintaining children’s attention, (d) providing clear directions before an activity begins, (e) monitoring, and (f) providing positive attention and encouragement. Although much of the research demonstrating positive effects of these behavior management practices has occurred in school settings (e.g., Hawkins, von Cleve, & Catalano, 1991; Nafpaktitis, Mayer, & Butterworth, 1985; Walker, Schwarz, Nippold, & Irvin, 1994), the research in child care and preschool settings has consistently matched the findings (e.g., Dunn, 1993; Howes, Phillips, & Whitebook, 1992; Webster-Stratton, Reid, & Hammond, 2001).
Module 3: Understanding and dealing with problem behavior
The content of the third training module focused on ways to deal with ongoing behavioral challenges. The module described and provided examples of (a) the coercive process, (b) effective strategies for dealing with challenging behavior, (c) understanding the function of recurring problem behavior, and (d) building a support plan for individual children who display ongoing behavioral challenges. It is expected that even with the environmental and proactive practices in place, a small proportion of children will continue to exhibit challenging behavior. Research in school settings indicates that students who exhibit elevated rates of problem behavior need a more individualized approach for intervening (Sprague, Sugai, & Walker, 1998). This module demonstrates appropriate consequences (promoting use of the least intrusive strategy) for varying challenging behaviors. It also offers a Behavior Support Guide, which helps child care providers understand the function of a child’s challenging behaviors and guides them through the development of a plan for teaching and supporting positive replacement behaviors. This module is based on functional behavior assessment and support—an individualized approach for clearly defining the problem behaviors, defining when and in what situation the problem behaviors tend to occur, and analyzing the contextual factors that maintain those behaviors (O’Neill et al., 1997). Experimental evaluations have shown that behavior support plans based on functional behavior assessment in school settings result in decreased aggressive and disruptive behaviors among a variety of children with behavior problems (Carr & Durand, 1985; Lalli, Browder, Mace, & Brown, 1993; Taylor & Romanczyk, 1994). Although developed in work with children with developmental disabilities, the approach has been shown to be effective with students with average to above-average intelligence with behavioral problems (Broussard & Northrup, 1995; Dunlap et al., 1993; Kern, Childs, Dunlap, Clarke, & Falk, 1994; Lewis & Sugai, 1996), with socially withdrawn behaviors (Lewis & Sugai, 1993), and with attention deficit hyperactivity disorder (Northrup et al., 1995; Umbreit, 1995).
Intervention development
Evidence supports that video-based modeling approaches can be both effective and efficient for training parents, teachers, and child care providers (Aguirre & Marshall, 1988; Taylor, Schmidt, Pepler, & Hodgins, 1998; Webster-Stratton, Hollinsworth, & Kolpacoff, 1989; Webster-Stratton et al., 2001). The video presentation was designed to feature “real-life” demonstrations of examples in family child care settings. Documentary footage was gathered from numerous family child care sites to provide diversity, and scripted vignettes were used whenever specific examples or negative examples were needed. The video and manual were designed for interactive use, providing a number of breaks for interactive opportunities (a viewer pauses the tape to complete an activity described in the manual). Feedback was provided on the drafts of the scripts and practice activities for each intervention module in separate focus groups of seven to eight family child care providers (59% Caucasian, 14% Hispanic/Latino, 18% Asian or Hawaiian/Pacific Islander, and 9% African-American). The feedback from focus groups was incorporated and then materials were reviewed by expert consultants. Four of the consultants had Ph.D.’s and were faculty or researchers with expertise in early intervention, child care environments, proactive management practices, functional behavior assessment and support, family interventions, and/or video-based training programs. One consultant was the co-director of the local Child Care Resource and Referral Network and had experience in training and resource development for child care providers. Based on consultant feedback the video script, manual, handouts, and child activities were finalized and the script provided a blueprint for the production of the video.
Intervention procedures and participation
Caregivers in the immediate intervention group were invited to participate in the set of three 3-hour workshops that were scheduled about 2 weeks apart. Caregivers were given a choice of whether they would like to attend the workshops on a weekday evening or a Saturday morning. Workshops were conducted in the caregivers’ local county Child Care Resource Referral agency or research institute meeting rooms and were provided by the program developer, the research scientist who was the Principal Investigator of this study. Caregivers who missed a given workshop were invited to attend the workshop on the alternative day in their community or to view the video and do the practice activities in the manual at home before the next workshop session. For caregivers who did a module through home study, the interventionist checked their activity work in their manual, answered questions, and checked for understanding of the content at the next workshop. Good participation rates were achieved—90% of the caregivers were exposed to module 1 (71% attended the workshop and 19% completed the home study), 90% received module 2 (81% attended the workshop and 9% did home study), and 87% received module 3 (80% attended the workshop and 7% did home study). A total of 97% of the caregivers in the intervention group received some exposure to the intervention and 90% received at least two modules of content.
Measures
Many studies on evaluating the effects of child care interventions have utilized global outcome measures of child care quality. Reviews of existing research suggest that several important dimensions of child care quality are not being adequately measured (Friedman & Amadeo, 1999; Lamb, 2000). Studies using more global measures of child care quality have had mixed results in predicting children’s developmental outcomes, particularly in the social domain. Indeed, some researchers hypothesize that divergent research results regarding the impact of child care quality are due, at least in part, to differences and inadequacies in measurement of child care quality (Hagekull & Bohlin, 1995; Lamb, 2006). We have therefore avoided using global measures of child care quality for this study, and have selected multiple assessment methodologies that specifically measure empirically supported child care environmental features and caregiver practices and that measure specific targets of the intervention content.
Measures for this study include caregiver questionnaires, ratings of the child care environment, and observations of caregiver practices and the overall behavior of preschool age children in the child care. Table 2 displays the items and reliability alphas for each composite score of caregiver reports and of observer ratings used in the present study.
Table 2.
Items and Reliability Alphas for Each Composite Measure
| Cronbach’s Alpha | ||
|---|---|---|
| Measure and items | Baseline | Post |
| Caregiver Report of Proactive Behavior Management | .79 | .65 |
| Taught or reminded children of rules | ||
| Prepared children for transitions | ||
| Taught social skills to children | ||
| Praised children for good behavior | ||
| Gave clear positive directions | ||
| CCEC: Enriched Environment | .91 | .89 |
| Activity areas are designed to promote social interaction | ||
| Toys and materials match children’s developmental level | ||
| Materials encourage children to engage in a variety of play | ||
| Variety of materials encourage cooperative and social play | ||
| Adequate amount of materials provided | ||
| Children are actively engaged with materials in all play areas | ||
| CCEC: Organized Environment | .88 | .90 |
| Physical space promotes intended activities | ||
| There are clearly defined activity areas | ||
| Compatible activity areas are next to each other | ||
| Materials are organized in a way so children can put them away | ||
| CCEC: Planned Activities and Schedule | .85 | .86 |
| Activities are planned ahead of time | ||
| Materials are prepared ahead of time | ||
| Children are playing throughout the child care home (reversed) | ||
| There is a sequence of activities, a schedule is followed | ||
| There is a balance of structured and unstructured activities | ||
| There is a balance of active and calm activities | ||
| CCEC: Monitoring | .82 | .84 |
| Activity areas defined by low boundaries, children are visible | ||
| Caregiver circulates through child care and/or area | ||
| Caregiver scans entire play area at least once per minute | ||
| Caregiver maintains proximity to children needing assistance | ||
| Observer Rating of Caregivers’ Effective Behavior Management | .85 | .86 |
| Supportive of children’s efforts | ||
| Encourages active participation | ||
| Intrusiveness (reversed) | ||
| Clear instructions or directions | ||
| Prepared children for transitions | ||
| Made unreasonable requests (reversed) | ||
| Monitored children | ||
| Gave reminders of expected behavior | ||
| Had good control or influence on children | ||
| Modeled positive behaviors | ||
| Problem solved with children | ||
| Was positive and reinforcing toward children | ||
| Consistent rules and consequences | ||
| Had little or no influence over children | ||
| Observer Ratings of Children’s Positive Behavior | .95 | .85 |
| Level of children’s compliance | ||
| Handled transitions well | ||
| Followed rules and expectations | ||
| Level of children’s cooperation | ||
| Engaged in problem solving | ||
| Expressed feelings appropriately | ||
| Level of interest, enthusiasm, and involvement | ||
| Level of focus and engagement | ||
Child Care Provider Survey
Caregivers filled out a questionnaire at baseline and postintervention on the strategies they have used to promote child development and to manage children’s behavior in their child care and the usefulness of those strategies, including the enrichment of the environment, planned activities, and their behavior management practices. A composite score of the caregivers’ self-report of proactive behavior management practices was computed by taking an average of items (see Table 2 for items and reliability alpha). This survey also included items on the caregiver’s perceptions of the density of problem behavior in the child care setting. Demographic information was also included in the survey, such as caregiver experience and education, child–adult ratio, and age range of children. This survey was developed and used in the preliminary study (phase 1) on family child care providers (Rusby et al., 2004) and includes salient demographic and provider strategies presented in the literature cited above.
Direct observations of caregiver practices and child problem behaviors
Direct observations of the child care providers’ behavior management practices and of overall child problem behavior occurred during three separate visits at baseline and post intervention. The observations of child behavior involved tallying all behaviors exhibited during the observation period by any of the children in the child care home. On each visit, caregiver and children’s behavior were observed for 20 minutes during free play, when the children tend to be more active. Observers were masked regarding the intervention condition of the child care site. The Assessing School Settings: Interactions of Students and Teachers (ASSIST; Rusby, Taylor, & Milchak, 2001) observation frequency coding system was adapted for use in child care settings. For this study, child care providers’ frequency of approvals (positive attention for children’s behavior) and criticisms per minute were calculated as well as a ratio of approvals to criticisms for each measurement time point. Interrater reliability was computed using a one-way random effects intraclass correlation coefficient (ICC; McGraw & Wong, 1996; Shrout & Fleiss, 1979). Good interrater reliability was achieved—the ICC for approval was .94 at baseline and .95 at postdata collection and for criticism was .86 at baseline and .91 at post. The approval-to-criticism ratio was significantly associated with observed fewer problem behaviors and more positive behaviors at baseline (see Table 3).
Table 3.
Correlations Between Child Care Constructs and Children’s Behavior at Baseline
| Problem Behavior2 | Positive Behavior3 | |
|---|---|---|
| Enriched Environment1 | −.14 | .48*** |
| Organized Environment1 | −.12 | .40*** |
| Planfulness1 | −.22 | .49*** |
| Monitoring1 | .00 | .27* |
| Approval:Criticism2 | −.28* | .46*** |
| Effective Behavior Management3 | −.41*** | .82*** |
Child Care Ecology Checklist.
Observation.
Obs Rating.
p < .05
p < .001.
During the three visits to each of the child care sites at baseline and at post test, project staff also observed the overall problem behavior of preschool-aged children at the child care. Observers tallied the rates of noncompliance, physical aggression, and potentially dangerous behavior that children exhibited during a 20-minute observation. Noncompliance was coded whenever a child did not follow a caregiver’s directive for a behavior change (to either start doing something or to stop doing something; for example, if the caregiver says it is time to put away the toys and a child continues to play with blocks). Physical aggression was coded for whenever a child engaged in aversive physical contact with another person; for example, when a child hit, pushed, or grabbed a toy away from another child. Potentially dangerous behavior was coded for behavior that was potentially dangerous to self or another child and for misuse of equipment. Examples include throwing a toy against the wall, running down the slide, rough and tumble play such as play wrestling, misuse of playground equipment. A composite score for problem behavior rates per minute was created by summing the counts of each of these observed behaviors and then dividing by the total minutes observed. The ICC reliability for the problem behavior composite was .90 at baseline and .94 at post. Finally, although the number of children in the child care home might influence the rate of problem behavior, a preliminary analysis found this not to be the case. The number of children in child care and the rates of problem behavior were not significantly associated. Therefore, it was not necessary to account for the number of children when calculating the rate of problem behavior score.
Observer ratings of effective behavior management and children’s positive behavior
During the three visits to each of the child care sites at baseline and at post test, project staff also completed an observer rating of their global impressions of caregiver practices for facilitating social development and managing behavior and of the children’s positive behavior. The observer ratings of caregivers behavior management practices were rated on a 5-point scale: 1 = “did not occur,” 2 = “occurred once,” 3 = “occurred 2 to 3 times,” 4 = “occurred multiple times (> 3),” and 5 = “constantly occurred.” Items were adapted from the coder impression inventory on preschool teacher behavior management skills (Webster-Stratton et al., 2001) which were originally derived from the Oregon Youth Study observer impressions of parent monitoring and discipline (Capaldi & Patterson, 1989). See Table 2 for items and reliability alpha for the present study. The items for the measures of overall child positive behavior were derived from the Classroom Atmosphere Rating Scale (Greenberg & Wehby, 1995) and were previously adapted for use in family child care settings (Rusby et al., 2004). These items were rated by the observer on a 5-point Likert scale, from 1 “very low” to 5 “very high”; see Table 2 for items and reliability. Significant associations were found between effective behavior management practices and fewer observed problem behaviors and more positive behaviors at baseline (see Table 3).
Child Care Ecology Checklist
Project staff completed the Child Care Ecology Checklist (CCEC) at each site, once before and once after intervention. Assessment staff observed the child care and provided ratings on the (a) physical space, (b) materials, (c) scheduling, (d) planning, (e) teaching routines and expectations, (f) monitoring, and (g) managing attention, each on a 4-point scale. The CCEC was adapted from the Early Childhood Classroom Ecology Checklist (Project STAR, 2002; Kaminski & Stormshak, 2006). Items included on this measure are based on the literature on effective practices in preschool and child care settings, and thus align with the practices promoted in the intervention described previously. This measure has been a useful consultation tool in Head Start classrooms (Kaminski & Stormshak, 2006; Yoshikawa & Knitzer, 1997). Good item correlations and adequate interrater reliability were found for a priori composites from this measure: organized environment, enriched environment, and planned activities; and the measure of toy variety, a subset of enriched environment, was sensitive to intervention (Rusby et al., 2004). Items and reliability alpha for the organized environment, enriched environment, planned activities/schedule, and monitoring composites used in the present study are in Table 2. These child care setting composite scores were positively associated with observer ratings of children’s positive behavior at baseline (see Table 3).
Caregiver Interaction Scale (CIS; Arnett, 1989)
During the three child care site visits at baseline and at post test, research staff also completed the Caregiver Interaction Scale. The CIS measures caregiver sensitivity and involvement. Arnett (1989) described four factors: positive interaction, punitiveness, permissiveness, and detachment; items on each factor had a minimum loading of .49. Other researchers have combined some of these factors into a caregiver sensitivity score (de Kruif, McWilliam, Ridley, & Wakely, 2000). The CIS predicted children’s secure attachment to their child care provider (Galinsky, Howes, Kontos, & Shimm, 1994). For this sample of family child care providers at baseline, alphas for the factors of the CIS ranged from .75 to .89.
Caregiver ratings of program usefulness
Following each workshop session, caregivers provided a report of their satisfaction with the workshop and materials and also were asked to identify any barriers they expected to find in trying to implement changes in the family child care environment and in their behavior management practices to facilitate social development. A fourth satisfaction questionnaire was mailed to caregivers in the intervention group about a month following the set of workshops to assess their continued satisfaction and whether they actually made changes in their child care based on the training. These caregiver satisfaction reports have been used to provide a summary of whether family child care providers learned new information, gained practical skills, and planned to make changes in their child care based on a workshop on promoting social development (Rusby et al., 2004).
Knowledge test on the Behavior Support Guide
This knowledge test was developed to assess whether caregivers understood the concepts about the function of problem behavior and developing effective behavior support plans presented in the third workshop module. During the workshop, caregivers completed a sample Behavior Support Guide based on a video example of a child’s problem behavior in a home child care setting. These were scored for how well each caregiver defined the problem behavior and its function, and developed a support plan.
Analytical Procedures
For data collected once before and once after intervention (i.e., the caregiver reports and the CCEC), a multivariate analysis of variance was conducted to identify effects by condition (intervention vs. waitlist control), time (baseline vs. post), and interaction between group and time (Cohen, Cohen, West, & Aiken, 2003). For data collected three times in each phase—three assessments before intervention and three assessments after intervention, including direct observations, observer ratings, and CIS—a longitudinal, random coefficients analysis (RCA) was conducted. This analysis is also called a growth model or multilevel model for change (Fitzmaurice, Laird, & Ware, 2004; Nich & Carroll, 1997; Singer & Willett, 2003). The RCA provides a more rigorous treatment for the analysis of repeated measures data than traditional methods (Fitzmaurice et al., 2004; Gueorguieva & Krystal, 2004; Nich & Carroll, 1997). RCA properly accounts for autocorrelation among repeated assessments of the same participant and, in this study, employed maximum likelihood estimation, which allowed for the use of all available data from all assessments. Such an analysis supplies unbiased results even in the face of substantial attrition, provided any missing data were missing at random (Laird, 1988; Shafer & Graham, 2002). In the present study, attrition or other missing data did not appear to represent a meaningful departure from the missing-at-random assumption, meaning that missing data were not likely to depend on unobserved determinants of the outcome of interest (Little & Rubin, 2002).
We fit models to our data with SAS PROC MIXED 9.1 (SAS Institute, 2004) using the restricted maximum likelihood method (REML) generally recommended for multilevel models (Hox 2002; Verbeke & Molenberghs 2000). Variance parameter estimates were not constrained to values at or above zero, and MIXED provided negative variance estimates for some models. Negative variances often result from computational limitations for estimates very near zero and do not represent problems with the models or analysis procedures (Kreft & de Leeuw, 1998; Singer & Willett 2003). Forcing non-negative estimates can lead to depressed Type I error rates and reduced statistical power in some situations (Murray, Hannan, & Baker, 1996). Finally, RCA models estimated with maximum likelihood procedures are relatively robust to violations of normality (Fitzmaurice et al., 2004; Maas & Hox, 2004).
Unlike standard regression software, PROC MIXED provides no standardized beta estimates. This effect-size formula transforms the t-value and degrees of freedom from a statistical test into a correlation coefficient (Rosenthal, Rosnow, & Rubin, 2000; Rosenthal & Rubin, 2003). In simple models with one outcome and one predictor, this provides an effect-size estimate interpreted just like the usual Pearson correlation coefficient. When squared, it gives the proportion of overlapping variance or variance explained and equals a usual R2 statistic. In standard regression models with multiple predictors or covariates, the r-value computed from this formula equals the partial correlation coefficient, which gives the magnitude of the relationship between two variables controlling for all other variables in the model.
The RCA approach also offers considerable flexibility (Fitzmaurice et al., 2004; Singer & Willett, 2003). A basic model, for example, would estimate an intercept or level and a slope for all participants. A more sophisticated model estimates separate intercepts and slopes by condition across the three pretest time points, change in level for intervention participants at the first postintervention time point, and change in slope for intervention participants across the three postintervention time points. Although this latter model was appropriate for the data collected, it was first compared to a somewhat simpler model to determine the best representation of the data. That is, before comparing conditions for each outcome measure, models that included the same preintervention intercepts and slopes for both intervention and waitlist control conditions were compared with models that fit separate preintervention slopes for intervention and waitlist control conditions. This comparison provided, essentially, a more sophisticated test of pretest differences than typically conducted, as it allowed for a comparison of both intercepts and slopes before the introduction of the intervention. The best fitting model was selected using the Akaike Information Criterion (AIC), an index of the relative fit of competing models to the same data (Akaike, 1974; Burnham & Anderson, 2002). Built upon the principle of Occam’s razor, the AIC leads to the selection of a more generalizable final model than does the reliance of significance tests of individual parameter estimates (Myung, 2000; Zucchini, 2000). Lower AIC values indicate greater empirical support, given the number of parameters estimated and the underlying data. For each of the outcome measures presented, the model that estimated the same preintervention intercept and slope across conditions fit the data best.
The final analysis provided estimates of (a) normative intercept or level at the first time point for all participants, (b) normative slope across the three pretest time points for intervention participants and all time points for waitlist control participants, (c) change in level for intervention participants at the first postintervention time point, and (d) change in slope for intervention participants across the three postintervention time points (Fitzmaurice et al., 2004). The change in level and slope represents differences from those expected from normative growth, which was estimated from waitlist control condition participants across all assessments and treatment condition participants from their preintervention assessments. These change parameters represent the hypotheses of interest, that is, the immediate and longer-term effects of intervention on each outcome measure.
Due to the relatively small sample, power to detect effects was low. Although power calculations for the model tested are very complicated, power for a simpler analysis of covariance, with a pretest covariate of r = .50, should provide a reasonable estimate, if not a slight underestimate (Muthén & Curran, 1997; Venter, Maxwell, & Bolig, 2002). Such an analysis has power of .64 to detect a medium effect of condition (d = .50; Cohen, 1988) at the .05 level. To balance the likelihood of Type I errors with the chance of Type II errors, Cohen (1990) and Rosnow and Rosenthal (1989) recommend an adjustment to alpha, the Type I error rate. Thus, results with p < .10 are interpreted, which increases power to .75. Furthermore, effect sizes for tests of condition are also presented to aid interpretation. An effect size equivalent to Cohen’s d (Cohen, 1988; Rosenthal & Rubin, 2003) was computed, which represents the proportion of the pooled standard deviation accounted for by the parameter estimate.
Effects on caregiver outcomes were expected to mediate child outcomes. For example, we hypothesized that the intervention would have effects on the child care environment and caregiver practices which would then lead to improvements in child behavior and promote positive social interactions among children. Thus, when significant intervention effects were found for measures of children’s behavior and for measures of caregivers’ practices, mediation models were tested to determine whether the change in caregivers’ practices were functionally related to the changes in children’s behavior (Baron & Kenny, 1986; Judd & Kenny, 1981). Demonstration of mediation requires three steps. First, changes in child outcomes must be associated with intervention condition. Second, the intervention must be shown to predict changes in caregiver practices. Third, the measure of caregiver practices are added into the model that tests the condition on child outcomes. In this third step, caregiver practices should “explain” the condition effect on child outcomes. That is, caregiver practices are expected to predict child outcomes and the condition effect is expected to decrease or disappear. Mediator effects with intervention exposure were also tested, as well as moderator effects for years of experience providing child care, using procedures suggested by Jaccard and Turrisi (2003). Hours of intervention exposure were calculated (3 hours for each workshop attended and 2 hours for each home study completed), ranging from 0 hours (no exposure) to 9 hours.
Results
Feedback from Child Care Providers on Satisfaction and Barriers to Implementation
A large majority of the child care providers reported that the Carescapes workshops were useful (see Table 4). For modules 1 and 2, 90% of the caregivers said that they learned “some” to “very many” new things and practical skills. For module 3, 100% of the caregivers said that they learned “some” to “very many” new things and practical skills. A large majority of caregivers reported that they planned to make “some” to “very many” new changes or try new things based on the workshops (86% for module 1, 82% for module 2, and 92% for module 3). Barriers to implementation were reported mostly for making changes in the child care environment (module 1)—30% said that changes would cost too much, 20% said that they did not have enough time, and 17% said that their place was too small. Only one caregiver reported that no changes or improvements were needed in her child care home. Time was a barrier for at least 10% of the caregivers for each of the modules. No caregivers reported needing more information before they could implement the practices presented in modules 1 and 2. Only 7% of the caregivers reported needing more information on dealing with challenging behaviors (module 3). The average score on the knowledge test on the Behavior Support Guide from module 3 was 80% (the median was 83% and range was 46% to 96%). Only one caregiver scored below 60% and four scored between 60% and 70%.
Table 4.
Caregiver Feedback on Program Usefulness
| Feedback questions for each workshop | Percent of Caregivers’ Responses | |||
|---|---|---|---|---|
| Workshop 1: Setting up to Support Social Development | Nothing new | A few new things | Some new things | Many or very many new things |
| How much did you learn? | 3% | 7% | 52% | 38% |
| How many practical skills did you gain? | 0% | 10% | 62% | 24% |
| Do you plan to make changes or try new things based on this workshop? | 0% | 14% | 62% | 24% |
|
| ||||
| Workshop 2: Approaches for Guiding Children’s Behavior | ||||
| How much did you learn? | 0% | 10% | 38% | 52% |
| How many practical skills did you gain? | 0% | 10% | 34% | 52% |
| Do you plan to make changes or try new things based on this workshop? | 0% | 17% | 41% | 41% |
|
| ||||
| Workshop 3: Understanding and Dealing with Challenging Behavior | ||||
| How much did you learn? | 0% | 0% | 15% | 85% |
| How many practical skills did you gain? | 0% | 0% | 35% | 65% |
| Do you plan to make changes or try new things based on this workshop? | 0% | 8% | 46% | 46% |
Note. Thirty caregivers in the intervention group provided program usefulness data.
Intervention Outcomes
Outcomes for observed caregiver practices
Random coefficients analyses were performed on observed caregiver approvals and criticisms, observer ratings of caregiver use of effective management practices, and on the CIS. No significant outcomes were found for observed rate of criticisms or for the approval-to-criticism ratio. A medium effect was found for increased rates of approvals in the intervention group (intercept t = 1.77, p = .081, d = .45). Rates of approval especially increased at immediate post (T4); however, decreases in slope for approvals were greater at post (T4–T6) for the intervention group compared to the waitlist control (slope t = −1.68, p = .094) as shown in Figure 2. Initial increases in caregiver’s use of approval were found for the intervention group, but over time approvals decreased at a greater rate for the intervention group than for the waitlist control group. Parameter estimates for the RCA for caregiver approval and effective behavior management are provided in Table 5. Significant improvements were found in caregivers’ effective behavior management for the intervention group (intercept t = 2.82, p = .006). The level-change represents a medium-to-large effect size (partial r = .34, d = .72; Rosenthal & Rubin, 2003). The intervention and control group slopes at post did not significantly differ (see Figure 3). Caregivers in the intervention group increased their use of effective behavior management practices compared to those in the waitlist control group and the rate of change in use of effective behavior management practices across the three postdata timepoints did not differ for the intervention and control groups.
Figure 2.

RCA for observed caregiver rates of approval.
Table 5.
Estimates from the Random Coefficients Analyses for Caregiver Approval, Caregiver Effective Behavior Management, and Child Problem Behavior
| Effect or statistic | Caregiver Approval | Caregiver Effective Behavior Management | Child Problem Behavior | |
|---|---|---|---|---|
| Fixed effects | Intercept | .339*** (.033) | 3.602*** (.056) | .138*** (.024) |
| Slope | −.008 (.009) | −.042** (.015) | .026* (.011) | |
| Condition × posttest intercept | .093* (.053) | .220** (.078) | −.130* (.052) | |
| Condition × posttest slope | −.061* (.036) | −.078 (.052) | .045 (.037) | |
| Variance components | Residual | .0631 | .1249 | .0593 |
| Intercept | .0346 | .1246 | .0008 | |
| Slope | −.0007 | −.0005 | .0008 |
Note: Entries for fixed effects include parameter estimates with standard errors in parentheses. To compute t-values, divide the estimate by the standard error; t-values may differ from text due to rounding.
p < .10.
p < .01.
p < .001.
Figure 3.

RCA for caregiver effective behavior management.
Outcomes for caregiver reports of their practices and of child behavior
Pre–post increases in self-reported improvements in environmental enrichment (physical layout and toy variety) were found in both the intervention and control groups (p = .011), yet no significant differences between the groups were found. No significant findings occurred for self-reported planfulness. A significant group-by-time interaction was found for self-reported proactive behavior management practices; the waitlist control group reported increased use of proactive practices, whereas the intervention group reported decreased use.
Outcomes on Child Care Ecology and Caregiver Interaction Scale
No significant pre-post differences were found between the intervention and waitlist control groups on the CCEC scores for organized environment, enriched environment, or planned activities (see Table 6). Monitoring was found to decrease in both groups over time; however, the decrease was smaller for the intervention group (p = .087) and a medium effect size was found for this difference (Cohen’s d = .51; Cohen, 1988). No significant outcomes were found for the CIS factors.
Table 6.
Multivariate Analysis of Variance to Identify Pre–Post Changes by Group
| Construct | Waitlist Control Group | Intervention Group | Analysis of Variance | ||||
|---|---|---|---|---|---|---|---|
| Baseline M (SD) | Posttest M (SD) | Baseline M (SD) | Posttest M (SD) | F | p | ||
| Child Care Ecology Checklist | |||||||
| Group | 0.08 | .78 | |||||
| Organized Environment | 1.70 (.70) | 1.71 (.65) | 1.68 (.73) | 1.83 (.80) | Time | 0.56 | .46 |
| G X T | 0.43 | .52 | |||||
| Group | 0.77 | .38 | |||||
| Enriched Environment | 2.05 (.65) | 2.14 (.63) | 2.12 (.72) | 2.33 (.56) | Time | 2.66 | .11 |
| G X T | 0.41 | .53 | |||||
| Group | 0.17 | .69 | |||||
| Planfulness | 2.25 (.48) | 2.08 (.57) | 2.10 (.72) | 2.12 (.67) | Time | 0.63 | .43 |
| G X T | 0.85 | .36 | |||||
| Group | 0.04 | .85 | |||||
| Monitoring | 2.30 (.41) | 1.96 (.56) | 2.14 (.53) | 2.08 (.62) | Time | 6.11* | .02 |
| G X T | 3.06 | .09 | |||||
| Caregiver Report | |||||||
| Group | 1.81 | .18 | |||||
| Enriched Environment | 2.11 (1.02) | 2.25 (1.07) | 2.30 (.81) | 2.72 (1.05) | Time | 6.98* | .01 |
| G X T | 1.73 | .19 | |||||
| Group | 0.75 | .39 | |||||
| Planfulness | 3.58 (1.59) | 3.77 (1.42) | 3.85 (.91) | 4.03 (.78) | Time | 1.71 | .20 |
| G X T | 0.01 | .95 | |||||
| Group | 0.17 | .68 | |||||
| Proactive Behavior Management | 6.01 (.81) | 6.23 (.47) | 6.32 (.43) | 6.04 (.84) | Time | 0.10 | .75 |
| G X T | 5.31* | .03 | |||||
| Group | 0.15 | .70 | |||||
| Children’s Problem Behavior | 3.40 (1.35) | 3.42 (1.61) | 3.48 (1.37) | 3.07 (1.48) | Time | 0.94 | .34 |
| G X T | 1.09 | .30 | |||||
Note. G X T = group-by-time interaction.
p < .05.
Because monitoring decreased over time, we conducted post hoc analyses and determined that a greater proportion of observations took place outdoors at baseline (43%) compared to posttest (14%; χ2 = 35.26, p < .001). The change in observation settings across time, however, did not differ by condition. We also tested whether monitoring depended on the setting and found no significant differences in monitoring between outdoor and indoor observations.
Outcomes for observed overall child behavior
Random coefficients analyses were conducted on observed children’s problem behavior and on observer ratings of children’s positive behavior. Overall, the rate of child problem behavior increased across time (t = 2.30, p = .022). Figure 4 shows this in the line for the control group across all six data points and in the first three data points for the intervention group. The children in the intervention child care homes showed a decreased level of problem behavior immediately after the intervention (t = −2.48, p = .016). This change in the level of problem behavior just after intervention represents a medium-to-large effect size (partial r = −.30, d = .63). The difference in the slopes after the intervention was not statistically significant between the intervention and control groups. In other words, the rates of change in problem behaviors following the intervention did not differ. RCA parameter estimates for child problem behavior are shown in Table 5. No significant outcomes were found for observer ratings of children’s positive behavior.
Figure 4.

RCA for children’s problem behavior.
The rate of problem behavior was not related to the number of children in the child care home, and therefore the calculation of the rate did not account for the number of children. The number of children in each child care site could nonetheless moderate differences in the impact of the intervention. To test for moderation, we added the number of children in child care and its interaction with condition into the random coefficients model of the rate of child problem behavior. Neither term was statistically significant. The number of children in the child care home did not impact the intervention outcomes found for overall children’s problem behavior.
Mediation model of caregiver effective management and children’s problem behavior
To test whether the change in caregivers’ practices due to intervention was functionally related to the changes in children’s behavior, we tested a mediation model (Baron & Kenny, 1986; Judd & Kenny, 1981; MacKinnon, Lockwood, Hoffman, West, & Sheets, 2002), shown in Figure 5. Two of the three steps to demonstrate mediation were shown previously: the intervention produced differences between conditions in caregivers’ effective behavior management (path a in Figure 5) and children’s problem behavior (path c). In the third step, we tested whether caregivers’ effective behavior management predicted children’s problem behavior (path b) and simultaneously reduced the condition effect on children’s problem behavior (path c’). Caregivers’ effective behavior management explained a significant portion of the intervention effect on children’s problem behavior (t = −6.38, p < .001). The effect size for this mediation effect was medium (partial r = −.37). The mediation model, with caregivers’ effective behavior management predicting children’s problem behavior, produced a decrease in the direct effect of condition onto children’s problem behavior from d = .63 (t = −2.48, p = .016) to d = .48 (t = −1.89, p = .064). The causal steps alone, however, are insufficient to demonstrate mediation (MacKinnon et al., 2002). A test of the product of paths a and b, a b, however, demonstration of mediation (MacKinnon et al., 2002; Sobel, 1982), and has been shown equivalent to a test of the reduction in effect of condition on the outcome, c – c’ (MacKinnon, Warsi, & Dwyer, 1995). This test was statistically significant (t = −2.58, p = .012). Thus, although caregivers’ effective behavior management did not completely reduce the effect of condition on children’s problem behavior, it did account for some of the statistically significant reduction in problem behavior associated with the intervention.
Figure 5.
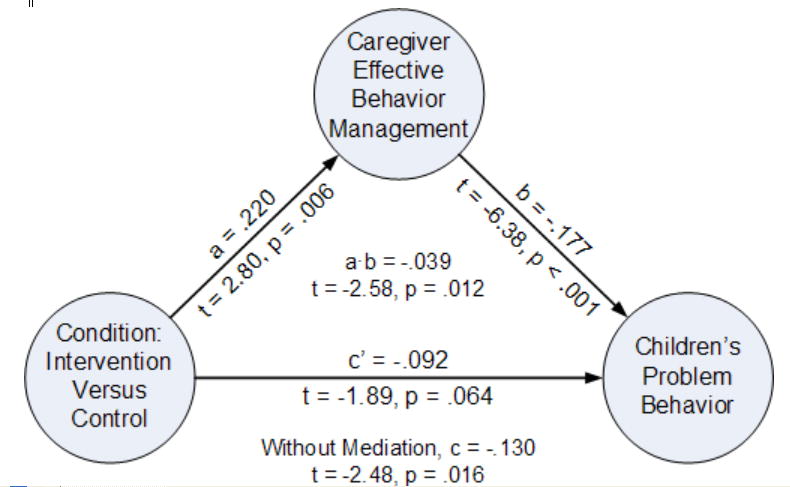
Mediation of caregiver effective behavior management on children’s problem behavior.
Effects of intervention exposure and years of experience providing child care
The extent of intervention exposure had no effect on caregivers’ classroom management practices or children’s rates of problem behavior. Experience providing family child care was associated with effective behavior management practices, where greater experience was associated with more effective practices (partial r = .25, t = 2.04, p = .046), but experience had no moderator effect. Child care experience also had no moderating effect on children’s problem behavior.
Discussion
This study had three primary goals. The first was to develop a research-based intervention for small groups of family child care providers serving preschool-aged children. The second was to evaluate the feasibility and acceptability of offering this intervention for the intended recipients. The third was to evaluate the immediate effects of the intervention in a small randomized efficacy trial on caregiver practices, the child care environment, and children’s behavior.
This project developed three research-based workshops with practical advice on promoting social development and managing challenging behavior. The workshops included presentations of video examples that were followed by discussion and practice activities. The development of the video-based program and a written manual increases the likelihood that the workshops can be readily replicated.
This study demonstrated that the intervention was highly appealing to family child care providers. In a previous survey about training needs, family child care providers reported that one of their biggest priorities for training is how to manage and reduce disruptive behavior (Rusby, 2002). In the present study, family child care providers confirmed this priority by the low attrition rate and good participation in the assessment and intervention activities, as well as through their positive evaluations of the workshops. Eighty-one percent maintained their participation in the study over the course of 2 years. Workshop attendance actually increased after the first workshop (from 71% to 81%). Those who missed a workshop watched the video and completed activities on their own time, resulting in 90% intervention participation for the first two modules and 87% for the third module. Between 90% and 100% of participants reported that they learned “some” to “very many” new things from the workshops and 86% to 100% reported learning “some” to “very many” practical skills. Collectively this demonstrates that this intervention was perceived by family child care providers as being useful and meeting an important need.
The third goal of this study was to conduct an initial experimental evaluation of the intervention. Perhaps the most important findings of the efficacy trial were that caregivers in the intervention group improved their observed effective behavior management practices (p = .006, d = .72). Reductions in overall problem behavior were found in the intervention child care homes compared to the waitlist control group (p = .016, d = .63). The medium-to-large effect sizes found for both these outcomes represent a change of approximately two-thirds of a standard deviation for intervention participants. The effective behavior management practices included supporting children’s efforts, encouraging active participation, providing clear instructions, preparing children for transitions, monitoring children, providing reminders of expectations, modeling positive behaviors, providing positive reinforcement to children, and being consistent with rules and consequences. A mediation model for these effects was tested, demonstrating that the improvements in behavior management practices were associated with reductions in children’s problem behavior (p < .001). A medium effect size was found for the mediation effect.
We adjusted the p-value to .10 to balance the likelihood of Type I and Type II errors in small-scale studies such as this (Cohen, 1990; Rosnow & Rosenthal, 1989). With the adjusted p-value, medium effects favoring the intervention group were found on the composite measure of caregiver monitoring, which included not only caregiver behavior (i.e., scanning, circulating, and maintaining proximity to children needing assistance) but also a rating of the extent to which the physical environment was set up to enhance visibility. A small effect was also found for observed positive attention, such as praise and approving gestures or physical contact. Caregivers in the intervention group increased the amount of positive attention provided to the children compared to the waitlist control group.
This study also detected evidence that the improvements in child care provider behavior faded over time. The greatest increases in effective behavior management and positive attention were found for the first observation, which occurred about a month following the intervention. Use of positive attention by child care providers in the intervention group decreased over time, indicating that this increase was not maintained 5 months following the intervention. Similarly, the improvements in effective behavior management practices and children’s behavior found in the intervention groups declined over time.
Maintaining effects in studies aimed at improving young children’s behavior and interpersonal skills has been a common challenge. For example, in school-based settings proactive behavior management practices for promoting positive behavior have been empirically tested and found to be effective; however, the difficulty is in maintaining the use of these practices over time (Sugai & Horner, 1999). In a review of randomized controlled trials aimed at improving children’s interpersonal skills, Taylor, Eddy, and Biglan (1999) also found evidence for short-term effects, but little evidence for maintenance of the effects. The authors surmise that the programs that do result in positive outcomes tend to be lengthy. This concurs with the results of a meta-analysis of preschool prevention programs (Nelson, Westhues, & MacLeod, 2003), in which the length of the intervention program significantly accounted for a portion of the variance in the maintenance of positive social outcomes into elementary and middle school. Perhaps breaking the intervention content into smaller “chunks” (e.g., provide a series of six workshop sessions that are 1½ hour long, rather than three workshop sessions that are 3 hours long) would allow caregivers to focus on and practice each strategy learned over a longer period of time. Attention to helping child care providers maintain their implementation of effective behavior management practices throughout the year would likely impact the maintenance of child outcomes. Such maintenance of effective practices could be promoted through booster sessions throughout the year. Booster sessions that include a review of main ideas, involve problem solving, and emphasize accomplishments and positive changes are more successful in achieving maintenance (Whisman, 1990). It also is possible that caregivers did not understand how to generalize the techniques learned to new problems or challenges that came up for them after the workshops were over. A follow-up booster session may help in learning how to apply what was learned to new situations.
Another approach for promoting generalization and maintenance of training outcomes involves behavioral consultation. Much of the research on the effectiveness of behavioral consultation has been done for school-age children in special education (e.g., Sheridan, Welch, & Orme, 1996). A consultation model of “coaching” that involves the caregiver in goal setting and intervention planning has been applied to child care (Hendrickson, Gardner, Kaiser, & Riley, 1993) and preschool settings (Kaminski & Stormchak, 2006). Such consultation approaches have also been described as “technical assistance” and resulted in preschool teachers’ generalization of instructional strategies (Peck, Killen, & Baumgart, 1989). Providing multiple examples of applying strategies to different situations via coaching facilitates maintenance and generalization (Stokes & Osnes, 1986). Positive outcomes were also found for preschool-age children who exhibited social and/or behavioral problems when consultation was provided that utilized assessment feedback (Schill, Kratochwill, & Elliott, 1998). Providing an on-site coaching method of consultation in addition to the workshop training would likely assist caregivers in understanding how to apply what was learned in the workshops to a variety of situations in their child care home and to get hands-on practice with goal setting and intervention planning, both of which would promote maintenance of their use of effective practices.
This study also found that, although intervention participants engaged in significantly more monitoring than waitlist control participants after intervention, both intervention and waitlist control groups showed a reduction in monitoring over time. In post hoc examination of the data, it appeared that baseline observations occurred more frequently on sunny days when children were outside and post observations occurred more frequently on rainy days when children were inside. Although it is plausible that higher levels of monitoring occurred in outdoor settings than inside the child care homes, that was not the case. The extent to which observations were conducted in indoor or outdoor settings did not differ by condition, and thus did not bias the outcomes. It is also possible that caregivers decreased monitoring to typical levels as they got more accustomed to the observers’ presence. In future studies, it may be important to increase the number of initial observations to acclimatize subjects to observers.
There was a lack of intervention outcomes for the child care environment from the Child Care Ecology Checklist (CCEC), which measured the organization of the environment, enrichment of the environment, and the planned activities. It is plausible that the CCEC was not sensitive to intervention change. A major change may only be reflected in one variable that comprised a composite score. Without sensitive measures, interventions may have beneficial effects that go unmeasured, resulting in potentially important interventions being discarded due to lack of evidence. Feedback from participants offered useful insights on barriers to change for these environmental features. Caregivers reported that the greatest barriers were in making changes to the physical environment compared to any other intervention component. These barriers were due to cost, time, and limited space. To facilitate such change, a combination of individualized consultation and financial support may be necessary. Given the associations between the environment in center-based child care and child behavior (Clarke-Stewart, 1987; Dunn, 1993), it seems reasonable to expect similar relationships in family child care settings. Modest investment in stimulating resources for child care homes would likely have a positive impact on many children.
One finding contrary to what was hypothesized was that caregivers in the intervention group reported decreased use of effective behavior management practices and the waitlist control group reported increased use. These results did not concur with observations of effective behavior management. Child care providers may not be valid reporters of their own behavior. Perhaps an assessment effect occurred for the waitlist control group where providers in the waitlist control condition became sensitized to behavior management concepts and increased their reporting of their use. It is also possible that once caregivers in the intervention group learned more about effective caregiver practices, they became more aware and possibly more critical of their own behavior.
Limitations of the Study and Future Research
An important limitation of this study is that it involved a relatively small sample. This small-scale efficacy study is the first step in examining the value of the developed intervention program for family child care providers. Since the intervention program was developed for caregivers of preschool-age children, the study sample was limited to child care homes with preschool-age children in attendance. The study sample also was limited to caregivers who had a good understanding of English. Study results therefore can be generalized solely to family child care providers who speak English and care for preschool-age children. A larger efficacy study is needed to test the extent to which outcomes found in this study are replicated. Depending on results of a larger replication efficacy trial, effectiveness studies in which the program is delivered in natural community settings would be the next step towards providing empirical evidence for the intervention program (Flay et al., 2005).
Another limitation of the study is that the effects are short-term, and there is reason to believe the benefits of the training would continue to fade with time without booster sessions or other strategies to promote maintenance. The data for this study are limited in that the last assessments were collected only five months following the intervention. It is important to recognize that outcomes of interventions for young children may occur at later developmental stages (e.g., Ialongo, Poduska, Werthamer, & Kellam, 2001; Olds et al., 2004), demonstrating the importance of long-term follow up. Replication studies with larger samples that incorporate maintenance strategies and evaluate them with long-term follow-up assessments would offer greater empirical evidence for the Carescapes program.
Another limitation of the efficacy trial was that all measures were aimed at the child care home, the care provider, and overall behavior of all children attending the child care home. No individual data on children were collected. The observation on children’s behavior involved the behavior of any children who were attending the child care home. Longitudinal measures at the individual child level would allow the examination of outcomes for children through different developmental stages. Moreover, with a larger sample size, it would allow for a study design in which children are nested in child care homes.
Summary
This study involved the development of a video-based intervention program for family child care providers aimed at promoting positive social development in preschool-age children and the first randomized controlled trial on its efficacy. This research highlights the importance of specific, proactive caregiver practices that encourage and support children and that prevent problems through monitoring and clearly defined expectations. These practices were found to be socially valid and useful for practitioners who provide child care in their home. However, results of the small-scale efficacy trial are mixed, as the positive outcomes on caregiver practices and child behavior that were found did not last. Clearly, further steps in evaluation are needed, such as larger-scale longitudinal efficacy and effectiveness studies to provide the empirical evidence needed for dissemination.
Given the dearth of interventions specifically designed for family child care providers, future early intervention and prevention work focused on family child care settings is called for. There are very few randomized controlled trials in preschools to promote social skills and reduce problem behaviors (Taylor et al., 1999) or in child care settings (Fukkink & Lont, 2007). This study stands as an example for conducting randomized controlled trials in child care settings, particularly in family child care in which experimental studies are lacking (Kontos, 1992). This study has shown that caregiver practices that have been found effective in preschool and group-based child care settings are also useful for home child care providers. It demonstrates the feasibility of such endeavors. Home child care providers were engaged in the training and they implemented some of the strategies learned in their child care home. Although increased effective behavior management was found immediately following the intervention and was related to decreased overall problem behavior of children in the child care home, the use of these strategies did not maintain over time. Further work on how to provide on-site consultation for family child care providers is needed to promote maintenance and generalization of effective caregiving practices. Also, further work is needed to address the barriers of the cost and time needed to implement environmental changes in child care homes. Such improvements imply the need for sources of funding for consultation and resources (such as age appropriate toys, equipment, furniture) for home child care settings. The many children who attend family child care are likely to benefit when the breadth of good quality early childhood practices and research extends to those settings.
Acknowledgments
This research was supported by grant # R42 HD042952 from the National Institute on Child Health and Human Development.
The authors are grateful for the contributions provided by the consultants, Ruth Kaminski, Ph.D., Thomas J. Dishion, Ph.D., Robert H. Horner, Ph.D., and Susan Norton, who offered a wealth of helpful advice. The assessment team, Cathy Milchak, Jules Gordon, Robin Ware, and Kristina Hulegaard, are to be commended for their quality work. Appreciation also goes to Helen Kuo for data preparation and Susan Long for her assistance with this manuscript.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- Aguirre BE, Marshall MG. Training family day care providers using self-study written and video materials. Child and Youth Care Quarterly. 1988;17:115–127. [Google Scholar]
- Akaike H. A new look at the statistical model identification. IEEE Transactions on Automatic Control. 1974;19:716–723. [Google Scholar]
- Arnett J. Caregivers in day-care centers: Does training matter? Journal of Applied Developmental Psychology. 1989;10:541–552. [Google Scholar]
- Baron RM, Kenny DA. The moderator-mediator distinction in social psychological research: Conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology. 1986;51:1173–1182. doi: 10.1037//0022-3514.51.6.1173. [DOI] [PubMed] [Google Scholar]
- Belsky J, Vandell DL, Burchinal M, Carke-Stewart KA, McCartney K, Owen MT. Are there long-term effects of early child care? Child Development. 2007;78:681–701. doi: 10.1111/j.1467-8624.2007.01021.x. [DOI] [PubMed] [Google Scholar]
- Bordin J, Machida S, Varnell H. The relation of quality indicators to provider knowledge of child development in family child care homes. Child and Youth Care Forum. 2000;29:323–341. [Google Scholar]
- Brooks-Gunn J, Duncan G, Aber JL. Neighborhood poverty: Context and consequences for children. New York: Russell Sage Foundation; 1997. [Google Scholar]
- Broussard CD, Northup J. An approach to functional assessment and analysis of disruptive behavior in regular education classrooms. School Psychology Quarterly. 1995;10(2):151–164. [Google Scholar]
- Burchinal M, Howes C, Kontos S. Structural predictors of child care quality in child care homes. Early Childhood Research Quarterly. 2002;17:87–105. [Google Scholar]
- Burnham KP, Anderson DR. Model selection and multi-model inference: A practical information-theoretic approach. 2. New York: Springer–Verlag; 2002. [Google Scholar]
- Campbell SB, Ewing LJ. Follow-up of hard-to-manage preschoolers: Adjustment at age 9 and predictors of continuing symptoms. Journal of Child Psychology and Psychiatry. 1990;31:871–889. doi: 10.1111/j.1469-7610.1990.tb00831.x. [DOI] [PubMed] [Google Scholar]
- Campbell FA, Ramey CT, Pungello E, Sparling J, Miller-Johnson S. Early childhood education: Young adult outcomes from the Abecedarian Project. Applied Developmental Science. 2002;6(1):42–57. [Google Scholar]
- Capaldi DM, Patterson GR. Psychometric properties of fourteen latent constructs from the Oregon Youth Study. New York: Springer–Verlag; 1989. [Google Scholar]
- Carnine DW. Bridging the research-to-practice gap. Issues in educating students with disabilities. In: Lloyd JW, Kameenui EJ, Chard D, editors. LEA's series on special education and disability. Mahwah, NJ: Lawrence Erlbaum Associates; 1997. [Google Scholar]
- Carr EG, Durand VM. Reducing behavior problems through functional communication training. Journal of Applied Behavior Analysis. 1985;18:111–126. doi: 10.1901/jaba.1985.18-111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chambless DL, Ollendick TH. Empirically supported psychological interventions: Controversies and evidence. Annual Review of Psychology. 2001;52:685–716. doi: 10.1146/annurev.psych.52.1.685. [DOI] [PubMed] [Google Scholar]
- Clarke-Stewart KA. Predicting child development from child care forms and features: The Chicago study. Vol. 1. Washington, DC: National Association for the Education of Young Children; 1987. [Google Scholar]
- Cohen J. Statistical power analysis for the behavioral sciences. Hillsdale, NJ: Erlbaum; 1988. [Google Scholar]
- Cohen J. Things I have learned (so far) American Psychologist. 1990;45:1304–1312. [Google Scholar]
- Cohen J, Cohen P, West SG, Aiken LS. Applied multiple regression/correlation analysis for the behavioral sciences. 3. Mahwah, NJ: Erlbaum; 2003. [Google Scholar]
- de Kruif REL, McWilliam RA, Ridley SM, Wakely MB. Classification of teachers' interaction behaviors in early childhood classroom. Early Childhood Research Quarterly. 2000;15:247–268. [Google Scholar]
- Dodge KA, Pettit GS, Bates JE. Socialization mediators of the relation between socioeconomic status and child conduct problems. Child Development. 1994;65:649–665. [PubMed] [Google Scholar]
- Dunlap G, Kern L, dePerczel M, Clark S, Wilson D, Childs K, et al. Functional analysis of classroom variables for students with emotional and behavioral disorders. Behavioral Disorders. 1993;18:275–291. [Google Scholar]
- Dunn L. Proximal and distal features of day care quality and children's development. Early Childhood Research Quarterly. 1993;8:167–192. [Google Scholar]
- Fitzmaurice GM, Laird NM, Ware JH. Applied longitudinal analysis. Hoboken, NJ: Wiley; 2004. [Google Scholar]
- Flay BR, Biglan A, Boruch RF, Gonzalez Castro F, Gottfredson D, Kellam S, et al. Standards of evidence: Criteria for efficacy, effectiveness and dissemination. Prevention Science. 2005;6:151–175. doi: 10.1007/s11121-005-5553-y. [DOI] [PubMed] [Google Scholar]
- Frankel AJ. Family day care in the United States. Families in Society: The Journal of Contemporary Human Services. 1994;75:550–560. [Google Scholar]
- Friedman SL, Amadeo J. The child-care environment: Conceptualizations, assessments, and issues. In: Friedman SL, Wacker D, editors. Measuring environment across the life span. Washington, DC: American Psychological Association; 1999. pp. 127–164. [Google Scholar]
- Fukkink RG, Lont A. Does training matter? A meta-analysis and review of caregiver training studies. Early Childhood Research Quarterly. 2007;22:294–311. [Google Scholar]
- Galinsky E, Howes C, Kontos S, Shimm M. The study of children in family child care and relative care. New York: Families and Work Institute; 1994. Retrieved May 23, 2003, at www.familiesandwork.org/publications. [Google Scholar]
- Goelman H, Pence AR. Children in three types of day care: Daily experiences, quality of care and developmental outcomes. In: Homing AS, editor. Optimizing early child care and education. New York, NY: Gordon & Breach Science Publishers; 1990. pp. 67–76. [Google Scholar]
- Greenberg MT, Wehby JH. Classroom Atmosphere Rating Scale. Fast Track: Conduct Problems Prevention Research Group. 1995. (Unpublished manual) [Google Scholar]
- Gueorguieva R, Krystal JH. Move over ANOVA: Progress in analyzing repeated-measures data and its reflection in papers published in the archives of general psychiatry. Archives of General Psychiatry. 2004;61:310–317. doi: 10.1001/archpsyc.61.3.310. [DOI] [PubMed] [Google Scholar]
- Hagekull B, Bohlin G. Day care quality, family and child characteristics and socioemotional development. Early Childhood Research Quarterly. 1995;10:505–526. [Google Scholar]
- Hawkins JD, von Cleve E, Catalano RF. Reducing early childhood aggression: Results of a primary prevention program. Journal of the American Academy of Child & Adolescent Psychiatry. 1991;30:208–217. doi: 10.1097/00004583-199103000-00008. [DOI] [PubMed] [Google Scholar]
- Hendrickson JM, Gardner N, Kaiser AP, Riley A. Evaluation of a social interaction coaching program in an integrated day-care setting. Journal of Applied Behavior Analysis. 1993;26:213–225. doi: 10.1901/jaba.1993.26-213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hilton A. Using ecological strategies when working with young children. Pointer. 1987;31:52–55. [Google Scholar]
- Hofferth SL, Shauman KA, Henke RR, West J. U.S. Department of Education, National Center for Education Statistics. Washington, DC: U.S. Government Printing Office; 1998. Characteristics of children’s early care and education programs: Data from the 1995 National Household Education Survey (NCES Statistical Analysis Report 98–128) [Google Scholar]
- Howes C. Caregiver behavior in center and family day care. Journal of Applied Developmental Psychology. 1983;4:99–107. [Google Scholar]
- Howes C, Hamilton CE. Child care for young children. In: Spodek B, editor. Handbook of research on the education of young children. New York: Macmillan; 1993. pp. 322–336. [Google Scholar]
- Howes C, Phillips DA, Whitebook M. Thresholds of quality: Implications for the social development of children in center-based child care. Child Development. 1992;63:449–460. doi: 10.1111/j.1467-8624.1992.tb01639.x. [DOI] [PubMed] [Google Scholar]
- Hox JJ. Multivariate analysis: Techniques and applications. Mahwah, NJ: Lawrence Erlbaum Associates; 2002. [Google Scholar]
- Ialongo N, Poduska J, Werthamer L, Kellam S. The distal impact of two first-grade prevention interventions on conduct problems and disorder in early adolescence. Journal of Emotional and Behavioral Disorders. 2001;9:146–160. [Google Scholar]
- Jaccard J, Turrisi R. Interaction effects in multiple regression. 2. Thousand Oaks, CA: Sage; 2003. [Google Scholar]
- Judd CM, Kenny DA. Estimating the effect of social interventions. Cambridge, UK: Cambridge University Press; 1981. [Google Scholar]
- Kaminski RA, Stormshak EA. Project STAR: Early intervention with preschool children and families for the prevention of substance abuse. In: Sanbrano S, Tolan P, Szapocznik J, editors. Preventing youth substance abuse: Science based programs for children and adolescents. Washington, DC: American Psychological Association; 2006. pp. 89–109. [Google Scholar]
- Kazdin AE. Treatment research: The investigation and evaluation of psychotherapy. In: Hersen M, Kazdin AE, Bellack AS, editors. Pergamon general psychology series: Vol. 120. The clinical psychology handbook. 2. Elmsford, NY: Pergamon Press; 1991. pp. 293–312. [Google Scholar]
- Kern L, Childs KE, Dunlap G, Clarke S, Falk GD. Using assessment-based curricular intervention to improve the classroom behavior of a student with emotional and behavioral challenges. Journal of Applied Behavior Analysis. 1994;27:7–19. doi: 10.1901/jaba.1994.27-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kontos S. The role of continuity and context in children's relationships with nonparental adults. In: Pianta RC, editor. New directions for child development: Vol. 57. Beyond the parent: The role of other adults in children's lives. San Francisco, CA: Jossey–Bass; 1992. pp. 109–119. [Google Scholar]
- Kontos S, Howes C, Galinsky E. Does training make a difference to quality in family child care? Early Childhood Research Quarterly. 1996;11:427–445. [Google Scholar]
- Kreft I, de Leeuw J. Introducing multilevel modeling. London: Sage; 1998. [Google Scholar]
- Laird NM. Missing data in longitudinal studies. Statistics in Medicine. 1988;7:305–315. doi: 10.1002/sim.4780070131. [DOI] [PubMed] [Google Scholar]
- Lalli JS, Browder DM, Mace FC, Brown DK. Teacher use of descriptive analysis data to implement interventions to decrease students' problem behaviors. Journal of Applied Behavior Analysis. 1993;26:227–238. doi: 10.1901/jaba.1993.26-227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lamb ME. The effects of quality of care on child development. Applied Developmental Science. 2000;4(3):112–115. [Google Scholar]
- Lamb ME. Nonparental child care: Context, quality, correlates and consequences. In: Damon W, Lerner RM, Renninger KA, Sigel IE, editors. Handbook of child psychology: Vol. 4. Child psychology in practice. 6. Hoboken, NJ: John Wiley & Sons; 2006. pp. 950–1016. [Google Scholar]
- Lewis TJ, Sugai G. Teaching communicative alternatives to socially withdrawn behavior: An investigation in maintaining treatment effects. Journal of Behavioral Education. 1993;3:61–75. [Google Scholar]
- Lewis TJ, Sugai G. Descriptive and experimental analysis of teacher and peer attention and the use of assessment-based intervention to improve pro-social behavior. Journal of Behavioral Education. 1996;6:7–24. [Google Scholar]
- Little RJA, Rubin DB. Statistical analysis with missing data. 2. New York: John Wiley & Sons; 2002. [Google Scholar]
- Loeb S, Fuller B, Kagan SL, Carrol B. Child care in poor communities: Early learning effects of type, quality, and stability. Child Development. 2004;75:47–65. doi: 10.1111/j.1467-8624.2004.00653.x. [DOI] [PubMed] [Google Scholar]
- Loeber R. Development and risk factors of juvenile antisocial behavior and delinquency. Clinical Psychology Review. 1990;10:1–41. [Google Scholar]
- Love JM, Harrison L, Sagi-Schwartz A, van Ijzendoorn MH, Ross CN, Ungerer JA, et al. Child care quality matters: How conclusions may vary with context. Child Development. 2003;74:1021–1033. doi: 10.1111/1467-8624.00584. [DOI] [PubMed] [Google Scholar]
- Maas CJM, Hox JJ. The influence of violations of assumptions on multilevel parameter estimates and their standard errors. Computational Statistics and Data Analysis. 2004;46:427–440. [Google Scholar]
- MacKinnon DP, Lockwood CM, Hoffman JM, West SG, Sheets V. A comparison of methods to test mediation and other intervening variable effects. Psychological Methods. 2002;7:83–104. doi: 10.1037/1082-989x.7.1.83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MacKinnon DP, Warsi G, Dwyer JH. A simulation study of mediated effect measures. Multivariate Behavioral Research. 1995;30:41–62. doi: 10.1207/s15327906mbr3001_3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maas CJM, Hox JJ. The influence of violations of assumptions on multilevel parameter estimates and their standard errors. Computational Statistics and Data Analysis. 2004;46:427–440. [Google Scholar]
- McCartney K, Scarr S, Phillips D, Grajek S. Day care as intervention: Comparisons of varying quality programs. Journal of Applied Developmental Psychology. 1985;6:247–260. [Google Scholar]
- McEvoy MA, Fox JJ, Rosenberg MS. Organizing preschool environments: Suggestions for enhancing the development/learning of preschool children with handicaps. Topics in Early Childhood Special Education. 1991;11(2):18–28. [Google Scholar]
- McGraw KO, Wong SP. Forming inferences about some intraclass correlation coefficients. Psychological Methods. 1996;1:30–46. [Google Scholar]
- Mesman J, Bongers IL, Koot HM. Preschool developmental pathways to preadolescent internalizing and externalizing problems. Journal of Child Psychology and Psychiatry. 2001;42:679–689. [PubMed] [Google Scholar]
- Moffitt TE. Adolescence-limited and life-course-persistent antisocial behavior: A developmental taxonomy. Psychological Review. 1993;100:674–701. [PubMed] [Google Scholar]
- Mulligan GM, Brimhall D, West J, Chapman C. Child care and early education arrangements of infants, toddlers, and preschoolers: 2001 (NCES Statistical Analysis Report 2006–039). U.S. Department of Education, National Center for Education Statistics. Washington, DC: U.S. Government Printing Office; 2005. [Google Scholar]
- Murray DM, Hannan PJ, Baker WL. A Monte Carlo study of alternative responses to intraclass correlation in community trials: Is it ever possible to avoid Cornfield's penalties? Evaluation Review. 1996;20:313–337. doi: 10.1177/0193841X9602000305. [DOI] [PubMed] [Google Scholar]
- Muthén BO, Curran PJ. General longitudinal modeling of individual differences in experimental designs: A latent variable framework for analysis and power estimation. Psychological Methods. 1997;2:371–402. [Google Scholar]
- Myung IJ. The importance of complexity in model selection. Journal of Mathematical Psychology. 2000;44:190–204. doi: 10.1006/jmps.1999.1283. [DOI] [PubMed] [Google Scholar]
- Nafpaktitis M, Mayer GR, Butterworth TW. Natural rates of teacher approval and disapproval and their relation to student behavior in intermediate school classrooms. Journal of Educational Psychology. 1985;77:362–367. [Google Scholar]
- National Research Council and Institute of Medicine. Community programs to promote youth development. Washington, DC: National Academy Press; 2002. [Google Scholar]
- Nelson G, Westhues A, MacLeod J. A meta-analysis of longitudinal research on preschool prevention programs for children. Prevention & Treatment. 2003;6 Article 31. Retrieved September 20, 2007, from http://journals.apa.org/prevention/volume6/pre631a.html.
- Nich C, Carroll K. Now you see it, now you don’t: A comparison of traditional versus random-effects regression models in the analysis of longitudinal follow-up data from a clinical trial. Journal of Consulting and Clinical Psychology. 1997;65:252–261. doi: 10.1037//0022-006x.65.2.252. [DOI] [PubMed] [Google Scholar]
- NICHD Early Child Care Research Network. Child-care and family predictors of preschool attachment and stability from infancy. Developmental Psychology. 2001;37:847–862. [PubMed] [Google Scholar]
- NICHD Early Child Care Research Network. Does quality of child care affect child outcomes at age 4½? Developmental Psychology. 2003;39:451–469. doi: 10.1037/0012-1649.39.3.451. [DOI] [PubMed] [Google Scholar]
- NICHD Early Child Care Research Network. Trajectories of physical aggression from toddlerhood to middle childhood. Monographs of the Society for Research in Child Development. 2004;69 doi: 10.1111/j.0037-976x.2004.00312.x. Serial No. 278. [DOI] [PubMed] [Google Scholar]
- Nordquist VM, Twardosz S. Preventing behavior problems in early childhood special education classrooms through environmental organization. Education and Treatment of Children. 1990;13:274–287. [Google Scholar]
- Norris DJ. Quality of care offered by providers with differential patterns of workshop participation. Child and Youth Care Forum. 2001;30:111–121. [Google Scholar]
- Northrup J, Broussard CD, Jones K, George T, Vollmer TR, Herring M. The differential effects of teacher and peer attention on the disruptive classroom behavior of three children with a diagnosis of attention deficit hyperactivity disorder. Journal of Applied Behavior Analysis. 1995;28:227–228. doi: 10.1901/jaba.1995.28-227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Odom SL, Ogawa I. Direct observation of young children's social interaction with peers: A review of methodology. Behavioral Assessment. 1992;14:407–441. [Google Scholar]
- Olds DL, Robinson J, Pettitt L, Luckey DW, Holmberg J, Ng RK, et al. Effects of home visits by paraprofessionals and by nurses: Age 4 follow-up results of a randomized trial. Pediatrics. 2004;114:1560–1568. doi: 10.1542/peds.2004-0961. [DOI] [PubMed] [Google Scholar]
- Olson SL. Development of conduct problems and peer rejection in preschool children: A social systems analysis. Journal of Abnormal Child Psychology. 1992;20:327–350. doi: 10.1007/BF00916696. [DOI] [PubMed] [Google Scholar]
- Olson SL, Rosenblum K. Preschool antecedents of internalizing problems in children. Early Education and Development. 1998;9:117–129. [Google Scholar]
- O'Neill RE, Horner RH, Albin RW, Sprague JR, Storey K, Newton JS. Functional assessment of problem behavior: A practical handbook. Pacific Grove, CA: Brooks/Cole; 1997. [Google Scholar]
- Patterson GR, Reid JB, Dishion TJ. Antisocial boys: A social interactional approach. Vol. 4. Eugene, OR: Castalia; 1992. [Google Scholar]
- Peck CA, Killen CC, Baumgart D. Increasing implementation of special education instruction in mainstream preschools: Direct and generalized effects of nondirective consultation. Journal of Applied Behavior Analysis. 1989;22:197–210. doi: 10.1901/jaba.1989.22-197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Peisner-Feinberg ES, Burchinal MR. Relations between preschool children's child-care experiences and concurrent development: The cost, quality, and outcomes study. Merrill–Palmer Quarterly. 1997;43:451–77. [Google Scholar]
- Peisner-Feinberg ES, Burchinal MR, Clifford RM, Culkin ML, Howes C, Kagan SL, et al. The relation of preschool child-care quality to children's cognitive and social developmental trajectories through second grade. Child Development. 2001;72:1534–1553. doi: 10.1111/1467-8624.00364. [DOI] [PubMed] [Google Scholar]
- Phillips D, McCartney K, Scarr S. Child-care quality and children's social development. Developmental Psychology. 1987;23:537–543. [Google Scholar]
- Project STAR. Early Childhood Classroom Ecology Checklist. Eugene, OR: University of Oregon; 2002. [Google Scholar]
- Richman N, Stevenson J, Graham PJ. Preschool to school: A behavioural study. San Diego, CA: Academic; 1982. [Google Scholar]
- Rosenthal R, Rosnow RL, Rubin DB. Contrasts and effect sizes in behavioral research: A correlational approach. New York: Cambridge University Press; 2000. [Google Scholar]
- Rosenthal R, Rubin DB. requivalent: A simple effect size indicator. Psychological Methods. 2003;8:492–496. doi: 10.1037/1082-989X.8.4.492. [DOI] [PubMed] [Google Scholar]
- Rosnow RL, Rosenthal R. Statistical procedures and the justification of knowledge in psychological science. American Psychologist. 1989;44:1276–1284. [Google Scholar]
- Rubin DB. Estimating causal effects of treatments in randomized and nonrandomized studies. Journal of Educational Psychology. 1974;66:688–701. [Google Scholar]
- Rusby JC. Training needs and challenges of family child care providers. Child and Youth Care Forum. 2002;31:287–299. [Google Scholar]
- Rusby JC, Taylor TK, Marquez B. Promoting positive social development in family childcare settings. Early Education and Development. 2004;15:449–470. [Google Scholar]
- Rusby JC, Taylor TK, Milchak C. Assessing school settings: Interactions of students and teachers. Eugene, OR: Oregon Research Institute; 2001. [Google Scholar]
- SAS Institute. SAS/STAT® 9.1 user's guide. Cary, NC: SAS Institute, Inc; 2004. [Google Scholar]
- Schafer JL, Graham JW. Missing data: Our view of the state of the art. Psychological Methods. 2002;7:147–177. [PubMed] [Google Scholar]
- Schill MT, Kratochwill TR, Elliott SN. Functional assessment in behavioral consultation: A treatment utility study. School Psychology Quarterly. 1998;13:116–140. [Google Scholar]
- Schweinhart LJ, Berrueta-Clement JR, Barnett WS, Epstein MH, Weikart DP. Effects of the Perry Preschool program on youths through age 19: A summary. Topics in Early Childhood Special Education. 1985;5(2):26–35. [Google Scholar]
- Sheridan SM, Welch M, Orme SF. Is consultation effective? A review of outcome research. Remedial and Special Education. 1996;17:341–354. [Google Scholar]
- Shonkoff JP, Phillips DA, editors. From neurons to neighborhoods: The science of early childhood development. Washington, DC: National Academy Press; 2000. [PubMed] [Google Scholar]
- Shrout PE, Fleiss JL. Intraclass correlations: Uses in assessing rater reliability. Psychological Bulletin. 1979;86:420–428. doi: 10.1037//0033-2909.86.2.420. [DOI] [PubMed] [Google Scholar]
- Singer JD, Willett JB. Applied longitudinal data analysis: Modeling change and event occurrence. New York: Oxford University Press; 2003. [Google Scholar]
- Sobel ME. Asymptotic confidence intervals for indirect effects in structural equations models. In: Leinhart S, editor. Sociological methodology 1982. San Francisco: Jossey–Bass; 1982. pp. 290–312. [Google Scholar]
- Sprague J, Sugai G, Walker H. Antisocial behavior in schools. In: Watson TS, Gresham FM, editors. Handbook of child behavior therapy. New York: Plenum; 1998. pp. 451–474. [Google Scholar]
- Stokes TF, Osnes PG. Programming for the generalization of children’s social behavior. In: Strain PS, Guralnick MJ, Walker HM, editors. Children’s social behavior: Development, assessment, and modification. Orlando, FL: Academic Press; 1986. pp. 337–355. [Google Scholar]
- Sugai G, Horner RH. Discipline and behavioral support: Practices, pitfalls, and promises. Effective School Practices. 1999;17(4):10–22. [Google Scholar]
- Taylor JC, Romanczyk RG. Generating hypotheses about the function of student problem behavior by observing teacher behavior. Journal of Applied Behavior Analysis. 1994;27:251–265. doi: 10.1901/jaba.1994.27-251. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Taylor TK, Eddy JM, Biglan A. Interpersonal skills training to reduce aggressive and delinquent behavior: Limited evidence and the need for an evidence-based system of care. Clinical Child and Family Psychology Review. 1999;2:169–182. doi: 10.1023/a:1021855022385. [DOI] [PubMed] [Google Scholar]
- Taylor TK, Schmidt F, Pepler D, Hodgins C. A comparison of eclectic treatment with Webster-Stratton's parents and children series in a children's mental health center: A randomized controlled trial. Behavior Therapy. 1998;29:221–240. [Google Scholar]
- Twardosz W, Risley TR. Community mental health and behavioral-ecology: A handbook of theory, research, and practice. New York: Plenum; 1982. Behavioral-ecological consultation to day care centers; pp. 147–159. [Google Scholar]
- Umbreit J. Functional assessment and intervention in a regular classroom setting for the disruptive behavior of a student with attention deficit hyperactivity disorder. Behavioral Disorders. 1995;20:267–278. [Google Scholar]
- Venter A, Maxwell SE, Bolig E. Power in randomized group comparisons: The value of adding a single intermediate time point to a traditional pretest–posttest design. Psychological Methods. 2002;7:194–209. doi: 10.1037/1082-989x.7.2.194. [DOI] [PubMed] [Google Scholar]
- Verbeke G, Molenberghs G. Linear mixed models for longitudinal data. New York: Springer–Verlag; 2000. [Google Scholar]
- Walker HM. The acting-out child: Coping with classroom disruption. Longmont, CO: Sopris West; 1995. [Google Scholar]
- Walker HM, Schwarz IE, Nippold MA, Irvin LK. Social skills in school-age children and youth: Issues and best practices in assessment and intervention. Topics in Language Disorders. 1994;14(3):70–82. [Google Scholar]
- Weaver RH. Predictors of quality and commitment in family child care: Provider education, personal resources, and support. Early Education and Development. 2002;13:265–282. [Google Scholar]
- Webster-Stratton C, Hollinsworth T, Kolpacoff M. The long-term effectiveness and clinical significance of three cost-effective training programs for families with conduct-problem children. Journal of Consulting and Clinical Psychology. 1989;57:550–553. doi: 10.1037//0022-006x.57.4.550. [DOI] [PubMed] [Google Scholar]
- Webster-Stratton C, Reid MJ, Hammond M. Preventing conduct problems, promoting social competence: A parent and teacher training partnership in head start. Journal of Clinical Child Psychology. 2001;30:283–302. doi: 10.1207/S15374424JCCP3003_2. [DOI] [PubMed] [Google Scholar]
- Whisman MA. The efficacy of booster maintenance sessions in behavior therapy: Review and methodological critique. Clinical Psychology Review. 1990;10:155–170. [Google Scholar]
- Yoshikawa H, Knitzer J. Lessons from the field: Head Start mental health strategies to meet changing needs. New York: National Center for Children in Poverty; 1997. [Google Scholar]
- Zucchini W. An introduction to model selection. Journal of Mathematical Psychology. 2000;44:41–61. doi: 10.1006/jmps.1999.1276. [DOI] [PubMed] [Google Scholar]