

Abstract
Objective
To assess aspirations for physical health over 18 months. To examine whether maintained importance of aspirations for physical health mediated and/or moderated the effect of an intensive intervention on long-term tobacco abstinence.
Methods
Participants were randomly assigned to an intervention based on self-determination theory or to community care, and provided data at baseline and at 18 and 30 months post-randomization.
Results
Aspirations for physical health were better maintained over 18 months among participants in the intervention (mean change = .05), relative to community care (mean change = -.13), t = 2.66, p < .01. Maintained importance of aspirations for physical health partially mediated the treatment condition effects on seven-day point prevalence tobacco abstinence (z′ = 1.68, p < .01) and the longest number of days not smoking (z′ = 2.16, p < .01), and interacted with treatment condition to facilitate the longest number of days not smoking (β = .08, p < .05).
Conclusion
Maintained importance of aspirations for physical health facilitated tobacco abstinence.
Practice implications
Smokers may benefit from discussing aspirations for physical health within autonomy-supportive interventions. Patients may benefit from discussing aspirations during counseling about therapeutic lifestyle change and medication use.
Keywords: health aspirations, self-determination theory, tobacco abstinence
1. Introduction
Life goals, or aspirations, are important to the organization and direction of behavior. Recent theory [1] and research [2] have suggested that people differ in the level of importance they place on certain aspirations, and that the importance of those goals predicts their attainment; that is, the more important the goal, the more progress one will make toward achieving it [3, 4]. Thus, the aspirations people value help shape their life course and are presumed to have consequences for their social and psychological adjustment.
Self-determination theory (SDT; 5, 6, 7) posits that humans have a natural tendency toward psychological growth and physical health. Surprisingly, however, within SDT little empirical attention has been given to the aspiration for physical health. Research has demonstrated that the aspiration for physical health typically aligns with intrinsic life goals (viz., personal growth, close relationships, and community involvement), which are associated with social adjustment and psychological well-being, whereas the aspiration for physical health is inversely related to extrinsic life goals (viz., money, fame, and image), which are associated with maladjustment and ill-being [e.g., 2, 3, 8, 9, 10, 11, 12, 13]. Importantly, some studies within the health domain have demonstrated a positive association between self-reported health values— specifically defined as the extent to which an individual believes it is important to be in good health [e.g., 14]—and health-related behaviors or healthy living [e.g., 15]. However, this research has been limited primarily to cross-sectional assessments that often are taken from highly-specified target groups (e.g., high-risk youths, the elderly, patients co-infected with HIV/hepatitis C). Thus, the role of aspirations for physical health in facilitating health-behavior change in general, and long-term tobacco abstinence in particular, remains largely unexplored.
The current study examined the relation of maintenance of smokers' aspirations for physical health over 18 months to long-term tobacco abstinence in a community sample of adults enrolled in the Smokers' Health Study (SHS; for an overview of the SHS, see 16). The SHS is a randomized clinical trial of the effectiveness of an SDT-based intervention that focused on supporting patient autonomy as the primary clinical goal, relative to community care, in facilitating long-term tobacco abstinence. One important component of the SDT-based intervention was that counselors, who were trained to use an autonomy-supportive approach, elicited from participants their life aspirations and encouraged participants to discuss the ways in which they believed smoking helped and/or hindered their attaining those goals. The effectiveness of the SDT-based intervention was compared to community care, in which practitioners may or may not have elicited participants' life aspirations using an autonomy-supportive approach. We suggest that when smokers discuss their life aspirations with healthcare practitioners in a context that provides support for autonomy, they will be better able to effectively utilize the innate energy of their aspirations for physical health to facilitate health-behavior change.
Our first aim was to examine the effect of the SDT-based intervention, relative to community care, on maintenance of smokers' aspirations for physical health over 18 months. Our second aim was to examine the relation of maintenance of smokers' aspirations for physical health over 18 months to long-term (i.e., 24 months post-intervention, which is 30 months post-randomization) tobacco abstinence. To carry out these objectives, we tested three hypotheses. First, because patients responded to a study aimed specifically at smokers' health, we expected that aspirations for physical health would be valued highly by participants upon entry into the study; however, we hypothesized that the high importance of those aspirations would be better maintained from baseline to 18 months among smokers in the SDT-based intervention because the counselors explicitly elicited participants' aspirations using an autonomy-supportive approach with the intent to facilitate integration of autonomous self-regulation with those goals. Second, we hypothesized that maintained aspirations for physical health would partially mediate the significant effect of treatment condition on long-term tobacco abstinence reported by Williams and his colleagues [17]. Third, we hypothesized that the relation of maintained aspirations for physical health to long-term tobacco abstinence would be moderated by treatment condition, such that maintained aspirations for physical health would have a stronger relation to the tobacco outcomes within the SDT-based intervention, relative to community care. We expected to find this interaction because aspirations for physical health are likely to have a stronger relation to behavior change in contexts designed to support autonomy for health-behavior change; that explicitly elicited and encouraged participants to discuss their life aspirations using an autonomy-supportive approach; and that asked participants about how smoking helped and/or hindered their attaining those goals, while remaining non-judgmental. Importantly, if results indicated that the SDT-based intervention supported the maintenance of smokers' aspirations for physical health, and that maintained aspirations for physical health related to long-term tobacco abstinence, it would suggest that the effectiveness of intensive interventions designed to facilitate tobacco abstinence may be augmented by health care practitioners' focusing explicitly on patients' life aspirations in a manner that supported their autonomy for health-behavior change.
2. Methods
2.1. Participants and procedure
Adult smokers were recruited using signs in physicians' offices and newspaper advertisements to participate in a study about “smokers' health.” Between January 2000 and July 2002, 2,681 smokers were screened for eligibility in the study, and 2,037 of those screened met eligibility criteria and provided phone consent to have two fasting lipid profiles seven days apart prior to their baseline appointment, which provided a risk-estimate of heart disease. Eligible participants were those who had smoked more than 100 cigarettes in their lifetime and had smoked five or more cigarettes per day during the week prior to enrollment, were 18 years of age or older, read and spoke English, had no history of psychotic illness (although anxiety and depression were allowed), had a minimal life expectancy of 18 months, and planned to live in the area for at least 18 months. Importantly, smokers were able to participate in the study regardless of whether they intended to quit smoking. Of those who were eligible, 1,006 (360 male, 643 female, and three who failed to indicate gender) came to an initial appointment, provided full informed consent, completed baseline questionnaires, and were randomized.
Randomization was stratified by whether participants met the National Cholesterol Education Program's LDL-C goals [18], which was based on the results of their fasting lipid profiles. Previous research indicated that the dietary intervention had no effect on the tobacco outcomes [19]. Accordingly, in the current study we collapsed across dietary and tobacco intervention conditions and focused only on the tobacco intervention and outcomes. Seventy percent of the participants (n = 714) were randomly assigned to a six-month SDT-based intervention designed to support autonomy for smoking cessation, whereas the rest (n = 292) received community care. This ratio for random assignment was used to minimize harm to the community care group, as the intensive intervention was expected to have a more pronounced effect on smoking cessation [20]. All community care participants were offered intensive treatment after the 24-month post-intervention follow-up. Participant flow through the 30-month study period is depicted in Figure 1. This study was approved by the University of Rochester Human Subjects Review Board and all participants provided informed consent prior to randomization.
Figure 1.

CONSORT recruitment and retention of participants.
A detailed description of the study design, recruitment procedures, and treatment approach have been presented elsewhere [16], as have baseline demographics and the primary outcome results at six, 18, and 30 months [17, 19, 21]. Following informed consent, completion of the baseline measures, and randomization, participants in the SDT-based intervention met with a counselor and were asked about their smoking history and their attitudes toward smoking, and were informed about the potential health benefits of tobacco abstinence (e.g., 12 months of tobacco abstinence could reduce the 10-year risk for developing coronary artery disease by 50%). Counselors encouraged participants to discuss their life aspirations and the ways in which they believed smoking helped and/or hindered their attaining those goals. Additionally, counselors were trained to remain non-judgmental regarding participants' life aspirations; specifically, counselors did not offer further comment on whether they believed participants' aspirations were good or bad, or whether they believed that continuing to smoke or quitting would help and/or hinder participants' attaining those aspirations. Finally, participants were asked whether they wanted to quit using tobacco. If yes, counselors provided competence support; if no, participants were asked to return in two months to discuss again. Counselors used an autonomy-supportive approach throughout the intervention, which means that they related to the participants from the participants' perspectives, emphasized the participants' choice to continue to smoke or to quit, and provided relevant information in a non-pressuring manner [22]. Participants who received community care were recommended to meet with their physician and were provided with contact information for all local smoking cessation resources, including the New York State Quit Line. All participants were paid $75, and those who provided data at 24 months post-intervention received an additional $5 honorarium.
2.2. Measures
2.2.1. Aspirations
At baseline, participants reported to the treatment facility and completed a battery of questionnaires that included five items from the Aspiration Index [e.g., 9], which assessed their level of importance of aspirations for physical health (viz., To be physically healthy; To feel good about my level of physical fitness; To keep myself healthy and well; To be relatively free from sickness; To have a physically healthy lifestyle). Completion of the Aspiration Index was not required for participants to continue treatment; however, if they did not complete this measure, the portion of their honoraria for completing questionnaires was subtracted. Eighteen months later, participants were mailed a follow-up questionnaire packet that included the same five items from the Aspiration Index. Responses were made on a 7-point Likert-type scale, ranging from 1 (not at all important) to 7 (very important). The Aspiration Index has been used widely in psychological research and, in the current study, the reliability for this measure was α = .87 at baseline and α = .89 at 18 months.
2.2.2. Primary tobacco outcome
The primary outcome was 24-month prolonged abstinence (24mPA) [23] from tobacco, which was assigned if a participant had quit smoking completely at the end of the six-month intervention (with a two week “grace period”)—which was assessed with a biochemically-validated, seven-day point prevalence measure—and had not used tobacco at all (including a pipe, cigars, snuff, and chewing tobacco) between that time and 24 months post-intervention.
2.2.3. Secondary tobacco outcome
The secondary outcome was seven-day point prevalence (7dPP) tobacco abstinence at 24 months post-intervention. Participants responded either “yes” or “no” to the following question: “Have you smoked a cigarette, even a puff, in the past seven days?” Participants also responded either “yes” or “no” to having currently used a pipe, cigars, snuff, or chewing tobacco. To be classified as having attained 7dPP at 24 months post-intervention, participants must have responded “no” to having used each form of tobacco listed above.
2.2.4. Tertiary tobacco outcome
The tertiary outcome was participants' reports of the longest number of days that they had not smoked a cigarette from baseline to 24 months post-intervention.
2.3. Analytic overview
Analyses were performed using “intention-to-treat,” which included all 1,006 participants. Missing data for the importance of aspirations for physical health and the tertiary tobacco outcome were replaced by the participant's last known report; if this was not available, mean replacement was used. If the primary or secondary tobacco outcomes were unavailable, the participant was considered smoking. This analytic technique is considered the standard for biomedical and epidemiological research. Parenthetically, we also conducted analyses without using “intention-to-treat.” Results largely were consistent with those reported herein, although in some cases statistical significance was not reached because of the reduced power.
3. Results
3.1. The effect of treatment condition on maintained importance of aspirations for physical health
At baseline, mean levels of importance of aspirations for physical health were high for both groups [community care: mean (standard deviation) = 6.29 (.89); intervention: mean (standard deviation) = 6.27 (.80)]. Randomization was effective, as groups did not differ on baseline levels of importance of aspirations for physical health, t (1004) = .33, ns. Hypothesis 1 stated that the importance of aspirations for physical health would be maintained better over 18 months by smokers in the SDT-based intervention, relative to those who received community care. To compute change in importance of aspirations for physical health, we regressed 18-month importance of aspirations for physical health onto baseline importance of aspirations for physical health. An independent-samples t-test on the standardized residual score of maintained importance of aspirations for physical health confirmed Hypothesis 1, such that smokers in the SDT-based intervention maintained their high levels of importance of aspirations for physical health (mean change = .05), whereas those who received community care declined in their levels of importance of aspirations for physical health (mean change = -.13), t (1004) = 2.66, p < .01. Thus, the hypothesis that treatment condition would differentially predict maintained importance of aspirations for physical health was supported. The results for Hypothesis 1 are presented in Table 1.
Table 1. Testing Hypothesis 1: The Effect of Treatment Condition on Maintained Importance of Aspirations for Physical Health.
| Intervention | Community Care | t (1004) | |
|---|---|---|---|
| Mean change in importance of aspirations for physical health over 18 months | .05 | -.13 | 2.66** |
Notes. The mean change score is the standardized residual computed by regressing 18-month importance of aspirations for physical health onto baseline importance of aspirations for physical health.
p < .01.
3.2. Mediation analyses
3.2.1. Preliminary analysis
Table 2 presents the intercorrelations among treatment condition, maintained importance of aspirations for physical health, and the three tobacco outcomes. As shown, treatment condition was associated with maintained importance of aspirations for physical health and all three tobacco outcomes, such that smokers in the intervention reported higher maintained importance of aspirations for physical health, likelihood of attaining 24mPA and 7dPP, and the longest number of days not smoking. Moreover, maintained importance of aspirations for physical health was positively associated with all three tobacco outcomes.
Table 2. Associations among Treatment Condition, Maintained Importance of Aspirations for Physical Health, and Tobacco Outcomes at 24 Months Post-intervention.
| Variables | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|
| 1. Treatment condition | ----- | ||||
| 2. Maintained importance of aspirations for physical health | .08** | ----- | |||
| 3. 24-month prolonged abstinence (24mPA) from tobacco | .07* | .12*** | ----- | ||
| 4. Seven-day point prevalence (7dPP) tobacco abstinence | .07* | .07* | .52*** | ----- | |
| 5. Longest number of days not smoking | .11*** | .12*** | .68*** | .65*** | ----- |
p < .05
p < .01
p < .001.
We used mediation analyses to examine Hypothesis 2, which stated that maintained importance of aspirations for physical health would partially mediate the effect of treatment condition on long-term tobacco abstinence. Mediation was tested using the Baron and Kenny [24] method, which specifies four conditions that must be met for mediation: (1) the independent variable (IV) must relate to the dependent variable (DV); (2) the IV must relate to the mediating variable (MV); (3) while controlling for the relation of the IV to the DV, the MV must relate to the DV; and (4) the relation of the IV to the DV must be reduced significantly or to nonsignificance when the MV is added to the model. The results for Hypothesis 2 are presented in Table 3.
Table 3. Testing Hypothesis 2: Mediation of the Effect of Treatment Condition on Long-term Tobacco Abstinence by Maintained Importance of Aspirations for Physical Health.
| Step 1 | Step 2 | Step 3 | Step 4 | z′ | |
|---|---|---|---|---|---|
| 24-month prolonged abstinence (24mPA) from tobacco | b = 1.12* | β = .08** | b = .81*** | b = 1.14* | 2.25** |
| Seven-day point prevalence (7dPP) tobacco abstinence | b = .54* | β = .08** | b = .27* | b = .52* | 1.68** |
| Longest number of days not smoking | β = .11*** | β = .08** | β = .12*** | β = .10** | 2.16** |
Notes. Step 1 refers to the relation of the independent variable (IV) to the dependent variable (DV). Step 2 refers to the relation of the IV to the mediating variable (MV). Step 3 refers to the relation of the MV to the DV while controlling for the IV. Step 4 refers to the relation of the IV to the DV while controlling for the MV. The z′ statistic refers to the significance of the indirect effect of the IV on the DV through the MV.
p < .05
p < .01
p < .001.
3.2.2. Primary analysis using 24mPA
As reported by Williams and his colleagues [17], using logistic regression there was a significant effect of treatment condition on 24mPA [b = 1.12; Wald z (1) = 4.29, p < .05; 95% confidence interval (CI): 1.06, 8.75], thus satisfying Step 1 for mediation. In Step 2, there was a significant effect of treatment condition on maintained importance of aspirations for physical health (β = .08, p < .01). In Step 3, while controlling for the effect of treatment condition, maintained importance of aspirations for physical health related positively to 24mPA [b = .81; Wald z (1) = 16.95, p < .001]. In Step 4, the effect of treatment condition essentially remained unchanged [b = 1.14; Wald z (1) = 4.38, p < .05]. The procedure outlined by MacKinnon, Lockwood, Hoffman, West, and Sheets [25] was used to test the significance of the indirect effect of treatment condition on 24mPA through maintained importance of aspirations for physical health. The z′ test indicated that this indirect effect was significant (z′ = 2.25, p < .01). These results suggest both that treatment condition had a direct effect on 24mPA and that treatment condition had an indirect effect on 24mPA through maintained importance of aspirations for physical health.
3.2.3. Primary analysis using 7dPP
As reported by Williams and his colleagues [17], using logistic regression there was a significant effect of treatment condition on 7dPP [b = .54; Wald z (1) = 4.31, p < .05; 95% CI: 1.03, 2.86], thus satisfying Step 1 for mediation. Step 2 was satisfied, as reported above (β = .08, p < .01). In Step 3, while controlling for the effect of treatment condition, maintained importance of aspirations for physical health related positively to 7dPP [b = .27; Wald z (1) = 5.07, p < .05]. In Step 4, the effect of treatment condition was reduced from b = .54 (p < .05) to b = .52 (p < .05), thus indicating partial mediation of the direct effect. The procedure outlined by MacKinnon and his colleagues [25] was used to test the significance of the mediation of the direct effect of treatment condition on 7dPP by maintained importance of aspirations for physical health. The z′ test indicated that maintained importance of aspirations for physical health was a significant partial mediator of the direct effect (z′ = 1.68, p < .01).
3.2.4. Primary analysis using the longest number of days not smoking
Using linear regression, there was a positive effect of treatment condition on the longest number of days not smoking (β = .11, p < .001), thus satisfying Step 1 for mediation. Step 2 was satisfied, as reported above (β = .08, p < .01). In Step 3, while controlling for the effect of treatment condition, maintained importance of aspirations for physical health related positively to the longest number of days not smoking (β = .12, p < .001). In Step 4, the effect of treatment condition was reduced from β = .11 (p < .001) to β = .10 (p < .01), thus indicating partial mediation of the direct effect. The procedure outlined by MacKinnon and his colleagues [25] was used to test the significance of the mediation of the direct effect of treatment condition on the longest number of days not smoking by maintained importance of aspirations for physical health. The z′ test indicated that maintained importance of aspirations for physical health was a significant partial mediator of the direct effect (z′ = 2.16, p < .01).
3.3. Moderation by treatment condition
Hypothesis 3 stated that the relation of maintained importance of aspirations for physical health to long-term tobacco abstinence would be moderated by treatment condition. First, treatment condition was centered (because the residual score of maintained importance of aspirations for physical health was standardized, it had a mean of zero), and the interaction term was created as the product of these two variables [26]. The results for Hypothesis 3 are presented in Table 4.
Table 4. Testing Hypothesis 3: Moderation of the Relation of Maintained Importance of Aspirations for Physical Health to Long-term Tobacco Abstinence by Treatment Condition.
| 24-month prolonged abstinence (24mPA) from tobacco | Seven-day point prevalence (7dPP) tobacco abstinence | Longest number of days not smoking | ||||
|---|---|---|---|---|---|---|
| Block 1 | Block 2 | Block 1 | Block 2 | Step 1 | Step 2 | |
| Treatment condition | b = 1.14* | b = .52* | β = .10** | |||
| Maintained importance of aspirations for physical health | b = .81** | b = .27* | β = .12*** | |||
| Interaction | b = .82+ | b = .44+ | β = .08* | |||
Notes. In Block 1 (using logistic regression) and Step 1 (using linear regression), the dependent variable was regressed onto the two main effects (viz., treatment condition and maintained importance of aspirations for physical health). In Block 2 (using logistic regression) and Step 2 (using linear regression), the interaction of the two main effects was added to the equation.
p < .10
p < .05
p < .01
p < .001.
3.3.1. Primary analysis using 24mPA
Using logistic regression, in block 1, 24mPA was regressed onto treatment condition and maintained importance of aspirations for physical health. The overall model was significant, χ2 (2) = 21.55, p < .001. As expected, treatment condition related positively to 24mPA [b = 1.14; Wald z (1) = 4.38, p < .05]. In addition, maintained importance of aspirations for physical health related positively to 24mPA [b = .81; Wald z (1) = 16.95, p < .001]. In block 2, the interaction term was added to the equation. The overall model was significant, χ2 (3) = 23.91, p < .001, and the interaction term was a marginal predictor of 24mPA [b = .82; Wald z (1) = 2.83, p = .09], such that smokers who received the intervention and had maintained their level of importance of aspirations for physical health had the highest likelihood of attaining 24mPA. Examining the simple slopes of this marginally-significant interaction, in the intervention condition there was a significant positive relation of maintained importance of aspirations for physical health to 24mPA [b = .93; Wald z (1) = 19.61, p < .001], whereas in the community care condition this relation was much weaker and not significant [b = .12; Wald z (1) = .07, ns].
3.3.2. Primary analysis using 7dPP
Using logistic regression, in block 1, 7dPP was regressed onto treatment condition and maintained importance of aspirations for physical health. The overall model was significant, χ2 (2) = 10.04, p < .01. As expected, treatment condition related positively to 7dPP [b = .52; Wald z (1) = 3.91, p < .05]. In addition, maintained importance of aspirations for physical health related positively to 7dPP [b = .27, Wald z (1) = 5.07, p < .05]. In block 2, the interaction term was added to the equation. The overall model was significant, χ2 (3) = 13.28, p < .01, and the interaction term was a marginal predictor of 7dPP [b = .44; Wald z (1) = 3.55, p = .06], such that smokers who received the intervention and had maintained their level of importance of aspirations for physical health had the highest likelihood of attaining 7dPP. Examining the simple slopes of this marginally-significant interaction, in the intervention condition there was a significant positive relation of maintained importance of aspirations for physical health to 7dPP [b = .43; Wald z (1) = 8.40, p < .01], whereas in the community care condition this relation was much weaker and not significant [b = -.01; Wald z (1) = .00, ns].
3.3.3. Primary analysis using the longest number of days not smoking
Using linear regression, in step 1, the longest number of days not smoking was regressed onto treatment condition and maintained importance of aspirations for physical health. The overall model was significant, F (2, 1003) = 12.45, p < .001. As expected, treatment condition related positively to the longest number of days not smoking (β = .10, p < .01). In addition, maintained importance of aspirations for physical health related positively to the longest number of days not smoking (β = .12, p < .001). In step 2, the interaction term was added to the equation, and the overall model for this step was significant, F (1, 1002) = 5.46, p < .05. As hypothesized, the interaction of treatment condition and maintained importance of aspirations for physical health related positively to the longest number of days not smoking (β = .08, p < .05), such that smokers who received the intervention and had maintained their level of importance of aspirations for physical health reported the longest number of days not smoking since beginning the study. Examining the simple slopes of this significant interaction, in the intervention condition there was a significant positive relation of maintained importance of aspirations for physical health to the longest number days not smoking (β = .19, b = 38.56, p < .001), whereas in the community care condition this relation was much weaker and not significant (β = .04, b = 8.32, ns). This interaction effect is displayed in Figure 2.
Figure 2.
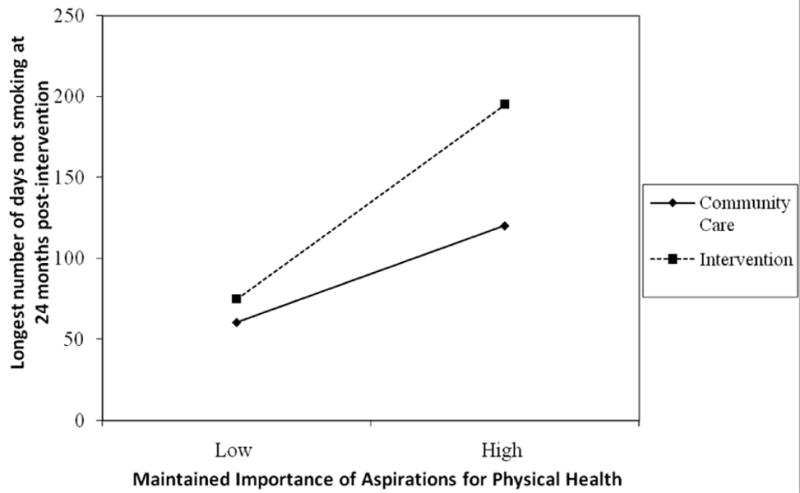
Interaction of treatment condition and maintained importance of aspirations for physical health related to the longest number of days not smoking at 24 months post-intervention.
4. Discussion and conclusion
4.1. Discussion
Data for the current study were collected in the context of a smokers' health study designed to examine the effects of providing an intervention for smokers that focused on supporting autonomous self-regulation for smoking cessation, in part by eliciting and discussing how smoking related to smokers' aspirations. In this report, we examined the antecedents and consequences of maintained importance of aspirations for physical health. We found support for our hypotheses, which we discuss below.
First, although participants reported high mean levels of importance of aspirations for physical health upon entry into the study (6.28 on a 7-point scale), only those who received the SDT-based intervention maintained their level of importance of aspirations for physical health over 18 months, whereas those who received community care reported a decline in their level of importance of aspirations for physical health over time. This finding is important because it demonstrates that, when smokers discuss their life aspirations and the ways in which they believe smoking helps and/or hinders their attaining those goals in the context of interpersonal supports for autonomy, they are more likely to maintain their high level of importance of aspirations for physical health, which is associated with psychological need satisfaction and various indices of health (see, e.g., 12).
Second, we hypothesized that maintained importance of aspirations for physical health would partially mediate the effect of treatment condition on long-term tobacco abstinence. In other words, we expected that better maintained importance of aspirations for physical health would account for some, although not all, of the treatment effects. We found that the SDT-based intervention related positively to maintained importance of aspirations for physical health, which in turn related positively to health-behavior change while controlling for the effect of treatment condition. However, because the effect of treatment condition on 24mPA was unchanged while controlling for maintained importance of aspirations for physical health (the presumed mediator), we concluded both that treatment condition had a direct effect on 24mPA and that treatment condition had an indirect effect on 24mPA through maintained importance of aspirations for physical health. In contrast, maintained importance of aspirations for physical health partially mediated the effects of treatment condition on both 7dPP and the longest number of days not smoking at 24 months post-intervention. Thus, the effect of treatment condition on maintained importance of aspirations for physical health accounted for some of the direct effects of treatment condition on the tobacco outcomes.
Third, we hypothesized that the relation of maintained importance of aspirations for physical health to health-behavior change would be moderated by treatment condition. Specifically, we expected that the salubrious relations of maintained importance of aspirations for physical health to long-term tobacco abstinence would be enhanced among those who received the SDT-based intervention because such a context elicited a consideration how health-behavior change may affect smokers' life aspirations while providing support for autonomy. We found evidence of moderation only on the longest number of days not smoking, thus providing partial support for our hypothesis. It should be noted, however, that the moderation effect also approached statistical significance in predicting 24mPA and 7dPP. Thus, these results suggest that the SDT-based intervention functioned to amplify the positive relation of maintained importance of aspirations for physical health to long-term tobacco abstinence at 24 months post-intervention.
4.2. Limitations
There were several limitations to the current study. First, because aspirations are only one component of patients' motivation, the strength of the associations among the study variables was small in magnitude. We caution against overgeneralization from these results and urge others to replicate and extend this line of research. Second, the pattern of results was more in line with study hypotheses when we assessed the continuous tobacco outcome. One possible explanation for the weaker pattern of findings when the dichotomous outcomes were assessed is that only 3.3% and 9.9% of the sample were classified as having attained 24mPA and 7dPP, respectively. Thus, there was only a small amount of variance to be accounted for in the dichotomous outcomes. Accordingly, we suggest that more research examine the impact of maintained importance of aspirations for physical health on those and other health outcomes.
4.3. Conclusion
Overall, these results suggest that, in addition to the primary objective of the intervention (i.e., facilitating autonomous self-regulation for smoking cessation; 16), the intervention also functioned to enhance smokers' ability to effectively utilize the innate energy of their aspirations for physical health to facilitate health-behavior change (viz., tobacco abstinence). That is, it appears that those who received the SDT-based intervention were more likely to maintain their level of importance of aspirations for physical health. Importantly, maintained importance of aspirations for physical health had a unique relation to long-term tobacco abstinence and interacted with the SDT-based intervention to enhance long-term tobacco abstinence. The findings thus point to the potential usefulness of specifically eliciting and discussing the relevance of life aspirations as they relate to health-behavior change within a structured intervention. It appears that, in the context of supports for autonomy, eliciting and discussing life aspirations may help to motivate individuals toward positive health-behavior change by maintaining a stronger value for their health.
4.4. Practice implications
Tobacco use is the leading cause of death in the United States [27, cf. 17] and thus presents a major threat to optimal health and well-being. Practitioners often discuss smoking with patients during health-care visits; however, practitioners may relate to their patients in ways that are perceived to be relatively controlling or relatively autonomy-supportive. The results of the current study suggest that smokers have a greater likelihood of attaining long-term abstinence from tobacco when practitioners explicitly ask patients to name two or three important life aspirations and to discuss how they believe continuing to smoke or quitting may facilitate or inhibit their attaining those goals. We believe it is important for practitioners to remain non-judgmental with respect to patients' life aspirations and to how patients perceive their smoking as affecting those goals because such an orientation provides a context that is supportive of smokers' autonomy and thus is facilitative of the process of internalization, through which smokers come to identify with the value of smoking cessation and experience volition in their regulation of health-behavior change. Importantly, autonomous self-regulation for smoking cessation, which results from the process of internalization, is known to facilitate tobacco abstinence [21].
Acknowledgments
This research was supported in part by grants from the National Institute of Mental Health (R01-MH59594) and the National Cancer Institute (R01-CA106668). Address correspondence concerning this article to Christopher P. Niemiec, Department of Clinical and Social Sciences in Psychology, Box 270266, University of Rochester, Rochester, NY 14627; Email: niemiec@psych.rochester.edu
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Trial Registration. ClinicalTrials.gov number, NCT00178685
References
- 1.Ryan RM, Sheldon KM, Kasser T, Deci EL. All goals are not created equal: an organismic perspective on the nature of goals and their regulation. In: Gollwitzer PM, Bargh JA, editors. The psychology of action: linking cognition and motivation to behavior. New York: Guilford Press; 1996. pp. 7–26. [Google Scholar]
- 2.Grouzet FME, Kasser T, Ahuvia A, Dols JMF, Kim Y, Lau S, et al. The structure of goal contents across 15 cultures. J Pers Soc Psychol. 2005;89:800–16. doi: 10.1037/0022-3514.89.5.800. [DOI] [PubMed] [Google Scholar]
- 3.Niemiec CP, Ryan RM, Deci EL. The path taken: consequences of attaining intrinsic and extrinsic aspirations in post-college life. Poster presented at the meeting of the Society for Personality and Social Psychology; New Orleans. January, 2005; [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Sheldon KM, Kasser T. Coherence and congruence: two aspects of personality integration. J Pers Soc Psychol. 1995;68:531–43. doi: 10.1037//0022-3514.68.3.531. [DOI] [PubMed] [Google Scholar]
- 5.Deci EL, Ryan RM. The “what” and “why” of goal pursuits: human needs and the self-determination of behavior. Psychol Inq. 2000;11:227–68. [Google Scholar]
- 6.Ryan RM, Deci EL. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am Psychol. 2000;55:68–78. doi: 10.1037//0003-066x.55.1.68. [DOI] [PubMed] [Google Scholar]
- 7.Niemiec CP, Ryan RM, Deci EL. Self-determination theory and the relation of autonomy to self-regulatory processes and personality development. In: Hoyle RH, editor. Handbook of personality and self-regulation. New York: Wiley-Blackwell; in press. [Google Scholar]
- 8.Kasser T, Ryan RM. A dark side of the American dream: correlates of financial success as a central life aspiration. J Pers Soc Psychol. 1993;65:410–22. doi: 10.1037//0022-3514.65.2.410. [DOI] [PubMed] [Google Scholar]
- 9.Kasser T, Ryan RM. Further examining the American dream: differential correlates of intrinsic and extrinsic goals. Pers Soc Psychol Bull. 1996;22:280–87. [Google Scholar]
- 10.Kasser T, Ryan RM. Be careful what you wish for: optimal functioning and the relative attainment of intrinsic and extrinsic goals. In: Schmuck P, Sheldon KM, editors. Life goals and well-being: towards a positive psychology of human striving. Seattle: Hogrefe & Huber Publishers; 2001. pp. 116–31. [Google Scholar]
- 11.Sheldon KM, Ryan RM, Deci EL, Kasser T. The independent effects of goal contents and motives on well-being: it's both what you pursue and why you pursue it. Pers Soc Psychol Bull. 2004;30:475–86. doi: 10.1177/0146167203261883. [DOI] [PubMed] [Google Scholar]
- 12.Vansteenkiste M, Neyrinck B, Niemiec CP, Soenens B, de Witte H, Van den Broeck A. On the relations among work value orientations, psychological need satisfaction and job outcomes: a self-determination theory approach. Journal of Occupational and Organizational Psychology. 2007;80:251–77. [Google Scholar]
- 13.Williams GC, Cox EM, Hedberg VA, Deci EL. Extrinsic life goals and health-risk behaviors in adolescents. J Appl Soc Psychol. 2000;30:1756–71. [Google Scholar]
- 14.Reifman A, Barnes GM, Dintcheff BA, Uhteg L, Farrell MP. Health values buffer social-environmental risks for adolescent alcohol misuse. Psychol Addict Behav. 2001;15:249–51. [PubMed] [Google Scholar]
- 15.Shi HJ, Nakamura K, Takano T. Health values and health-information-seeking in relation to positive change of health practice among middle-aged urban men. Prev Med. 2004;39:1164–71. doi: 10.1016/j.ypmed.2004.04.030. [DOI] [PubMed] [Google Scholar]
- 16.Williams GC, Minicucci DS, Kouides RW, Levesque CS, Chirkov VI, Ryan RM, et al. Self-determination, smoking, diet and health. Health Educ Res. 2002;17:512–21. doi: 10.1093/her/17.5.512. [DOI] [PubMed] [Google Scholar]
- 17.Williams GC, Niemiec CP, Patrick H, Ryan RM, Deci EL. The importance supporting autonomy in facilitating long-term tobacco abstinence. Paper presented at the meeting of the Health Maintenance Consortium; Washington DC. October, 2006. [Google Scholar]
- 18.National Cholesterol Education Program (NCEP) Cholesterol lowering in the patient with coronary heart disease: physician monograph. NIH Publication No. 97-3794. Bethesda, MD: Institutes of Health, National Heart, Lung, and Blood Institute; 1997. [Google Scholar]
- 19.Williams GC, McGregor H, Sharp D, Kouides RW, Lévesque CS, Ryan RM, et al. A self-determination multiple risk intervention trial to improve smokers' health. J Gen Intern Med. 2006;21:1288–94. doi: 10.1111/j.1525-1497.2006.00621.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Fiore MC, Bailey WC, Cohen SJ, Dorfman SF, Goldstein MG, Gritz ER, et al. Treating tobacco use and dependence. Rockville, MD: U.S. Department of Health and Human Services (DHHS); 2000. [Google Scholar]
- 21.Williams GC, McGregor HA, Sharp D, Levesque C, Kouides RW, Ryan RM, et al. Testing a self-determination theory intervention for motivating tobacco cessation: supporting autonomy and competence in a clinical trial. Health Psychol. 2006;25:91–101. doi: 10.1037/0278-6133.25.1.91. [DOI] [PubMed] [Google Scholar]
- 22.Williams GC, Deci EL, Ryan RM. Building health-care partnerships by supporting autonomy: promoting maintained behavior change and positive health outcomes. In: Suchman AL, Hinton-Walker P, Botelho R, editors. Partnerships in healthcare: transforming relational process. Rochester, NY: University of Rochester Press; 1998. pp. 67–87. [Google Scholar]
- 23.Hughes JR, Keely JP, Niaura RS, Ossip-Klein DJ, Richmond RL, Swan GE. Measures of abstinence in clinical trials: issues and recommendations. Nicotine Tob Res. 2003;5:13–25. [PubMed] [Google Scholar]
- 24.Baron RM, Kenny DA. The moderator-mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. J Pers Soc Psychol. 1986;51:1173–82. doi: 10.1037//0022-3514.51.6.1173. [DOI] [PubMed] [Google Scholar]
- 25.MacKinnon DP, Lockwood CM, Hoffman JM, West SG, Sheets V. A comparison of methods to test mediation and other intervening variable effects. Psychol Methods. 2002;7:83–104. doi: 10.1037/1082-989x.7.1.83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Aiken LS, West SG. Multiple regression: testing and interpreting interactions. Newbury Park, CA: Sage; 1991. [Google Scholar]
- 27.Mokdad AH, Marks JS, Stroup DF, Gerberding JL. Actual causes of death in the United States, 2000. J Am Med Assoc. 2004;291:1238–45. doi: 10.1001/jama.291.10.1238. [DOI] [PubMed] [Google Scholar]