

Abstract
AIM: To investigate in vitro effects of propofol, midazolam and dexmedetomidine, which are commonly used anaesthesic or sedatives, on spontaneous contractions of the ileum both in normal rats and those exposed to hyperdynamic peritonitis.
METHODS: Spontaneous contractions of isolated ileum muscle segments from sham operated rats and those exposed to peritonitis, were studied in vitro. The amplitude and the frequency of spontaneous contractions of ileum muscle segments were studied after adding dexmetetomidine, propofol, and midazolam to the organ bath in a cumulative manner.
RESULTS: Both amplitude (85.2 ± 6.6 vs 47.4 ± 7.1) and frequency (32.8 ± 4.6 vs 20.2 ± 3.9) of spontaneous contractions in ileum smooth muscle segments were decreased significantly in the peritonitis group compared to the control group (P < 0.05). Dexmedetomidine significantly increased the amplitude of spontaneous contractions (85.2 ± 6.6 vs 152.0 ± 5.4, P < 0.05) whereas, propofol (85.2 ± 6.6 vs 49.6 ± 4.8, P < 0.05) and midazolam (85.2 ± 6.6 vs 39.2 ± 4.5, P < 0.05) decreased it in both control and peritonitis groups. The frequency of spontaneous contractions were significantly decreased by propofol in both control (32.8 ± 4.6 vs 18.2 ± 3.4, P < 0.05) and peritonitis groups 20.2 ± 3.9 vs 11.6 ± 3.2, P < 0.05). Dexmedetomidine and midazolam did not cause significant changes in the number of spontaneous contractions in both control and the peritonitis groups (P > 0.05).
CONCLUSION: Propofol, midazolam and dexmede-tomidine have various in vitro effects on spontaneous contractions of the rat ileum. While dexmedetomidine augments the spontaneous contraction of the rat ileum, propofol attenuates it. However, the effects of these compounds were parallel in both control and peritonitis groups.
Keywords: Ileum, Propofol, Midazolam, Dexmedeto-midine, Peritonitis
INTRODUCTION
Dysmotility of the gastrointestinal tract is a major complication in critically ill patients in intensive care units. Most of the time, this dysmotility manifests itself as inhibition of gastrointestinal motility, and rarely as hypermotility[1]. Hypomotility can cause a functional, nonmechanical obstruction, most commonly an adynamic ileus. Impaired motility in critically ill patients can be caused by intestinal ischemia, electrolyte imbalances, peritoneal injury, abdominal surgery, lower-lobe pneumonia, pancreatitis, cholecystitis, intraabdominal abscesses, and medications (opiates, dopamine, diltiazem, verapamil, and anticholinergics)[2]. Sedatives such as propofol and midazolam further inhibit delayed intestinal transit in critically ill patients in a dose dependent manner. The delay may cause complications such as intolerance to enteral feeding and overgrowth of bacteria in the gastrointestinal tract resulting in increase the incidence of aspiration pneumonitis[3].
Abdominal sepsis or peritonitis is also a major cause of morbidity and mortality in surgical intensive care units. Gastrointestinal dysmotility commonly accompany peritonitis and those patients suffering peritonitis are also exposed to the additive effects of sedatives or anesthetics in surgical intensive care units. Koyluoglu et al[4] recently demonstrated that peritonitis induced a decrease in the amplitude and frequency of spontaneous contractions of ileum and jejunum segments from rats. Therefore, it is preferable to use a sedative or an anaesthetic that has few inhibitory effects on gastrointestinal transit in patients with peritonitis. However, there has been little study on this topic in the literature. In the present study, we aimed to investigate in vitro effects of propofol, midazolam and dexmedetomidine on spontaneous contractions of the ileum both in normal rats and those are exposed to hyperdynamic peritonitis.
MATERIALS AND METHODS
Animal preparation
Sixteen male Wistar albino rats each weighing approximately 280 g were used in this study. The study was approved by the ethics committee of Cumhuriyet University School of Medicine. Cecal ligation and puncture were used as the peritonitis model[5]. Animals were divided into two groups. The first group consisted of sham surgical controls that underwent the same procedure as the peritonitis group, such that laparotomy was performed under anesthesia, with manipulation of the cecum, but cecum ligation and puncture were not performed. Rats in the second group underwent cecal puncture and ligation as previously described by Martin et al[5]. Animals were anesthetized with intramuscular injections of 3 mg/kg xylazine (Rompun®, Bayer, Istanbul, Turkey) and 90 mg/kg ketamine (Ketalar®, Pfizer, Istanbul, Turkey), following which, laparotomy was performed via a 2 cm midline incision and the cecum was exposed. The cecum was ligated using 4/0 silk suture material just below the ileocecal valve, so that intestinal continuity was maintained. Then, the cecum was punctured using an 18-gauge needle in three locations, 1 cm apart, on the antimesenteric surface of the cecum, and cecum was gently compressed until feces were extruded. The cecum was replaced into the peritoneal cavity and the abdomen was then closed. When the animals were alert, they were transferred to single housing cages where they were left with ad libitum food and water. We then observed the rats in a recovery cage for 24 h.
A summary of the experimental treatments is presented below: Groups: Group I (n = 8): Sham surgical controls; Group II (n = 8): Peritonitis group.
At the second laparotomy, 24 h later, the rats were killed by cervical dislocation. The abdomen was opened with a midline incision and the ileum was removed and placed in previously aerated (95% O2 and 5% CO2) Krebs-bicarbonate solution (composition in mmol/L: NaCl, 120; KCl, 4.6; CaCl2, 2.5; MgCl2, 1.2; NaHCO3, 22; NaH2PO4 and glucose 11.5). Whole full-thickness segments of ileum were placed in circular direction in a 10 mL tissue baths, filled with pre-aerated Krebs-bicarbonate solution (KBS) at 37°C. The upper end of the preparation was tied to an isometric transducer (Grass FT 03, Quincy, MA, USA) and preloaded with 1-1.5 g. Tissues were allowed to equilibrate for 30 min.
In vitro muscle contractility studies
Muscle segments from each group were contracted with 80 mmol/L KCl to ensure that they worked properly at the beginning and end of each experiment.
At the beginning of each experiment, 80 mmol/L KCl was added to the organ bath, and the contraction was considered as reference response. Subsequently, the amplitude of spontaneous contractions of the isolated ileum muscle segments were calculated as a percentage of the contraction induced by KCl (80 mmol/L) from both control and peritonitis groups. Changes in the frequency (number/min.) of spontaneous contractions were expressed as the number of contractions for 10 min intervals.
Following the KCl response, smooth muscle segments were allowed to equilibrate for 30 min before addition of cumulative doses of propofol (10-8-10-4 mol/L), midazolam (10-8-10-4 mol/L) and dexmedetomidine (10-8-10-4 mol/L). Amplitudes of the contractions induced by these compounds from both control and peritonitis groups were calculated as the percentage of the initial spontaneous contractions. Changes in the frequency of spontaneous contractions were expressed as the number of spontaneous contractions for 10 min after drug application. Isometric tensions were recorded on a Grass model 79 E polygraph. All experiments were performed in duplicate.
Drugs
The following compounds were used: Propofol (2,6diisopropylphenol®, Aldrich Chemicals Co., USA), Midazolam (Midazolam hydrochloride®, Sigma, St Louis, USA), Dexmedetomidine (Abbot Laboratories, Abbot Park, IL, USA). All drugs were dissolved in distilled water. All drugs were freshly prepared on the day of the experiment.
Data analysis
All data are expressed as mean ± SD. Statistical comparisons between groups were performed using general linear models of analysis of variance (ANOVA) followed by the Newman-Keuls test and a t test when appropriate and P-values of less than 0.05 were considered to be statistically significant.
RESULTS
Contractions induced by 80 mmol/L KCl were not significantly different between the peritonitis group and the control group in isolated ileum smooth muscle segments which indicated that muscle segments from both groups worked properly (Figure 1).
Figure 1.
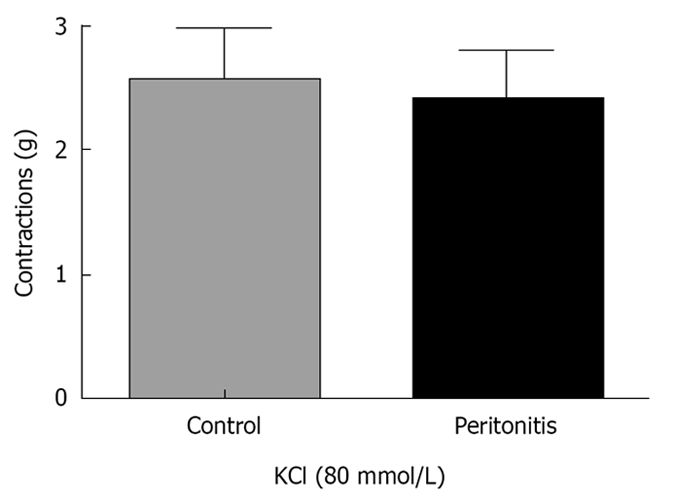
KCl (80 mmol/L) induced contractions of isolated ileum muscle segments in control and peritonitis groups. No statistical difference was observed between groups (P > 0.05).
The mean amplitude of the spontaneous contractions was 85.2 ± 6.6 in the control and 47.4 ± 7.1 in the peritonitis group, respectively. The number of spontaneous contractions obtained in 10 min in the peritonitis group was 32.8 ± 4.6 and 20.2 ± 3.9 in the control group. Both the amplitude and the frequency of spontaneous contractions of ileum smooth muscle segments were decreased significantly in the peritonitis group compared to the control group (P < 0.05), (Figure 2A and B).
Figure 2.
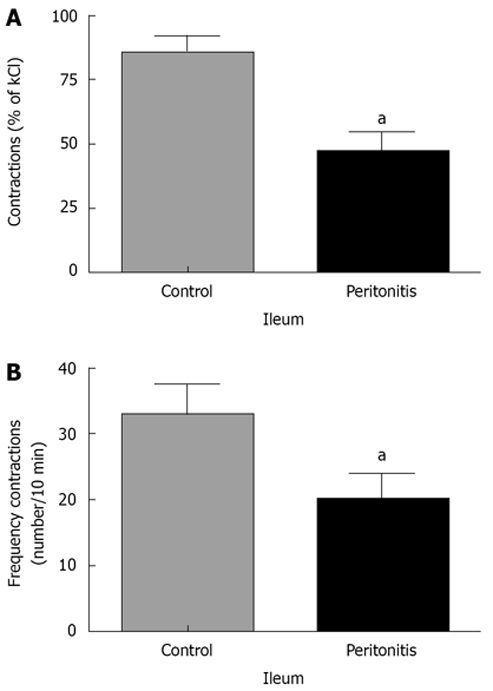
Changes in the spontaneous contractions of the isolated ileum muscle segments. A: Amplitudes were calculated as a percentage of the contraction induced by KCl (80 mmol/L) from both control and peritonitis groups; B: Frequencies were expressed as the number of contractions for 10 min from both control and peritonitis groups. (aP < 0.05 vs control group; analysis of variance followed by Newman-Keuls test).
The amplitudes of spontaneous contractions of ileum muscle segments were studied after adding dexmetetomidine, propofol, and midazolam to the organ bath. Dexmedetomidine (10-8-10-4 mol/L) significantly increased the amplitude of spontaneous contractions starting from 10-7 mol/L in isolated ileum muscle segments, in both the control and peritonitis groups, in a concentration-dependent manner. Propofol (10-8-10-4 mol/L) and midazolam (10-8-10-4 mol/L) decreased the amplitude of spontaneous contractions starting from 10-7 mol/L as the molar concentrations of these drugs were increased (P < 0.05). However, there was no statistical difference between the decreasing effects of propofol and midazolam (P > 0.05), (Figure 3A and B), (Tables 1 and 2).
Figure 3.
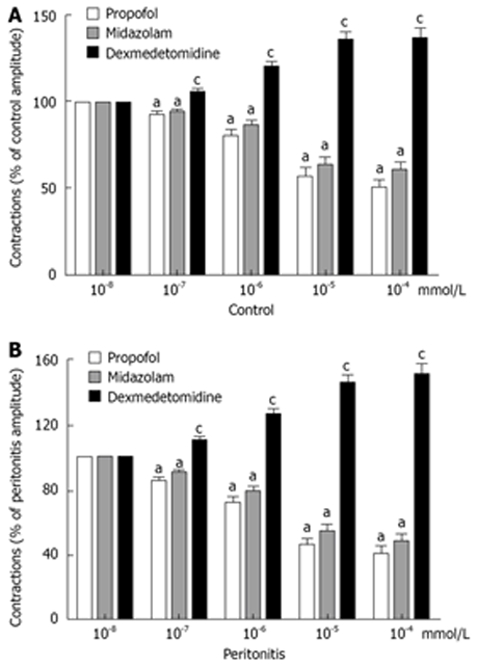
Amplitudes of the contractions induced by anaesthetic agents. A: Control group; B: Peritonitis group; both were calculated as the percentage of the initial contractions. (aP < 0.05 vs initial contractions, cP < 0.05 vs propofol and midazolam; analysis of variance followed by Newman-Keuls test).
Table 1.
Effects of Propofol, midazolam and dexmedetomidine on spontaneous contractions in experiment groups
| Control | Peritonitis | |
| Amplitude (%)1 | 85.2 ± 6.6 (100) | 47.4 ± 7.1a (100) |
| Propofol | 49.6 ± 4.8b | 59.4 ± 5.2b |
| Midazolam | 39.2 ± 4.5b | 51.8 ± 5.0b |
| Dexmedetomidine | 136.6 ± 5.8bc | 152.0 ± 5.4bc |
| Frequency (#/10 min) | 32.8 ± 4.6 | 20.2 ± 3.9a |
| Propofol | 18.2 ± 3.4b | 11.6 ± 3.2b |
| Midazolam | 28.2 ± 3.8 | 17.4 ± 3.0 |
| Dexmedetomidine | 36.2 ± 4.0 | 22.2 ± 3.1 |
Amplitudes of the contractions induced by anesthetic agents from both control and peritonitis groups were calculated as the percentage of the initial spontaneous contractions;
P < 0.05 vs control;
P < 0.05 vs initial spontaneous contractions;
P < 0.05 vs propofol and midazolam.
Table 2.
Effects of Propofol, midazolam and dexmedetomidine on amplitude and frequency of the spontaneous contractions
| Amplitude | Frequency | |
| Propofol | Decreased | Decreased |
| Midazolam | Decreased | No significant change |
| Dexmedetomidine | Increased | No significant change |
The frequency of spontaneous contractions of the ileum segments were significantly decreased by cumulative doses of propofol (10-8-10-4 mol/L) in both the control and peritonitis groups (P < 0.05). Dexmedetomidine (10-8-10-4 mol/L) and midazolam (10-8-10-4 mol/L) did not cause a significant change in the number of spontaneous contractions of the isolated ileum muscle segments in both the control and peritonitis groups (P > 0.05) (Figure 4A and B) (Tables 1 and 2).
Figure 4.
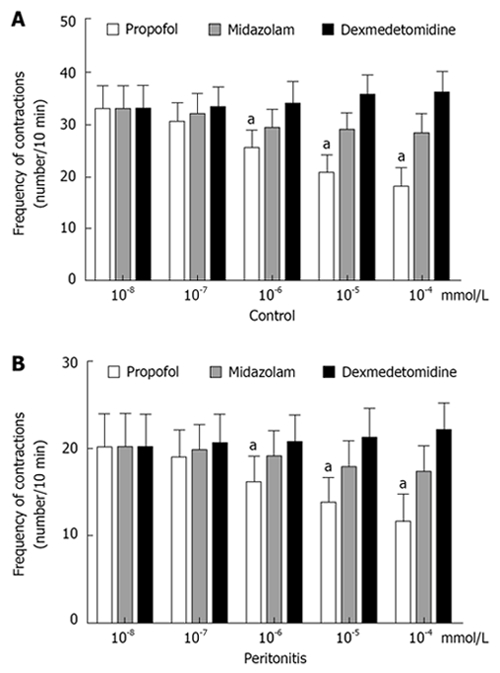
Changes in the frequency of spontaneous contractions. A: Control group; B: Peritonitis group. Both were expressed as the number of contractions for 10 min. (aP < 0.05 vs initial contractions; analysis of variance followed by Newman-Keuls test).
DISCUSSION
The first finding of our study is that peritonitis altered the spontaneous activity of the rat ileum by decreasing both the amplitude and the frequency of the contractions in accordance with the previous study reported recently by Koyluoglu et al[4]. The main findings are that dexmedetomidine, a selective alpha2-adrenergic agonist, increased the amplitude, midazolam decreased the amplitude and propofol decreased both the amplitude and frequency of the spontaneous contractions in rat ileum in a concentration-dependent manner in both the control and peritonitis groups. Liu et al[6] reported that the alpha2-adrenoceptors inhibited neurogenic contractions of the rat ileum. Dexmedetomidine inhibited peristalsis in the guinea pig small intestine in vitro in a concentration dependent manner[7]. Dexmedetomidine strongly inhibited intestinal transit in the rat, however this inhibition was less potent than morphine[8]. However, in our study, dexmedetomidine, when applied in a concentration dependent manner significantly increased the amplitude but did not change the frequency of spontaneous contractions in the rat ileum in vitro both in the control and peritonitis groups. Our result seems to contradict previous reports. However, similarly to our results, Karaman et al[9] showed that dexmedetomidine in vitro caused a significant increase in the amplitude and frequency of spontaneous contractions in rat myometrium in a dose-dependent manner. The augmenting effect of this agent on spontaneous contractions needs to be investigated further.
Lee et al[10] demonstrated that propofol has an in vitro inhibitory effect on spontaneous contractile activity and causes acetylcholine induced contractions of human gastric and colonic smooth muscles at clinically relevant concentrations. It was demonstrated in a previous study that propofol, at concentrations of 10-7 and 10-6 mol/L, potentiated the guinea pig ileum contractile responses to g-aminobutyric acid (GABA), but only at the lower dose range of applied GABA; at a concentration of 10-5 mol/L, it inhibited the contractile effect over the entire dose range of applied GABA[11]. In the present study, propofol decreased both amplitude and frequency of contractions of rat ileum muscle segments in the control and peritonitis groups. Previous studies have reported the relaxant effects of propofol on other smooth muscle tissues such as vascular[12] and uterine smooth muscles[13]. The action of propofol involves a positive modulation of the inhibitory function of the neurotransmitter GABA through GABA A receptors[14]. Jensen et al[15] evaluated the influences of propofol, nitrous oxide and isoflurane and found that recovery and postoperative bowel function were not influenced by the anaesthetic technique after major gastrointestinal surgery. However, it might be different in case of a critically ill patient with peritonitis in an intensive care unit. The combined inhibitory effects of peritonitis and propofol might further slow intestinal transit and lead to an adynamic ileus.
Like other benzodiazepines, midazolam acts on the benzodiazepine binding site of GABA A receptors. When bound, it enhances the binding of GABA to the GABA A receptor, resulting in inhibitory effects on the central nervous system[16]. Castedal et al[17] reported in their manometric study that midazolam had relatively few effects on small bowel motility. In the present study, midazolam decreased the amplitude but caused very little change in the frequency of ileum contractions. Midazolam is often used for intravenous conscious sedation in endoscopic retrograde cholangiopancreatography (ERCP). Midazolam significantly altered the mobility of the sphincter of Oddi and caused a significant reduction in basal pressure of the sphincter of Oddi but did not affect the phasic frequency[18].
In conclusion, dexmedetomidine, midazolam and propofol have various in vitro effects on spontaneous contractions of the rat ileum. While dexmedetomidine augments the spontaneous contraction of the rat ileum, propofol attenuates it. The effects of these agents were parallel in both control and peritonitis groups. The clinical implications of these findings need to be tested in surgical intensive care units, which might help in choosing the most appropriate drug for the sedation of patients with peritonitis.
COMMENTS
Background
Gastrointestinal dysmotility commonly accompanies peritonitis and those patients suffering peritonitis are also exposed to the additive effects of sedatives or anaesthetics in surgical intensive care units. Therefore, it is preferable to use a sedative or an anaesthetic that has few inhibitory effects on gastrointestinal transit in the patients with peritonitis. The in vitro effects of propofol, midazolam and dexmedetomidine, which are commonly used anaesthesic or sedatives, are worth investigating for that purpose.
Research frontiers
The first finding of the study is that peritonitis altered the spontaneous activity of the rat ileum by decreasing both the amplitude and the frequency of the contractions. The main findings are that dexmedetomidine increased the amplitude, midazolam decreased the amplitude and propofol decreased both the amplitude and frequency of the spontaneous contractions of the rat ileum in a concentration-dependent manner in both the control and peritonitis groups.
Innovations and breakthroughs
In this study, the in vitro effects of dexmedetomidine, midazolam and propofol on spontaneous contractions of ileum muscle in rats exposed to peritonitis were demonstrated.
Applications
These findings will aid the selective use of sedatives or anaesthetics that have fewer inhibitory effects on gastrointestinal transit in patients with peritonitis.
Peer review
The authors of the present study have compared the acute effects of different sedatives or anaesthetics on the spontaneous contractions in the ileum of sham-operated rats and rats with peritonitis. The amplitude and the frequency of the spontaneous contractions were affected to a different extent by the respective sedatives. This study was well performed.
Peer reviewer: Inge I Depoortere, PhD, Centre for Gastroenterological Research, Gasthuisberg OandN, bus 701, Leuven 3000, Belgium.
S- Editor Tian L L- Editor Stewart GJ E- Editor Yin DH
References
- 1.Ritz MA, Fraser R, Tam W, Dent J. Impacts and patterns of disturbed gastrointestinal function in critically ill patients. Am J Gastroenterol. 2000;95:3044–3052. doi: 10.1111/j.1572-0241.2000.03176.x. [DOI] [PubMed] [Google Scholar]
- 2.Martin B. Prevention of gastrointestinal complications in the critically ill patient. AACN Adv Crit Care. 2007;18:158–166. doi: 10.1097/01.AACN.0000269259.91546.d8. [DOI] [PubMed] [Google Scholar]
- 3.Inada T, Asai T, Yamada M, Shingu K. Propofol and midazolam inhibit gastric emptying and gastrointestinal transit in mice. Anesth Analg. 2004;99:1102–1106, table of contents. doi: 10.1213/01.ANE.0000130852.53082.D5. [DOI] [PubMed] [Google Scholar]
- 4.Koyluoglu G, Bagcivan I, Karadas B, Guney C, Durmus N, Altun A, Kaya T. Alterations in spontaneous contractions of rat ileum and jejunum after peritonitis. Eur J Pharmacol. 2008;580:250–255. doi: 10.1016/j.ejphar.2007.10.064. [DOI] [PubMed] [Google Scholar]
- 5.Martin CM, Yaghi A, Sibbald WJ, McCormack D, Paterson NA. Differential impairment of vascular reactivity of small pulmonary and systemic arteries in hyperdynamic sepsis. Am Rev Respir Dis. 1993;148:164–172. doi: 10.1164/ajrccm/148.1.164. [DOI] [PubMed] [Google Scholar]
- 6.Liu L, Coupar IM. Characterisation of pre- and post-synaptic alpha-adrenoceptors in modulation of the rat ileum longitudinal and circular muscle activities. Naunyn Schmiedebergs Arch Pharmacol. 1997;356:248–256. doi: 10.1007/pl00005048. [DOI] [PubMed] [Google Scholar]
- 7.Herbert MK, Roth-Goldbrunner S, Holzer P, Roewer N. Clonidine and dexmedetomidine potently inhibit peristalsis in the Guinea pig ileum in vitro. Anesthesiology. 2002;97:1491–1499. doi: 10.1097/00000542-200212000-00022. [DOI] [PubMed] [Google Scholar]
- 8.Asai T, Mapleson WW, Power I. Differential effects of clonidine and dexmedetomidine on gastric emptying and gastrointestinal transit in the rat. Br J Anaesth. 1997;78:301–307. doi: 10.1093/bja/78.3.301. [DOI] [PubMed] [Google Scholar]
- 9.Karaman S, Evren V, Firat V, Cankayali I. The effects of dexmedetomidine on spontaneous contractions of isolated gravid rat myometrium. Adv Ther. 2006;23:238–243. doi: 10.1007/BF02850129. [DOI] [PubMed] [Google Scholar]
- 10.Lee TL, Ang SB, Dambisya YM, Adaikan GP, Lau LC. The effect of propofol on human gastric and colonic muscle contractions. Anesth Analg. 1999;89:1246–1249. [PubMed] [Google Scholar]
- 11.Koutsoviti-Papadopoulou M, Akahori F, Kounenis G, Nikolaidis E. Propofol's biphasic effect on GABA(A)-receptor-mediated response of the isolated guinea pig ileum. Pharmacol Res. 1999;40:313–317. doi: 10.1006/phrs.1999.0523. [DOI] [PubMed] [Google Scholar]
- 12.Chang KS, Davis RF. Propofol produces endothelium-independent vasodilation and may act as a Ca2+ channel blocker. Anesth Analg. 1993;76:24–32. doi: 10.1213/00000539-199301000-00005. [DOI] [PubMed] [Google Scholar]
- 13.Karsli B, Kaya T, Cetin A. Effects of intravenous anesthetic agents on pregnant myometrium. Pol J Pharmacol. 1999;51:505–510. [PubMed] [Google Scholar]
- 14.Trapani G, Altomare C, Liso G, Sanna E, Biggio G. Propofol in anesthesia. Mechanism of action, structure-activity relationships, and drug delivery. Curr Med Chem. 2000;7:249–271. doi: 10.2174/0929867003375335. [DOI] [PubMed] [Google Scholar]
- 15.Jensen AG, Kalman SH, Nyström PO, Eintrei C. Anaesthetic technique does not influence postoperative bowel function: a comparison of propofol, nitrous oxide and isoflurane. Can J Anaesth. 1992;39:938–943. doi: 10.1007/BF03008343. [DOI] [PubMed] [Google Scholar]
- 16.Olkkola KT, Ahonen J. Midazolam and other benzodiazepines. Handb Exp Pharmacol. 2008;39:335–360. doi: 10.1007/978-3-540-74806-9_16. [DOI] [PubMed] [Google Scholar]
- 17.Castedal M, Björnsson E, Abrahamsson H. Effects of midazolam on small bowel motility in humans. Aliment Pharmacol Ther. 2000;14:571–577. doi: 10.1046/j.1365-2036.2000.00741.x. [DOI] [PubMed] [Google Scholar]
- 18.Fazel A, Burton FR. The effect of midazolam on the normal sphincter of Oddi: a controlled study. Endoscopy. 2002;34:78–81. doi: 10.1055/s-2002-19385. [DOI] [PubMed] [Google Scholar]