

Abstract
Herein, we describe the case of a 50-year-old man who had a fistula, located between the left anterior descending coronary artery and the left ventricle, that caused myocardial infarction. Electrocardiography revealed a loss of R-wave progression in leads V1 through V4, and transthoracic echocardiography showed an apical aneurysm. Selective coronary angiography was performed. Dimensions of the left anterior descending coronary artery, and digital caliper measurements of stenosis within, were normal. After the injection of angiographic contrast material from the distal part of the left anterior descending coronary artery, a smoky, opaque accumulation colored the left ventricle. The digital caliper measurement of the left anterior descending coronary artery was again found to be normal. In the apex of the left ventricle, ventriculography in the left anterior oblique position revealed a small aneurysm, and a myocardial perfusion scan showed a fixed perfusion defect.
Cases of coronary fistulae that result in myocardial infarction are rare. Because the patient had no ongoing symptoms after his myocardial infarction, medical therapy was prescribed.
Key words: Angina pectoris/etiology, arterio-arterial fistulas/complications/congenital/diagnosis/radiography, coronary angiography, coronary vessel anomalies/complications/diagnosis/epidemiology/radiography, fistula/complications/congenital, heart ventricles/abnormalities/physiology, myocardial infarction/etiology, vascular fistula/complications/diagnosis/therapy
Coronary artery fistula is a very rare cause of coronary artery disease, and it rarely causes coronary ischemia. Most affected patients are asymptomatic. Morphologically, coronary fistulae vary greatly, and they manifest themselves in widely differing clinical presentations; most often, respiratory difficulty and congestive heart failure accompany coronary fistulae. Investigators have reported that coronary artery fistulae can lead to symptoms of angina pectoris.1–4 More rarely, fistulae can precipitate myocardial infarction.1,2,4 Here, we present the case of a man in whom a coronary artery fistula caused myocardial infarction. We discuss coronary fistulae in general, and describe the treatment decided upon for our patient.
Case Report
In January 2007, a 50-year-old man was referred to our institution from another hospital. For 2 years, the patient had experienced exertional chest pain that resolved upon rest. After sustained pain for 2 weeks, he presented at a hospital. His cardiac enzyme levels were found to be elevated, and he was admitted with the diagnosis of acute coronary syndrome. He was subsequently referred to our institution for coronary angiography.
The patient's medical history revealed no other conditions related to acute coronary syndrome, although he had smoked 1 pack of cigarettes per day for 30 years. Upon physical examination, his blood pressure was 120/70 mmHg, and his heart rate was 69 beats/min. Other systems were normal. Laboratory values included total cholesterol, 214 mg/dL; low-density-lipoprotein cholesterol, 130 mg/dL; blood urea nitrogen, 17 mg/dL; and creatinine, 0.8 mg/dL. The levels of cardiac enzymes were normal by that time. Electrocardiography revealed a loss of R-wave progression in leads V1 through V4, with T-wave inversion. Transthoracic echocardiography revealed a left ventricular (LV) apical aneurysm; the LV dimensions were normal.
Selective coronary angiography was performed. The left coronary artery was normal in external dimension and upon digital caliper measurement of the lumen within. After the injection of a contrast agent from the distal part of the left anterior descending coronary artery, that artery was seen to drain into the LV (Fig. 1). An opaque, smoke-like accumulation colored the LV and then the aorta (Figs. 2 and 3). The right coronary artery was normal. Ventriculography at the left anterior oblique position revealed a small aneurysm in the LV apex (Fig. 4), and myocardial perfusion scanning revealed a fixed perfusion defect in the apex. These findings led to the diagnosis of a coronary fistula. Because the patient had no chest pain or other symptoms, he was discharged from the hospital on a medical regimen of metoprolol (50 mg daily), aspirin (300 mg daily), and atorvastatin (20 mg daily).
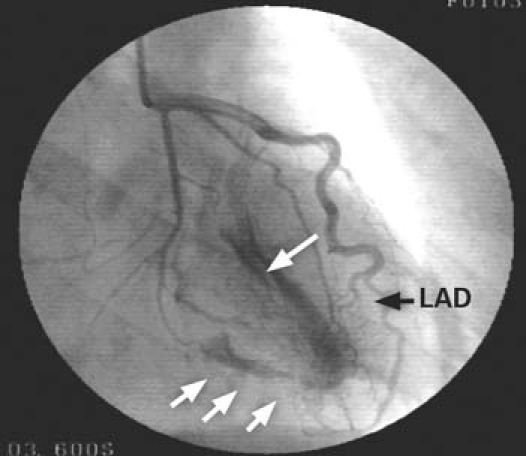
Fig. 1 Coronary angiography (right anterior oblique and caudal view) shows the left anterior descending coronary artery (LAD, black arrow) draining into the left ventricle (white arrows).

Fig. 2 Coronary angiography (left anterior oblique caudal view) shows an intense accumulation of opaque contrast material on the left ventricular apex (white arrows) due to a fistula (LAD, black arrow).

Fig. 3 On ventriculography via coronary injection (lateral view), an intense accumulation of opaque contrast material is seen on the left ventricle due to a fistula (Fis) between the distal part of the left anterior descending coronary artery (LAD, black arrow) and the apex of the left ventricle (white arrow).

Fig. 4 On ventriculography in the left anterior oblique position, a small aneurysm is visible in the apical region of the left ventricle (arrow).
Discussion
Although the actual incidence of congenital coronary artery fistula is unknown, it was reported as 0.13 (0.8%) in a 1980s study of 14,708 patients who underwent coronary angiography.5 Coronary artery fistula, which is among the rarer causes of coronary artery disease, generally does not lead to significant sequelae. The most prevalent are angina pectoris2 and congestive heart failure6; more rarely, infective endocarditis,3 thrombosis,4 embolism, and atrial fibrillation may result. Of 9 patients reported with coronary artery fistulae in Turkey, only 1 patient experienced expansion of the fistula to the LV.7 In another study,8 only 2% to 3% of coronary artery fistulae were found to have expanded to the LV. The chief differential diagnosis is patent ductus arteriosus.
Among methods used in the diagnosis of coronary fistulae, electrocardiography is unhelpful, although it can sometimes point out LV overload and ischemic ST-segment changes.9 Echocardiography may help to identify large fistulae. However, exact diagnosis is possible only upon coronary angiography. Besides detecting the presence of coronary artery fistulae, coronary angiography helps clinicians to determine the type of intervention that may be necessary.10
Myocardial infarction in cases of coronary artery fistula is rare.4 In a study of patients with coronary artery fistula, a 5% prevalence of myocardial infarction was found.11 A retrospective study2 revealed myocardial infarction in 9 of 51 instances of coronary artery fistula. Coronary fistulae that expand to the LV are known to cause coronary ischemia due to coronary steal syndrome, but they rarely lead to hemodynamic impairment, due to high pressure in the LV. Right-sided fistulae increase the volume load of the right heart chambers and the pulmonary bed.12 Although left-sided fistulae do not affect the pulmonary bed, they do cause volume load in the left chambers.6 In our patient, it was thought that the volume increase in the LV due to coronary steal syndrome formed conditions suitable for thrombosis.
Indications for treatment include a large left-to-right shunt, myocardial ischemia, endocarditis, and congestive heart failure. The goal of treatment is to occlude the fistula while providing normal coronary circulation.13 In some cases, coronary fistulae are spontaneously obstructed as a result of atherosclerosis, leading to asymptomatic patients.14
Surgical intervention is not without risk. Myocardial infarction may develop in 5% of patients during surgery, and then fistula may recur.15 Medical treatment is recommended for such patients, and the number of surgical procedures has decreased considerably due to the development of percutaneous closure methods.16 Such methods include the use of coils, detachable balloons, or alcohol injection.4,13,16–18 When symptoms occur, intervention is essential in order to avoid complications. Because our patient had no further symptoms and a fixed perfusion defect that was in a relatively small area, medical therapy was prescribed.
In conclusion, coronary artery fistulae are a rare cause of myocardial infarctions that develop in the absence of coronary artery disease. Although a fistula between the left anterior descending coronary artery and the LV rarely leads to myocardial infarction, one did so in our patient.
Footnotes
Address for reprints: Ibrahim H. Kurt, MD, Kurtulus mah. 10 sok. Ruhi Camurdan apt. kat: 5 No: 5, 01300 Adana, Turkey. E-mail: ibrahimhalilkurt@gmail.com
References
- 1.Kiuchi K, Nejima J, Kikuchi A, Takayama M, Takano T, Hayakawa H. Left coronary artery-left ventricular fistula with acute myocardial infarction, representing the coronary steal phenomenon: a case report. J Cardiol 1999;34(5):279–84. [PubMed]
- 2.Said SA, van der Werf T. Dutch survey of coronary artery fistulas in adults: congenital solitary fistulas. Int J Cardiol 2006; 106(3):323–32. [DOI] [PubMed]
- 3.Alkhulaifi AM, Horner SM, Pugsley WB, Swanton RH. Coronary artery fistulas presenting with bacterial endocarditis. Ann Thorac Surg 1995;60(1):202–4. [PubMed]
- 4.Khan MD, Qureshi SA, Rosenthal E, Sharland GK. Neonatal transcatheter occlusion of a large coronary artery fistula with Amplatzer duct occluder. Catheter Cardiovasc Interv 2003;60(2):282–6. [DOI] [PubMed]
- 5.Gillebert C, Van Hoof R, Van de Werf F, Piessens J, De Geest H. Coronary artery fistulas in an adult population. Eur Heart J 1986;7(5):437–43. [DOI] [PubMed]
- 6.Rivera IR, Moises VA, Tebexreni AS, Silva CC, Andrade JL, Campos Filho O, Carvalho AC. Right coronary artery fistula with congestive heart failure in the neonate. Doppler echocardiographic diagnosis and closure with detachable balloon [in English, Portuguese]. Arq Bras Cardiol 2000;74(3):243–52. [DOI] [PubMed]
- 7.Karagoz HY, Zorlutuna YI, Babacan KM, Tasdemir O, Yakut C, Kutuk E, et al. Congenital coronary artery fistulas. Diagnostic and surgical considerations. Jpn Heart J 1989;30(5): 685–94. [DOI] [PubMed]
- 8.Yamanaka O, Hobbs RE. Coronary artery anomalies in 126,595 patients undergoing coronary arteriography. Cathet Cardiovasc Diagn 1990;21(1):28–40. [DOI] [PubMed]
- 9.Oshiro K, Shimabukuro M, Nakada Y, Chibana T, Yoshida H, Nagamine F, et al. Multiple coronary LV fistulas: demonstration of coronary steal phenomenon by stress thallium scintigraphy and exercise hemodynamics. Am Heart J 1990;120(1):217–9. [DOI] [PubMed]
- 10.Luo L, Kebede S, Wu S, Stouffer GA. Coronary artery fistulae. Am J Med Sci 2006;332(2):79–84. [DOI] [PubMed]
- 11.Wong CK, Lau CP, Cheng CH. Coronary artery-left ventricular fistula with apical hypertrophic cardiomyopathy. Eur Heart J 1991;12(2):283–5. [DOI] [PubMed]
- 12.Jaffe RB, Glancy DL, Epstein SE, Brown BG, Morrow AG. Coronary arterial-right heart fistulae. Long-term observations in seven patients. Circulation 1973;47(1):133–43. [DOI] [PubMed]
- 13.Behera SK, Danon S, Levi DS, Moore JW. Transcatheter closure of coronary artery fistulae using the Amplatzer Duct Occluder. Catheter Cardiovasc Interv 2006;68(2):242–8. [DOI] [PubMed]
- 14.Muthusamy R, Gupta G, Ahmed RA, de Giovanni J, Singh SP. Fistula between a branch of left anterior descending coronary artery and pulmonary artery with spontaneous closure. Eur Heart J 1990;11(10):954–6. [DOI] [PubMed]
- 15.Kirklin JW, Barratt-Boyes BG. Cardiac surgery: morphology, diagnostic criteria, natural history, techniques, results, and indications. 2nd ed. New York: Churchill Livingstone Inc.; 1993. p. 945–55.
- 16.Cheung DL, Au WK, Cheung HH, Chiu CS, Lee WT. Coronary artery fistulas: long-term results of surgical correction. Ann Thorac Surg 2001:71(1):190–5. [DOI] [PubMed]
- 17.Spaedy TJ, Wilensky RL. Coronary artery fistulas: clinical implications. ACC Curr J Rev 1994;3:24–5.
- 18.Liberthson RR, Sagar K, Berkoben JP, Weintraub RM, Levine FH. Congenital coronary arteriovenous fistula. Report of 13 patients, review of the literature and delineation of management. Circulation 1979;59(5):849–54. [DOI] [PubMed]