

Abstract
Background:
Stiff-person syndrome (SPS), formerly Stiff-man syndrome, is a rare autoimmune disease usually exhibiting severe spasms and thoracolumbar stiffness, with very elevated glutamic acid decarboxylase antibodies (GAD Ab). A paraneoplastic variant, less well characterized, is associated with amphiphysin antibodies (amphiphysin Ab). The objective of this study was to identify distinctive clinical features of amphiphysin Ab-associated SPS.
Methods:
Records associated with 845 sera tested in the Yale SPS project were examined, and 621 patients with clinically suspected SPS were included in the study. Clinical characteristics were assessed with correction for multiple comparisons.
Results:
In all, 116 patients had GAD antibodies and 11 patients had amphiphysin Ab; some clinical information was available for 112 and 11 of these patients, respectively. Patients with amphiphysin Ab-associated SPS were exclusively female; mean age was 60. All except one had breast cancer; none had diabetes. Compared to patients with GAD Ab-associated SPS, those with amphiphysin Ab were older (p = 0.02) and showed a dramatically different stiffness pattern (p < 0.0000001) with cervical involvement more likely, p ≤ 0.001. Electromyography showed continuous motor unit activity or was reported positive in eight. Benzodiazepines at high dose (average 50 mg/day diazepam) were partially effective. Four patients were steroid responsive and tumor excision with chemotherapy produced marked clinical improvement in three of five patients.
Conclusions:
Amphiphysin Ab-associated stiff-person syndrome is strongly associated with cervical region stiffness, female sex, breast cancer, advanced age, EMG abnormalities, and benzodiazepine responsiveness. The condition may respond to steroids and can dramatically improve with cancer treatment.
GLOSSARY
- EAE
= experimental autoimmune encephalitis;
- GAD Ab
= glutamic acid decarboxylase antibodies;
- ICC
= immunocytochemistry;
- PERM
= progressive variant with encephalomyelitis, rigidity, and myoclonus;
- SPS
= stiff-person syndrome.
Stiff-person syndrome (SPS), formerly known as stiff-man syndrome, is a rare neuroimmunologic disease, the understanding and diagnosis of which greatly advanced with the identification of disease-associated autoantibodies.1,2 The principal form of SPS is characterized by severe stiffness predominantly of spine and legs with superimposed muscle spasms worsened by emotional stress and triggers.3 It is associated with high levels of antibodies against glutamic acid decarboxylase (GAD Ab).4 Variant forms of SPS, less strongly associated with GAD Ab, have been described, including a limited variant (stiff-limb syndrome) and a progressive variant with encephalomyelitis, rigidity, and myoclonus (PERM).5,6
Another variant of SPS, associated with autoantibodies against amphiphysin (amphiphysin Ab) and possibly with breast cancer, is recognized but represents a small minority of SPS cases.7,8 Amphiphysin Ab are frequently coexpressed with other paraneoplastic antibodies and have, in this setting, been associated with other neurologic disorders, especially sensory neuronopathy, encephalopathy, and myelopathy. Nonetheless, amphiphysin Ab-associated SPS is a recognized clinical entity.9 The clinical features of amphiphysin Ab-associated SPS include profound muscle stiffness but remain to be better defined. The incidence of amphiphysin Ab-associated SPS is low and for this reason, progress in defining the principal features of the syndrome has been slow. Nonetheless, improved recognition of this clinical syndrome has important implications. First, amphiphysin Ab are typically paraneoplastic, while GAD Ab are not.10,11 Secondly, evidence suggests that GAD Ab-associated SPS responds to IVIg while amphiphysin Ab-associated SPS may require steroids, plasmapheresis, or cancer treatment.12
We hypothesized, based on case reports and clinical observations, that certain features of amphiphysin Ab-associated SPS might be distinct from the principal GAD Ab-associated form of the disease.13
METHODS
A total of 845 case records were reviewed for this study; these were acquisitioned between 1986 and 1998 as described previously.4 The case records were continuously maintained and updated from 1998 until December 2007. All records were evaluated by a single investigator (B.B.M.) and checked for accuracy. Records were first evaluated for the a priori suspicion of SPS as a diagnosis; those patients not referred for SPS testing and any duplicates were removed from further study, leaving 621 patient records. In one case, 71 patients tested for GAD Ab in the setting of type I diabetes were excluded; in another, two patients who tested positive for amphiphysin Ab were excluded from further study as they had sensory neuronopathy and not SPS. Next, the type of antibody testing that was sought (if specified) and the nature of clinical information provided was determined. Finally, the presence of antibodies to GAD or amphiphysin I (confirmed by Western blot) was noted as determined using previously reported methods.7 Properties of the GAD antibody testing method in this study were previously reported.4 This testing was performed as part of the Yale SPS caseload. Johns Hopkins IRB exemption was obtained for this study.
There were 621 patients referred for testing of antineuronal antibodies with a clinical suspicion of SPS. Some of these patients have been described elsewhere.7,12,14 All pertinent information was extracted from the records and where possible included in the calculation of selected statistics, e.g., for GAD Ab-associated SPS, the mean age was calculated for n = 100; for GAD Ab-associated SPS, the sex ratio was based on n = 112. Those records that contained detailed clinical information, i.e., a comprehensive letter of referral, history and physical, published case history, completed questionnaire, or electronic correspondence, were examined systematically for the presence of stiffness-related symptoms in specific body regions, i.e., face (and bulbar musculature), neck, arms, spine, abdomen, and legs. Patient gender; age; stiffness, rigidity, increased tone, spasms, or pain as symptoms; response to benzodiazepines and other treatments; cancer presence/type; and EMG results were recorded.
One patient has been previously reported elsewhere as having both amphiphysin and GAD antibodies.14 In this patient, GAD Ab were not present at first testing but developed 2 years later at intermediate levels, the significance of which is not known; GAD Ab immunocytochemistry was persistently negative. Because immunocytochemistry showed only amphiphysin Ab, the patient was included in the amphiphysin Ab-associated SPS group; this did not change the results.
The age of the patients in the two groups was compared using a rank-sum test.
Involvement of body regions was compared for amphiphysin and GAD Ab-associated SPS patients using a χ2 test, with the hypothesis that the two syndromes had dissimilar patterns of stiffness. Comparisons between specific regions were made using a proportions test.15 Differences were significant for α ≤ 0.05 following correction for multiple comparisons.
RESULTS
A total of 11 patients with suspected SPS were found to have amphiphysin Ab; another 116 patients were found to have GAD antibodies. Of the 11 patients with amphiphysin Ab, some clinical information was available for 11 and detailed information for 10. There were 112 GAD Ab-associated patients with some clinical information; 84 had detailed information.
As a group, the amphiphysin Ab-associated SPS patients studied were exclusively female (n = 11), and the mean age at symptom onset was 58 (range 39–73). These patients were older than those with GAD Ab-associated SPS (p = 0.02). All except one had breast cancer, as noted in the table. Of the patients with detailed clinical information (n = 10), all had stiffness, rigidity, or increased tone; five had substantial pain. None had diabetes. Eight patients had an EMG showing continuous motor unit activity or noted to be consistent with SPS. Nine were described as benzodiazepine responsive, and specified doses were high, e.g., diazepam averaged >50 mg per day. Importantly, 10 of the amphiphysin Ab-associated SPS patients were found to have breast cancer. In one patient, this developed 5 years after initial assessment. Four patients were described as steroid responsive; IVIg efficacy was not reported. Three patients were described as dramatically better following tumor excision and chemotherapy, one did not respond to this intervention and subsequently died, one patient was described as symptom-free with immunosuppression prior to breast cancer diagnosis and treatment.
Table Amphiphysin and GAD Ab-associated SPS characteristics
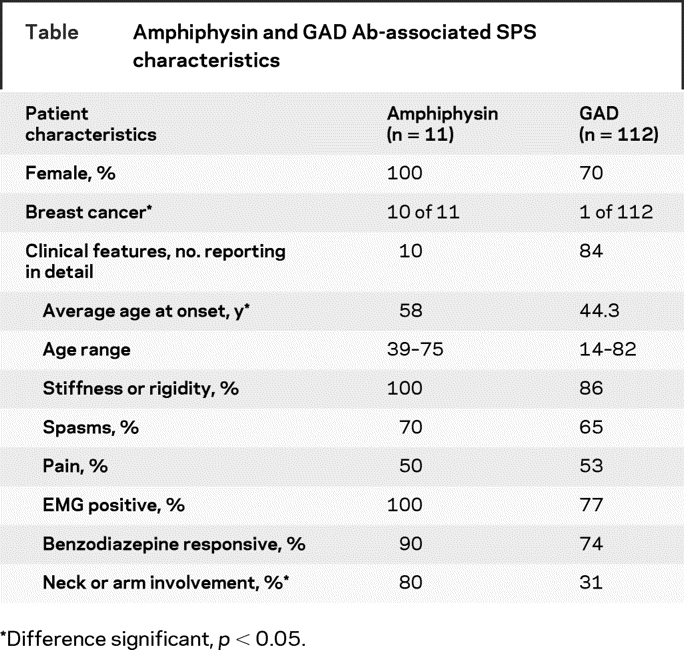
As a group, the GAD Ab-associated SPS patients studied in detail were 70% female and the mean age at symptom onset was 44 (range 11–82). The age distribution of the SPS patients with antineuronal antibodies is shown in figure 1. Interestingly, the age range for male patients was 14–82, while that for female patients was 30–73; the difference in age variability between the two sexes approached but did not reach significance (F-test, p = 0.06). Almost all of the patients with GAD Ab-associated SPS had stiffness, rigidity, or increased tone; a majority had pain. Most were described as benzodiazepine responsive and doses were also high; diazepam averaged 37 mg per day and clonazepam 4 mg per day. Over half had an EMG showing continuous motor unit activity although 20% of those undergoing EMG were described as having a negative result. One patient was noted to have cancer; it was breast adenocarcinoma.

Figure 1 Age distribution of patients with stiff-person syndrome with antineuronal antibodies
The localization of symptoms to various body regions was evaluated and is shown for amphiphysin Ab-associated and GAD Ab-associated SPS in figure 2. Comparison of these patterns demonstrated marked differences (χ2, p < 0.0000001). Arm and neck involvement was described as prominent or specifically noted by the referring clinician in 80% of the patients with amphiphysin Ab-associated SPS but was specifically noted in just 37% of the patients with GAD Ab-associated SPS. This difference was significant, p = 0.001. The overall pattern of involvement appeared to be different. In patients with high levels of GAD antibodies, the pattern was legs and spine > abdomen and arms > neck > bulbar. In amphiphysin Ab-associated SPS, the pattern was arms, neck, abdomen, spine, and legs almost equally involved. Thus in GAD Ab-associated SPS, stiffness showed a caudal to rostral gradient, while amphiphysin Ab-associated SPS had a different pattern of stiffness, frequently involving the arms and neck.

Figure 2 Regions of the body affected by stiff-person syndrome (SPS)
(A) GAD Ab-associated SPS shows a distinct pattern of stiffness with a rostral to caudal gradient of involvement. (B) Percent of patients with amphiphysin Ab-associated stiffness in various body regions. The regional pattern of stiffness is different from that of GAD Ab-associated SPS, p < 0.001. The arms exhibit more stiffness in amphiphysin Ab-associated SPS, p = 0.01.
DISCUSSION
This study demonstrates that distinct clinical features characterize amphiphysin Ab-associated SPS; most especially, a pattern of stiffness that is more broadly distributed and more likely to involve the arms and neck. In GAD Ab-associated SPS, stiffness predominantly affects the thoracolumbar musculature. Importantly, amphiphysin Ab-associated SPS is much rarer, one-tenth the number (10%) of GAD Ab-associated SPS patients in our series, and the clinical features of these patients have until now eluded detailed characterization.
Our study provides valuable guidance for clinicians with SPS patients: we demonstrate that amphiphysin Ab-associated SPS is a cancer-associated syndrome, while GAD Ab-associated SPS is not. Identification of amphiphysin antibodies in patients with profound stiffness mandates a search for breast cancer, and secondarily, lung cancer.16 In the absence of atypical features, our data do not support extensive cancer screening in GAD Ab-associated SPS. Additionally, we find that diabetes is infrequently associated with amphiphysin Ab-associated SPS. In contrast, diabetes occurs frequently in GAD Ab-associated SPS.2 GAD is a major autoantigen in diabetes and diabetes monitoring for patients with GAD Ab-associated SPS is essential for comprehensive care.
Regarding treatment, there are critical differences between amphiphysin Ab-associated and GAD Ab-associated forms of SPS. GAD Ab-associated SPS is responsive to IVIg.17 Anecdotal evidence and clinical experience suggest that amphiphysin Ab-associated SPS may not respond to IVIg; however, case reports propose plasmapheresis with steroids or treatment of the primary process, i.e., breast cancer. Our study suggests that amphiphysin Ab-associated SPS is steroid responsive and raises the possibility that tumor excision with chemotherapy may produce profound benefits.
With current laboratory testing practices, refined clinical criteria for the recognition of amphiphysin Ab-associated SPS are indispensable. Testing for the relevant antibodies is no longer performed by immunocytochemistry (ICC), a labor-intensive method that could identify multiple antigens in a single serum sample.18 SPS-associated antibodies are now measured by immunoassay (RIA or ELISA), using purified antigen and detecting only the antibody specifically requested. Furthermore, although GAD Ab testing is widely available, amphiphysin Ab are measured in very few laboratories. Thus, amphiphysin Ab must be specifically suspected and sought out.
The reasons why amphiphysin Ab-associated and GAD Ab-associated SPS have different patterns of regional involvement remain uncertain. Beyond this, it is not clear whether amphiphysin Ab and GAD Ab are directly pathogenic, as both GAD and amphiphysin are intracellular proteins, in principle shielded from direct interactions with circulating antibodies. Interestingly, the administration of human amphiphysin Ab to rats, in the setting of experimental autoimmune encephalitis (EAE), produced a syndrome of truncal and hindlimb stiffness.19 In this model, forelimb stiffness was not noted; however, the pattern of hindlimb involvement may have, in part, reflected the loss of blood–brain barrier intrinsic to the underlying EAE model.
Although additional studies of patients with amphiphysin Ab-associated SPS are needed, clinical recognition of this unusual syndrome will likely speed diagnosis and increase delivery of effective treatments.
ACKNOWLEDGMENT
The authors thank Michele Solimena, Pietro de Camilli, Margaret Butler, and Hans-Michael Meinck for discussions of this work and contributions to the preparation of this manuscript, and Vikki Spelleda for technical support.
Supplementary Material
Address correspondence and reprint requests to Dr. Beth B. Murinson, 600 N. Wolfe Street, Pathology 509, Baltimore, MD 21287 bb@jhmi.edu
Editorial, page 1938
e-Pub ahead of print on October 29, 2008, at www.neurology.org.
Supported in part by NIH career development grant NS048146 (B.B.M.) and the Stephen Hyde Fund for SPS Research (B.B.M.).
Disclosure: The authors report no disclosures.
Received February 25, 2008. Accepted in final form June 13, 2008.
REFERENCES
- 1.Solimena M, Folli F, Denis-Donini S, et al. Autoantibodies to glutamic acid decarboxylase in a patient with stiff-man syndrome, epilepsy, and type I diabetes mellitus. N Engl J Med 1988;318:1012–1020. [DOI] [PubMed] [Google Scholar]
- 2.Levy LM, Dalakas MC, Floeter MK. The stiff-person syndrome: an autoimmune disorder affecting neurotransmission of gamma-aminobutyric acid. Ann Intern Med 1999;131:522–530. [DOI] [PubMed] [Google Scholar]
- 3.Lorish TR, Thorsteinsson G, Howard FM, Jr. Stiff-man syndrome updated. Mayo Clin Proc 1989;64:629–636. [DOI] [PubMed] [Google Scholar]
- 4.Murinson BB, Butler M, Marfurt K, Gleason S, De CP, Solimena M. Markedly elevated GAD antibodies in SPS: effects of age and illness duration. Neurology 2004;63:2146–2148. [DOI] [PubMed] [Google Scholar]
- 5.Brown P, Marsden CD. The stiff man and stiff man plus syndromes. J Neurol 1999;246:648–652. [DOI] [PubMed] [Google Scholar]
- 6.Meinck HM, Faber L, Morgenthaler N, et al. Antibodies against glutamic acid decarboxylase: prevalence in neurological diseases. J Neurol Neurosurg Psychiatry 2001;71:100–103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Folli F, Solimena M, Cofiell R, et al. Autoantibodies to a 128-kd synaptic protein in three women with the stiff-man syndrome and breast cancer. N Engl J Med 1993;328:546–551. [DOI] [PubMed] [Google Scholar]
- 8.De Camilli P, Thomas A, Cofiell R, et al. The synaptic vesicle-associated protein amphiphysin is the 128-kD autoantigen of stiff-man syndrome with breast cancer. J Exp Med 1993;178:2219–2223. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Pittock SJ, Lucchinetti CF, Parisi JE, et al. Amphiphysin autoimmunity: paraneoplastic accompaniments. Ann Neurol 2005;58:96–107. [DOI] [PubMed] [Google Scholar]
- 10.Antoine JC, Absi L, Honnorat J, et al. Antiamphiphysin antibodies are associated with various paraneoplastic neurological syndromes and tumors. Arch Neurol 1999;56:172–177. [DOI] [PubMed] [Google Scholar]
- 11.Floyd S, Butler MH, Cremona O, et al. Expression of amphiphysin I, an autoantigen of paraneoplastic neurological syndromes, in breast cancer. Mol Med 1998;4:29–39. [PMC free article] [PubMed] [Google Scholar]
- 12.Schmierer K, Valdueza JM, Bender A, et al. Atypical stiff-person syndrome with spinal MRI findings, amphiphysin autoantibodies, and immunosuppression. Neurology 1998;51:250–252. [DOI] [PubMed] [Google Scholar]
- 13.Murinson BB. Stiff-person syndrome. Neurologist 2004;10:131–137. [DOI] [PubMed] [Google Scholar]
- 14.Rosin L, DeCamilli P, Butler M, et al. Stiff-man syndrome in a woman with breast cancer: an uncommon central nervous system paraneoplastic syndrome. Neurology 1998;50:94–98. [DOI] [PubMed] [Google Scholar]
- 15.Dixon WJ, Massey FJ. Enumeration statistics. In: Dixon WJ, Massey FJ, eds. Introduction to Statistical Analysis, 4th ed. New York: McGraw-Hill Book Company, 1983:272–300. [Google Scholar]
- 16.Nguyen-Huu BK, Urban PP, Schreckenberger M, Dieterich M, Werhahn KJ. Antiamphiphysin-positive stiff-person syndrome associated with small cell lung cancer. Mov Disord 2006;21:1285–1287. [DOI] [PubMed] [Google Scholar]
- 17.Dalakas MC, Fujii M, Li M, Lutfi B, Kyhos J, McElroy B. High-dose intravenous immune globulin for stiff-person syndrome. N Engl J Med 2001;345:1870–1876. [DOI] [PubMed] [Google Scholar]
- 18.Butler MH, Hayashi A, Ohkoshi N, et al. Autoimmunity to gephyrin in Stiff-Man syndrome. Neuron 2000;26:307–312. [DOI] [PubMed] [Google Scholar]
- 19.Sommer C, Weishaupt A, Brinkhoff J, et al. Paraneoplastic stiff-person syndrome: passive transfer to rats by means of IgG antibodies to amphiphysin. Lancet 2005;365:1406–1411. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.