

Abstract
Background:
Obesity and restless legs syndrome (RLS) are both associated with hypofunction of dopamine in the CNS. We therefore examined whether individuals who are obese have an increased risk of RLS in two ongoing US cohorts, the Nurses’ Health Study II and the Health Professional Follow-up Study.
Methods:
We included 65,554 women and 23,119 men free of diabetes, arthritis, and pregnancy in the current analyses. Information on RLS was assessed using a set of standardized questions. Participants were considered to have RLS if they met four RLS diagnostic criteria recommended by the International RLS Study Group and had restless legs ≥5 times/month. Odds ratios (ORs) and 95% confidence intervals (CIs) were computed using logistic regression models adjusting for age, smoking, use of antidepressant, phobic anxiety score, and other covariates. Log ORs from the two cohorts were pooled by a fixed-effects model.
Results:
There were 6.4% of women and 4.1% of men who were considered to have RLS. Multivariate adjusted ORs for RLS were 1.42 (95% CI: 1.3, 1.6; p trend <0.0001) for participants with body mass index (BMI) >30 vs <23 kg/m2 and 1.60 (95% CI: 1.5, 1.8; p trend <0.0001) for highest vs lowest waist circumference quintiles. Greater BMI in early adulthood (age 18–21 years) and weight gain were also associated with a higher prevalence of RLS (p trend <0.01 for both).
Conclusions:
Both overall and abdominal adiposity are associated with increased likelihoods of having restless legs syndrome (RLS). Further prospective studies are warranted to clarify causative association between obesity and risk of developing RLS.
GLOSSARY
- BMI
= body mass index;
- CI
= confidence interval;
- HPFS
= Health Professionals Follow-up Study;
- NHS II
= Nurses’ Health Study II;
- OR
= odds ratios;
- RLS
= restless legs syndrome.
Restless legs syndrome (RLS) is a common movement disorder, characterized by an almost irresistible urge to move the legs. According to recent estimates, it affects 5–20% of adults and often has a substantial impact on sleep, daily activities, and quality of life.1,2 Cross-sectional studies have shown that participants with RLS had a significantly higher prevalence of depression, diabetes, and cardiovascular disease, and a lower mental health score than participants without RLS.1-7 Patients with RLS also had a reduced quality of life compared with the general population comparable with that experienced by those with other serious chronic medical conditions, such as type 2 diabetes mellitus, chronic obstructive pulmonary disorder, or depression.8 There is strong evidence of environmental causes of RLS, but the etiology remains unknown. Dopaminergic hypofunction in the CNS is believed to have a crucial role in disease pathophysiology.9,10 Thus, environmental factors, which affect CNS dopaminergic status, may have a role in RLS. Exploring potential associations between these dopamine-related factors and RLS risk could not only improve our understanding of RLS pathogenesis but provide a practicable method for RLS prevention as well.
Obese persons have decreased dopamine D2 receptor availability in brain,11 and could thus be at increased risk of RLS. However, the relationship between obesity and RLS remains uncertain and valid data to assess this hypothesis are limited. Some epidemiologic studies have reported that body mass index (BMI) was associated with a higher likelihood of having RLS,7,12,13 but none of them adjusted for anxiety status, use of antidepressant, and presence of chronic diseases, which may confound the observed associations.2,3,14 In some of these studies, RLS was assessed by a single question.7,13 We therefore conducted a large-scale study to examine associations between overall obesity (reflected by higher BMI), abdominal adiposity (reflected by higher waist circumference or waist-to-hip ratio), and risk of having RLS in the two ongoing US cohorts of men and women: the Health Professionals Follow-up Study (HPFS) and the Nurses’ Health Study II (NHS II).
METHODS
Study populations.
The NHS II cohort comprises 116,686 registered nurses (women) who were 25 to 42 years of age and resided in 1 of 14 US states at the time of enrollment in 1989. The HPFS is a cohort of men established in 1986, when 51,529 US health professionals (dentists, optometrists, osteopaths, podiatrists, pharmacists, and veterinarians) aged 40–75 years completed a mailed questionnaire about their medical history and lifestyle. Follow-up questionnaires have been mailed to participants every 2 years to update information on potential risk factors and to ascertain newly diagnosed diseases in both cohorts. The institutional review board at Brigham and Women’s Hospital reviewed and approved this study, and receipt of each questionnaire implies the participant’s consent.
Assessment of RLS.
We asked questions about RLS diagnosis and severity based on the International RLS Study Group criteria in 2005 for NHS II (n = 97,642, mean age 50.4 ± 5 years) and 2002 for HPFS (n = 37,431, mean age 68.9 ± 9 years) among participants who were still alive and actively participating in the study. The following question was asked: “Do you have unpleasant leg sensations (like crawling, paraesthesia, or pain) combined with motor restlessness and an urge to move?” The possible responses were as follows: no, less than once/month, 2–4 times/month, 5–14 times/month, and 15 or more times per month. Those who answered that they had these feelings were asked the following two questions: 1) “Do these symptoms occur only at rest and does moving improve them?” and 2) “Are these symptoms worse in the evening/night compared with the morning?” A probable RLS case was considered to be present if the participant answered “yes” for all three of the above questions, and has a frequency of ≥5 times/month.
The questions on RLS were completed by 79,992 (82%) women and 31,729 (85%) men. Participants who did not complete the RLS questions had similar age (mean 50.4 vs 50.4 years in women and 69.0 vs 68.6 years in men) and BMI (27.1 vs 26.5 kg/m2 in women and 26.5 vs 26.2 kg/m2 in men) as those with RLS information. To reduce a possible misclassification of RLS, we excluded participants with diabetes, arthritis, and pregnancy (women), leaving 65,554 women and 23,119 men in primary analyses. In a secondary analysis, we further examined the association between obesity and RLS including all participants with RLS information.
Assessment of obesity and covariates.
Information on weight and height was obtained on the baseline questionnaires. The questionnaire also asked about weight in early adulthood (age 18 years in women and 21 years in men). Self-reported weight was updated every 2 years. BMI was calculated as weight (kg)/height (m).2 Self-reported weight has been validated previously.15 Self-reported weights from 123 men and 140 women who participated in the HPFS and NHS I were highly correlated with values obtained by technicians who visited the participants at home (r = 0.97 for men and women).15 We asked participants to rate their body shape at age 20 years by choosing an image that corresponded to their figure on a scale ranging from 1 (thinnest) to 9 (largest) in 1989 for the NHS II and 1988 for the HPFS. The figure rating scale was adapted from Stunkard et al.16 Because of few RLS cases reporting a body shape type 7 (case number = 3 in men and 24 in women) and 9 (case number = 0 in men and 2 in women), we combined type 7 with 6 and type 9 with 8, and therefore grouped participants into seven body shape categories in our analyses.
Waist and hip circumference were reported in 1993 and 2005 in the NHS II, and in 1987 and 1996 in the HPFS. For waist circumference, participants were instructed to measure their waist circumference at the level of the navel, and for hip circumference they were instructed to measure the largest circumference around the hips (including the buttocks). The questionnaire also instructed the participants to perform the measurements while standing and to avoid measuring over bulky clothing. Participants reported their waist and hip circumference to the nearest quarter inch (0.64 cm). The self-reported measures of waist and hip circumference have also been validated: the correlation coefficients between self-reported estimates and measurements obtained by technicians sent to the home of participants were 0.89–0.95 for waist circumference and 0.84–0.88 for hip circumference in men and women.15 We used waist circumference and waist-to-hip ratio in 2005 in the NHS II and in 1996 in the HPFS as exposures in the current analyses.
Information on potential confounders, including age, ethnicity, smoking status, physical activity, use of medicines, history of major chronic diseases, history of blood donation, use of nutritional supplement, and rotating night shift work, was collected via biennial questionnaires through the follow-up. The phobic anxiety scale was assessed by the Crown-Crisp phobia index, a short, clinical self-rating scale for common phobias such as fear of enclosed spaces, illness, going out alone, heights, and crowds.17
Statistical analyses.
Statistical analyses were completed with SAS version 9.1 (SAS Institute, Inc, Cary, NC). To minimize the potential effects of extreme values on regression analyses and to allow for nonlinear association, we categorized the measures of obesity before conducting the analyses. Logistic regression was used to test differences in prevalence across categories and to calculate odds ratios (ORs) and 95% confidence intervals (CIs). Analyses were adjusted for age (years), ethnicity (Caucasian, African American, or Asian and other), smoking (never smoker, former smoker, or current smoker: 1–14 or ≥15 cigarettes/day), physical activity (quintiles), use of antidepressant (yes/no), the Crown-Crisp phobia index (0–1, 2, 3, or ≥ 4), and presence of stroke, hypertension, or myocardial infarction (yes/no). Linear trends were tested for significance by assigning each participant the median value in each category to create a continuous variable. Log ORs from the two cohorts were pooled by a fixed-effects model, weighted by the inverse of their variances as significance tests did not suggest heterogeneity between cohorts (p > 0.1 for all).18 The continuous measure of BMI was used to fit a restricted cubic spline model and to obtain a smooth representation of the OR of RLS as a function of BMI with adjustment for the effects of potential confounders.
We examined potential interactions of BMI with physical activity (high vs lowest, based on median) and smoking status (never vs ever). We included multiplicative terms in the logistic regression models, with adjustment for other potential confounders.
RESULTS
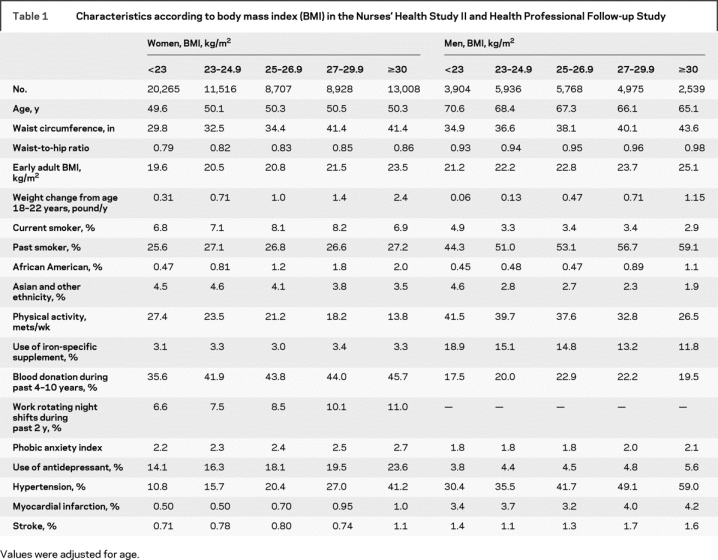
Participants in the highest category of BMI were more likely to be past smokers and to be hypertensive, to work rotating night shifts during past 2 years (women only), and exercised less than lean participants (table 1). There were 6.4% of women and 4.1% of men who met RLS diagnostic criteria and reported RLS symptoms ≥5 times/month, including 2.7% of women and 1.7% of men with RLS symptoms ≥15 times/month. Prevalences of RLS increased with age (figure e-1 on the Neurology® Web site at www.neurology.org). Caucasians had a higher RLS prevalence relative to other ethnicities. Prevalences were 6.6% in women and 4.2% in men among Caucasians, relative to 3.8% among non-Caucasian women and 2.4% among non-Caucasian men.
Table 1 Characteristics according to body mass index (BMI) in the Nurses’ Health Study II and Health Professional Follow-up Study
Obesity was associated with a higher likelihood of having RLS in women and men. The adjusted OR for BMI ≥30 vs <23 kg/m2 was 1.41 (95% CI: 1.3, 1.6; p trend <0.0001) for women and 1.48 (95% CI: 1.2, 1.9; p trend = 0.0008) for men after adjusting for age, ethnicity, physical activity, smoking, use of antidepressant, anxiety score, and presence of a number of chronic diseases (table 2). Effect sizes of obesity on RLS were similar between men and women (p for heterogeneity in ORs = 0.34). Pooled OR was 1.42 (95% CI: 1.3, 1.6; p trend <0.0001) for participants with BMI ≥30 kg/m2, relative to those with BMI <23 kg/m2. Additional adjustment for use of iron-specific supplement and history of blood donation did not materially change the associations between BMI and RLS (pooled adjusted OR comparing two extreme BMI categories = 1.41, p trend < 0.00001). After further adjusting for night shift work among women, the OR for BMI ≥30 vs <23 kg/m2 decreased slightly from 1.41 to 1.38 (p < 0.0001). A test for nonlinearity, using spline regression, was significant in men but not in women. Spline regression analysis demonstrated a monotonic dose-response relationship between BMI and increased risk of having RLS for all women and for men with BMI ≥23. The deviation from linearity in men was due to a non-significantly increased risk of RLS among men with low BMI (figure e-2). It remains unclear whether this was driven by chance as a relative small sample size in men. Further studies are needed. We observed similar associations between higher BMI in early adulthood (age 18–21 years) and a higher likelihood of having RLS. The adjusted OR for BMI ≥30 vs <23 kg/m2 was 1.24 (95% CI: 1.0, 1.5; p trend = 0.004). Perceived body shape at age 20 years was also positively associated with RLS. The multiple-adjusted ORs across seven categories were 1.0 (ref), 1.12, 1.13, 1.16, 1.16, 1.21, and 1.38 (95% CI: 0.7, 2.7; p trend = 0.05). Consistently, greater weight gain was associated with a higher risk of having RLS (p trend < 0.0001): the adjusted OR for the highest vs lowest quintile of weight gain was 1.41 (95% CI: 1.3, 1.6).
Table 2 Odds ratio (OR) (95% confidence interval) of restless legs syndrome according to body mass index (BMI) and weight change

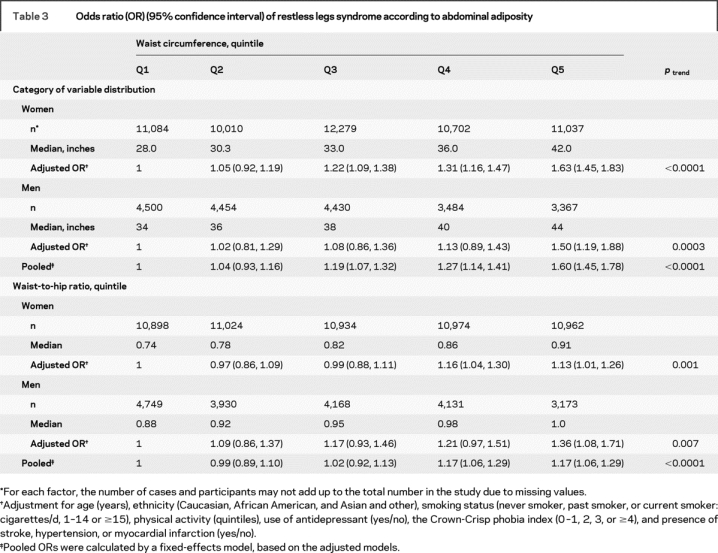
Abdominal adiposity was also associated with a higher likelihood of having RLS (table 3). Multiple-adjusted ORs were 1.60 (95% CI: 1.5, 1.8; p trend < 0.0001) for the highest quintiles of waist circumference and 1.17 (95% CI: 1.1, 1.3, p trend < 0.0001) for waist-to-hip-ratio, relative to those in the lowest quintiles.
Table 3 Odds ratio (OR) (95% confidence interval) of restless legs syndrome according to abdominal adiposity
When we used participants with frequency of restless legs ≥15 times/month as an outcome, the associations between BMI, waist circumference, and RLS changed slightly. Multivariate OR was 1.47 (95% CI: 1.3, 1.7; p trend < 0.0001) comparing two extreme categories of BMI and 1.68 (95% CI: 1.4, 2.0; p trend < 0.0001) for waist circumference.
To test the robustness of our observations, we conducted several sensitivity analyses and obtained similar results. Multiple-adjusted ORs comparing the highest to lowest categories of BMI were 1.43 (95% CI: 1.3, 1.6) after excluding participants with highest levels of phobic anxiety, 1.40 (95% CI: 1.3, 1.5) after excluding participants with myocardial infarction or stroke, and 1.41 (95% CI: 1.3, 1.6) after excluding those with hypertension. After further inclusion of participants with diabetes or arthritis, association between BMI and RLS did not change materially. The multiple-adjusted OR comparing the highest to lowest categories of BMI was 1.53 (95% CI: 1.4, 1.6).
We did not find significant interaction between BMI and physical activity and smoking status (p interaction > 0.3 for both). The associations between BMI and RLS persisted in subgroup analysis according to physical activity and smoking status (p trend < 0.0001 among all subgroups) (figure e-3).
DISCUSSION
In these large cohorts, 6.4% of women and 4.1% of men had RLS according to the diagnostic criteria recommended by the International RLS Study Group, and the prevalence increased progressively with increasing BMI and waist circumference. The association was independent of age, smoking status, anxiety score, use of antidepressant, and presence of a number of chronic diseases. A similar association was found between obesity in early adulthood (age 18 or 21) and RLS prevalence in mid-life or later (age 40 years and higher), suggesting that obesity is a risk factor for the development of RLS.
Although the influence of obesity on RLS may be modest, the implication of these results may be substantial as obesity is a modifiable factor which is becoming increasingly prevalent in the United States. Strengths of the study include the population-based design and adjustment for a number of potential confounders. Multiple markers of adiposity were employed in the current analyses and generated similar results. Further, in a variety of sensitivity analyses, we observed similar significant dose-response relationship between obesity and RLS.
An association between obesity and a higher RLS prevalence has been seen in most studies,7,12,13 but not all.19 In a cross-sectional study including 1,803 men and women aged 18 years or older, each increase of 5 kg/m2 BMI was associated with a 31% increased likelihood of having RLS.7 In another cross-sectional study conducted in five European countries (n = 18,890), the crude OR for RLS was 1.22 (95% CI: 1.0, 1.5) for BMI of > 27 vs 20–25 kg/m2.12 In a Korean population (n = 9,939), a significant association between BMI and RLS was seen among women (OR = 1.2 for BMI >25 vs ≤25 kg/m2) but not among men (OR = 1.1).13
The mechanisms through which obesity is associated with RLS are likely to be multiple. Cardiovascular diseases are associated with an increased risk of both obesity and RLS,3 and it has been suggested that vascular pathology may contribute to RLS.20 However, exclusion of participants with cardiovascular diseases had a minimal effect on our results, suggesting that other factors mediate the relation between obesity and RLS. Results from several investigations suggest that the dopaminergic system in the CNS may be affected in both obesity and RLS. In a case-control study, obese individuals (n = 10, BMI >40 kg/m2) had a significantly lower number of striatal dopamine D2 receptors, as measured by PET and (C-11) raclopride, than controls (p < 0.01), and among obese individuals the number of dopamine receptors was inversely correlated with BMI.11 These findings were supported by observations from animal studies where obese rats had lower D2 dopamine receptors.21,22 Genetic studies have shown a link between obesity and variants of dopamine metabolism-relevant genes, such as MAOA and MAOB.23 Further, in some longitudinal studies individuals with higher levels of body fat, as measured by BMI and midlife triceps skin-fold thickness, have been found to have a higher risk of PD,24,25 although this finding was not confirmed in other investigations, including the HPFS.26
Obesity and RLS could share some unknown common causes. Although we excluded participants with diabetes in the analyses, obesity could also be an indictor of undiagnosed diabetes, and some individuals with RLS could have undiagnosed diabetic neuropathy. However, the effects of undiagnosed diabetes on the observed obesity–RLS relationships should be moderate, as the number of these participants should be relatively small. Further experimental studies are needed to explore biologic mechanisms underlying the potential roles of obesity in RLS.
A limitation of our study is that misreporting of BMI or waist circumference could cause misclassification, but because of the very strong correlation between self-reported and measured obesity indicators,15 error from this source is most likely minimal. Moreover, the diagnosis of RLS was based on self-report, and some degree of diagnostic error is thus likely. However, a validation study showed a relative good sensitivity (87.5%) and specificity (96%) of the three-question set of RLS diagnosis, which is used in the current study, compared with the physician diagnoses.4,27 Further, confounding by genetic risk factors for RLS28,29 cannot be excluded, but it is unlikely to fully explain the results of our study because there is no evidence that risk alleles for RLS are related to obesity. We were also unable to directly adjust for status of iron deficiency, another well-known risk factor of RLS, because we did not collect this information in our cohorts. However, further adjusting for surrogates for iron status, including use of iron-specific supplements and number of blood donations, which was found to be a strong determinant of ferritin concentration in a subsample of participants in the HPFS,30 did not materially change the observed significant associations between obesity and higher risk of RLS.
AUTHOR CONTRIBUTIONS
Dr. Gao conducted the statistical analysis.
Supplementary Material
Address correspondence and reprint requests to Dr. Xiang Gao, Channing Laboratory, Department of Medicine, Brigham and Women’s Hospital, and Harvard Medical School, 181 Longwood Avenue, Boston, MA 02115
xiang.gao@channing.harvard.edu
Supplemental data at www.neurology.org
Supported by NIH/NINDS grant R01 NS048517.
Disclosure: The authors report no disclosures.
Received October 13, 2008. Accepted in final form January 23, 2009.
REFERENCES
- 1.Garcia-Borreguero D, Odin P, Schwarz C. Restless legs syndrome: an overview of the current understanding and management. Acta Neurol Scand 2004;109:303–317. [DOI] [PubMed] [Google Scholar]
- 2.Kushida CA. Clinical presentation, diagnosis, and quality of life issues in restless legs syndrome. Am J Med 2007;120:S4–S12. [DOI] [PubMed] [Google Scholar]
- 3.Winkelman JW, Shahar E, Sharief I, Gottlieb DJ. Association of restless legs syndrome and cardiovascular disease in the Sleep Heart Health Study. Neurology 2008;70:35–42. [DOI] [PubMed] [Google Scholar]
- 4.Rothdach AJ, Trenkwalder C, Haberstock J, Keil U, Berger K. Prevalence and risk factors of RLS in an elderly population: the MEMO study: memory and morbidity in Augsburg elderly. Neurology 2000;54:1064–1068. [DOI] [PubMed] [Google Scholar]
- 5.Phillips B, Hening W, Britz P, Mannino D. Prevalence and correlates of restless legs syndrome: results from the 2005 National Sleep Foundation Poll. Chest 2006;129:76–80. [DOI] [PubMed] [Google Scholar]
- 6.Lopes LA, Lins C, de M, et al. Restless legs syndrome and quality of sleep in type 2 diabetes. Diabetes Care 2005;28:2633–2636. [DOI] [PubMed] [Google Scholar]
- 7.Phillips B, Young T, Finn L, Asher K, Hening WA, Purvis C. Epidemiology of restless legs symptoms in adults. Arch Intern Med 2000;160:2137–2141. [DOI] [PubMed] [Google Scholar]
- 8.Allen RP, Walters AS, Montplaisir J, et al. Restless legs syndrome prevalence and impact: REST general population study. Arch Intern Med 2005;165:1286–1292. [DOI] [PubMed] [Google Scholar]
- 9.Allen RP. Controversies and challenges in defining the etiology and pathophysiology of restless legs syndrome. Am J Med 2007;120:S13–21. [DOI] [PubMed] [Google Scholar]
- 10.Paulus W, Trenkwalder C. Less is more: pathophysiology of dopaminergic-therapy-related augmentation in restless legs syndrome. Lancet Neurol 2006;5:878–886. [DOI] [PubMed] [Google Scholar]
- 11.Wang GJ, Volkow ND, Logan J, et al. Brain dopamine and obesity. Lancet 2001;357:354–357. [DOI] [PubMed] [Google Scholar]
- 12.Ohayon MM, Roth T. Prevalence of restless legs syndrome and periodic limb movement disorder in the general population. J Psychosom Res 2002;53:547–554. [DOI] [PubMed] [Google Scholar]
- 13.Kim J, Choi C, Shin K, et al. Prevalence of restless legs syndrome and associated factors in the Korean adult population: the Korean Health and Genome Study. Psychiatry Clin Neurosci 2005;59:350–353. [DOI] [PubMed] [Google Scholar]
- 14.Sevim S, Dogu O, Kaleagasi H, Aral M, Metin O, Camdeviren H. Correlation of anxiety and depression symptoms in patients with restless legs syndrome: a population based survey. J Neurol Neurosurg Psychiatry 2004;75:226–230. [PMC free article] [PubMed] [Google Scholar]
- 15.Rimm EB, Stampfer MJ, Colditz GA, Chute CG, Litin LB, Willett WC. Validity of self-reported waist and hip circumferences in men and women. Epidemiology 1990;1:466–473. [DOI] [PubMed] [Google Scholar]
- 16.Stunkard AJ, Sorensen T, Schulsinger F. Use of the Danish Adoption Register for the study of obesity and thinness. Res Publ Assoc Res Nerv Ment Dis 1983;60:115–120. [PubMed] [Google Scholar]
- 17.Weisskopf MG, Chen H, Schwarzschild MA, Kawachi I, Ascherio A. Prospective study of phobic anxiety and risk of Parkinson’s disease. Mov Disord 2003;18:646–651. [DOI] [PubMed] [Google Scholar]
- 18.Berlin JA, Longnecker MP, Greenland S. Meta-analysis of epidemiologic dose-response data. Epidemiology 1993;4:218–228. [DOI] [PubMed] [Google Scholar]
- 19.Sevim S, Dogu O, Camdeviren H, et al. Unexpectedly low prevalence and unusual characteristics of RLS in Mersin, Turkey. Neurology 2003;61:1562–1569. [DOI] [PubMed] [Google Scholar]
- 20.Rajaram SS, Shanahan J, Ash C, Walters AS, Weisfogel G. Enhanced external counter pulsation (EECP) as a novel treatment for restless legs syndrome (RLS): a preliminary test of the vascular neurologic hypothesis for RLS. Sleep Med 2005;6:101–106. [DOI] [PubMed] [Google Scholar]
- 21.Hamdi A, Porter J, Prasad C. Decreased striatal D2 dopamine receptors in obese Zucker rats: changes during aging. Brain Res 1992;589:338–340. [DOI] [PubMed] [Google Scholar]
- 22.Huang XF, Zavitsanou K, Huang X, et al. Dopamine transporter and D2 receptor binding densities in mice prone or resistant to chronic high fat diet-induced obesity. Behav Brain Res 2006;175:415–419. [DOI] [PubMed] [Google Scholar]
- 23.Need AC, Ahmadi KR, Spector TD, Goldstein DB. Obesity is associated with genetic variants that alter dopamine availability. Ann Hum Genet 2006;70:293–303. [DOI] [PubMed] [Google Scholar]
- 24.Abbott RD, Ross GW, White LR, et al. Midlife adiposity and the future risk of Parkinson’s disease. Neurology 2002;59:1051–1057. [DOI] [PubMed] [Google Scholar]
- 25.Hu G, Jousilahti P, Nissinen A, Antikainen R, Kivipelto M, Tuomilehto J. Body mass index and the risk of Parkinson disease. Neurology 2006;67:1955–1959. [DOI] [PubMed] [Google Scholar]
- 26.Chen H, Zhang SM, Schwarzschild MA, Hernan MA, Willett WC, Ascherio A. Obesity and the risk of Parkinson’s disease. Am J Epidemiol 2004;159:547–555. [DOI] [PubMed] [Google Scholar]
- 27.Allen RP, Picchietti D, Hening WA, Trenkwalder C, Walters AS, Montplaisi J. Restless legs syndrome: diagnostic criteria, special considerations, and epidemiology: a report from the restless legs syndrome diagnosis and epidemiology workshop at the National Institutes of Health. Sleep Med 2003;4:101–119. [DOI] [PubMed] [Google Scholar]
- 28.Winkelmann J, Schormair B, Lichtner P, et al. Genome-wide association study of restless legs syndrome identifies common variants in three genomic regions. Nat Genet 2007;39:1000–1006. [DOI] [PubMed] [Google Scholar]
- 29.Stefansson H, Rye DB, Hicks A, et al. A genetic risk factor for periodic limb movements in sleep. N Engl J Med 2007;357:639–647. [DOI] [PubMed] [Google Scholar]
- 30.Ascherio A, Rimm EB, Giovannucci E, Willett WC, Stampfer MJ. Blood donations and risk of coronary heart disease in men. Circulation 2001;103:52–57. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.