

Abstract
Objective
The multiplanar display is a modality that allows the simultaneous visualization of three orthogonal planes from volume datasets obtained with three- (3D) and four-dimensional (4D) ultrasonography. Simultaneous display of standard views used in fetal echocardiography and their orthogonal planes may provide novel sonographic views for examination of the fetal heart and its vascular connections. This study was designed to determine the clinical utility of the multiplanar display in the examination of abnormal vascular connections to the fetal heart.
Methods
We reviewed four-dimensional volume datasets, acquired with the spatiotemporal image correlation technique (STIC), from patients with abnormal vascular connections to the fetal heart. Multiplanar views of the fetal heart were used to simultaneously display standard planes used in fetal echocardiography and their corresponding orthogonal planes.
Results
This study included four volume datasets from fetuses with confirmed abnormal vascular connections to the heart including: 1) interrupted inferior vena cava with azygos or hemiazygos vein continuation; 2) persistent left superior vena cava draining into a dilated coronary sinus; and 3) a dilated superior vena cava associated to a thoracic lymphangioma. Simultaneous visualization of orthogonal planes displaying abnormal vascular connections to the fetal heart facilitated the identification of the abnormal vessels and their spatial relationships with other vascular structures.
Conclusion
Multiplanar imaging can be used to assess abnormal vascular connections to the fetal heart and may provide novel sonographic planes for fetal echocardiography using 3D and 4D ultrasonography.
Keywords: Fetal echocardiography, vascular connections, STIC, spatiotemporal, congenital heart disease, prenatal diagnosis
Introduction
Prenatal visualization of abnormal venous connections to the fetal heart with two-dimensional (2D) ultrasonography requires the examiner to continuously scan these vascular structures in multiple sonographic planes. This process also involves simultaneous analysis of anatomic structures through mental reconstruction of their spatial relationships. This process can be facilitated using three- and four-dimensional (3D/4D) ultrasonography. For example, power Doppler reconstruction of 3D and 4D volume datasets have been used to visualize the spatial configuration of abnormal vasculature in the fetal liver,1,2 other vascular territories1,3 and abnormal arterial connections to the fetal heart.4,5 Recently, 3D and 4D rendering algorithms including the minimum projection mode,6 inversion mode,7–9 and B-flow10–14 have been employed to visualize normal and abnormal vascular connection to the fetal heart. However, these rendering algorithms frequently require image optimization increasing the time needed for off-line volume analysis.
Volume datasets obtained with 3D and 4D ultrasonography can be compared to blocks of pathologic specimens where the anatomic and, in some instances, functional-information, obtained will depend on the level that the block or volume is cut. Multiplanar imaging is a unique display modality (available in 3D and 4D ultrasonography) that allows for the simultaneous visualization of three anatomic planes, which are orthogonal to each other: the transverse, sagittal and coronal planes. Using the analogy of the block of pathological specimen, the multiplanar display would allow the simultaneous visualization of three sections of the block that are perpendicular to each other. Moreover, an imaging tool referred to as the “reference dot” can be used to localize the same anatomic structure in these three orthogonal planes.
Multiplanar display has been used in the evaluation of the fetal heart9,15–21 and other fetal structures.1,22–26 However, a systematic approach for the use of this display modality in the evaluation of abnormal vascular connections to the fetal heart has not been reported. The objective of this study was to describe a standardized method to use the multiplanar display in the evaluation of abnormal vascular connections to the fetal heart.
Material and Methods
Volume Acquisition and Analysis
Four-dimensional volume datasets of the fetal heart were acquired with transverse sweeps through the fetal chest. Multiplanar views of the fetal heart were used to simultaneously display the standard planes used in fetal echocardiography and their corresponding orthogonal planes. Patients with confirmed abnormal vascular connections to the fetal heart by post-natal echocardiography or during surgery were included in this study. Examinations were performed with STIC (Voluson 730 Expert, release BTO4, GE Healthcare, Milwaukee, Wisconsin, USA) using hybrid mechanical and curved array transducers (RAB 4–8P, RAB 4–8L, RAB 2–5P, RAB 2–5L). Acquisition time ranged from 7.5 to 15 seconds and the angle of acquisition ranged between 20 and 40 degrees, depending on fetal motion and gestational age.
After removal of patient identifiers, ultrasound images were retrospectively reviewed offline with the use of the 4DView software version 5.0 (4D VIEW 5.0, General Electric Medical Systems, Kretztechnik, Zipf, Austria). The volume dataset considered by the investigator to be of highest quality was selected on the basis of the following characteristics: 1) the fetal spine was positioned between 3 and 9 o’clock, minimizing the possibility of shadowing from the ribs or spine; and 2) minimal or no motion artifact were observed on the sagittal plane. B-mode and color Doppler ultrasonography was used to acquire all volume datasets.
Visualization of the orthogonal planes
All volume datasets were analyzed using a multiplanar display, which allows simultaneous display of images in three orthogonal planes (panels A, B and C, Figure 1) as follows:
Figure 1.
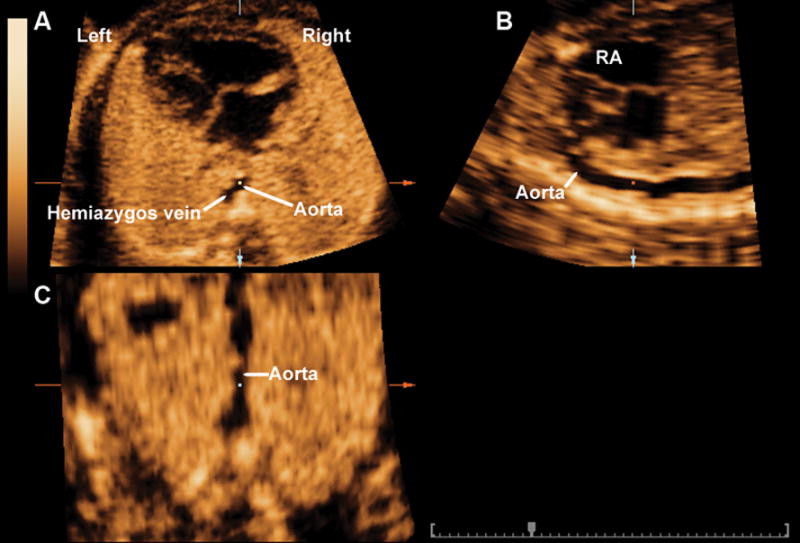
Multiplanar display of the sagittal view of the ductal arch in a fetus with an interrupted left-sided inferior vena cava with hemiazygos continuation. The four-chamber view is displayed in panel A, in which a “two-vessel sign” can be seen, representing the hemiazygos vein to left of the aorta. The sagittal view of the ductal arch and the coronal view of the aorta are displayed in panels B and C, respectively. RA: right atrium.
Standard views used in fetal echocardiography including the three-vessel view and four chamber view were displayed in panel A.
The reference dot was positioned in the abnormal vascular structure in panel A to identify the nature of the vessel and its connections with the help of the sagittal and coronal planes in panels B and C, respectively. In some instances, the sagittal view was optimized by rotating the coronal view of the abnormal vessel to a vertical position in panel C.
All patients were enrolled in research protocols approved by the Institutional Review Board of the National Institute of Child Health and Human Development (NICHD/NIH/DHHS), as well as the Human Investigation Committees of both Wayne State University (Detroit, Michigan, USA) and William Beaumont Hospital (Royal Oak, Michigan, USA). All women signed a written informed consent before participating in the study.
Results
This study included four volume datasets from fetuses with the following abnormal vascular connections to the heart: 1) interrupted inferior vena cava (IVC) with azygos (n=1) or hemiazygos (n=1) vein continuation; 2) persistent left superior vena cava (SVC) draining into a dilated coronary sinus (n=1); and 3) a dilated SVC associated to a thoracic lymphangioma (n=1). These diagnoses were confirmed by neonatal echocardiography and/or during postnatal surgical correction.
The simultaneous visualization of orthogonal planes displaying abnormal vascular connections to the fetal heart facilitated the identification of the abnormal vessel and the visualization of its spatial relationships with other vascular structures. Indeed, in two cases of interrupted inferior vena cava with azygos or hemiazygos vein continuation, the placement of the reference dot in the dilated azygos/hemiazygos vein in the four chamber view of the heart in panel A, allowed for the visualization of the sagittal view of the azygos or hemiazygos vein draining into either the SVC or persistent left SVC in panel B, and the visualization of the coronal view of the dilated azygos/hemiazygos vein in panel C (Figures 2, 3 and 4). The rotation of the coronal view of the azygos/hemiasygos veins to a vertical position allowed the visualization of the sagittal view of these vessels in panel B.
Figure 2.
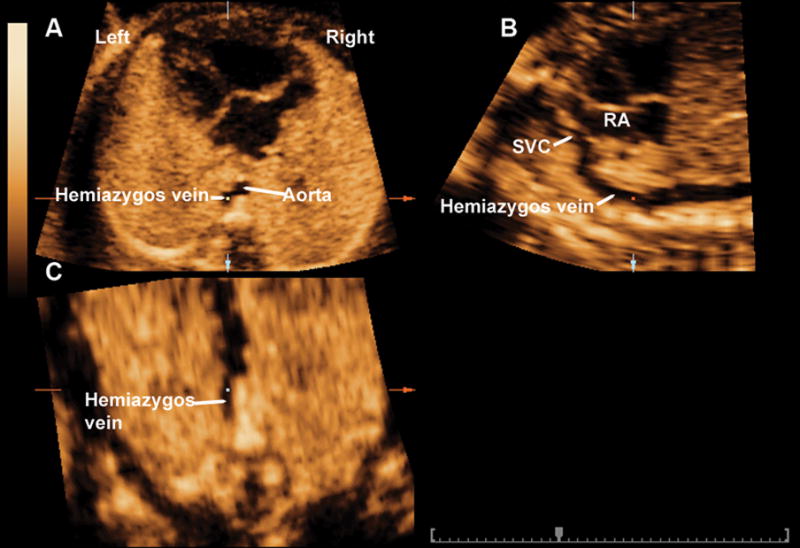
Multiplanar display of a dilated hemiazygos vein in a fetus with interrupted left-sided inferior vena cava with hemiazygos continuation. The reference dot was placed in the dilated hemiazygos vein in the four chamber view of the heart (panel A). This allowed for both the visualization of both the sagittal view of the hemiazygos vein in panel B and the coronal view of the dilated hemiazygos vein in panel C. Rotation of the coronal view to a vertical position on panel C allowed for visualization of the dilated hemiazygos vein draining into a persistent left SVC. SVC: superior vena cava; RA: right atrium.
Figure 3.
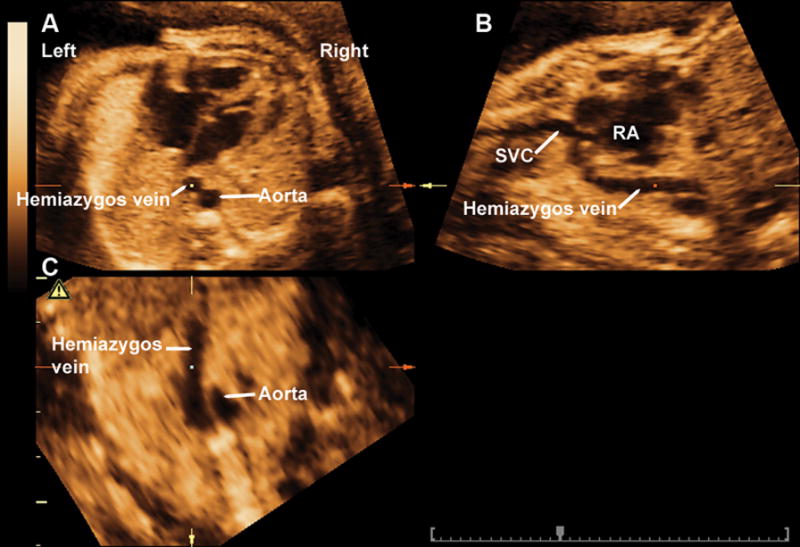
Multiplanar display of a dilated hemiazygos vein in a fetus with interrupted inferior vena cava and dextrocardia. The reference dot was placed in the dilated hemiazygos vein in the four chamber view of the heart in panel A. This allowed for both the visualization of the sagittal view of the hemiazygos vein in panel B and the coronal view of the dilated hemiazygos vein in panel C. Rotation of the coronal view to a vertical position in panel C allowed for the visualization of the dilated hemiazygos vein draining into the SVC. SVC: superior vena cava; RA: right atrium.
Figure 4.
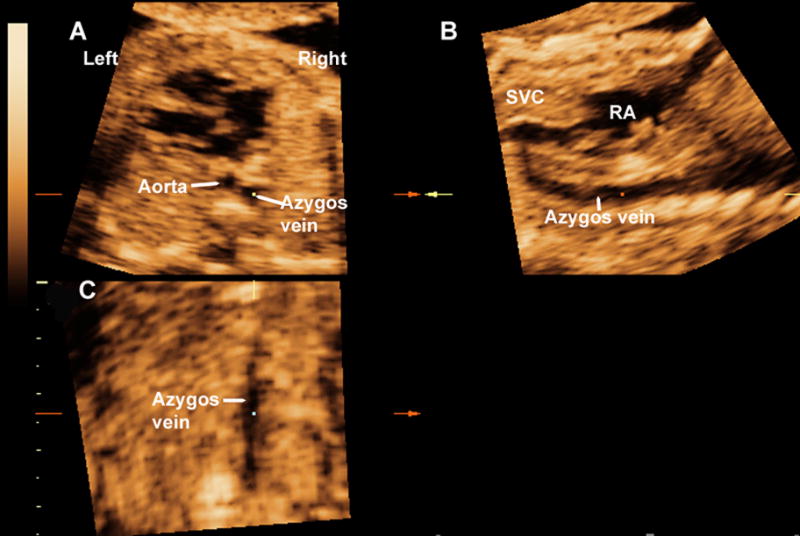
Multiplanar display of a dilated azygos vein in a fetus with interrupted inferior vena cava. The reference dot was placed in the dilated azygos vein (located to right of the aorta) in the four chamber view of the heart (panel A). This allowed for both the visualization of the sagittal view of the azygos vein in panel B and the coronal view of the dilated azygos vein in panel C. The rotation of the coronal view to a vertical position in panel C allowed for the visualization of the dilated azygos vein draining into the SVC. SVC: superior vena cava; RA: right atrium.
Figure 5a and video clip 1 represent the multiplanar display of the three-vessel view of a fetus with persistent left SVC and dilated coronary sinus. Of note, the persistent left SVC was suspected based on the latter sonographic finding and not due to visualization of an additional vascular structure in the three-vessel view. Panel A displays the three-vessel view where the reference dot was placed on the additional vascular structure to the left of the pulmonary artery. This allowed for the clear visualization of a vascular structure joining a dilated coronary sinus in the sagittal (panel B) and coronal views (panel C). The same procedure was adopted to document the normal vascular connection of the normal (right sided) SVC (Figure 5b, video clip 2).
Figure 5.
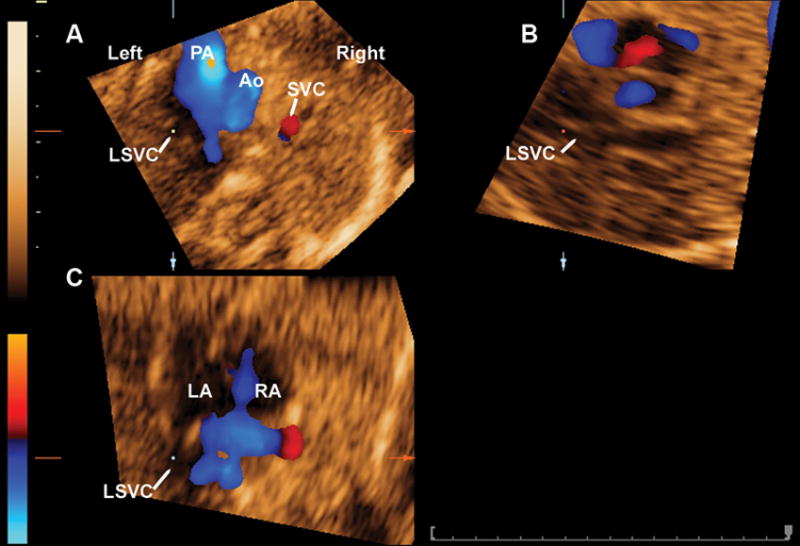
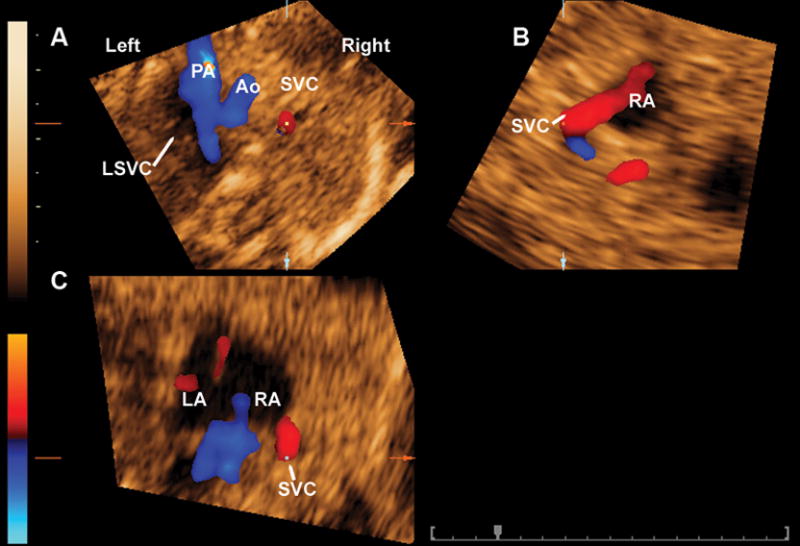
A) Figure 5a shows the mutiplanar display of the three-vessel view of a fetus with persistent left SVC with dilated coronary sinus. The reference dot was placed on the vascular structure to the left of the pulmonary artery (panel A), which allowed for the clear visualization of a vascular structure (panel B) joining a dilated coronary sinus, which is projected into the left atrium (panel C). B) The same procedure was used to document the normal vascular connections of the SVC (Figure 5b). PA: pulmonary artery; Ao: aorta; LSVC: left superior vena cava; SVC: superior vena cava; RA; right atrium; LA: left atrium.
Figure 6 represents the multiplanar display of the three-vessel view of a fetus with a lymphagioma of the upper part of the chest draining into the SVC. The SVC is markedly dilated in the three-vessel view in panel A. Panels B and C show that the dilated SVC drains into the right atrium. In addition, the coronal view in panel C shows part of the lymphagioma draining into the dilated SVC.
Figure 6.
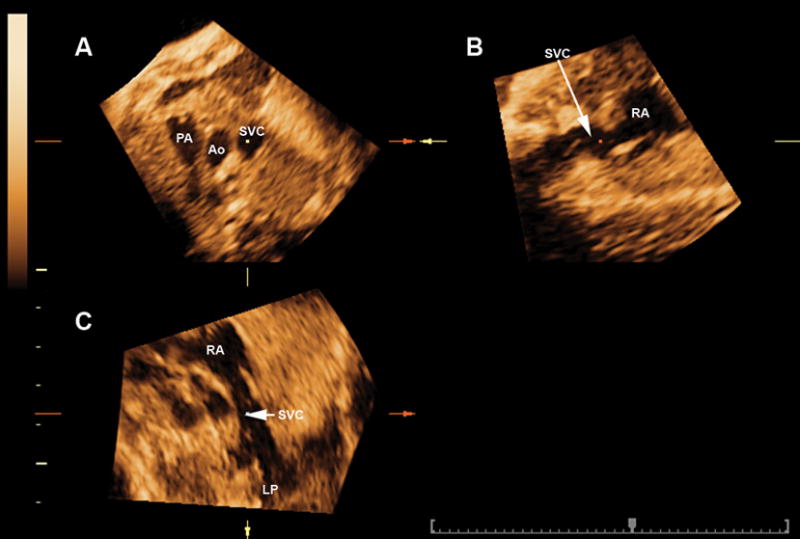
Multiplanar display of the three-vessel view of a fetus with a lymphagioma on the upper chest draining into the SVC. The SVC is markedly dilated in the three-vessel view in panel A. Panels B and C show that the dilated SVC drains into the right atrium. In addition, panel C shows part of the lymphagioma draining into the dilated SVC. PA: pulmonary artery; Ao: aorta; SVC: superior vena cava; RA; right atrium; LP: lymphangioma.
Discussion
Our study shows that multiplanar display may facilitate the identification of abnormal vascular connections to the fetal heart, as well as the visualization of their spatial relationships.
Two-dimensional (2D) ultrasonography relies on standard anatomic planes for the examination of the fetal heart, including the four-chamber view, three-vessel and trachea view, and the left and right outflow tracts.27–32 However, visualization of abnormal venous connections to the fetal heart with two-dimensional (2D) ultrasonography requires the examiner to scan these vascular structures in multiple scanning planes to obtain a mental reconstruction of their spatial relationships. This process can be facilitated with the help of display modalities used in 3D and 4D ultrasonography including power Doppler reconstruction 3D and 4D volume datasets,1–5 minimum projection mode,6 inversion mode,7–9 and B-flow.10–14
The multiplanar display allows for the simultaneous visualization of three orthogonal planes from volume datasets obtained with 3D and 4D ultrasonography. A central feature of this display modality is the ability to focus on a specific anatomic structure in panel A by placing the reference dot in the structure and visualizing the same structure in two perpendicular planes displayed in panels B and C (Figure 1). With this approach, we demonstrated that the simultaneous display of orthogonal planes of abnormal vascular connections to the fetal heart facilitated the identification of the nature of the abnormal vessel and the visualization of its spatial relationships with other vascular structures. Indeed, the multiplanar view allowed for the visualization of the drainage of dilated azygos or hemiazygos17 veins into the SVC (Figures 2 and 3).
A dilated coronary sinus is frequently associated with a persistent left SVC,33,34 which can be identified using the three vessel view. However, the cross-section of a fourth vessel to the left of the pulmonary artery is not always clearly visualized. In these cases, placement of the reference dot in the abnormal vessel and its simultaneous display in the sagittal and coronal views may help to confirm its vascular nature and visualize its connections to the fetal heart (see Figure 5a). The motion provided by volume datasets obtained with color Doppler and STIC facilitated this process (video clips 1 and 2). However, the multiplanar display could possibly be used to examine abnormal vascular connections to the fetal heart using volume datasets obtained with 3D ultrasonography.
The association of a lymphangioma and a dilated SVC in the fetus has not been reported. In adults, lymphangiohemangiomas of the mediastinum are rare and has been associated with the presence of persistent left SVC.35 The multiplanar display of the SVC described herein allowed the simultaneous visualization of a dilated SVC in the three-vessel view, the drainage of the SVC to the right atrium in the sagittal view, and drainage of the lymphangioma draining into the SVC in the coronal plane.
Collectively, the results of this study indicate that a systematic approach for the use of mutiplanar display in 3D and 4D ultrasonography provides important insight into their nature and spatial relationships of abnormal vascular connections to the fetal heart.
Video clip 1. Multiplanar display of the three-vessel view of a fetus with persistent left SVC associated with a dilated coronary sinus. The reference dot was placed on the vascular structure to the left of the pulmonary artery (panel A), which allowed for the clear visualization of a vascular structure (panel B) joining a dilated coronary sinus, which is projected into the left atrium (panel C).
Video clip 2. Multiplanar display of the three-vessel view of a fetus with persistent left superior vena cava (SVC) associated with a dilated coronary sinus. The reference dot was placed on the SVC (panel A), which allowed for the clear visualization of the SVC draining into the right atrium in the sagittal (panel B) and coronal (panel C) views.
Supplementary Material
{kind=link}
{kind=link}
Acknowledgments
This research was supported by the Intramural Research Program of the National Institute of Child Health and Human Development, NIH, DHHS.
Reference List
- 1.Lee W, Kalache KD, Chaiworapongsa T, et al. Three-dimensional power Doppler ultrasonography during pregnancy. J Ultrasound Med. 2003;22:91–97. doi: 10.7863/jum.2003.22.1.91. [DOI] [PubMed] [Google Scholar]
- 2.Kalache K, Romero R, Goncalves LF, et al. Three-dimensional color power imaging of the fetal hepatic circulation. Am J Obstet Gynecol. 2003;189:1401–1406. doi: 10.1067/s0002-9378(03)00774-9. [DOI] [PubMed] [Google Scholar]
- 3.Ruano R, Benachi A, Aubry MC, et al. Perinatal three-dimensional color power Doppler ultrasonography of vein of Galen aneurysms. J Ultrasound Med. 2003;22:1357–1362. doi: 10.7863/jum.2003.22.12.1357. [DOI] [PubMed] [Google Scholar]
- 4.Chaoui R, Schneider MB, Kalache KD. Right aortic arch with vascular ring and aberrant left subclavian artery: prenatal diagnosis assisted by three-dimensional power Doppler ultrasound. Ultrasound Obstet Gynecol. 2003;22:661–663. doi: 10.1002/uog.933. [DOI] [PubMed] [Google Scholar]
- 5.Goncalves LF, Romero R, Espinoza J, et al. Four-dimensional ultrasonography of the fetal heart using color Doppler spatiotemporal image correlation. J Ultrasound Med. 2004;23:473–481. doi: 10.7863/jum.2004.23.4.473. [DOI] [PubMed] [Google Scholar]
- 6.Espinoza J, Goncalves LF, Lee W, et al. The use of the minimum projection mode in 4-dimensional examination of the fetal heart with spatiotemporal image correlation. J Ultrasound Med. 2004;23:1337–1348. doi: 10.7863/jum.2004.23.10.1337. [DOI] [PubMed] [Google Scholar]
- 7.Goncalves LF, Espinoza J, Lee W, Mazor M, Romero R. Three- and four-dimensional reconstruction of the aortic and ductal arches using inversion mode: a new rendering algorithm for visualization of fluid-filled anatomical structures. Ultrasound Obstet Gynecol. 2004;24:696–698. doi: 10.1002/uog.1754. [DOI] [PubMed] [Google Scholar]
- 8.Espinoza J, Goncalves LF, Lee W, Mazor M, Romero R. A novel method to improve prenatal diagnosis of abnormal systemic venous connections using three- and four-dimensional ultrasonography and ‘inversion mode’. Ultrasound Obstet Gynecol. 2005;25:428–434. doi: 10.1002/uog.1877. [DOI] [PubMed] [Google Scholar]
- 9.Benacerraf BR. Inversion mode display of 3D sonography: applications in obstetric and gynecologic imaging. AJR Am J Roentgenol. 2006;187:965–971. doi: 10.2214/AJR.05.1462. [DOI] [PubMed] [Google Scholar]
- 10.Pooh RK. New application of B-flow sono-angiography in perinatology. Ultrasound Obstet Gynecol. 2000;15:163. doi: 10.1046/j.1469-0705.2000.00025.x. [DOI] [PubMed] [Google Scholar]
- 11.Deng J, Rodeck CH. New fetal cardiac imaging techniques. Prenat Diagn. 2004;24:1092–1103. doi: 10.1002/pd.1066. [DOI] [PubMed] [Google Scholar]
- 12.Goncalves LF, Espinoza J, Lee W, et al. A new approach to fetal echocardiography: digital casts of the fetal cardiac chambers and great vessels for detection of congenital heart disease. J Ultrasound Med. 2005;24:415–424. doi: 10.7863/jum.2005.24.4.415. [DOI] [PubMed] [Google Scholar]
- 13.Pooh RK, Korai A. B-flow and B-flow spatio-temporal image correlation in visualizing fetal cardiac blood flow. Croat Med J. 2005;46:808–811. [PubMed] [Google Scholar]
- 14.Volpe P, Campobasso G, Stanziano A, et al. Novel application of 4D sonography with B-flow imaging and spatio-temporal image correlation (STIC) in the assessment of the anatomy of pulmonary arteries in fetuses with pulmonary atresia and ventricular septal defect. Ultrasound Obstet Gynecol. 2006;28:40–46. doi: 10.1002/uog.2818. [DOI] [PubMed] [Google Scholar]
- 15.Nelson TR, Pretorius DH, Sklansky M, Hagen-Ansert S. Three-dimensional echocardiographic evaluation of fetal heart anatomy and function: acquisition, analysis, and display. J Ultrasound Med. 1996;15:1–9. [PubMed] [Google Scholar]
- 16.DeVore GR, Falkensammer P, Sklansky MS, Platt LD. Spatio-temporal image correlation (STIC): new technology for evaluation of the fetal heart. Ultrasound Obstet Gynecol. 2003;22:380–387. doi: 10.1002/uog.217. [DOI] [PubMed] [Google Scholar]
- 17.Goncalves LF, Lee W, Chaiworapongsa T, et al. Four-dimensional ultrasonography of the fetal heart with spatiotemporal image correlation. Am J Obstet Gynecol. 2003;189:1792–1802. doi: 10.1016/s0002-9378(03)00913-x. [DOI] [PubMed] [Google Scholar]
- 18.Vinals F, Poblete P, Giuliano A. Spatio-temporal image correlation (STIC): a new tool for the prenatal screening of congenital heart defects. Ultrasound Obstet Gynecol. 2003;22:388–394. doi: 10.1002/uog.883. [DOI] [PubMed] [Google Scholar]
- 19.Abuhamad A. Automated multiplanar imaging: a novel approach to ultrasonography. J Ultrasound Med. 2004;23:573–576. doi: 10.7863/jum.2004.23.5.573. [DOI] [PubMed] [Google Scholar]
- 20.Chaoui R, Hoffmann J, Heling KS. Three-dimensional (3D) and 4D color Doppler fetal echocardiography using spatio-temporal image correlation (STIC) Ultrasound Obstet Gynecol. 2004;23:535–545. doi: 10.1002/uog.1075. [DOI] [PubMed] [Google Scholar]
- 21.Goncalves LF, Espinoza J, Romero R, et al. Four-dimensional fetal echocardiography with spatiotemporal image correlation (STIC): a systematic study of standard cardiac views assessed by different observers. J Matern Fetal Neonatal Med. 2005;18 doi: 10.1080/14767050500127765. in press. [DOI] [PubMed] [Google Scholar]
- 22.Garjian KV, Pretorius DH, Budorick NE, et al. Fetal skeletal dysplasia: three-dimensional US--initial experience. Radiology. 2000;214:717–723. doi: 10.1148/radiology.214.3.r00mr23717. [DOI] [PubMed] [Google Scholar]
- 23.Lee W, Kirk JS, Shaheen KW, et al. Fetal cleft lip and palate detection by three-dimensional ultrasonography. Ultrasound Obstet Gynecol. 2000;16:314–320. doi: 10.1046/j.1469-0705.2000.00181.x. [DOI] [PubMed] [Google Scholar]
- 24.Benoit B. The value of three-dimensional ultrasonography in the screening of the fetal skeleton. Childs Nerv Syst. 2003;19:403–409. doi: 10.1007/s00381-003-0776-3. [DOI] [PubMed] [Google Scholar]
- 25.Merz E, Welter C. 2D and 3D Ultrasound in the evaluation of normal and abnormal fetal anatomy in the second and third trimesters in a level III center. Ultraschall Med. 2005;26:9–16. doi: 10.1055/s-2004-813947. [DOI] [PubMed] [Google Scholar]
- 26.Mittal P, Goncalves LF, Kusanovic JP, et al. Objective evaluation of sylvian fissure development by multiplanar 3-dimensional ultrasonography. J Ultrasound Med. 2007;26:347–353. doi: 10.7863/jum.2007.26.3.347. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Allan L. Technique of fetal echocardiography. Pediatr Cardiol. 2004;25:223–233. doi: 10.1007/s00246-003-0588-y. [DOI] [PubMed] [Google Scholar]
- 28.Chaoui R. The examination of the normal fetal heart using two-dimensional fetal echocardiography. 2003:141–149. [Google Scholar]
- 29.Carvalho JS, Mavrides E, Shinebourne EA, Campbell S, Thilaganathan B. Improving the effectiveness of routine prenatal screening for major congenital heart defects. Heart. 2002;88:387–391. doi: 10.1136/heart.88.4.387. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Bromley B, Estroff JA, Sanders SP, et al. Fetal echocardiography: accuracy and limitations in a population at high and low risk for heart defects. Am J Obstet Gynecol. 1992;166:1473–1481. doi: 10.1016/0002-9378(92)91622-h. [DOI] [PubMed] [Google Scholar]
- 31.Benacerraf BR. Sonographic detection of fetal anomalies of the aortic and pulmonary arteries: value of four-chamber view vs direct images. AJR Am J Roentgenol. 1994;163:1483–1489. doi: 10.2214/ajr.163.6.7992752. [DOI] [PubMed] [Google Scholar]
- 32.Comstock CH. What to expect from routine midtrimester screening for congenital heart disease. Semin Perinatol. 2000;24:331–342. doi: 10.1053/sper.2000.16724. [DOI] [PubMed] [Google Scholar]
- 33.Chaoui R, Heling KS, Kalache KD. Caliber of the coronary sinus in fetuses with cardiac defects with and without left persistent superior vena cava and in growth-restricted fetuses with heart-sparing effect. Prenat Diagn. 2003;23:552–557. doi: 10.1002/pd.626. [DOI] [PubMed] [Google Scholar]
- 34.Rein AJ, Nir A, Nadjari M. The coronary sinus in the fetus. Ultrasound Obstet Gynecol. 2000;15:468–472. doi: 10.1046/j.1469-0705.2000.00142.x. [DOI] [PubMed] [Google Scholar]
- 35.Riquet M, Briere J, Pimpec-Barthes F, Puyo P. Lymphangiohemangioma of the mediastinum. Ann Thorac Surg. 1997;64:1476–1478. doi: 10.1016/S0003-4975(97)00937-5. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.