

Abstract
AIM: To examine if the rate of decrease in serum bilirubin after preoperative biliary drainagecan be used as a predicting factor for surgical complications and postoperative recovery after pancreaticoduodenectomy in patients with distal common bile duct cancer.
METHODS: A retrospective study was performed in 49 consecutive patients who underwent pancreaticoduodenectomy for distal common bile duct cancer. Potential risk factors were compared between the complicated and uncomplicated groups. Also, the rates of decrease in serum bilirubin were compared pre- and postoperatively.
RESULTS: Preoperative biliary drainage (PBD) was performed in 40 patients (81.6%). Postoperative morbidity and mortality rates were 46.9% (23/49) and 6.1% (3/49), respectively. The presence or absence of PBD was not different between the complicated and uncomplicated groups. In patients with PBD, neither the absolute level nor the rate of decrease in serum bilirubin was significantly different. Patients with rapid decrease preoperatively showed faster decrease during the first postoperative week (5.5 ± 4.4 μmol/L vs -1.7 ± 9.9 μmol/L, P = 0.004).
CONCLUSION: PBD does not affect the surgical outcome of pancreaticoduodenectomy in patients with distal common bile duct cancer. There is a certain group of patients with a compromised hepatic excretory function, which is represented by the slow rate of decrease in serum bilirubin after PBD.
Keywords: Distal bile duct cancer, Drainage, Bilirubin, Rate
INTRODUCTION
In spite of recent advances in surgical techniques and perioperative management, pancreaticoduodenectomy still carries a significant morbidity and mortality[1,2]. Many studies have been performed to identify the high risk patients for the operation with inconsistent results. The diversity of those study results may be due in part to the heterogeneity of the disease entities included, and also to the patient’s conditions which in turn affect the outcome of the complex operative procedures. One of the prime interests has been the effectiveness of preoperative biliary drainage. Many studies favored the usefulness of biliary drainage in improving the surgical outcome[3–7], while others questioned its effectiveness[8–10], and even concluded it provokes more complications[11–15]. The underlying rationale for the preoperative decompression of the bile duct is that obstructive jaundice may interfere with the hepatic function, and relieving the obstruction could improve the recovery of the patients and hence the surgical results[16,17]. It was our impression that there are a certain group of patients whose concentration of total serum bilirubin drops faster after biliary drainage than others. Presumably, the more slowly the concentration of serum bilirubin drops, the higher the risk of developing complications following pancreaticoduodenectomy might be. If the surgical outcome is complicated by obstructive jaundice, this should be measured by not only the absolute concentration of serum bilirubin but also its rate of decrease after biliary drainage, which is the indicator for hepatic excretory dysfunction and further the presence of liver damage[18–21].
We conducted this study to examine whether the rate of decrease in the concentration of serum bilirubin, as well as its absolute preoperative level per se, are different between the patients with and without major complications after pancreaticoduodenectomy. To avoid skewed results by confounding variables, we included patients with distal common bile duct cancer only.
MATERIALS AND METHODS
Study patients and data collection
A retrospective chart review was done in 49 consecutive patients who received pancreaticoduodenectomy for distal common bile duct cancer from July 1996 to June 2005. Patients were divided into complicated and uncomplicated groups according to whether the complications occurred. We compared the potential risk factors including demo-graphic data, laboratory values, operative data and the history of preoperative biliary drainage between the two groups. Then, the patients with biliary drainage were divided further into two arbitrary subgroups with same sample size according to the rate of decrease in the concentration of serum bilirubin after preoperative biliary drainage, and the incidence of postoperative complications and the postoperative decrease in serum bilirubin were compared between the two subgroups.
Regarding the total serum bilirubin level, we used six parameters defined as follows: (1) the serum bilirubin at presentation as the initial bilirubin (Bi), (2) the preoperative concentration of serum bilirubin (Bo), (3) the ratio of decrease in serum bilirubin [(Bi-Bo)/Bi], (4) the rate of decrease in serum bilirubin per day [(Bi-Bo)/(days of biliary drainage)], (5) the rate of decrease in serum bilirubin during the first week following surgery (Bpod1), (6) the rate of decrease in serum bilirubin during the second week following surgery (Bpod2).
Preoperative biliary drainage
No absolute criterion existed for performing the preoperative biliary drainage. In general, when there were suspicions as to the nature of obstructive jaundice such as benign stricture and choledocholithiasis or malignant obstruction, endoscopic retrograde cholangiography (ERC) was performed for both diagnostic and therapeutic purposes. After the ERC, the patients were usually followed by endoscopic nasobiliary drainage (ENBD) to avoid secondary cholangitis. When malignant jaundice was strongly suspected, magnetic resonance cholangiography (MRC) was performed rather than ERC, in that MRC is a less invasive procedure than ERC. After the presence of malignant biliary obstruction was confirmed, the patients were either followed by percutaneous transhepatic biliary drainage (PTBD) or surgery at surgeon’s discretion. The absolute level of serum bilirubin was not regarded as a criterion for the timing of operation. In cases in which the preoperative biliary drainage was considered to be inadequate, in terms of the small daily drainage amount or suspicions for displacement, either the drainage was replaced or the operation schedule was advanced.
Operative procedures
The resection phase of pancreaticoduodenectomy consisted of the standard operative procedures including the regional lymphnode dissection of the porta hepatis, retropancreatic and celiac artery area. When the tumor was suspected to be advanced locally, the distal stomach was resected and the procedure was directed to the standard Whipple’s operation. Otherwise, the pylorus was preserved at the pylorus-preserving pancreaticoduodenectomy. The pancreatico-enteric anastomosis was done by either end-to-side pancreaticojejunostomy or duct to mucosa technique. Two active suction drains were applied at the pancreatico-enteric anastomosis site.
Definition of complications
Surgical mortality was defined as the death noted within 30 d postoperatively. Postoperative complications included delayed gastric emptying, pancreatic fistula, intraabdominal abscess and postoperative bleeding. Systemic complications such as pulmonary and cardiac complications were also noted. Delayed gastric emptying was defined as the inability to resume oral intake of food for more than 10 d postoperatively without the evidence of mechanical bowel obstruction. Pancreatic fistula was defined as a drain output more than 10 mL per day of amylase-rich fluid after postoperative day 8 or for more than 8 days postoperatively[22,23]. An intraabdominal abscess was present when there was pus collected intraperitoneally causing symptoms that warranted either surgical or interventional drainage. Postoperative bleeding was defined as a significant drop in hemoglobin concentration with the evidence of intraluminal and/or extraluminal bleeding that required re-exploration or interventional bleeding control. Minor complications such as wound infection that did not affect the overall recovery were not included in the complication.
Statistical analysis
For nominal variables, either χ2-test or Fisher’s exact test was applied where appropriate, and Mann-Whitney U test was used for interval variables. Because of the limited number of cases, multivariate analysis was considered inappropriate and not performed. Statistical analysis was done using SPSS for Windows Ver. 12.0.1 (SPSS Inc., Chicago, Illinois). A P value less than 0.05 was considered statistically significant.
RESULTS
Demographics of the 49 patients are summarized in Table 1. A total of 26 patients (53.1%) with no major complications were assigned to the uncomplicated group. The remaining 23 patients (46.9%) with major complications were classified as complicated group. In the complicated group, 3 patients (6.1%) died of complications. A detailed description of the morbidity and mortality is presented in Table 2. On univariate analysis, none of the age, sex, preoperative laboratory values and operative data was statistically different between the two groups.
Table 1.
Patient characteristics n (%)
| Demographics | Total | Uncomplicated | Complicated | P |
| (n = 49) | (n = 26) | (n = 23) | ||
| Age (yr) | 64.0 ± 8.9 | 62.0 ± 9.9 | 65.5 ± 7.3 | 0.228 |
| Sex | 0.475 | |||
| Male | 36 (73.5) | 18 (69.2) | 18 (78.3) | |
| Female | 13 (26.5) | 8 (30.8) | 5 (21.7) | |
| Diabetes | 0.483 | |||
| Yes | 10 (20.4) | 4 (15.4) | 6 (26.1) | |
| No | 39 (79.6) | 22 (84.6) | 17 (73.9) | |
| Operation | 0.879 | |||
| Whipple procedure | 24 (49.0) | 13 (50.0) | 11 (47.8) | |
| PPPD | 25 (51.0) | 13 (50.0) | 12 (52.2) | |
| Biliary drainage | 0.472 | |||
| Yes | 40 (81.6) | 20 (76.9) | 20 (87.0) | |
| No | 9 (18.4) | 6 (23.1) | 3 (13.0) | |
| 1Leukocytosis | 1.000 | |||
| Yes | 4 (8.2) | 2 (7.7) | 2 (8.7) | |
| No | 45 (91.8) | 24 (92.3) | 21 (91.3) | |
| Bilirubin (μmol/L) | 116.3 ± 92.3 | 107.7 ± 92.0 | 124.8 ± 97.5 | 0.652 |
| Albumin (g/L) | 34.2 ± 4.3 | 34.0 ± 4.4 | 34.4 ± 4.4 | 0.912 |
| Creatinine (μmol/L) | 70.7 ± 17.7 | 70.7 ± 26.5 | 70.7 ± 17.7 | 0.481 |
| Alkaline phosphatase (U/L) | 601 ± 450 | 632 ± 544 | 565 ± 322 | 0.764 |
| Hemoglobin (g/L) | 121.0 ± 16.5 | 117.8 ± 14.6 | 124.7 ± 18.0 | 0.193 |
| Hematocrit (%) | 35.6 ± 4.8 | 34.8 ± 4.3 | 36.4 ± 5.3 | 0.307 |
| Operation data | ||||
| Red cell transfusion (mL) | 522 ± 401 | 442 ± 358 | 613 ± 435 | 0.116 |
| Operation time (min) | 515 ± 107 | 510 ± 104 | 520 ± 111 | 0.825 |
Defined as leukocyte count more than 10.8 × 103/mm3. All laboratory values are preoperative serum levels expressed as mean ± SD, unless specified otherwise. PPPD: Pylorus preserving pancreaticoduodenectomy.
Table 2.
Surgical morbidity and mortality n (%)
| Morbidity and mortality | Number of patients |
| 1Morbidity | 23 (46.9) |
| Bleeding | 4 (8.2) |
| Intraabdominal abscess | 6 (12.2) |
| Pancreatic fistula | 7 (14.3) |
| Delayed gastric emptying | 7 (14.3) |
| Pulmonary complication | 2 (4.1) |
| Mortality | 3 (6.1) |
| Bleeding, DIC | 2 (4.1) |
| Intraabdominal abscess, sepsis | 1 (2.0) |
A patient may have more than one complication. DIC: Disseminated intravascular coagulation.
In our series, 40 patients (81.6%) underwent preoperative biliary drainage. There was no difference in the preoperative bilirubin level whether or not the biliary drainage procedure was performed between the uncomplicated and complicated groups (76.9% vs 87.0%, respectively, P = 0.472), although the preoperative bilirubin level was significantly lower in those patients without biliary drainage than in those with biliary drainage (41.0 ± 45.8 vs 132.2 ± 93.0 μmol/L, respectively, P = 0.001). The parameters related to the biliary drainage are shown in Table 3. ENBD was performed in 29 patients (72.5%) and PTBD in 11 patients (27.5%). The method of drainage was not different between the two groups. The initial, preoperative total serum bilirubin level or the duration of drainage was not different between the two groups. Also, neither the ratio nor the rate of decrease in serum bilirubin showed a statistically significant difference (P = 0.892 and 0.425, respectively), although there was a tendency for the rate of decrease in serum bilirubin to be higher in the uncomplicated group (Figure 1). The bilirubin drop during the first and second postoperative weeks was not different between the two groups. When the patients were regrouped according to the rate of decrease in serum bilirubin after biliary drainage, those with a rapid decrease preoperatively showed a significantly faster decrease during the first postoperative week as well, than those with a slower decrease preoperatively (P = 0.004). This difference was not seen during the second postoperative week (Table 4, Figure 2).
Table 3.
Analysis of preoperative biliary drainage-related factors n (%)
| Factors | Total | Uncomplicated | Complicated | P |
| (n = 40) | (n = 20) | (n = 20) | ||
| Drainage methods | 0.723 | |||
| ENBD | 29 (72.5) | 15 (75.0) | 14 (70.0) | |
| PTBD | 11 (27.5) | 5 (25.0) | 6 (30.0) | |
| Initial bilirubin (Bi) | 229.1 ± 135.1 | 210.3 ± 157.3 | 246.2 ± 111.2 | 0.223 |
| (μmol/L) | ||||
| Preop. bilirubin (Bo) | 131.7 ± 92.3 | 123.1 ± 94.1 | 140.2 ± 94.1 | 0.552 |
| (μmol/L) | ||||
| Duration of | 10 ± 9 | 8 ± 5 | 12 ± 12 | 0.392 |
| drainage (d) | ||||
| Decrease in bilirubin | 95.8 ± 104.3 | 87.2 ± 94.1 | 104.3 ± 114.6 | 0.715 |
| (Bi–Bo, dB, μmol/L) | ||||
| Ratio of decrease | 0.37 ± 0.35 | 0.37 ± 0.31 | 0.38 ± 0.40 | 0.892 |
| in bilirubin (dB/Bi) | ||||
| Rate of decrease | 10.1 ± 16.6 | 13.2 ± 14.5 | 7.0 ± 18.1 | 0.425 |
| in bilirubin | ||||
| (dB/d, μmol/L) | ||||
| Bpod1 (μmol/L) | 1.9 ± 8.6 | 4.4 ± 5.4 | -0.6 ± 10.3 | 0.180 |
| Bpod2 (μmol/L) | 2.2 ± 9.1 | 4.4 ± 5.8 | -0.1 ± 11.2 | 0.228 |
Variables are presented as mean ± SD, unless specified otherwise. ENBD: Endoscopic nasobiliary drainage; PTBD: Percutaneous transhepatic biliary drainage; Bpod1: Decrease in serum bilirubin during the first postoperative week; Bpod2: Decrease in serum bilirubin during the second postoperative week.
Figure 1.
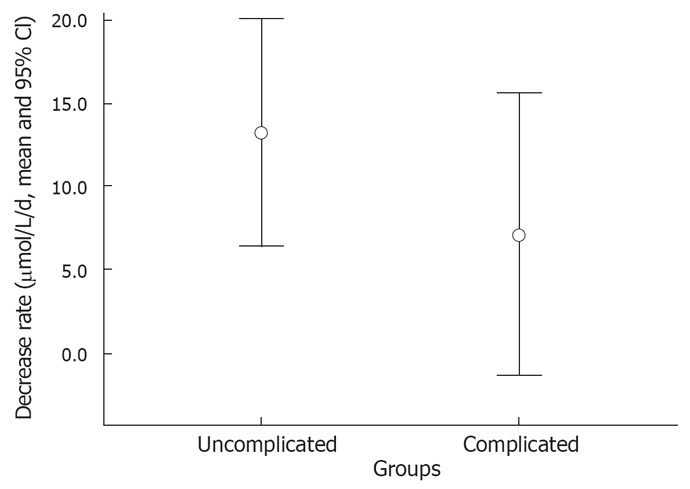
Rate of decrease in serum bilirubin comparing the uncomplicated and complicated groups (CI: Confidence interval).
Table 4.
Rate of decrease in serum bilirubin after preoperative biliary drainage n (%)
| Factors | Total (n = 40) | Fast decrease group (n = 20) | Slow decrease group (n = 20) | P |
| Drainage methods | 0.723 | |||
| ENBD | 29 (72.5) | 14 (70) | 15 (75) | |
| PTBD | 11 (27.5) | 6 (30) | 5 (25) | |
| Complication | 0.527 | |||
| Uncomplicated | 20 (50) | 11 (55) | 9 (45) | |
| Complicated | 20 (50) | 9 (45) | 11 (50) | |
| Bpod1 (μmol/L) | 1.9 ± 8.6 | 5.5 ± 4.4 | -1.7 ± 9.9 | 0.004 |
| Bpod2 (μmol/L) | 2.2 ± 9.1 | 1.9 ± 4.3 | 2.4 ± 12.3 | 0.818 |
Variables are presented as mean ± SD, unless specified otherwise. ENBD: Endoscopic nasobiliary drainage; PTBD: percutaneous transhepatic biliary drainage; Bpod1: decrease in serum bilirubin during the first postoperative week; Bpod2: decrease in serum bilirubin during the second postoperative week.
Figure 2.
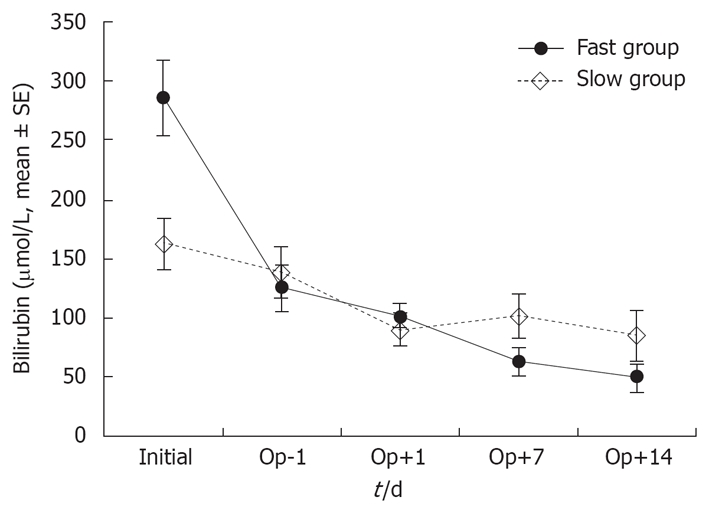
Changes in serum bilirubin comparing the fast and slow decrease groups (Op: Operation).
DISCUSSION
The effect of preoperative biliary drainage in preventing the operative complications after pancreaticoduodenectomy has been addressed in patients with obstructive jaundice due to periampullary tumors. To date, many studies have examined the issue with inconsistent results[10–12]. Periampullary tumors include various benign tumorous conditions such as chronic pancreatitis occurring at the periampullary region, in addition to the malignant lesions developed in the pancreas head, distal common bile duct, ampulla of Vater and duodenum. While the malignant diseases developing at the periampullary region have many characteristics in common, the biologic behavior of each is believed to be different from one another[24], which may in turn affect the surgical results. Also, the standard surgical procedure of pancreaticoduodenectomy is a complicated one with diverse technical variations, and the choice of reconstruction method and the extent of dissection may be dependent on both the operator and the disease entity. In analyzing the effect of preoperative biliary drainage, these factors are intermingled with each other, making the analysis difficult. To minimize the confounding variables, the present study limited the disease entity to the distal common bile duct cancers only. The rationale of selecting distal common bile duct cancers among the other periampullary malignancies is that these cancers are usually fairly confined within the periampullary region compared to the more aggressive diseases such as the pancreas head cancers, while the volume of cases in our database is large enough to make the statistical analysis valid. Nevertheless, it is not so large as to satisfy the requirements for the multivariate analysis, and we performed the univariate analysis only.
Many reports showed that the effectiveness of preoperative biliary drainage is measured by the surgical outcome following pancreaticoduodenectomy according to the specific complication items[8,9,14,15]. The surgical morbidities are commonly classified as bleeding, pancreatic leakage, intraabdominal abscess, delayed gastric emptying and others which include wound infection and systemic complications such as pneumonia or cardiac problems. While the complications are distinct entities clinically, the causes for each complication are either interrelated or obscure, and may be related to the basic fundamental defect, i.e. pancreaticojejunostomy failure[25–27]. Postoperative hemorrhage, when clinically significant, usually originates from the rupture of pseudoaneurysm, which in turn develops most frequently from the inflammatory erosion of arterial wall due to the leaked pancreatic juice[28]. Intraabdominal abscess can be caused by any leakage from the anastomoses, and the pancreaticoenteric anastomosis is the most frequent one to leak[27]. Also, the underlying mechanism of delayed gastric emptying is still unclear, but many authors suggest that the local inflammation induced by the leaked pancreatic enzymes may play an important role[27,29]. Some of the studies performed to date have classified the surgical results as complicated and uncomplicated[7,10–12]. This simple classification of surgical outcome measurement is advantageous in controlling as many confounding variables as possible. Surely, this simplified approach may not identify the risk factors predisposing the specific complications. However, based on the limited number of cases in the current study, it is more plausible to classify the surgical results as complicated and uncomplicated. In essence, this study was designed to investigate if the relief of obstructive jaundice preoperatively can reduce the incidence of the pancreatic anastomosis failure after pancreaticoduodenectomy.
Obstructive jaundice can cause tissue damage by various inflammatory mediators including oxygen free radicals[30]. Animal experiments suggested that the inflammatory mediators have a deleterious effect on not only the hepatic sinusoidal endothelium and then the hepatic function, but also the functions of other remote organs[31,32]. Both clinical and experimental studies have also shown that obstructive jaundice impairs the healing of abdominal wounds[33], although there is still a controversy in this series[17]. Arnaud et al[34] observed that the healing of gastric wounds and abdominal wounds, is delayed in experimentally jaundiced animals. Also, Takahashi[35] showed that the bursting strength of pancreaticojejunostomy is higher and the incidence of anastomotic leakage is lower in dogs with their concentration of serum bilirubin < 5 mg/dL. Considering such evidence, it seems prudent to assume that the high concentration of serum bilirubin is closely associated with the impaired healing of intestinal anastomoses, although the relevant mechanism and the magnitude of such association are still unclear.
Some studies have examined whether the relief of obstructive jaundice could improve the healing of anastomotic wound[36]. Vendemiale et al[16] showed that the impairment of hepatic redox status caused by cholestasis in patients with extra-hepatic biliary obstruction could be almost completely resolved by surgical biliary drainage. In addition, Koivukangas et al[17] observed that the decreased baseline collagen synthesis in jaundiced patients is partly restored by the resolution of jaundice, although the healing of the blister wound is not affected.
In spite of the scattered evidence that favors the possible positive effect of preoperative biliary drainage on the operative results after pancreaticoduodenectomy, many studies performed so far have failed to show any preferable impact. Povoski et al[11] have extensively reviewed the effectiveness of biliary drainage reported in the literature with their own experiences and concluded that the preoperative biliary drainage has no beneficial effect on the surgical results, and rather increases the infectious complications following pancreaticoduodenectomy. In another meta-analysis, Sewnath et al[10] also concluded that the preoperative biliary drainage prolongs hospital stay and has its own procedure-related complications without any proven positive effect on immediate postoperative results.
It is our experience that there is a certain group of patients whose serum bilirubin level decrease faster after biliary drainage procedures while there are others in whom the serum bilirubin fails to decrease effectively or even increases despite of good-functioning drainage route. We assume that if the surgical outcome is complicated by obstructive jaundice, this can be measured by not only the absolute serum bilirubin level[18,19], but also its rate of decrease after biliary drainage which is the indicator for hepatic excretory dysfunction and further the presence of liver damage. To date, a few studies have focused on the rate of decrease in the concentration of serum bilirubin[9,20,21]. Even though these studies may have their own limitations, such as the limited number of cases or the inclusion of heterogeneous disease entities, they have shown that the postoperative complications are more prone to develop in patients whose rate of decrease in the level of serum bilirubin is slower after drainage[20,21].
We used two indicators for the changes in the concentration of serum bilirubin: the ratio and rate. None of these indicators showed any statistically significant difference between the complicated and uncomplicated groups, although the serum bilirubin in the uncomplicated group tended to decrease faster than that in the complicated group after biliary drainage. To further investigate the postoperative recovery of hepatic excretory function, we divided the patients into two subgroups according to the rate of decrease in serum bilirubin after drainage. Patients with a higher rate of decrease in the concentration of serum bilirubin did not show a significantly lower rate of postoperative complications. In these patients, however, the rate of decrease in serum bilirubin was also higher during the first postoperative week. These results indicate that the rate of decrease in serum bilirubin after drainage can predict the immediate postoperative hepatic excretory functional recovery, although it cannot select high risk patients. Our results also show that there was a certain group of patients with their hepatic excretory function already compromised by obstructive jaundice before it was relieved by surgical resection of the causative lesion. These findings are in agreement with those presented by Sano et al[21], who showed that biliary obstruction causes liver damage represented by the slower rate of serum bilirubin decrease in patients who underwent biliary drainage.
Our study could not disclose the relationship between the compromised hepatic excretory function and surgical morbidity of pancreaticoduodenectomy. We think that the negative results may be due to the limited number of cases. Well-designed, prospective randomized studies in a larger number of cases are warranted to assess the clinical usefulness of the serum bilirubin decrease rate in selecting high risk patients to whom greater attention must be paid during surgery.
COMMENTS
Background
In spite of recent advances in surgical techniques and perioperative management, pancreaticoduodenectomy still carries a significant morbidity and mortality. Many studies have been performed to identify the high risk patients for the operation with inconsistent results. One of the prime interests has been the effectiveness of preoperative biliary drainage, but the issue is under debate.
Research frontiers
Many studies favored the usefulness of preoperative biliary drainage in improving the surgical outcome, while others questioned its effectiveness, and even concluded it provokes more complications. Further studies are warranted on the subject.
Innovations and breakthroughs
If the surgical outcome is complicated by obstructive jaundice, this should be measured by not only the absolute concentration of serum bilirubin but also its rate of decrease after biliary drainage, which is the indicator for hepatic excretory dysfunction and further the presence of liver damage. So far, few studies have focused on the rate of decrease in serum bilirubin.
Applications
We conducted this study to examine whether the rate of decrease in the concentration of serum bilirubin, as well as its absolute preoperative level per se, is different between the patients with and without major complications after pancreaticoduodenectomy. To avoid skewed results by confounding variables, we included patients with distal common bile duct cancer only.
Peer review
The study has certain merits since the authors consider several different variables for each patient. Also, the manuscript is easy to follow and its content is rich.
Supported by Inha University Research Grant
Peer reviewer: Giammarco Fava, MD, via Gervasoni 12, 60129 Ancona, Italy; Andreas Geier, Associate Professor, Department of Internal Medicine ¢ó, University Hospital Aachen, Aachen University (RWTH), Pauwelsstrasse 30, D-52074 Aache, Germany
S- Editor Zhu LH L- Editor Wang XL E- Editor Liu Y
References
- 1.Yeo CJ, Cameron JL, Sohn TA, Lillemoe KD, Pitt HA, Talamini MA, Hruban RH, Ord SE, Sauter PK, Coleman J, et al. Six hundred fifty consecutive pancreaticoduodenectomies in the 1990s: pathology, complications, and outcomes. Ann Surg. 1997;226:248–257; discussion 257-260. doi: 10.1097/00000658-199709000-00004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Tran KT, Smeenk HG, van Eijck CH, Kazemier G, Hop WC, Greve JW, Terpstra OT, Zijlstra JA, Klinkert P, Jeekel H. Pylorus preserving pancreaticoduodenectomy versus standard Whipple procedure: a prospective, randomized, multicenter analysis of 170 patients with pancreatic and periampullary tumors. Ann Surg. 2004;240:738–745. doi: 10.1097/01.sla.0000143248.71964.29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Denning DA, Ellison EC, Carey LC. Preoperative percutaneous transhepatic biliary decompression lowers operative morbidity in patients with obstructive jaundice. Am J Surg. 1981;141:61–65. doi: 10.1016/0002-9610(81)90013-1. [DOI] [PubMed] [Google Scholar]
- 4.Gundry SR, Strodel WE, Knol JA, Eckhauser FE, Thompson NW. Efficacy of preoperative biliary tract decompression in patients with obstructive jaundice. Arch Surg. 1984;119:703–708. doi: 10.1001/archsurg.1984.01390180065011. [DOI] [PubMed] [Google Scholar]
- 5.Robison R, Madura J, Scholten D, Lempke R, Rabe F, Glover J, Becker G, Cockerill E, Broadie T. Percutaneous transhepatic drainage for malignant biliary obstruction. Am Surg. 1984;50:329–333. [PubMed] [Google Scholar]
- 6.Kawarada Y, Higashiguchi T, Yokoi H, Vaidya P, Mizumoto R. Preoperative biliary drainage in obstructive jaundice. Hepatogastroenterology. 1995;42:300–307. [PubMed] [Google Scholar]
- 7.Adam U, Makowiec F, Riediger H, Schareck WD, Benz S, Hopt UT. Risk factors for complications after pancreatic head resection. Am J Surg. 2004;187:201–208. doi: 10.1016/j.amjsurg.2003.11.004. [DOI] [PubMed] [Google Scholar]
- 8.Martignoni ME, Wagner M, Krahenbuhl L, Redaelli CA, Friess H, Buchler MW. Effect of preoperative biliary drainage on surgical outcome after pancreatoduodenectomy. Am J Surg. 2001;181:52–59; discussion 87. doi: 10.1016/s0002-9610(00)00528-6. [DOI] [PubMed] [Google Scholar]
- 9.Sewnath ME, Birjmohun RS, Rauws EA, Huibregtse K, Obertop H, Gouma DJ. The effect of preoperative biliary drainage on postoperative complications after pancreaticoduodenectomy. J Am Coll Surg. 2001;192:726–734. doi: 10.1016/s1072-7515(01)00819-5. [DOI] [PubMed] [Google Scholar]
- 10.Sewnath ME, Karsten TM, Prins MH, Rauws EJ, Obertop H, Gouma DJ. A meta-analysis on the efficacy of preoperative biliary drainage for tumors causing obstructive jaundice. Ann Surg. 2002;236:17–27. doi: 10.1097/00000658-200207000-00005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Povoski SP, Karpeh MS Jr, Conlon KC, Blumgart LH, Brennan MF. Association of preoperative biliary drainage with postoperative outcome following pancreaticoduodenectomy. Ann Surg. 1999;230:131–142. doi: 10.1097/00000658-199908000-00001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Pisters PW, Hudec WA, Hess KR, Lee JE, Vauthey JN, Lahoti S, Raijman I, Evans DB. Effect of preoperative biliary decompression on pancreaticoduodenectomy-associated morbidity in 300 consecutive patients. Ann Surg. 2001;234:47–55. doi: 10.1097/00000658-200107000-00008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Srivastava S, Sikora SS, Kumar A, Saxena R, Kapoor VK. Outcome following pancreaticoduodenectomy in patients undergoing preoperative biliary drainage. Dig Surg. 2001;18:381–387. doi: 10.1159/000050178. [DOI] [PubMed] [Google Scholar]
- 14.Hodul P, Creech S, Pickleman J, Aranha GV. The effect of preoperative biliary stenting on postoperative complications after pancreaticoduodenectomy. Am J Surg. 2003;186:420–425. doi: 10.1016/j.amjsurg.2003.07.005. [DOI] [PubMed] [Google Scholar]
- 15.Jagannath P, Dhir V, Shrikhande S, Shah RC, Mullerpatan P, Mohandas KM. Effect of preoperative biliary stenting on immediate outcome after pancreaticoduodenectomy. Br J Surg. 2005;92:356–361. doi: 10.1002/bjs.4864. [DOI] [PubMed] [Google Scholar]
- 16.Vendemiale G, Grattagliano I, Lupo L, Memeo V, Altomare E. Hepatic oxidative alterations in patients with extra-hepatic cholestasis. Effect of surgical drainage. J Hepatol. 2002;37:601–605. doi: 10.1016/s0168-8278(02)00234-9. [DOI] [PubMed] [Google Scholar]
- 17.Koivukangas V, Oikarinen A, Risteli J, Haukipuro K. Effect of jaundice and its resolution on wound re-epithelization, skin collagen synthesis, and serum collagen propeptide levels in patients with neoplastic pancreaticobiliary obstruction. J Surg Res. 2005;124:237–243. doi: 10.1016/j.jss.2004.10.017. [DOI] [PubMed] [Google Scholar]
- 18.Chen CY, Shiesh SC, Lin XZ. Indicators of liver excretory function in patients undergoing biliary decompression for obstructive jaundice. Hepatogastroenterology. 1998;45:786–790. [PubMed] [Google Scholar]
- 19.Singh V, Kapoor VK, Saxena R, Kaushik SP. Recovery of liver functions following surgical biliary decompression in obstructive jaundice. Hepatogastroenterology. 1998;45:1075–1081. [PubMed] [Google Scholar]
- 20.Nakayama T, Tamae T, Kinoshita H, Okuda K, Imayama Y, Saitoh N, Shibata J, Aoki E, Hasuda A, Saitsu H. Evaluation of surgical risk in preoperative biliary drainage patients by blood chemistry laboratory data--with special reference to rate of reduction of serum bilirubin levels. Hepatogastroenterology. 1995;42:338–342. [PubMed] [Google Scholar]
- 21.Sano K, Kubota K, Bandai Y, Makuuchi M. Rate of bilirubin decrease as a risk predictor in hepato-biliary-pancreatic surgery. Hepatogastroenterology. 1999;46:2171–2177. [PubMed] [Google Scholar]
- 22.Bassi C, Butturini G, Molinari E, Mascetta G, Salvia R, Falconi M, Gumbs A, Pederzoli P. Pancreatic fistula rate after pancreatic resection. The importance of definitions. Dig Surg. 2004;21:54–59. doi: 10.1159/000075943. [DOI] [PubMed] [Google Scholar]
- 23.Bassi C, Dervenis C, Butturini G, Fingerhut A, Yeo C, Izbicki J, Neoptolemos J, Sarr M, Traverso W, Buchler M. Postoperative pancreatic fistula: an international study group (ISGPF) definition. Surgery. 2005;138:8–13. doi: 10.1016/j.surg.2005.05.001. [DOI] [PubMed] [Google Scholar]
- 24.Sarmiento JM, Nagomey DM, Sarr MG, Farnell MB. Periampullary cancers: are there differences? Surg Clin North Am. 2001;81:543–555. doi: 10.1016/s0039-6109(05)70142-0. [DOI] [PubMed] [Google Scholar]
- 25.Cullen JJ, Sarr MG, Ilstrup DM. Pancreatic anastomotic leak after pancreaticoduodenectomy: incidence, significance, and management. Am J Surg. 1994;168:295–298. doi: 10.1016/s0002-9610(05)80151-5. [DOI] [PubMed] [Google Scholar]
- 26.Grobmyer SR, Rivadeneira DE, Goodman CA, Mackrell P, Lieberman MD, Daly JM. Pancreatic anastomotic failure after pancreaticoduodenectomy. Am J Surg. 2000;180:117–120. doi: 10.1016/s0002-9610(00)00423-2. [DOI] [PubMed] [Google Scholar]
- 27.Niedergethmann M, Farag Soliman M, Post S. Postoperative complications of pancreatic cancer surgery. Minerva Chir. 2004;59:175–183. [PubMed] [Google Scholar]
- 28.Rumstadt B, Schwab M, Korth P, Samman M, Trede M. Hemorrhage after pancreatoduodenectomy. Ann Surg. 1998;227:236–241. doi: 10.1097/00000658-199802000-00013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Riediger H, Makowiec F, Schareck WD, Hopt UT, Adam U. Delayed gastric emptying after pylorus-preserving pancreatoduodenectomy is strongly related to other postoperative complications. J Gastrointest Surg. 2003;7:758–765. doi: 10.1016/s1091-255x(03)00109-4. [DOI] [PubMed] [Google Scholar]
- 30.Tu W, Kitade H, Satoi S, Zhang ZT, Kaibori M, Kwon AH, Kamiyama Y, Okumura T. Increased nitric oxide production in hepatocytes is involved in liver dysfunction following obstructive jaundice. J Surg Res. 2002;106:31–36. doi: 10.1006/jsre.2002.6436. [DOI] [PubMed] [Google Scholar]
- 31.Yoshidome H, Miyazaki M, Shimizu H, Ito H, Nakagawa K, Ambiru S, Nakajima N, Edwards MJ, Lentsch AB. Obstructive jaundice impairs hepatic sinusoidal endothelial cell function and renders liver susceptible to hepatic ischemia/reperfusion. J Hepatol. 2000;33:59–67. doi: 10.1016/s0168-8278(00)80160-9. [DOI] [PubMed] [Google Scholar]
- 32.Ito Y, Machen NW, Urbaschek R, McCuskey RS. Biliary obstruction exacerbates the hepatic microvascular inflammatory response to endotoxin. Shock. 2000;14:599–604. doi: 10.1097/00024382-200014060-00005. [DOI] [PubMed] [Google Scholar]
- 33.Grande L, Garcia-Valdecasas JC, Fuster J, Visa J, Pera C. Obstructive jaundice and wound healing. Br J Surg. 1990;77:440–442. doi: 10.1002/bjs.1800770426. [DOI] [PubMed] [Google Scholar]
- 34.Arnaud JP, Humbert W, Eloy MR, Adloff M. Effect of obstructive jaundice on wound healing. An experimental study in rats. Am J Surg. 1981;141:593–596. doi: 10.1016/0002-9610(81)90059-3. [DOI] [PubMed] [Google Scholar]
- 35.Takahashi S. The influence of obstructive jaundice on wound healing of pancreatico-jejunostomy with reference to the function of the pancreas as assessed by glucose tolerance and pancreozymin-secretin test. Nippon Geka Gakkai Zasshi. 1984;85:1332–1343. [PubMed] [Google Scholar]
- 36.O'Connor MJ. Mechanical biliary obstruction. A review of the multisystemic consequences of obstructive jaundice and their impact on perioperative morbidity and mortality. Am Surg. 1985;51:245–251. [PubMed] [Google Scholar]