

In comparison with other industrialized countries, the United States has exceptionally high rates of adolescent pregnancy and abortion. In 1999, nearly half of high-school students reported having had sexual intercourse, and 6 percent said they had been pregnant or gotten someone pregnant (CDC 2000). American adolescents are especially unlikely to use birth control, and those who do practice contraception tend to rely on inefficient methods (Forrest 1990).
Sexual behavior at first intercourse is of particular interest because early entry into sexual activity is associated with contraceptive nonuse and a heightened risk of pregnancy (Abma and Sonenstein 2001;Koenig and Zelnik 1982;Zabin, Kantner, and Zelnik 1979). Moreover, the timing of first intercourse may be a useful marker for risky sexual behavior and a history of sexually transmitted diseases (Greenberg, Magder, and Aral 1992). For example, age at first intercourse is inversely associated with the number of lifetime sexual partners (McGuire et al. 1992). This is important from a health policy perspective because the risk of contracting a sexually transmitted disease increases with the number of current and lifetime sex partners (Aral 2001).
Family-planning behavior at first intercourse also is important. Adolescents who use birth control at first sex—in particular, those who use medical methods—are especially likely to be consistent users of birth control later on (Sorensen 1973;Zelnik and Kanter 1978). Moreover, adolescents who practice contraception at first sex appear to have longer subsequent periods of nonexposure (Hayward, Grady, and Billy 1992) and are less likely to experience a premarital pregnancy (Mosher and McNally 1991). Information on adolescent contraceptive behavior is especially valuable in the development of strategies to help prevent the spread of sexually transmitted diseases (STDs). The majority of STD cases occur in individuals under the age of 25 (Wilson et al. 1994), and sexually active adolescents have especially high rates of gonorrhea and chlamydia, infections that may lead to pelvic inflammatory disease and infertility (Nguyet et al. 1994). While barrier methods of contraception such as condoms provide full or partial protection from a variety of diseases, including herpes simplex, chlamydia, gonorrhea, and HIV (Aral 2001;Mahler 1996; National Research Council 1989;Nguyet et al. 1994;Stigum et al. 1995), inconsistent contraceptive use is common among adolescents (Glei 1999). Moreover, methods such as withdrawal and rhythm fail to provide any protection against STDs.
A thorough understanding of the factors that influence adolescents’ sexual activity is of vital importance to policymakers concerned with designing effective sexual education programs and reducing the likelihood that adolescents will engage in unsafe sexual behaviors. Researchers investigating the role of familial factors in adolescents’ initiation into sexual activity and contraceptive use have identified a number of key determinants, including family structure, communication between parent and child, and parental supervision. At the same time, the research to date has not examined one potentially important familial factor—the extent to which parents engage in unsafe behaviors. To the extent that risky parental behavior is linked to precocious and unsafe sexual activity among adolescents, intervention strategies should encourage healthy behaviors in both adolescents and their parents. In this article we use nationally representative data to explore the impact of risky parental behaviors on early sexual activity and contraceptive use at first coitus among male and female adolescents in the United States.
Risky Parental Behavior and Adolescent Sexual Activity
Parents play a crucial role in defining normative behavior for their children (Foshee and Bauman 1992). In fact, many adolescents report that their parents, especially their mothers, are the most important people in their lives (Wilks 1986). Because parents serve as important role models for their children, it stands to reason that parents who exhibit unsafe behaviors are especially likely to have children with similar tendencies. Even though the effect of risky parental behaviors (i.e., those behaviors that endanger one's physical well-being or health) on adolescent sexual activity has not been studied, the strong links between parents’ and their children's participation in unhealthy activities have been documented. For example, parents who smoke are more likely to have children who smoke (Charlton and Blair 1989;Chassin et al. 1984;Flay et al. 1994;Foshee and Bauman 1992;Needle et al. 1986).
The likelihood of early sexual activity and teenage pregnancy is influenced by a variety of factors. For example, substance use among adolescents has been closely linked to permissive sexual attitudes (Whitbeck et al. 1993) and to sexual activity and teenage pregnancy (Biglan et al. 1990;Elliott and Morse 1989;Gillmore et al. 1992;Harvey and Spigner 1995;Hockaday et al. 2000;Mensch and Kandel 1992;Mott et al. 1996;Mott and Haurin 1988;Pugh et al. 1990;Streetman 1995;Udry, Kovenock, and Morris 1996;Zabin et al. 1986). Sexual activity is associated with relatively high rates of alcohol consumption and, among boys, with a tendency to engage in physical fights (Harvey and Spigner 1995). Because of the strong associations among alcohol use, cigarette smoking, marijuana use, general deviance, and precocious sex, many authors refer to these activities collectively as problem behavior. Problem behavior often reflects unconventionality in both personality and social environment (Donovan and Jessor 1985;Donovan, Jessor, and Costa 1988;Jessor, Donovan, and Costa 1991;Jessor and Jessor 1977;Pugh et al. 1990;Turbin, Jessor, and Costa 2000).
Adolescent problem behavior is most likely in families with high levels of conflict, low family involvement, and inadequate parental monitoring (Ary et al. 1999).Williams and associates (2000) found that adolescents who perceive their parents to be low in autonomy support are more likely to have extrinsic values (e.g., emphasis on fame as opposed to personal growth) and more likely to engage in a wide range of risky behaviors, including substance use and sexual activity. Children whose parents fail to accept and encourage their independence (those who overprotect, worry excessively about their children's health and safety, etc.) are also more likely to initiate sexual intercourse (Turner et al. 1993). At the same time, children whose parents are more liberal or approve of adolescent sexual activity are only slightly more likely than others to be sexually active. Moreover, these same children are especially likely to use contraception when they do have sex (Baker, Thalberg, and Morrison 1988). Recent research confirms that parental and peer expectations for alcohol use and engagement in sexual activity are significantly correlated with attitudes toward coitus among adolescents (Watts and Nagy 2000).
Parental supervision has been identified as a significant factor in understanding the variation in initiation of sexual activity among adolescents in the United States and elsewhere (Hogan and Kitagawa 1985; Meschke and Silbereisen 1997). Strict supervision of females who date has been shown to delay the onset of sexual activity (Hogan and Kitagawa 1985), and sexually active adolescents whose parents closely monitor them are especially likely to minimize their sexual risks (Rodgers 1999).Jemmott and Jemmott (1992) report that maternal strictness reduces the frequency of coital activity and that paternal strictness encourages more consistent use of condoms. Some research, however, suggests that the influence of parents’ supervision on adolescent sexual behavior is largely indirect. For example, Ary and colleagues (1999) found that poor parental monitoring was closely associated with a greater likelihood of association with deviant peers and with the subsequent development of problem behaviors.
Like parents, peers have a major impact on substance use among adolescents (see, e.g., Alexander et al. 1983;Ary et al. 1999;Charlton and Blair 1989;Chassin et al. 1984;Foshee and Bauman 1992;Mettlin 1976;Sarigiani, Ryan, and Petersen 1999;Urberg, Cheng, and Shyu 1991;Wilks, Callan, and Austin 1989). Teens with friends who smoke, drink, or use drugs are more often exposed to substance use and to the idea that such use is acceptable. At the same time, adolescents who drink or smoke may seek out friends with similar attitudes and behaviors (Grube and Morgan 1990). Association with deviant peers also encourages the transition from virginity to nonvirginity, particularly among females (Jessor and Jessor 1975). As Udry and Billy stated, “Friends influence the sexual behavior of friends” (1987, 843). For example, white female respondents’ sexual behavior was closely tied to their friends’ sexual behavior. No such effect was found among white boys, however, a finding that Udry and Billy attributed to girls’ more accurate knowledge of their friends’ sexual experiences.
Just as unsafe parental behavior increases the chance that adolescents will drink, smoke, or use drugs, parents who engage in risky behaviors may encourage early sexual activity and contraceptive nonuse by providing a model of low self-efficacy. We hypothesize that adolescents whose parents smoke, drink, or drive without seat belts are especially likely to engage in early and unsafe sexual activity. Moreover, we expect that the relationship between parents’ risky behaviors and their children's sexual practices can be only partially attributed to the link between parents’ risky behaviors (smoking, drinking, driving without wearing a seat belt) and adolescents’ risky behaviors (smoking, drinking, delinquent activity, association with substance-using peers).
Risky behaviors are defined here as those that jeopardize one's physical well-being. Risky peer associations are social relationships with persons who engage in such unsafe behaviors. (One exception to this rule is our inclusion of juvenile delinquency as a component of adolescent risky behavior. While delinquent behavior—stealing, selling drugs, and the like—does not necessarily endanger one's physical well-being, such activity violates social norms and threatens the adolescent's social well-being through the possibility of arrest, social ostracism, and so on.)
Our theoretical model is shown in figure 1. In this study we relied on a national sample of male and females adolescents to assess the extent to which risky behavior among parents influences the sexual activity of adolescents and their use of contraception at first coitus.
fig. 1.
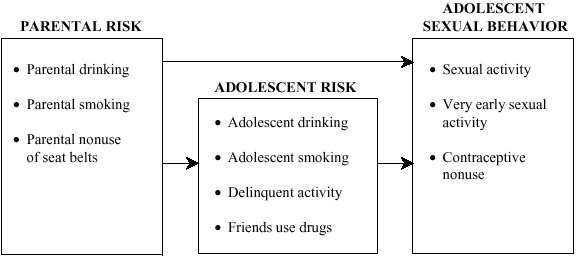
Expected influence of parental risk on adolescent sexual behavior.
Data and Methods
Data for this analysis were drawn from the National Longitudinal Study of Adolescent Health (Add Health). Add Health is a large, school-based study of the health-related behaviors of adolescents in grades 7 through 12. The project looked at a wide variety of health behaviors such as substance use, diet, physical disability, and sexual behavior. It also tried to identify the social context of such behavior and thus examined individual, family, peer, school, and community characteristics as well. The study was designed by the Carolina Population Center (University of North Carolina at Chapel Hill) and funded by 18 federal agencies, including the National Institute of Child Health and Human Development.1
Fieldwork for the Add Health survey was conducted by the National Opinion Research Center (University of Chicago) between September 1994 and August 1996. Our analysis relied on the first wave of the survey (April through December 1995), which looked at a nationally representative sample of adolescents, their parents, and their school administrators. Given our interest in the links between parental behavior and adolescent sexual activity, the Add Health data offered us a unique opportunity to use information from both the parental and the adolescent questionnaires. For example, we did not have to depend on parents’ perceptions of their children's behavior, since we had firsthand information from the children themselves (and vice versa). Female interviewers conducted most of the adolescent interviews in the respondents’ homes, and computer-aided self-interviewing was used to protect the respondents’ privacy in the more sensitive sections of the interview (including the questions on sexual behavior). For the parental questionnaire, respondents were asked to complete an interviewer-assisted questionnaire covering topics ranging from inheritable health conditions to parent-adolescent communication and interaction. The mother or female guardian was the parental respondent in 95 percent of the cases.
The Add Health Study provided information on the sexual behavior of approximately 19,000 adolescents. The survey was designed within a cluster-sampling framework in which the clusters were sampled with unequal probability. Because of this complicated sample design, we analyzed the data using STATA, a software package designed specifically for use with complex survey data. We followed the procedure recommended by Chantala and Tabor (1999), selecting the sample design characteristics from the panel data most recently collected, excluding all cases with missing weights, and applying the Add Health adolescent weights contained in the data set. These weights correct for design effects and unequal probability of selection, ensuring that our results were nationally representative.
Our sample excluded adolescents who reported that their first sexual experience occurred before age 8, as previous research has shown that a sizable proportion of very early sexual experiences—especially among females—are actually instances of sexual abuse (Abma 1999;Abma, Driscoll, and Moore 1998;Hofferth, Kahn, and Baldwin 1987). We also excluded from the analysis those immigrant adolescents whose first intercourse occurred outside the United States (n= 44), since their experience may have occurred in a very different cultural context.
In accordance with our theoretical model (figure 1), we first examined the influence of risky parental behaviors on risky adolescent behaviors (tables 3 and 4). We then investigated the impact of risky parental behaviors, risky adolescent behaviors, and other covariates on each of three adolescent sexual behaviors: sexual activity (table 5), very early sexual activity (table 6), and contraceptive use at first sex (table 7).
TABLE 3.
Parameter Estimates Predicting Risky Adolescent Behavior among Females
| Model 1: Friends Use Substances vs. Don't | Model 2: Teen Smokes vs. Doesn't | Model 3: Teen Drinks vs. Doesn't | Model 4: Teen Is Delinquent vs. Isn't Delinquent | |||||
|---|---|---|---|---|---|---|---|---|
| Variable | Odds Ratio | t | Odds Ratio | t | Odds Ratio | t | Odds Ratio | t |
| Parent smokes | 1.48 | 4.37*** | 1.52 | 4.47*** | 1.29 | 1.96** | 1.20 | 2.27* |
| Parent drank heavily past month | 1.45 | 4.23*** | 1.53 | 3.78*** | 1.52 | 2.80 | 1.12 | .87 |
| No/Irregular seat belt use | 1.39 | 3.20** | 1.17 | 1.79 | .91 | −.73 | 1.12 | 1.49 |
| Paternal supervision | .98 | −1.02 | .95 | −2.80** | .96 | −2.04* | .96 | −3.31*** |
| Maternal supervision | .95 | −3.72*** | .93 | −4.42*** | .93 | −3.81*** | .92 | −6.22*** |
| $14,999 or below | 1.33 | 1.67 | 1.18 | .78 | 1.02 | .06 | 1.10 | .44 |
| $15,000 to $29,999 | 1.35 | 2.11* | .98 | −.12 | .74 | −1.25 | 1.11 | .70 |
| $50,000 to $79,999 | 1.23 | 1.38 | 1.13 | .71 | .67 | −1.85 | 1.13 | .75 |
| $80,000 or above | 1.22 | 1.69 | 1.25 | 1.28 | .67 | −2.15* | 1.13 | .90 |
| Missing income | 1.01 | .05 | 1.10 | .50 | .79 | −.97 | .93 | −.35 |
| Welfare receipt | 1.29 | 2.35* | 1.09 | .59 | 1.05 | .25 | 1.09 | .82 |
| Less than high school | 1.43 | 2.67** | 1.34 | 1.72 | .93 | −.32 | .99 | −.06 |
| High-school graduate | 1.28 | 2.71** | 1.07 | .52 | 1.12 | .83 | .95 | −.53 |
| Some college/technical | 1.12 | .91 | 1.05 | .37 | 1.09 | .53 | 1.00 | −.02 |
| Graduate school | 1.05 | .38 | .79 | −1.38 | .93 | −.42 | 1.05 | .37 |
| Black | .51 | −6.10*** | .14 | −11.50*** | .52 | −3.16** | .99 | −.10 |
| Latina | .64 | −2.97** | .42 | −4.53*** | .75 | −1.46 | 1.57 | 2.67** |
| Asian | .75 | −1.00 | .51 | −3.10** | .78 | −.79 | 2.07 | 3.28*** |
| Other race | 1.32 | 1.66 | .80 | −1.06 | .83 | −.67 | 1.27 | 1.63 |
| Catholic | .73 | −2.76** | .75 | −2.20* | 1.13 | .67 | .90 | −.90 |
| Protestant | .89 | −1.06 | .88 | −.87 | .85 | −1.21 | .82 | −1.72 |
| Other religion | .82 | −1.75 | .85 | −1.06 | .74 | −1.51 | .88 | −.93 |
| Religion fairly important | .75 | −2.40* | .81 | −1.64 | .63 | −3.31*** | .84 | −1.62 |
| Religion very important | .48 | −6.21*** | .46 | −5.92*** | .41 | −5.90*** | .47 | −6.10*** |
| Stepfamily | 1.20 | 1.54 | 1.49 | 3.17** | 1.39 | 2.40* | 1.12 | .89 |
| Single parent | 1.15 | .84 | 1.10 | .75 | .91 | −.47 | .81 | −1.54 |
| Other family | 1.69 | 2.72** | 1.81 | 2.61** | 1.24 | .75 | 1.26 | 1.12 |
| Suburban | 1.10 | 1.04 | 1.22 | 1.98* | .99 | −.10 | 1.28 | 2.34* |
| Urban | 1.06 | .59 | 1.23 | 2.02* | 1.00 | .03 | 1.16 | 1.20 |
| Current age of respondent | 1.25 | 9.24*** | 1.31 | 10.26*** | 1.32 | 7.78*** | .90 | −4.58*** |
| F | 14.57 | 13.67 | 8.12 | 8.43 | ||||
n= 7555;
p ≥ .001;
p ≥ .01;
p ≥ .05.
TABLE 4.
Parameter Estimates Predicting Risky Adolescent Behaviour among Males
| Model 1: Friends Use Substances vs. Don't | Model 2: Teen Smokes vs. Doesn't | Model 3: Teen Drinks vs. Doesn't | Model 4: Teen Is Delinquent vs. Isn't Delinquent | |||||
|---|---|---|---|---|---|---|---|---|
| Variable | Odds Ratio | t | Odds Ratio | t | Odds Ratio | t | Odds Ratio | t |
| Parent smokes | 1.58 | 5.86*** | 1.44 | 3.69*** | 1.33 | 2.79** | 1.04 | .41 |
| Parent drank heavily past month | 1.19 | 1.61 | 1.03 | .25 | 1.33 | 2.21* | .95 | −.52 |
| No/Irregular seat belt use | 1.23 | 2.36* | 1.14 | 1.20 | 1.19 | 1.46 | 1.07 | .75 |
| Paternal supervision | 1.00 | −.28 | 1.00 | −.07 | .99 | −0.49 | .97 | −2.14* |
| Maternal supervision | .97 | −2.39* | .97 | −2.37* | .95 | −3.29*** | .96 | −3.77*** |
| $14,999 or below | 1.00 | −.03 | 1.11 | .49 | .81 | −.82 | .59 | −3.12** |
| $15,000 to $29,999 | 1.05 | .32 | 1.16 | .73 | .86 | −.74 | .78 | −1.77 |
| $50,000 to $79,999 | 1.05 | .33 | 1.14 | .71 | 1.06 | .32 | .81 | −1.64 |
| $80,000 or above | 1.00 | −.02 | 1.17 | .83 | 1.12 | .58 | .85 | −1.27 |
| Missing income | 1.05 | .24 | 1.39 | 1.36 | .99 | −.02 | .62 | −2.85** |
| Welfare receipt | 1.16 | 1.15 | .91 | −.68 | 1.13 | .82 | 1.18 | 1.48 |
| Less than high school | 1.24 | 1.58 | 1.07 | .37 | 1.14 | .68 | .86 | −.99 |
| High-school graduate | 1.21 | .22 | 1.10 | .83 | .96 | −.33 | .90 | −1.28 |
| Some college/technical | 1.03 | .15 | .86 | −1.00 | .92 | −.58 | 1.08 | .82 |
| Graduate school | .99 | −.08 | .82 | −1.30 | .98 | −.15 | 1.00 | .04 |
| Black | .66 | −3.34*** | .30 | −7.73*** | .73 | −1.80 | .80 | −2.31* |
| Latino | 1.00 | −.02 | .64 | −2.65** | .89 | −.74 | 1.03 | .23 |
| Asian | .86 | −.74 | .52 | −2.27* | .76 | −.96 | 1.02 | .09 |
| Other race | 1.20 | .99 | 1.38 | 1.68 | 1.47 | 1.67 | 1.91 | 3.33*** |
| Catholic | .89 | −1.05 | .87 | −1.19 | 1.02 | .11 | 1.16 | 1.46 |
| Protestant | .95 | −.46 | 1.18 | 1.45 | .94 | −.50 | .89 | −1.08 |
| Other religion | .85 | −1.24 | .90 | −.69 | .75 | −1.86 | .87 | −1.19 |
| Religion fairly important | .82 | −1.66 | .81 | −1.72 | .72 | −2.63** | .88 | −1.23 |
| Religion very important | .57 | −4.76*** | .60 | −3.94*** | .47 | −5.40*** | .56 | −4.83*** |
| Stepfamily | 1.36 | 2.63* | 1.33 | 2.22* | 1.24 | 1.61 | 1.17 | 1.49 |
| Single parent | 1.50 | 2.81** | 1.74 | 3.82*** | 1.51 | 2.63** | 1.32 | 2.30* |
| Other family | 1.53 | 1.82 | 1.56 | 2.06* | 1.73 | 2.26* | 1.25 | 1.09 |
| Suburban | .87 | −1.24 | 1.00 | .02 | .84 | −1.18 | 1.17 | 1.80 |
| Urban | .95 | −.50 | 1.08 | .61 | .80 | −1.42 | 1.18 | 1.77 |
| Current age of respondent | 1.36 | 13.71*** | 1.36 | 10.09*** | 1.48 | 13.76*** | 1.02 | .98 |
| F | 15.78 | 11.87 | 15.04 | 5.27 | ||||
n = 7275;
p ≥ .001;
p ≥ .01;
p ≥ .05.
TABLE 5.
Parameter Estimates of the Odds of Having Experienced Intercourse
| Females | Males | |||||||
|---|---|---|---|---|---|---|---|---|
| Model 1: Ever Had Sex vs. No Sex | Model 2: Ever Had Sex vs. No Sex | Model 3: Ever Had Sex vs. No Sex | Model 4: Ever Had Sex vs. No Sex | |||||
| Variable | Odds Ratio | t | Odds Ratio | t | Odds Ratio | t | Odds Ratio | t |
| Parent smokes | 1.69 | 6.60*** | 1.51 | 4.67*** | 1.52 | 4.84*** | 1.35 | 3.23** |
| Parent drank heavily past month | 1.18 | 1.36 | 1.00 | −.04 | 1.09 | .73 | 1.02 | .13 |
| No/Irregular seat belt use | 1.08 | .76 | 1.00 | −.02 | 1.37 | 3.29*** | 1.31 | 2.59* |
| Paternal supervision | .97 | −1.86 | .98 | −.90 | .96 | −2.28* | .96 | −2.21* |
| Maternal supervision | .93 | −4.72*** | .96 | −2.61** | .98 | −1.24 | 1.00 | .02 |
| $14,999 or below | 1.08 | .40 | .98 | −.07 | .95 | −.23 | .96 | −.21 |
| $15,000 to $29,999 | 1.17 | .83 | 1.16 | .66 | 1.16 | .84 | 1.15 | .80 |
| $50,000 to $79,999 | 1.28 | 1.57 | 1.25 | 1.32 | .92 | −.55 | .87 | −.86 |
| $80,000 or above | 1.26 | 1.64 | 1.22 | 1.13 | .91 | −.74 | .85 | −1.08 |
| Missing income | 1.06 | .30 | 1.04 | .19 | .89 | −.63 | .78 | −1.38 |
| Welfare receipt | 1.26 | 1.93 | 1.21 | 1.58 | .95 | −.39 | .91 | −.63 |
| Less than high school | 1.34 | 1.94 | 1.26 | 1.54 | 1.48 | 2.45* | 1.46 | 2.46* |
| High-school graduate | 1.45 | 2.48* | 1.46 | 2.50* | 1.37 | 3.53*** | 1.39 | 3.63*** |
| Some college/technical | 1.10 | .69 | 1.09 | .64 | 1.22 | 1.65 | 1.27 | 1.88 |
| Graduate school | .68 | −2.68** | .67 | −2.71** | .91 | −.69 | .93 | −.48 |
| Black | 1.75 | 5.05*** | 2.92 | 8.59*** | 3.50 | 10.62*** | 5.07 | 13.04*** |
| Latina/Latino | .86 | −.89 | 1.13 | .78 | 1.40 | 2.33* | 1.62 | 2.98** |
| Asian | .60 | −1.86 | .68 | −1.38 | .63 | −1.78 | .71 | −1.46 |
| Other race | .75 | .19 | 1.10 | .41 | 2.04 | 4.04*** | 1.98 | 3.38*** |
| Catholic | .64 | −3.55*** | .66 | −3.54*** | .83 | −1.73 | .82 | −1.85 |
| Protestant | .85 | −1.47 | .89 | −.99 | 1.06 | .51 | 1.05 | .46 |
| Other religion | .75 | −1.92 | .80 | −1.36 | .88 | −.85 | .96 | −.29 |
| Religion fairly important | .87 | −1.23 | 1.02 | .13 | .77 | −2.49* | .85 | −1.24 |
| Religion very important | .46 | −6.46*** | .64 | −3.27*** | .48 | −6.29*** | .60 | −3.71*** |
| Stepfamily | 1.73 | 5.25*** | 1.61 | 4.30*** | 1.44 | 2.91** | 1.34 | 2.34* |
| Single parent | 1.17 | 1.13 | 1.17 | 1.06 | 1.23 | 1.48 | 1.01 | .10 |
| Other family | 1.53 | 1.98* | 1.29 | 1.20 | 2.21 | 4.09*** | 1.83 | 3.11** |
| Suburban | 1.02 | .24 | .96 | −.40 | .77 | −2.44* | .78 | −2.23* |
| Urban | 1.17 | 1.38 | 1.11 | .88 | .89 | −1.17 | .91 | −.97 |
| Current age of respondent | 1.88 | 19.51*** | 1.87 | 18.40*** | 1.79 | 23.22*** | 1.65 | 18.88*** |
| Friends use substances | 1.96 | 6.35*** | 2.12 | 7.33*** | ||||
| Adolescent smokes | 3.56 | 9.45*** | 2.43 | 8.15*** | ||||
| Adolescent drinks | 2.04 | 5.11*** | 2.80 | 6.66*** | ||||
| Adolescent is delinquent | 1.58 | 5.11*** | 1.09 | .98 | ||||
| F | 18.02 | 28.67 | 32.91 | 37.19 | ||||
| n | 7,496 | 7,496 | 7,214 | 7,214 | ||||
p ≥ .001;
p ≥ .01;
p ≥ .05.
TABLE 6.
Parameter Estimates of the Odds of Having Experienced Very Early Intercourse (before Age 15)
| Females | Males | |||||||
|---|---|---|---|---|---|---|---|---|
| Model 1: Had Early Sex vs. No Early Sex | Model 2: Had Early Sex vs. No Early Sex | Model 3: Had Early Sex vs. No Early Sex | Model 4: Had Early Sex vs. No Early Sex | |||||
| Variable | Odds Ratio | t | Odds Ratio | t | Odds Ratio | t | Odds Ratio | t |
| Parent smokes | 1.57 | 4.02*** | 1.42 | 2.95** | 1.67 | 3.97*** | 1.49 | 3.01** |
| Parent drank heavily past month | 1.20 | 1.16 | .98 | −.13 | 1.12 | .78 | 1.09 | .52 |
| No/Irregular seat belt use | 1.15 | 1.00 | 1.13 | .82 | 1.07 | .57 | 1.03 | .21 |
| Paternal supervision | .97 | −1.68 | .98 | −.82 | .99 | −.85 | .99 | −.90 |
| Maternal supervision | .93 | −4.40*** | .94 | −3.49*** | .98 | −1.34 | .99 | −.63 |
| $14,999 or below | .86 | −.52 | .82 | −.62 | 1.59 | 1.82 | 1.72 | 2.07* |
| $15,000 to $29,999 | .91 | −.35 | .89 | −.39 | 2.10 | 3.29*** | 2.18 | 3.22** |
| $50,000 to $79,999 | .92 | −.33 | .87 | −.50 | 1.40 | 1.35 | 1.38 | 1.25 |
| $80,000 or above | .87 | −.53 | .82 | −.73 | 1.13 | .55 | 1.12 | .48 |
| Missing income | .59 | −1.95 | .56 | −2.08* | 1.49 | 1.56 | 1.43 | 1.43 |
| Welfare receipt | 1.04 | .25 | 1.00 | −.01 | .88 | −.79 | .83 | −1.09 |
| Less than high school | 1.25 | 1.18 | 1.15 | .76 | 1.11 | .60 | 1.08 | .43 |
| High-school graduate | 1.28 | 1.39 | 1.28 | 1.39 | 1.10 | .69 | 1.07 | .46 |
| Some college/technical | .88 | −.59 | .91 | −.46 | 1.09 | .45 | 1.12 | .62 |
| Graduate school | .79 | −1.11 | .80 | −1.04 | .66 | −1.84 | .68 | −1.73 |
| Black | 1.53 | 2.70** | 2.62 | 5.49*** | 3.41 | 8.17*** | 4.89 | 9.81*** |
| Latina/Latino | .81 | −.89 | 1.10 | .42 | 1.39 | 1.64 | 1.55 | 2.07* |
| Asian | .60 | −1.37 | .72 | −.82 | .93 | −.19 | 1.16 | .46 |
| Other race | 1.24 | .80 | 1.50 | 1.38 | 2.36 | 3.48*** | 2.38 | 3.09** |
| Catholic | .66 | −2.45* | .65 | −2.65** | .81 | −1.41 | .79 | −1.53 |
| Protestant | .68 | −2.57* | .69 | −2.47* | .74 | −2.04* | .71 | −2.18* |
| Other religion | .80 | −1.15 | .83 | −.95 | .67 | −2.14* | .71 | −1.74 |
| Religion fairly important | .81 | −1.13 | .90 | −.51 | .83 | −1.11 | .93 | −.46 |
| Religion very important | .57 | −2.75** | .73 | −1.47 | .48 | −4.10*** | .60 | −2.78** |
| Stepfamily | 1.35 | 1.70 | 1.25 | 1.19 | 1.69 | 2.90** | 1.57 | 2.43* |
| Single parent | 1.40 | 1.90 | 1.45 | 1.95 | 1.40 | 2.12* | 1.19 | 1.04 |
| Other family | 1.84 | 2.34* | 1.67 | 1.97 | 2.33 | 4.24*** | 2.15 | 3.99*** |
| Suburban | .98 | −.11 | .92 | −.53 | .80 | −1.79 | .82 | −1.54 |
| Urban | 1.16 | 1.00 | 1.10 | .66 | .81 | −1.45 | .84 | −1.12 |
| Current age of respondent | .79 | −4.87*** | .74 | −6.02*** | 1.05 | .96 | .96 | −.83 |
| Friends use substances | 1.56 | 3.40*** | 1.81 | 5.33*** | ||||
| Adolescent smokes | 2.95 | 8.08*** | 1.90 | 4.60*** | ||||
| Adolescent drinks | 1.80 | 3.51*** | 2.03 | 4.78*** | ||||
| Adolescent is delinquent | 1.14 | 1.24 | 1.13 | 1.06 | ||||
| F | 6.78 | 14.93 | 9.57 | 13.14 | ||||
| n | 5,274 | 5,274 | 5,350 | 5,350 | ||||
Note: Sample was restricted to respondents aged 15 and over. Early sex refers to sex prior to the respondent's 15th birthday.
p ≥ .001;
p ≥ .01;
p ≥ .05.
TABLE 7.
Parameter Estimates of the Odds of Having Used Contraception at First Coitus
| Females | Males | |||||||
|---|---|---|---|---|---|---|---|---|
| Model 1: Used Contra. vs. No Contra. | Model 2: Used Contra. vs. No Contra. | Model 3: Used Contra. vs. No Contra. | Model 4: Used Contra. vs. No Contra. | |||||
| Variable | Odds Ratio | t | Odds Ratio | t | Odds Ratio | t | Odds Ratio | t |
| Parent smokes | .97 | −.23 | .99 | −.08 | 1.35 | 2.00* | 1.34 | 1.99* |
| Parent drank heavily past month | .87 | −.85 | .91 | −.58 | .92 | −.47 | .92 | −.48 |
| No/Irregular seat belt use | .98 | −.14 | .98 | −.18 | .99 | −.09 | 1.01 | .06 |
| Paternal supervision | 1.01 | .57 | 1.01 | .53 | .98 | −.90 | .99 | −.85 |
| Maternal supervision | 1.00 | −.17 | .99 | −.41 | 1.02 | .86 | 1.01 | .60 |
| $14,999 or below | .92 | −.30 | .92 | −.29 | .72 | −1.13 | .68 | −1.30 |
| $15,000 to $29,999 | 1.08 | .29 | 1.06 | .24 | .88 | −.48 | .86 | −.57 |
| $50,000 to $79,999 | .97 | −.13 | .94 | −.23 | 1.01 | .04 | 1.00 | −.01 |
| $80,000 or above | 1.31 | 1.10 | 1.31 | 1.07 | .82 | −.82 | .81 | −.87 |
| Missing income | .99 | −.05 | 1.00 | −.00 | 1.05 | .15 | .99 | −.03 |
| Welfare receipt | .85 | −.75 | .86 | −.73 | .91 | −.50 | .94 | −.31 |
| Less than high school | .55 | −2.84** | .55 | −2.83** | .83 | −.87 | .80 | −.97 |
| High-school graduate | .80 | −1.51 | .80 | −1.49 | .89 | −.63 | .88 | −.71 |
| Some college/technical | .76 | −1.31 | .76 | −1.29 | .93 | −.32 | .95 | −.27 |
| Graduate school | .98 | −.07 | 1.00 | .01 | 1.13 | .46 | 1.16 | .52 |
| Black | 1.22 | 1.09 | 1.10 | .54 | 1.07 | .49 | 1.05 | .32 |
| Latina/Latino | .83 | −.95 | .81 | −1.14 | .93 | −.47* | .90 | −.65 |
| Asian | .64 | −1.16 | .62 | −1.20 | .53 | −2.36 | .53 | −2.32* |
| Other race | 1.31 | .94 | 1.31 | .96 | 1.17 | .56 | 1.20 | .62 |
| Catholic | .88 | −.66 | .87 | −.67 | 1.26 | 1.41 | 1.31 | 1.69 |
| Protestant | .71 | −1.59 | .70 | −1.68 | 1.36 | 1.79 | 1.37 | 1.83 |
| Other religion | .64 | −1.37 | .63 | −1.42 | 1.38 | 1.90 | 1.38 | 1.83 |
| Religion fairly important | 1.08 | .39 | 1.04 | .21 | 1.16 | 1.07 | 1.12 | .81 |
| Religion very important | .92 | −.34 | .87 | −.60 | 1.23 | 1.38 | 1.18 | 1.04 |
| Stepfamily | .85 | −.94 | .86 | −.86 | 1.14 | .68 | 1.17 | .82 |
| Single parent | 1.30 | 1.30 | 1.30 | 1.30 | .80 | −1.10 | .84 | −.88 |
| Other family | .90 | −.40 | .90 | −.39 | .87 | −.58 | .88 | −.53 |
| Suburban | 1.02 | .11 | 1.04 | .25 | 1.05 | .39 | 1.07 | .59 |
| Urban | .85 | −1.07 | .86 | −1.04 | .96 | −.31 | .98 | −.17 |
| Age 14–16 at first sex | 1.48 | 2.47* | 1.43 | 2.28* | 1.20 | 1.14 | 1.22 | 1.30 |
| Age 17–21 at first sex | 1.84 | 2.88** | 1.74 | 2.65** | 1.43 | 1.62 | 1.39 | 1.48 |
| Had first sex 1991–3 | 1.66 | 1.96 | 1.67 | 1.88 | 1.80 | 3.04** | 1.77 | 3.03** |
| Had first sex 1994 or later | 1.95 | 2.35* | 1.96 | 2.24* | 1.51 | 2.14* | 1.48 | 2.05* |
| Friends use substances | .87 | −1.02 | .95 | −.40 | ||||
| Adolescent smokes | .93 | −.50 | 1.18 | 1.15 | ||||
| Adolescent drinks | .77 | −2.01* | .85 | −1.16 | ||||
| Adolescent is delinquent | .87 | −.97 | .67 | −3.31*** | ||||
| F | 2.29 | 2.57 | 2.15 | 2.20 | ||||
| n | 2,557 | 2,557 | 2,573 | 2,573 | ||||
Note: Sample was restricted to respondents who reported prior sex.
p ≥ .001;
p ≥ .01;
p ≥ .05.
Tables 5 through 7 present four binary logit models for each of the three dependent variables, that is, each of the three adolescent sexual behaviors. Specifically, each table includes two logit models for males and two for females, since sexual behaviors and social influences are likely to vary by gender. Within each pair of models, the first regression shows the impact of risky parental behaviors plus a variety of socioeconomic covariates. The second regression of each pair introduces additional covariates representing risky adolescent behaviors. Together, these models helped us determine (1) the extent to which risky parental behaviors have an independent affect on adolescent sexual behaviors and (2) the extent to which risky parental behaviors influence adolescent sexual practices by encouraging (or discouraging) risky adolescent behaviors.
Dependent Variables and Descriptive Data
Table 1 shows the variables we used in our multivariate analyses. We began by exploring the extent to which risky parental behaviors influenced risky adolescent behaviors: substance use, smoking, drinking, and delinquent activity. We subsequently included these measures of adolescent risk as independent variables in our models predicting adolescent sexual activity and contraceptive use.
TABLE 1.
Dependent Variables Used in Analysis (Sample sizes are in parentheses)
| Percentage with Stated Characteristic | ||
|---|---|---|
| Variable | Females | Males |
| Respondent's friend(s) use substancesa | (9,601) | (9,165) |
| 31% | 32% | |
| Respondent smokesa | (9,601) | (9,165) |
| 22% | 21% | |
| Respondent drinksa | (9,601) | (9,165) |
| 11%*** | 17% | |
| Respondent engages in delinquent activitya | (9,601) | (9,165) |
| 25%*** | 39% | |
| Respondent ever had sex | (9,495) | (9,056) |
| 37%** | 39% | |
| Respondent had sex before 15th birthdayb | (6,940) | (6,901) |
| 17%** | 20% | |
| Respondent used contraception at first sexc | (3,956) | (3,700) |
| 64% | 65% | |
Used as an independent variable in models predicting sexual activity among adolescents.
Sample restricted to respondents at least 15 years old.
Sample restricted to respondents who reported prior sexual activity.
Note: One-tailed t-tests were conducted to identify significant sex-related differences in risky adolescent behavior (including peer associations), previous sexual experience, and the use of contraception at first intercourse. The significance of these differences is shown in the Females column.
p ≥ .001;
p ≥ .01;
p ≥ .05.
While all tobacco and alcohol use may be considered risky behavior, we have tried to identify those adolescents who exhibited a more generalized pattern of unsafe behavior extending beyond one or two isolated episodes. (Although a large proportion of adolescents experiment with substances, we were more interested in identifying habitual users.) Adolescent smokers are those who answered yes to the question, “Have you ever smoked cigarettes regularly, that is, at least one cigarette every day for 30 days?” Adolescent drinkers are those who either (1) drank five or more drinks in a row for at least two or three days a month in the past 12 months or (2) got drunk or “very, very high” on alcohol more than three times in the past 12 months. Finally, adolescents with substance-using friends are those for whom two of their three best friends habitually smoke (at least one cigarette each day) and/or use marijuana (at least once a month).
Our measure of delinquency assessed whether adolescents had recently engaged in criminal activity. Specifically, adolescents were characterized as delinquent if they responded yes (once or more) to any of the following five questions: (1) In the past 12 months, how often did you deliberately damage property that didn't belong to you? (2) In the past 12 months, how often did you steal something worth more than $50? (3) How often did you steal something worth less than $50? (4) How often did you use or threaten to use a weapon to get something from someone? and (5) How often did you sell marijuana or other drugs? Although these questions suggest different dimensions of criminal activity, other researchers have combined similar indicators to measure antisocial behavior (see, e.g., Ary et al. 1999).
We employed several measures of adolescent sexual behavior and contraceptive use (see table 1), including (1) whether respondents had had sex and (2) whether they first had sex before age 15. An increasing proportion of adolescents are having sex at an early age (Terry and Manlove 2000), and girls introduced to sex early in life are especially likely to report multiple sex partners as well as sexual relations with bisexual, intravenous drug–using, and HIV-infected men (Greenberg, Magder, and Aral 1992). For those adolescents with previous sexual experience (all ages), we also looked at contraceptive use (did or did not use contraception) and at contraceptive method choice at first intercourse.
Table 1 also shows the results of t-tests comparing males and females on each of the dependent variables. While boys and girls were almost equally likely to smoke and/or associate with substance-using friends, boys were significantly more likely than girls to be heavy drinkers and to engage in delinquent behaviors. With regard to sexual behaviors, boys were significantly more likely than girls to report prior sex and to have had sex before age 15. This finding is consistent with previous research showing earlier sexual activity among males (e.g., Elliott and Morse 1989;Holmbeck et al. 1994;McGuire et al. 1992;Miller et al. 1997;Needle 1975;Poppen 1994;St. Lawrence and Scott 1996;Zelnik and Shah 1983).
Among those adolescents who reported having had sex, almost two-thirds used contraception at first intercourse (table 1). This figure is slightly lower than the percentage reported in the 1995 National Survey of Family Growth (Terry and Manlove 2000), although it does indicate that the rate of contraceptive use has risen substantially since the 1970s and 1980s (see appendix 1 for a review of previous research). Our data further revealed that the condom was the most popular birth control method. Among those adolescents who used contraception at first sex, nearly all (94.7%) used condoms. This rate is high but consistent with recent research showing high rates of condom use among young, sexually active males (Murphy and Boggess 1998).
While recent cohorts of adolescents may feel more comfortable obtaining prophylactics and broaching the subject of contraceptive use with their partners, the fact that one-third of adolescents used no contraception at first intercourse is cause for concern. Our data are congruent with those of Abma and Sonenstein (2001), who reported that 30 percent of sexually active girls and 18 percent of sexually active boys did not use contraception the last time they had intercourse. Among females, the proportion using no contraceptive method at last intercourse rose significantly between 1988 and 1995, from 20 to 29 percent.
Independent Variables
The independent variables are presented in table 2. Our indicators of risky parental behavior were parental smoking, drinking, and seat belt nonuse. We obtained these data solely from the parents’ questionnaire, which represents the behavior of the responding parent only (usually the mother). The parents’ survey asked the respondents whether they smoked, and an affirmative response led to a code of 1 (yes) for the parental smoking variable. Drinkers are those who gave responses of once or more to the question, “How often in the last month have you had five or more drinks on one occasion?” Seat belt nonusers are those who wear seat belts only sporadically—those who answered never, rarely, or sometimes to a question on seat belt use. While we experimented with combining our three measures of parental risk into a single scale, there was too little internal consistency to justify merging the variables (Cronbach's alpha = 0.25 for females and 0.22 for males).
TABLE 2.
Independent Variables Used in Analysis (Sample sizes are in parentheses)
| Females | Males | ||||
|---|---|---|---|---|---|
| Variable | Values | Mean or Proportiona | Std Dev.b | Mean or Proportiona | Std. Dev.b |
| Parent smokes | (8,089) | (7,818) | |||
| 0 = noc, 1 = yes | 31% | 31% | |||
| Parent drank heavily in the past month | (8,065) | (7,786) | |||
| 0 = noc, 1 = yes | 13% | 14% | |||
| Parent seatbelt use | (8,098) | (7,823) | |||
| 0 = most of the time/alwaysc | 19% | 20% | |||
| 1 = never or irregularly | |||||
| Paternal supervision | (9,571) | (9,133) | |||
| Scale: 0 to 12 | 4.9 | 3.9 | 5.3 | 3.9 | |
| Maternal supervision | (9,561) | (9,143) | |||
| Scale: 0 to 12 | 8.7 | 3.1 | 8.6 | 3.2 | |
| 1994 family income | (9,601) | (9,165) | |||
| Below $15,000 | 12.2% | 11.7% | |||
| $15,000 to $29,999 | 15.9% | 15.2% | |||
| $30,000 to $49,999c | 19.9% | 21.6% | |||
| $50,000 to $79,999 | 19.2% | 19.9% | |||
| $80,000 and above | 9.1% | 8.6% | |||
| Missing incomed | 23.8% | 23.0% | |||
| Parent receives welfare | (9,601) | (9,165) | |||
| 0 = noc, 1 = yes | 13% | 13% | |||
| Parental education | (9,020) | (8,613) | |||
| Less than high school | 13.2% | 12.0% | |||
| High-school graduate | 40.0% | 39.5% | |||
| Some college/technical | 14.2% | 13.8% | |||
| College graduatec | 21.7% | 23.5% | |||
| Graduate school | 10.9% | 11.2% | |||
| Race/ethnicity of respondent | (9,590) | (9,160) | |||
| Whitec | 65.0% | 65.3% | |||
| Black | 15.6% | 15.0% | |||
| Latino/a | 12.0% | 12.1% | |||
| Asian | 3.8% | 3.8% | |||
| Other | 3.5% | 3.8% | |||
| Religion of respondent | (9,601) | (9,165) | |||
| Fundamentalistc,e | 30.7% | 27.3% | |||
| Catholic | 26.6% | 26.8% | |||
| Protestant | 24.3% | 24.1% | |||
| Other | 18.4% | 21.8% | |||
| Importance of religion | (9,581) | (9,151) | |||
| Not important/fairly unimportantc | 22.0% | 26.9% | |||
| Fairly important | 34.5% | 37.0% | |||
| Very important | 43.5% | 36.1% | |||
| Family structure | (9,601) | (9,165) | |||
| Two biological parentsc | 53.5% | 54.9% | |||
| Stepfamily | 10.2% | 11.1% | |||
| Single parent | 29.6% | 27.9% | |||
| Other | 6.6% | 6.1% | |||
| [-.5pt] Residence | (9,493) | (9,023) | |||
| Ruralc | 27.6% | 28.3% | |||
| Suburban | 37.8% | 38.5% | |||
| Urban | 34.6% | 33.2% | |||
| Current age of respondent | (9,595) | (9,159) | |||
| Current age, in years | 15.4 | 1.8 | 15.6 | 1.9 | |
| Age at first intercourse | (3,423) | (3,343) | |||
| 8 to 13c | 22.1% | 35.8% | |||
| 14 to 16 | 64.5% | 49.0% | |||
| 17 to 21 | 13.3% | 15.3% | |||
| Year of first intercourse | (3,485) | (3,437) | |||
| 1990 or earlierc | 6.0% | 18.6% | |||
| 1991 to 1993 | 42.4% | 35.3% | |||
| 1994 to 1995 | 51.6% | 46.1% | |||
For variables coded 0 = no/1 = yes, the mean value is equal to the proportion responding yes
For continuous variables only.
Reference category in multivariate models.
Families with missing income values were no more or less likely to be receiving welfare benefits than those who provided income information. Parental education levels were somewhat lower among those respondents with missing income values.
The following denominations were considered fundamentalist: Adventist, AME, AME Zion, CME, Assembly of God, Christian Church (Disciples of Christ), Christian Science, Holiness, Jehovah's Witness, Latter Day Saints (Mormon), Pentecostal, and United Church of Christ. Respondents who self-identified as Baptist and agreed that “the Scriptures are the word of God” were also included in this category.
Our measure of parental supervision indicates the likelihood that each resident parent was at home when the respondent (1) left for school, (2) returned home from school, and (3) went to bed. Each adolescent respondent was asked to indicate whether his or her father and mother were present never, rarely, some of the time, most of the time, or always at each of these three times during the day. The results of the six questions (three for each resident parent) were summed (never= 0; rarely= 1; some= 2; most= 3; always= 4) to create two separate scales measuring paternal and maternal supervision. If only one parent resided in the household, we assigned the nonresident parent an overall score of zero. While the alphas for the maternal scales were somewhat lower than anticipated (0.62 for females and 0.64 for males), the alphas for the paternal supervision scales were quite satisfactory (0.75 for females and 0.73 for males).
Following the lead of Kahn, Rindfuss, and Guilkey (1990), we identified four types of religious denominations: fundamentalist, Protestant, Catholic, and other. Race was coded according to each respondent's self-reported identity. If a respondent listed more than one race, he or she was asked to indicate the category that best described his or her racial identity. The parental education variable gives the highest level of education attained by the adolescent's parents, that is, the educational level of the parent with the most education. We obtained our information on welfare receipt from the adolescent questionnaire, which measured whether either resident parent was receiving welfare benefits at the time of the survey. Information on family income was derived from the parental questionnaire. Because of the large number of missing cases (>20%), we included a dummy category for missing income values. We also ran our models using income as a continuous variable and obtained results very similar to those presented here. (The results for the models using income as a continuous variable are available from the authors.) Residence (urban, suburban, or rural) was assessed by the interviewer at the time of the interview.
We also included a variable indicating the year of first intercourse in the models predicting contraceptive use, since previous reports suggested that contraceptive use may have increased significantly over the years covered by our study. For example, Murphy and Boggess (1998) reported that condom use rose by 24 percent among American males between 1988 and 1995.
Tests for multicollinearity among the independent variables revealed no significant problems.
Multivariate Results
Risky Behavior among Parents and Adolescents
The impact of risky parental behavior on adolescent sexual practices may be partly due to the fact that risky parental behavior encourages risky adolescent behavior. Tables 3 and 4 show the extent to which risky adolescent behaviors (smoking, drinking, delinquency, and substance use among friends) were influenced by risky parental behaviors (smoking, drinking, and nonuse of seat belts).
Overall, our findings revealed that unsafe parental behaviors–especially smoking—greatly increased adolescent risk. Moreover, the effects of unsafe parental behaviors extended beyond encouraging analogous behaviors among adolescents. For example, parental smoking was associated with an increased likelihood not only that adolescents smoked but also that they drank heavily, engaged in delinquent activity (females only), and associated with friends who used substances. Similarly, adolescents who associated with friends who used substances were more likely to have parents who not only drank (females only) and smoked but also did not consistently wear their seat belts. These findings imply that parents who exhibit risky behavior in various realms of social life provide a model of low self-efficacy that encourages (or fails to deter) a wide range of problem behaviors among their children.
Parental supervision is also pertinent to understanding variation in adolescent problem behavior. Most notably, high levels of maternal supervision reduced the likelihood that both male and female adolescents smoked, drank, engaged in delinquent activity, and/or associated with friends who used substances. High levels of paternal supervision discouraged delinquent activity as well as female smoking and drinking, although maternal supervision clearly had the stronger impact. Overall, our findings suggest that maternal supervision may be more important than paternal supervision in preventing problem behavior among teens.
Risky Parental Behavior and Adolescent Sexual Experience
Tables 5 and 6 present the results of our logit analyses predicting the likelihood of sexual experience (table 5) and sexual activity before age 15 (table 6). Our results support the hypothesis that risky parental behavior is central to understanding variation in the sexual behavior of adolescents. For example, adolescents whose parents smoked were significantly more likely than others to report prior sexual activity as well as a very early age at first coitus. Similarly, boys whose parents failed to wear seat belts regularly were more likely to report having had intercourse (see table 5, model 4).
It is important to note that the effects of risky parental behavior remained significant even when we controlled for smoking, drinking, delinquency, and substance use among adolescents and their peers (tables 5 and 6, models 2 and 4). This confirmed our hypothesis that the impact of risky parental behavior on adolescent sexual practices can be only partially attributed to the link between risky parental behavior and risky adolescent behavior. (It is also possible, of course, that other, unmeasured, factors might help explain the apparently independent effects of the parental risk variables. While we tried to include all theoretically relevant variables in our regressions, the models may nonetheless be subject to specification bias.)
As demonstrated earlier (tables 3 and 4), parents who exhibited unsafe behaviors were especially likely to have adolescent children who acted similarly. In turn, adolescents who engaged in risky behaviors were especially likely to have had sex (tables 5 and 6). Specifically, boys and girls who smoked, drank, or had substance-using friends were more likely than others to have had sex— and were more likely to have had sex before age 15. Delinquency was linked to prior sexual activity only among females, however. Overall, these results confirm earlier reports of a strong association between adolescent substance use and early sexual activity (Crockett et al. 1996;Elliot and Morse 1989;Mott et al. 1996;Paul et al. 2000).
As tables 5 and 6 show, parental supervision also had a substantial effect on the likelihood of early sexual experience. High levels of paternal supervision discouraged sexual activity among male adolescents, whereas high levels of maternal supervision discouraged sexual activity (including very early sex) among females. Interestingly, paternal supervision had no effect on girls’ likelihood of intercourse, and maternal supervision had no effect on boys’.
Risky Parental Behavior and Contraceptive Use at First Coitus
While risky parental behaviors had a major impact on the likelihood of adolescent sex, these same behaviors had only a negligible effect on contraceptive use at first intercourse. By and large, parental risk was unrelated to contraceptive use at first coitus among sexually experienced American adolescents (see table 7). There was one notable exception, however: males whose parents smoked were slightly more likely than others to have used contraception at first coitus. Although this finding was unexpected, a possible explanation is that parental smoking reflects a liberalism and openness to communication about contraception. A separate analysis (not shown) provided some support for this explanation. Specifically, the apparent relationship between parental smoking and contraceptive use failed to achieve significance when we introduced controls for parent-child discussion of topics relating to sexuality, birth control, and STDs. We did not include these discussion variables in our final models, however, because of problems of endogeneity. That is, we had no way of knowing whether parent-child discussions of sexual matters took place before or after first intercourse. It also is important to emphasize that the relationship between smoking and contraception applied only to sexually experienced adolescents. Further analysis is necessary to determine whether this relationship persists among those who postpone their sexual activity.
As we have seen, risky parental behavior affected the timing of first coitus but had virtually no impact on contraceptive use at first sex. The reasons for this are not entirely clear. It is possible, however, that risky parental behaviors encourage adolescents to make the transition to perceived adulthood, a status characterized by sexual activity but not necessarily by contraceptive use. This explanation is consistent with the work of Upchurch and associates (1998), who contend that a person's first sexual experience helps redefine his or her identity from child to developing teenager. Meanwhile, it also is important to emphasize that our models predict contraceptive use only among individuals who first had sex as adolescents. It is possible, for example, that risky parental behavior has a greater impact on contraceptive use among those adolescents who delayed sexual activity until after their teens.
Unlike risky parental behaviors, risky adolescent behaviors are important determinants of contraceptive use at first coitus. For example, girls who drink heavily are unlikely to report having used birth control at first sex. (Because heavy drinking is relatively uncommon among girls, those who drink heavily are presumably far less risk averse than their nondrinking peers.) Likewise, male adolescents who engage in delinquent activity are especially unlikely to use birth control. Since males tend to engage in more serious forms of delinquent activity than females do—males are far more likely to threaten someone with a weapon, for example—it may be that only the more serious, gender-linked forms of delinquent activity indicate a willingness to engage in risky behavior in other realms of social life.
Neither paternal nor maternal supervision had a significant influence on contraceptive use at first coitus, although age at first coitus was significantly associated with contraceptive use among girls. Specifically, females who had their first sexual experience in late adolescence were more likely to report having used contraception than were those who first had sex at earlier ages. Other studies have shown that age at first sex is associated with contraceptive use not only at first coitus but also during subsequent sexual encounters (Abma and Sonenstein 2001). Since parental risk has a strong influence on adolescent sexual activity, it may indirectly influence contraceptive use through its effect on the timing of first coitus.
Interestingly, one of the more important variables for understanding variation in contraceptive use among sexually experienced adolescents is the year in which they first had sex. Adolescents who first had sex in 1991 or later were significantly more likely than others to report having used birth control. This finding points to a greater incidence of safety-conscious sexual behavior over time. Further investigation revealed increasing use of the condom at first coitus during this time period, a finding that may be related to AIDS awareness campaigns that had become nearly universal by 1995 (Ku et al. 1998).
Risky Parental Behavior and Contraceptive Method Choice at First Coitus
In two additional models, we examined the relationships between risky parental behaviors and contraceptive method choice at first coitus. Specifically, we investigated the impact of risky parental behaviors on (1) the odds of having used a condom at first sex and (2) the odds of having used a medical method of contraception at first sex. (These two categories are not mutually exclusive, since the Add Health Survey allowed respondents to indicate multiple methods of birth control at first intercourse.) Medical methods of contraception include the pill, Depo-Provera, the diaphragm, IUD, Norplant, and the ring. Ninety-five percent of adolescents who used medical methods at first coitus chose the pill; 1 percent chose Depo-Provera; and less than 1 percent chose each of the other methods.
The distinction between condoms and other methods is important chiefly due to the condom's effectiveness in preventing the spread of sexually transmitted diseases (e.g., Aral 2001;Mahler 1996;Nguyet et al. 1994). Condoms also are more effective than either rhythm or withdrawal in preventing pregnancy in teens (Kahn, Rindfuss, and Guilkey 1990). Moreover, adolescents who use condoms at their first sexual experience tend to use them more consistently and to disengage sexual activity from substance use, a finding that has important implications for adolescent health and well-being (St. Lawrence and Scott 1996). The distinction between medical methods of contraception and others is important for at least two reasons. First, medical methods are generally more efficient. (There is a lower risk of unwanted pregnancy associated with their use.) Second, these methods require consultation with a physician before use and therefore indicate considerable foresight.
Altogether 60 percent of sexually experienced males and 61 percent of sexually experienced females used a condom at first sex. Twenty percent of males and 14 percent of females relied on medical methods. (The gender difference in the use of medical methods is statistically significant, p < 001.) Males’ higher rate of reliance on medical methods may be related to the sexual experience of the male respondents’ partners at first sex. The medical methods of contraception are controlled by the female and require considerable foresight and planning. Because the use of medical methods rises as women become more sexually experienced, men who first engage in sexual relations with more experienced women are especially likely to report that medical methods were used at first coitus. (The results reported here are consistent with those of Zelnik and Shah 1983, who found that males were more likely than females to report having used a prescription method of contraception at first sex.)
By and large, parental risk variables did not affect the choice of contraceptive method. (The table is not shown, but the binary logit results are available from the authors.) This finding is not surprising given our results for contraceptive use overall (table 7). Since 95 percent of contracepting adolescents used a condom at first sex, the results of our models predicting condom use closely paralleled our results for the use of any contraceptive method.
With regard to the medical methods of contraception, only paternal supervision emerged as significant, and only for boys. Specifically, high levels of paternal supervision were inversely associated with the use of medical methods of contraception. Since the medical methods of contraception are controlled by the female, boys whose fathers provide more supervision may have been less likely to initiate sexual activity with a female partner who used such methods.
Like parental risk, adolescent risk had very little bearing on the choice of contraceptive method at first coitus. One notable exception, however, was that boys who engaged in delinquent activity were significantly less likely to have used either a condom or a medical method of contraception. Otherwise, none of the adolescent risk variables emerged as significant predictors of contraceptive method choice at first coitus.
Conclusions
Nearly 38 percent of American boys and girls in grades 7 through 12 have had sexual intercourse. Moreover, 18 percent of those aged 15 and older first had sex before reaching age 15. Teenage sexual activity does not necessarily lead to sexually irresponsible behavior, however. The majority of sexually active adolescents (65%) used contraception at first sex, and nearly all the contraceptors (95%) used condoms. This heavy reliance on the condom gives us reason for some optimism, since condom use at first intercourse is associated with safety-conscious attitudes and relatively high rates of precautionary behavior during subsequent sexual experiences (St. Lawrence and Scott 1996). At the same time, it is important to emphasize that contraceptive failure rates are especially high among adolescents, particularly among those who are unmarried, black or Hispanic, and poor (Fu et al. 1999). Many adolescents practice contraception inconsistently (Glei 1999), and 35 percent used no form of contraception at first intercourse.
Our research has shown that parents’ risky behaviors (smoking, drinking, and seat belt nonuse) have substantial and independent effects on their children's sexual behavior. Adolescents whose parents engage in risky behavior, particularly smoking, are especially likely to be sexually active. They also are more likely to smoke, drink, associate with substance-using peers, and participate in delinquent activity. Our findings further support the notion that risk is “reproduced” across the generations, perhaps because parents often serve as role models for their children—willingly or unwillingly, consciously or unconsciously. In this respect, our study is consistent with that of Mott and associates (1996), who found that children were significantly more likely to become sexually active before age 14 if their mothers had had sex at an early age.
Although parental risk has only a negligible effect on the contraceptive practices of adolescents at first intercourse, adolescent risk (heavy drinking among females and delinquent activity among males) is inversely associated with the odds of contraceptive use. Because risky parental behaviors are closely associated with risky adolescent behaviors, parental risk appeared to influence contraceptive use through its effect on self-efficacy more generally.
A few caveats are in order concerning our findings. First, the absence of information about the timing of parental and adolescent behaviors prevented us from disentangling cause and effect for many of the relationships documented here. For example, it is possible that adolescents begin to drink (or smoke, engage in delinquent activity, etc.) only after they become sexually active. Second, our measures of parental risk did not capture the behavior of both parents, since only one parent (usually the mother) responded to the Add Health questionnaire. To the extent that fathers’ risky behavior plays a critical role in explaining variation in adolescent sexual activity, we may have overlooked important information. Finally, we were constrained by the limited nature of some of the parental risk questions asked in the Adolescent Health Survey. For example, our measure of parental drinking asked only whether the responding parent consumed five or more drinks on one occasion in the past month. Thus we had no information about past alcohol abuse or about adolescents’ perceptions that their parents drank excessively. Future studies that try to link parental and adolescent risk will need to include data on the behavior of both parents, on the timing of risky behavior, and on the sociodemographic characteristics of the respondents’ sexual partner(s). Subsequent research might also benefit from an assessment of the extent to which the impact of parental risk varies across particular demographic, cultural, and socioeconomic groups.
Parents who exhibit low levels of self-efficacy are especially likely to have children at risk of engaging in a variety of problem behaviors. Efforts to promote safe sexual practices among adolescents will therefore need to consider the role of parents as socializing influences on their children's health practices and their propensity for problem behavior. Moreover, programs promoting adolescent health and safe sex might be most successful if they encouraged all family members to engage in healthy behaviors. Given the importance of parental risk in explaining both early sexual activity and a host of problem behaviors linked to contraceptive nonuse, public health campaigns that urge parents to act responsibly by engaging in health-conscious behaviors are likely to help reduce precocious and unsafe sexual activity among teens.
Acknowledgments
We are grateful for the comments of William H. Walters and for the thoughtful feedback provided by the Milbank Quarterly's reviewers.
APPENDIX
Sexual Experience and Contraceptive Use at First Coitus in the United States
| Researcher(s) | Survey Instrument and/or Sample Population | Age at First Sex or Percentage Reporting Prior Sex | Percentage Who Used Birth Control at First Sex | Method of Birth Control Used at First Sex |
|---|---|---|---|---|
| Sorensen 1973 | A probability sample of U.S. households, 393 adolescents aged 13 to 19. | 52% of adolescents had experienced intercourse: 59% of boys and 45% of girls. | 32% of respondents reported using birth control at first sex: 37% of girls and 28% of boys. | |
| Needle 1975 | College men and women at the University of Maryland. Date of survey is unclear. | 65% of women and 75% of men reported having had sex. 51% of men and 34% of women first had sex at age 17 or younger. | Among those who had experienced intercourse, 60% of men and 61% of women used either no contraception or an unreliable method (withdrawal, rhythm, or douche) at first sex. | |
| Zelnik and Kantner 1978 | A 1976 national probability sample survey of ever-married and never-married women 15–19 years of age living in households in the continental United States. | Almost 40% of all teenage women with premarital sexual experience used contraception the first time they had sex. | One-quarter of those who used contraception at first sex used a medical method (pill, IUD, or diaphragm). | |
| Zelnik, Kantner, and Ford 1981 | Two national probability samples of women aged 15–19 in the continental United States. | Among young women aged 15–19 who had premarital intercourse, the mean age at first sex was 16.4 in 1971 and 16.1 in 1976. | About 60% of young women with premarital sexual experience were unprotected at first coitus (based on 1976 interviews). | Slightly less than one-quarter of contracepting women (24%) used a medical method at first sex. |
| Zelnik and Shah 1983 | A national probability survey, carried out in 1979, of young women aged 15–19 and young men aged 17–21 living in households in metropolitan areas in the coterminous United States. | In 1979, 50% of women aged 15–19 and 70% of men aged 17–21 reported that they had ever had sex. The average age at first sex was 16.2 for women and 15.7 for men. | 49% of women and 44% of men used contraception at first intercourse. | Male methods of contraception (condom and withdrawal) were most popular. 20% of women and 22% of men reported having used a prescription method of contraception at first sex. |
| Mosher and Bachrach 1987 | 1982 National Survey of Family Growth, American women aged 15–44 who first had premarital intercourse in 1960 or later. | Although the tabulations are not shown, the authors report that the mean age at first intercourse in the 1980s was slightly higher than in the 1970s. This may be an artifact of the sampling method, however. | The percentage of women who used any method at first intercourse increased significantly, from 39% in the early 1960s to 48% in the late 1970s. Contraceptive use at first intercourse increased sharply between the 1970s and the 1980s. | The condom was the leading method at first intercourse, chosen by 41% of those using contraception. |
| Forste and Heaton 1988 | National Survey of Family Growth, conducted in 1982; women aged 15–44. | 70% of adolescent women who had premarital sex experienced first intercourse before their 20th birthday; 30% began sexual activity before age 16. | About half those who initiated sexual activity before age 20 used contraception at first sex. | |
| Kahn, Rindfuss, and Guilkey 1990 | National Survey of Family Growth, Cycle 3 (1982). The analysis was limited to the subsample of young women (aged 15–24 in 1982) who had premarital sex as teenagers. | Slightly less than half of all teenagers used contraception at first intercourse. | The condom was the most popular method of contraception at first sex. | |
| Mosher and McNally 1991 | National Survey of Family Growth, cycle 4 (1988); includes a representative sample of 8,450 women 15–44 years old. | The proportion of women who used birth control at first sex remained roughly constant from 1965 to 1979 (44–47%) but increased to 53% in 1980–82 and to 65% in 1983–88. | The condom was the most popular method. The proportion of women whose partners used a condom at first premarital intercourse rose from about 22% in 1975–79 to 42% in 1983–88. | |
| Rind 1991 | A subgroup of 1,833 women from the 1982 National Survey of Family Growth, in which the women studied were aged 15–24 and had had premarital sex in their teens. | Two-thirds of black adolescents and almost one-half of whites used no contraception at first sex. | The condom was the most popular method used at first sex. Of those who reported prior sex, 14% of black teenagers and 22% of whites used a condom at first coitus. | |
| Poppen 1994 | Undergraduate students living in residence halls at a major private mid-Atlantic university, surveyed in 1979 and 1989. | In 1979, 86% of males and 73% of females reported having had sex. (Average age at first sex: 16.4 for males, 16.8 for females.) In 1989, 85% of males and 66% of females reported having had sex. (Average age at first sex: 16.7 for males, 16.7 for females.) | In 1979, 70% of respondents reported using contraception at first intercourse, compared with 71% in 1989. | In 1979 the condom was the most common contraceptive method used at first sex; 35% of respondents used it. The condom remained the most popular method in 1989, when 49% of respondents used it. |
| Mauldon and Luker 1996 | 1988 National Survey of Family Growth, American women aged 15–44. The data are from respondents aged 15–24 at the survey date who had lived in the United States at age 15. | Approximately 50% of women reported that they first had sex between the ages of 16 and 18. | The percentage of women who used contraception at first sex increased from 45% among women born between 1963 and 1966 to 59% among the 1970–72 birth cohort. | The condom was the most popular method of birth control at first sex. |
| Abma 1999 | National Survey of Family Growth, cycles 3 (1982), 4 (1988), and 5 (1995), women aged 15–44. | In 1995, 18% of teens had experienced sex by age 15, compared with 12% in 1988 and 1982. | Over time there has been an increase in the percentage of women who use contraception at first sex (48% in 1960–74, 76% in 1990–95). | |
| Terry and Manlove 2000 | National Survey of Family Growth, 1982, 1988, and 1995; National Survey of Adolescent Males, 1988 and 1995; and the Youth Risk Behavior Survey, 1990, 1993, and 1995. | In 1995, about 25% of all 15-to-17-year-olds and more than half of all 17-year-olds (59% of males and 52% of females) reported having had sex. Among 19-year-olds, 85% of males and 77% of females reported having had sex. | In 1982, 48% of females aged 15–19 used contraception at first sex. By 1995, 76% of teens reported having used birth control at first sex. | In 1988, 55% of sexually experienced males reported using a condom at first sex. By 1995 this percentage had increased to 69%. |
| Santelli et al. 2000 | National Survey of Family Growth (1988, 1995); National Survey of Adolescent Males (1988, 1995); Youth Risk Behavior Survey (1991, 1993, 1995, 1997); and the National Longitudinal Study of Adolescent Health (1995). | Summarizes the sexual experience of adolescents as reported in several major surveys. Provides gender-, race-, and ethnicity-specific data on the percentage of high-school adolescents (ages 15–17) who have had sex, from 32.2% (white females, NSFG 1988) to 89.5% (black males, YRBS 1993). |
Endnote
This research is based on data from the Add Health project, a program project designed by J. Richard Udry (PI) and Peter Bearman and funded by grant P01-HD31921 from the National Institute of Child Health and Human Development to the Carolina Population Center, University of North Carolina at Chapel Hill, with cooperative funding participation by the National Cancer Institute; the National Institute of Alcohol Abuse and Alcoholism; the National Institute on Deafness and Other Communication Disorders; the National Institute on Drug Abuse; the National Institute of General Medical Sciences; the National Institute of Mental Health; the National Institute of Nursing Research; the Office of AIDS Research, NIH; the Office of Behavior and Social Science Research, NIH; the Office of the Director, NIH, the Office of Research on Women's Health, NIH; the Office of Population Affairs, DHHS; the National Center for Health Statistics; the Centers for Disease Control and Prevention, DHHS; the Office of Minority Health; the Office of Public Health and Science, DHHS; the Office of the Assistant Secretary for Planning and Evaluation, DHHS; and the National Science Foundation. Persons interested in obtaining data files from the National Longitudinal Study of Adolescent Health should contact Jo Jones, Carolina Population Center, 123 West Franklin Street, Chapel Hill, NC 27516-3997 (jo_jones@unc.edu).
References
- Abma JC. Circumstances of First Sex among U.S. Women: Examining Trends Using Retrospective Reports in a Cross-Sectional Survey. 1999. Paper presented at the annual meeting of the Population Association of America, New York City.
- Abma JC, Driscoll A, Moore K. Young Women's Degree of Control over First Intercourse: An Exploratory Analysis. Family Planning Perspectives. 1998;30(1):12–8. [PubMed] [Google Scholar]
- Abma JC, Sonenstein FL. Sexual Activity and Contraceptive Practices among Teenagers in the United States, 1988 and 1995. Vital and Health Statistics. 2001;23(21):1–88. doi: 10.1037/e304002003-001. [DOI] [PubMed] [Google Scholar]
- Alexander HM, Callcott R, Dobson AJ, Hardes GR, Lloyd DM, O'Connell DL, Leeder SR. Cigarette Smoking and Drug Use in Schoolchildren: IV—Factors Associated with Changes in Smoking Behavior. International Journal of Epidemiology. 1983;12(1):59–66. doi: 10.1093/ije/12.1.59. [DOI] [PubMed] [Google Scholar]
- Aral SO. Sexually Transmitted Diseases: Magnitude, Determinants and Consequences. International Journal of STD and AIDS. 2001;12(4):211–5. doi: 10.1258/0956462011922814. [DOI] [PubMed] [Google Scholar]
- Ary DV, Duncan TE, Biglan A, Metzler CM, Noell JW, Smolkowski K. Development of Adolescent Problem Behavior. Journal of Abnormal Psychology. 1999;27(2):141–50. doi: 10.1023/a:1021963531607. [DOI] [PubMed] [Google Scholar]
- Baker SA, Thalberg SP, Morrison DM. Parents’ Behavioral Norms as Predictors of Adolescent Sexual Activity and Contraceptive Use. Adolescence. 1988;23(90):265–82. [PubMed] [Google Scholar]
- Biglan A, Metzler CW, Wirt R, Ary D, Noell J, Ochs L, French C, Hood D. Social and Behavioral Factors Associated with High-Risk Sexual Behavior among Adolescents. Journal of Behavioral Medicine. 1990;13(3):245–61. doi: 10.1007/BF00846833. [DOI] [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention (CDC) Youth Risk Behavior Surveillance—United States, 1999. MMWR Surveillance Summaries. 2000;49:1–96. SS05. [PubMed] [Google Scholar]
- Chantala K, Tabor J. Strategies to Perform a Design-Based Analysis Using the Add Health Data. Unpublished manuscript. University of North Carolina at Chapel Hill.
- Charlton A, Blair V. Predicting the Onset of Smoking in Boys and Girls. Social Science and Medicine. 1989;29(7):813–8. doi: 10.1016/0277-9536(89)90080-4. [DOI] [PubMed] [Google Scholar]
- Chassin L, Presson CC, Sherman SJ, Corty E, Olshavsky RW. Predicting the Onset of Cigarette Smoking in Adolescents: A Longitudinal Study. Journal of Applied Social Psychology. 1984;14(3):224–43. [Google Scholar]
- Crockett LJ, Bingham CR, Chopak JS, Vicary JR. Timing of First Sexual Intercourse: The Role of Social Control, Social Learning, and Problem Behavior. Journal of Youth and Adolescence. 1996;25(1):89–111. doi: 10.1007/BF01537382. [DOI] [PubMed] [Google Scholar]
- Donovan JE, Jessor R. Structure of Problem Behavior in Adolescence and Young Adulthood. Journal of Counseling and Clinical Psychiatry. 1985;53(6):890–904. doi: 10.1037//0022-006x.53.6.890. [DOI] [PubMed] [Google Scholar]
- Donovan JE, Jessor R, Costa FM. Syndrome of Problem Behavior in Adolescence and Young Adulthood. Journal of Consulting and Clinical Psychology. 1988;56(5):762–5. doi: 10.1037//0022-006x.56.5.762. [DOI] [PubMed] [Google Scholar]
- Elliott DS, Morse BJ. Delinquency and Drug Use as Risk Factors in Teenage Sexual Activity. Youth and Society. 1989;21(1):32–60. [Google Scholar]
- Flay BR, Hu FB, Siddiqui O, Day LE, Hedeker D, Petraitis J, Richardson J, Sussman S. Differential Influence of Parental Smoking and Friends’ Smoking on Adolescent Initiation and Escalation of Smoking. Journal of Health and Social Behavior. 1994;35(3):248–65. [PubMed] [Google Scholar]
- Forrest JD. Adolescent Reproductive Behavior: An International Comparison of Developed Countries. In: Stiffman Arlene Rubin, Feldman Ronald A., editors. Advances in Adolescent Health. London: Jessica Kingsley; 1990. pp. 13–33. [PubMed] [Google Scholar]
- Forste RT, Heaton TB. Initiation of Sexual Activity among Female Adolescents. Youth and Society. 1988;19(3):250–68. doi: 10.1177/0044118x88019003002. [DOI] [PubMed] [Google Scholar]
- Foshee V, Bauman KE. Parental and Peer Characteristics as Modifiers of the Bond-Behavior Relationship: An Elaboration of Control Theory. Journal of Health and Social Behavior. 1992;33(1):66–76. [PubMed] [Google Scholar]
- Fu H, Darroch JE, Haas T, Ranjit N. Contraceptive Failure Rates: New Estimates from the 1995 National Survey of Family Growth. Family Planning Perspectives. 1999;31(2):56–63. [PubMed] [Google Scholar]
- Gillmore MR, Butler SS, Lohr MJ, Gilchrist L. Substance Use and Other Factors Associated with Risky Sexual Behavior among Pregnant Adolescents. Family Planning Perspectives. 1992;24(6):255–61. 268. [PubMed] [Google Scholar]
- Glei DA. Measuring Contraceptive Use Patterns among Teenagers and Adult Women. Family Planning Perspectives. 1999;31(2):73–80. [PubMed] [Google Scholar]
- Greenberg J, Magder L, Aral S. Age at First Coitus. A Marker for Risky Sexual Behavior in Women. Sexually Transmitted Diseases. 1992;19(6):331–4. [PubMed] [Google Scholar]
- Grube JW, Morgan M. Attitude–Social Support Interactions: Contingent Consistency Effects in the Prediction of Adolescent Smoking, Drinking and Drug Use. Social Psychology Quarterly. 1990;53(4):329–39. [Google Scholar]
- Harvey SM, Spigner C. Factors Associated with Sexual Behavior among Adolescents: A Multivariate Analysis. Adolescence. 1995;30(118):253–64. [PubMed] [Google Scholar]
- Hayward MD, Grady WR, Billy JO. The Influence of Socioeconomic Status on Adolescent Pregnancy. Social Science Quarterly. 1992;73(4):750–72. [Google Scholar]
- Hockaday C, Crase SJ, Shelley MC, II, Stockdale DF. A Prospective Study of Adolescent Pregnancy. Journal of Adolescence. 2000;23(4):423–38. doi: 10.1006/jado.2000.0329. [DOI] [PubMed] [Google Scholar]
- Hofferth SL, Kahn JR, Baldwin W. Premarital Sexual Activity among U.S. Teenage Women over the Past Three Decades. Family Planning Perspectives. 1987;19(2):46–53. [PubMed] [Google Scholar]
- Hogan DP, Kitagawa EM. The Impact of Social Status, Family Structure, and Neighborhood on the Fertility of Black Adolescents. American Journal of Sociology. 1985;90(4):825–55. [Google Scholar]
- Holmbeck GN, Crossman RE, Wandrei ML, Gasiewski E. Cognitive Development, Egocentrism, Self-Esteem, and Adolescent Contraceptive Knowledge, Attitudes, and Behavior. Journal of Youth and Adolescence. 1994;23(2):169–93. doi: 10.1007/BF01537444. [DOI] [PubMed] [Google Scholar]
- Jemmott LW, Jemmott JB., III Family Structure, Parental Strictness, and Sexual Behavior among Inner-City Black Male Adolescents. Journal of Adolescent Research. 1992;7(2):192–207. [Google Scholar]
- Jessor R, Donovan JE, Costa FM. Beyond Adolescence: Problem Behavior and Young Adult Development. Cambridge: Cambridge University Press; 1991. [Google Scholar]
- Jessor R, Jessor SL. Problem Behavior and Psychosocial Development: A Longitudinal Study of Youth. New York: Academic Press; 1977. [Google Scholar]
- Jessor SL, Jessor R. Transition from Virginity to Nonvirginity among Youth: A Social-Psychological Study over Time. Developmental Psychology. 1975;11(4):473–84. [Google Scholar]
- Kahn JR, Rindfuss RR, Guilkey DK. Adolescent Contraceptive Method Choices. Demography. 1990;27(3):323–35. [PubMed] [Google Scholar]
- Koenig MA, Zelnik M. The Risk of Premarital First Pregnancy among Metropolitan-Area Teenagers: 1976 and 1979. Family Planning Perspectives. 1982;14(5):239–41. 243–7. [PubMed] [Google Scholar]
- Ku L, Sonenstein FL, Lindberg LD, Bradner CH, Boggess S, Pleck JH. Understanding Changes in Sexual Activity among Young Metropolitan Men: 1979–1995. Family Planning Perspectives. 1998;30(6):256–62. [PubMed] [Google Scholar]
- Mahler K. Condom Use Increase in Norway Appears Related More to Contraception Than to Disease Prevention. Family Planning Perspectives. 1996;28(2):82–3. [Google Scholar]
- Mauldon J, Luker K. The Effects of Contraceptive Education on Method Use at First Intercourse. Family Planning Perspectives. 1996;28(1):19–24. 41. [PubMed] [Google Scholar]
- McGuire E, III, Shega J, Nicholls G, Deese P, Landefeld CS. Sexual Behavior, Knowledge, and Attitudes about AIDS among College Freshmen. American Journal of Preventive Medicine. 1992;8(4):226–34. [PubMed] [Google Scholar]
- Mensch B, Kandel DB. Drug Use as a Risk Factor for Premarital Teen Pregnancy and Abortion in a National Sample of Young White Women. Demography. 1992;29(3):409–29. [PubMed] [Google Scholar]
- Meschke LL, Silbereisen RK. The Influence of Puberty, Family Processes, and Leisure Activities on the Timing of First Sexual Experience. Journal of Adolescence. 1997;20(4):403–18. doi: 10.1006/jado.1997.0096. [DOI] [PubMed] [Google Scholar]
- Mettlin C. Peer and Other Influences on Smoking Behavior. Journal of School Health. 1976;46(9):529–36. doi: 10.1111/j.1746-1561.1976.tb02047.x. [DOI] [PubMed] [Google Scholar]
- Miller KS, Clark LF, Wendell DA, Levin ML, Gray-Ray P, Velez CN, Webber MP. Adolescent Heterosexual Experience: A New Typology. Journal of Adolescent Health. 1997;20(3):179–86. doi: 10.1016/S1054-139X(96)00182-6. [DOI] [PubMed] [Google Scholar]
- Mosher WD, Bachrach CA. First Premarital Contraceptive Use: United States, 1960–1982. Studies in Family Planning. 1987;18(2):83–95. [PubMed] [Google Scholar]
- Mosher WD, McNally JW. Contraceptive Use at First Premarital Intercourse: United States, 1965–1988. Family Planning Perspectives. 1991;23(3):108–16. [PubMed] [Google Scholar]
- Mott FL, Fondell MM, Hu PN, Kowaleski-Jones L, Menaghan EG. The Determinants of First Sex by Age 14 in a High-Risk Adolescent Population. Family Planning Perspectives. 1996;28(1):13–8. [PubMed] [Google Scholar]
- Mott FL, Haurin RJ. Linkages between Sexual Activity and Alcohol and Drug Use among American Adolescents. Family Planning Perspectives. 1988;20(3):128–36. [PubMed] [Google Scholar]
- Murphy JJ, Boggess S. Increased Condom Use among Teenage Males, 1988–1995: The Role of Attitudes. Family Planning Perspectives. 1998;30(6):276–80. 303. [PubMed] [Google Scholar]
- National Research Council. Contraception and Reproduction: Health Consequences for Women and Children in the Developing World. Washington, D.C.: National Academy Press; 1989. [PubMed] [Google Scholar]
- Needle RH. The Relationship between First Sexual Intercourse and Ways of Handling Contraception among College Students. Journal of the American College Health Association. 1975;24(2):106–11. [PubMed] [Google Scholar]
- Needle R, McCubbin H, Wilson M, Reineck R, Lazar A, Mederer H. Interpersonal Influences in Adolescent Drug Use—The Role of Older Siblings, Parents and Peers. International Journal of the Addictions. 1986;21(7):739–66. doi: 10.3109/10826088609027390. [DOI] [PubMed] [Google Scholar]
- Nguyet NTM, Maheux B, Beland F, Pica LA. Sexual Behaviors and Condom Use: A Study of Suburban Male Adolescents. Adolescence. 1994;29(113):37–48. [PubMed] [Google Scholar]
- Paul C, Fitzjohn J, Herbison P, Dickson N. The Determinants of Sexual Intercourse before Age 16. Journal of Adolescent Behavior. 2000;27(2):136–47. doi: 10.1016/s1054-139x(99)00095-6. [DOI] [PubMed] [Google Scholar]
- Poppen PJ. Adolescent Contraceptive Use and Communication: Changes over a Decade. Adolescence. 1994;29(115):503–14. [PubMed] [Google Scholar]
- Pugh MD, DeMaris A, Giordano PC, Groat HT. Delinquency as a Risk Factor in Teenage Pregnancy. Sociological Focus. 1990;23(2):89–100. [Google Scholar]
- Rind P. Adolescents Are More Likely to Use Condom Than Pill at First Coitus. Family Planning Perspectives. 1991;23(2):92–3. [Google Scholar]
- Rodgers KB. Parenting Processes Related to Sexual Risk-Taking Behaviors of Adolescent Males and Females. Journal of Marriage and the Family. 1999;61(1):99–109. [Google Scholar]
- Santelli JS, Lindberg LD, Abma J, McNeely CS, Resnick M. Adolescent Sexual Behavior: Estimates and Trends from Four Nationally Representative Surveys. Family Planning Perspectives. 2000;32(4):156–65. 194. [PubMed] [Google Scholar]
- Sarigiani PA, Ryan L, Petersen AC. Prevention of High-Risk Behaviors in Adolescent Women. Journal of Adolescent Health. 1999;25(2):109–19. doi: 10.1016/s1054-139x(99)00015-4. 10.1016/S1054-139X(99)00015-4. [DOI] [PubMed] [Google Scholar]
- Sorensen RC. Adolescent Sexuality in Contemporary America. New York: World Publishing; 1973. [Google Scholar]
- St Lawrence JS, Scott CP. Examination of the Relationships between African American Adolescents’ Condom Use at Sexual Onset and Later Sexual Behavior: Implications for Condom Distribution Programs. AIDS Prevention and Education. 1996;8(3):258–66. [PubMed] [Google Scholar]
- Stigum H, Magnus p, Veierød MB, Bakketeig LS. Impact on Sexually Transmitted Disease Spread of Increased Condom Use by Young Females, 1987–1992. International Journal of Epidemiology. 1995;24(4):813–20. doi: 10.1093/ije/24.4.813. [DOI] [PubMed] [Google Scholar]
- Streetman LG. University of Delaware; 1995. The Relationship of Delinquent Behavior and Alcohol/Drug Involvement to Adolescent Nonmarital Pregnancy and Its Resolution. Ph.D. diss. [Google Scholar]
- Terry E, Manlove J. Child Trends Research Brief. Washington, D.C.: Child Trends; 2000. Trends in Sexual Activity and Contraceptive Use among Teens. [Google Scholar]
- Turbin MS, Jessor R, Costa FM. Adolescent Cigarette Smoking: Health-Related Behavior or Normative Transgression. Prevention Science. 2000;1(3):115–24. doi: 10.1023/a:1010094221568. 10.1023/A:1010094221568. [DOI] [PubMed] [Google Scholar]
- Turner RA, Irwin CE, Jr, Tschann JM, Millstein SG. Autonomy, Relatedness, and the Initiation of Health Risk Behaviors in Early Adolescence. Health Psychology. 1993;12(3):200–8. doi: 10.1037//0278-6133.12.3.200. [DOI] [PubMed] [Google Scholar]
- Udry JR, Billy JOG. Initiation of Coitus in Early Adolescence. American Sociological Review. 1987;52(6):841–55. [Google Scholar]
- Udry JR, Kovenock J, Morris NM. Early Predictors of Nonmarital First Pregnancy and Abortion. Family Planning Perspectives. 1996;28(3):113–6. [PubMed] [Google Scholar]
- Upchurch DM, Levy-Storms L, Sucoff CA, Aneshensel CS. Gender and Ethnic Differences in the Timing of First Intercourse. Family Planning Perspectives. 1998;30(3):121–7. [PubMed] [Google Scholar]
- Urberg KA, Cheng CH, Shyu SJ. Grade Changes in Peer Influence on Adolescent Cigarette Smoking: A Comparison of Two Measures. Addictive Behaviors. 1991;16(1–2):21–8. doi: 10.1016/0306-4603(91)90036-h. [DOI] [PubMed] [Google Scholar]
- Watts GF, Nagy S. Sociodemographic Factors, Attitudes, and Expectations toward Adolescent Coitus. American Journal of Health Behavior. 2000;24(4):309–17. [Google Scholar]
- Whitbeck LB, Conger RD, Simons RL, Kao MY. Minor Deviant Behavior and Adolescent Sexual Activity. Youth and Society. 1993;25(1):24–37. [Google Scholar]
- Wilks J. The Relative Importance of Parents and Friends in Adolescent Decision Making. Journal of Youth and Adolescence. 1986;15(4):323–34. doi: 10.1007/BF02145729. [DOI] [PubMed] [Google Scholar]
- Wilks J, Callan VJ, Austin DA. Parent, Peer and Personal Determinants of Adolescent Drinking. British Journal of Addiction. 1989;84(6):619–30. doi: 10.1111/j.1360-0443.1989.tb03477.x. [DOI] [PubMed] [Google Scholar]
- Williams GC, Cox EM, Hedberg VA, Deci EL. Extrinsic Life Goals and Health-Risk Behaviors in Adolescents. Journal of Applied Social Psychology. 2000;30(8):1756–71. [Google Scholar]
- Wilson MD, Kastrinakis M, D'Angelo LJ, Getson P. Attitudes, Knowledge, and Behavior Regarding Condom Use in Urban Black Adolescent Males. Adolescence. 1994;29(113):13–26. [PubMed] [Google Scholar]
- Zabin LS, Hardy JB, Smith EA, Hirsch MB. Substance Use and Its Relation to Sexual Activity among Inner-City Adolescents. Journal of Adolescent Health Care. 1986;7(5):320–31. doi: 10.1016/s0197-0070(86)80160-7. [DOI] [PubMed] [Google Scholar]
- Zabin LS, Kantner JF, Zelnik M. The Risk of Adolescent Pregnancy in the First Months of Intercourse. Family Planning Perspectives. 1979;11(4):215, 217–22. [PubMed] [Google Scholar]
- Zelnik M, Kantner JF. Contraceptive Patterns and Premarital Pregnancy among Women Aged 15–19 in 1976. Family Planning Perspectives. 1978;10(3):135–42. [PubMed] [Google Scholar]
- Zelnik M, Kantner JF, Ford K. Sex and Pregnancy in Adolescence. Beverly Hills, Calif.: Sage; 1981. [Google Scholar]
- Zelnik M, Shah FK. First Intercourse among Young Americans. Family Planning Perspectives. 1983;15(2):64–70. [PubMed] [Google Scholar]