

Abstract
The NIH roadmap has among its goals, to promote studies designed to improve public understanding of biomedical and behavioral science, and to develop strategies for promoting collaborations between scientists and communities toward improving the public’s health. Here, we report findings on the impact of a partnership between the Oregon Health and Science University (OHSU) and the Oregon Museum of Science and Industry (OMSI) designed to inform the public about health research being conducted in Oregon, which was linked to a 17-week traveling exhibition of BodyWorlds3. Measures included the public’s understanding of health knowledge, attitudes, intended health behaviors, and visitor experience in their interactions with OHSU experts/volunteers, which were collected using exit surveys administered verbally. Nine hundred fifty-three surveys were included in analyses. Among those who felt that health behavior change was relevant to them, 67.4% of smokers (n = 133) intended to change their smoking behavior, 58.6% (of 677) intended to change their eating habits, 60.3% (of 667) intended to change their exercise routine, and 47% (of 448) intended to change their dental care habits. Forty-six percent of these visited the OHSU research exhibits (n = 437), and responded to how the exhibit changed their understanding about and openness to participate in health research. Greater than 85% had a much improved understanding of NIH research at OHSU and >58% reported they would be willing to participate in future research studies at OHSU. In conclusion, research partnerships between academic institutions and community-based museums appear to be viable ways to inform the public about research, stimulate their interest as future participants, and possibly influence their intention to improve health behaviors.
Keywords: Community health, Health education, Health promotion research
Introduction
In the decades since chronic illnesses replaced infectious diseases as the leading causes of death, public health researchers have shifted their focus from the individual to the community in recognition that community-level changes will foster and sustain behavior change. The prior emphasis on individual lifestyle change has been broadened to include social and environmental factors, often without increased resources [1, 2]. In 2007, the National Center for Chronic Disease Prevention and Health Promotion and the Division of Adult and Community Health hosted a panel of expert advisors to participate in the National Expert Panel on Community Health Promotion. Their charge was specifically to identify new ways to support community health promotion at the national level [3]. Recommendations from this panel included promoting community-based participatory research, surveillance, training and capacity building [3]. Similarly, the NIH (National Institutes of Health) roadmap has among its goals, to promote studies designed to improve public understanding of biomedical and behavioral science, and to develop strategies for promoting collaborations between scientists and communities toward improving the public’s health [4].
Though laudable as a goal, studies on how to accomplish NIH’s goal successfully are limited. Many research papers on health promotion, research, and educating the public focus on use of the Internet [5–7], which are individualized versus community-based activities. Other studies have focused on using tighter social networks, such as senior centers or church-based programs to reach the public [8–12]. Much less is known about research partnerships with non-faith based programs or those where membership is more loosely characterized.
We created a partnership between the Oregon Health and Science University (OHSU) and the Oregon Museum of Science and Industry (OMSI) designed to inform the public about health research being conducted in Oregon. A central feature of this partnership was a combined exhibit project where OHSU co-sponsored a 17-week exhibition of BodyWorlds3, a traveling exhibition of preserved human bodies and body parts that are prepared using a technique called plastination to reveal inner anatomical structures on over 200 authentic human specimens [13]. At the time of the OHSU/OMSI partnership, there were three versions of the exhibit, and OHSU received the 3rd one. The mission and purpose of BodyWorlds is to educate the lay public about the human body, leading to a greater appreciation of its complexities and better health awareness [14]. All the human plastinates are from people who donated their bodies for plastination via a body donation program. More than 25 million people have seen at least one of the BodyWorlds exhibits to-date [15]. We linked a series of 17 thematic research exhibits to the BodyWorlds exhibit to educate the public about research going on at OHSU. The Oregon Clinical and Translational Research Institute (NIH Clinical and Translational Science Award), in part, funded this project to develop and staff the OHSU research exhibits, especially the evaluation activities. The purpose of this paper is to report on our mixed methods approach to evaluating the impact of this program on the public’s understanding of health knowledge, attitudes, intended health behaviors, and visitor experience in their interactions with OHSU clinical experts, NIH researchers and other volunteers.
Methods
A planning committee was formed between OHSU basic science, clinical and research faculty and leadership, and administrative staff from the OMSI. The planning committee developed strategies for creating 17 thematic research presentations, which were rotated weekly for one of each of the 17 weeks of the BodyWorlds exhibit as well as media/marketing strategies to engage the public. A subcommittee was formed to create evaluation instruments, develop assessment approaches, and collect and analyze evaluation data. All evaluation activities were reviewed and approved by the OHSU Institutional Review Board (IRB). Finally, a sub-committee was formed to recruit and train OHSU faculty in how to respond to questions regarding both the BodyWorlds exhibit and the OHSU/NIH research being presented during the theme weeks.
The Exhibits
OHSU schools, departments or programs developed two types of exhibits on NIH-funded research at OMSI. The two formats were designed to address different types of health messaging. The first format was the permanent, unstaffed exhibits, produced to introduce the public to the NIH, translational research, and that federal tax dollars funds most of the biomedical research at OHSU. The unstaffed exhibits required large amounts of time and financial resources to design, prototype, construct, and then deploy to emphasize the role of the NIH in biomedical research at OHSU and the importance of current research on informing modern practices. The dentistry exhibit is an example of a permanent unstaffed exhibit designed to introduce the public to modern dental practice and the importance of oral hygiene on whole body health. This was accomplished through an animated interactive game, Jeopardy-style matching game and videos of modern oral surgery and a display of museum specimens of oral and dental anomalies. This type of exhibit was accessible to the public during all hours of the BodyWorlds exhibit.
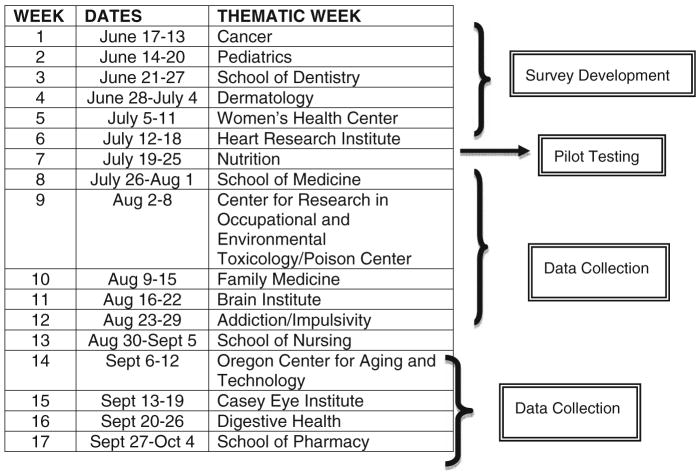
The second exhibit format consisted of staffed exhibits where NIH researchers directly interfaced with the public and developed a series of schematic posters and simple mechanisms to help explain their research. To optimize the opportunities for interaction with the public, there was a new research theme every week of the 17-week duration of the BodyWorlds exhibit (Table 1). Each theme week exhibit was staffed with at least two people for 8 h each day of 12 h that the main BodyWorlds exhibit was open. Using this approach, visitors to the NIH-funded OHSU exhibits would have a consistent exposure to unstaffed exhibits and a changing theme of the staffed exhibit upon exiting BodyWorlds.
Table 1.
Thematic weeks and data collection activities
|
Survey Design and Testing Procedures
The survey instrument was developed by a team of individuals from multiple departments and centers around OHSU and included twenty-seven questions, which were phrased to measure change as a result of exhibit attendance, and addressed intent to change specific health-related behaviors, knowledge of and willingness to participate in research at OHSU, the role of NIH, and interest in participating in research at OHSU. Questions also covered visitor perception of the OHSU ask the experts and theme displays outside the BodyWorlds exhibit, prior experience with OHSU, personal health concerns and basic demographics. The majority of these items were measured using a Likert scale with values ranging from one to five (strongly disagree, disagree, neutral, agree, and strongly agree). Participants could indicate when an item was not applicable to them. The evaluation team met multiple times to refine question and answer category wording, formatting and to oversee pilot testing of the instrument at the beginning of the project. Lastly, the survey asked two open ended questions, one about the top three health or healthcare concerns of the participants and their families, and the other about how the exhibits improved their understanding of research at OHSU.
Data Collection
Eight data collectors were recruited and specially trained on the background of the project, goals for the evaluation, ethics in human subjects research, pre-survey script, and recruitment tactics, survey instrument, data quality, and data collection logistics. To ensure consistency with the interviewer-administered survey instrument the team reviewed each question one by one, role-played in front of the rest of the team, and split into pairs and took turns as interviewer/interviewee. The team supervisor was also present during each data collector’s first shift to ensure uniformity in data collection methods. Surveys were completed interview-style and took 5–10 min to complete. Data collectors recorded participants’ responses on a scannable form. Participants received two tickets for a scenic aerial tram ride in Portland in appreciation for their assistance. Data collection was conducted over the course of 2 months between July 30th and September 29th, 2007. Data collection shifts were 4 hours long. Originally the data collection schedule was designed to cover morning, afternoon and evening blocks on every day of the week. Evening shifts turned out to be much slower, however, and about half way through data collection we changed the remaining evenings to day shifts in order to reach our target of 1,000 completed surveys. We conducted evaluation activities during all but one of the OHSU theme week exhibits during the data collection period, which after pilot testing, occurred between Week 8 and Week 17. The 1 week where data collection was missed occurred inadvertently due to an unanticipated scheduling problem.
Sampling Strategy
The first person who passed the data collectors at the start of each shift was approached and asked to complete the survey; if that person declined to participate, the next person would be approached, and so on, until an individual agreed to participate. Once the data collector completed a survey, reviewed the form for accuracy and filed it away, s/he was instructed to approach the second (rather than the first) person who passed. If this person refused, s/he was told to approach each following person as above. Only one member of a family or group was interviewed in order to optimize sample diversity.
Data Analysis
Descriptive statistics were used to characterize study participants’ responses. Not applicable responses were excluded from some results, which are described. Reponses to questions with strongly agree and agree were collapsed into one category for overall agreement, and strongly disagree, disagree, and neutral were collapsed as indicated in other analyses. Text responses from the open-ended questions were analyzed using a standardized iterative process [16], facilitated by the qualitative data management and analysis software QSR NVivo. Key themes emerging from the open-ended answers were transformed into codes, and the codes applied to the data. Two team members independently coded a percentage of the text responses, and code definitions were revised and data re-coded until acceptable agreement was reached.
Results
A total of 984 surveys were returned, scanned, and verified. Five people were under 18 years of age and 26 were current or former OHSU employees. Thus, 31 participants were not eligible to complete the adult survey, leaving 953 surveys for analysis. The demographics of the sample are summarized in Table 2. The age and gender distribution of the sample was very similar to the survey conducted by OMSI during the BodyWorlds exhibit. The majority was female, in the 45–64 year age category, well educated and Caucasian.
Table 2.
Demographic characteristics of sample
| Percent (N) | |
|---|---|
| Gender | |
| Female | 60.0% (571) |
| Age | |
| 18–24 | 13.1% (125) |
| 25–44 | 37.7% (359) |
| 45–64 | 41.0% (391) |
| 65 or older | 8.2% (78) |
| Race | |
| White | 92.5% (882) |
| Black | 1.0% (10) |
| Asian/Pacific Islander | 3.9% (37) |
| American Indian/Alaska Native | 1.5% (14) |
| Other | 3.6% (34) |
| Hispanic Origin | 4.6% (44) |
| Education | |
| Less than HS graduate | 0.7% (7) |
| HS graduate | 8.9% (85) |
| Some college or community college | 34.3% (327) |
| 4-year college graduate | 28.4% (270) |
| Some graduate school | 7.2% (69) |
| Advanced degree (Masters or doctorate) | 20.4% (194) |
| State of residence | |
| Living in Oregon or SW Washington | 81.2% (774) |
| Received health care from OHSU in past 5 years | |
| Never | 85.9% (817) |
| Once | 5.4% (51) |
| 2–3 times | 3.4% (32) |
| More than 3 times | 5.4% (51) |
| Prior research experience | |
| Previously volunteered for OHSU research study | 5.9% (57) |
While all respondents (n = 953) viewed the BodyWorlds exhibit, less than half (46%) additionally viewed the OHSU research exhibits. Reasons for not viewing the OHSU exhibits included (categories not mutually exclusive): not enough time (35.0%), not interested/not aware (48.5%), and 35.9% had other reasons (tired or hungry or overwhelmed by BodyWorlds, kids who were ready to go home, wanted to move on to other parts of OMSI, exhibits were too crowded or unmanned).
Participants were asked how their experience at BodyWorlds influenced their intentions to change health behaviors in three areas: eating and exercise habits, smoking, and dental care. Approximately 30% of those surveyed (n = 286) did not feel that changing the amount of exercise they do was applicable to them, 29% (n = 276) did not feel that changing their eating habits was applicable to them, >86% of the sample did not smoke (n = 820), and 45% (n = 429) did not feel that changing the care of their teeth was applicable to them. Figure 1 provides the percent of respondents that intend to change their health behavior among those for whom the question was applicable (response numbers vary because categories were not mutually exclusive). Among those who smoked, the intention to change behavior was highest, with exercise change and eating habits change closely following.
Fig. 1.

Intention to change health behaviors as a result of the exhibits
Figure 2 illustrates, among those who visited the OHSU research exhibits (n = 437), respondents’ reactions to how the exhibit changed their understanding about and openness to participate in health research. Greater than 85% had a much improved understanding of research at OHSU and >58% reported they would be willing to participate in future research studies at OHSU.
Fig. 2.

Respondent understanding about/interest in research at OHSU (n = 437). *NIH = National Institutes of Health
Thematically coded responses to the open-ended text questions are included in Tables 3 and 4. Top health/healthcare concerns were lifestyle-related items such as diet, fitness, weight and prevention, and health maintenance, as well as access to care and potentially life-threatening diseases like heart disease, cancer, and diabetes. When asked the most important thing they had learned about research at OHSU, respondents discussed gaining a better understanding of anatomy and organ systems, amazement at the amount and variety of research conducted, a greater awareness that the ultimate goal of research is better population health, and an appreciation that an academic institution was reaching out to the community. Eighty-one respondents could not characterize what they learned, left this variable blank or said they did not learn anything.
Table 3.
Text responses to the survey question: What are the top three health or healthcare concerns for you or your family (n = 953 total responses)
| Text response category | Number of responses |
|---|---|
| General health/healthcare concerns | |
| Access to healthcare | 92 |
| Accidents & injuries | 17 |
| Aging | 88 |
| Alternative medicine | 3 |
| Cancer—all | 311 |
| Children | 22 |
| Dental | 48 |
| Ear | 7 |
| Environment | 37 |
| Eyes | 27 |
| For family member | 51 |
| Genetics | 8 |
| Lifestyle (total = 603) | |
| Chronic disease management | 1 |
| Diet | 191 |
| Fitness | 166 |
| Hygiene | 1 |
| Motivation | 2 |
| Prevention & health maintenance | 106 |
| Vaccination | 5 |
| Weight | 153 |
| No health issues | 40 |
| Other | 26 |
| Research | 16 |
| Sleep | 9 |
| Substance abuse | 27 |
| Treatment | 13 |
| Women’s health | 6 |
| Major organ systems concerns | |
| Circulatory System (total = 372) | |
| Blood pressure | 82 |
| Cholesterol | 54 |
| Heart | 230 |
| Digestive system | 56 |
| Endocrine system (total = 160) | |
| Diabetes | 151 |
| Integumentary system | 32 |
| Lymphatic system | 24 |
| Musculo-skeletal system (total = 169) | |
| Arthritis | 52 |
| Nervous system (total = 67) | |
| Mental health | 55 |
| Reproductive system (total = 99) | |
| Breast cancer | 56 |
| Respiratory system (total = 133) | |
| Smoking | 65 |
| Urinary system | 19 |
Table 4.
Text responses to the survey question: As a result of this exhibit, what is the most important thing you learned about research at OHSU? (n = 437 total responses, some responses double coded)
| Response category | Definition | # Mentions | Sample quotes |
|---|---|---|---|
| Body and clinical | When people say they gained a better understanding of anatomy or a specific organ system | 108 | “Learned anatomy”; “Effects of drugs and alcohol on the body”; “Brain 80% water”; “Learned more about mammography”; “Research about sleeping problems—found interesting”; “Smoking info was eye opening” |
| Scope of research | Includes amount of research, learned that OHSU does a specific type of research, variety of research | 72 | “There’s lots”; “How much there was, the variety”; “Oral care research” |
| General statements on value of research | Non-specific statements on the importance, necessity and informative value of research/the exhibits | 50 | “Research is important”; “Needed!”; “Very informative” |
| Improves lives | Statements that research helps people, either in the short or long-term. Also comments that learned that should care for either the entire body or a specific body part. Includes statements on prevention or preventive care. | 38 | “Research helps a lot of people.”; “How important it is to improve quality of life”; To take care of your body”; “To take care of teeth more”; “Need to prevent illnesses as well as cure them” |
| Community outreach and education | Statements about involving or reaching out to or educating the public/community, out of the academic environment. | 35 | “Helps inform public”; “Involved with community and were here” |
| OHSU-specific | Any mention of OHSU-specific information or fact learned | 21 | “Learned about an OHSU website, and can check website from home”; “Sophisticated local facility (research)” |
| Advances knowledge | Statements that research leads to new knowledge, answers, advances in science and clinical care. | 20 | “Helps find new answers”; “Medical advances in research” |
| Funding | Any mention of research funding or money needed for research/medicine; includes mention of NIH as a funder | 14 | “Takes a lot of money”; “That more money should be allocated to medicine.” |
| Progressive | Mentions of technology or cutting edge research, or advances that have allowed health care to be conducted in non-traditional settings. | 11 | “State of the art”; “That testing can be done in home instead of doing them in the labs” |
| Nature of research | Statements on what goes on in research, how it is conducted or what it takes to do research/how research is done. | 10 | “A lot of people it takes to do the research”; “Different methods used” |
| Other | Answers that do not fit into the defined categories | 9 | |
| Negative comment | Any negative comment in response to the question, no matter what topic the comment is directed at. | 4 | “The OHSU exhibits were a letdown after BodyWorlds.” |
| Plastination | Any mention of plastination, or the bodies in the BodyWorlds exhibit. | 4 | “Idea of plastination.” |
| Research is fun | Statements that research is fun, interesting, exciting. | 4 | “Research is cool” |
Only 26% of those surveyed asked a question of or listened to one of the OHSU experts, either in the BodyWorld3 exhibit or the OHSU research exhibits. Of the 247 people (26% of those surveyed) who asked a question of or listened to an OHSU expert, 97.6% found it helpful to very helpful. Only 2.4% found that the interaction was not helpful at all.
Of the 699 individuals (74% of those surveyed) who did not interact with an OHSU expert, 43.5% (n = 304) did not have questions for the expert, 15.7% (n = 110) said it was hard to find an expert, 4.3% (n = 30) said it would take too long to wait to speak to an expert, and about 52% (N = 361) had other reasons; for those who listed a reason, 216 said there were no experts present, 51 said the BodyWorlds audio tour answered their questions, 40 were experts or had access to an expert elsewhere, and 28 said the written explanations in the BodyWorlds exhibit answered their questions, 18 did not feel like talking to the experts, BodyWorlds was a personal experience, and 11 said their kids prevented them from asking questions of the expert.
Discussion
Our study is significant in that our findings suggest that this partnership between an academic medical center and a community science museum made a positive impact in two important areas: intention to improve health habits in diet and exercise, and participants’ knowledge about and interesting health research being conducted at OHSU. The BodyWorlds exhibit provided a vehicle to bring approximately 400,000 visitors to OMSI, and we used this opportunity to improve the public’s understanding of NIH funded research being conducted at OHSU schools of medicine, nursing, dentistry and engineering, all related to the health professions. Our findings suggest that we have made a positive impact in two important areas: intention to improve habits in diet and exercise, and participants’ knowledge about and interest in health research being conducted at OHSU. Why is intention to change health behaviors important? Several studies have shown that the greatest predictor of behavior change is change in intention to change that behavior [17, 18]. If our participants were considering a health behavior change and we were able to reinforce that intention or identify the initial need to change behavior, then we may have had an impact on their stage of health behavior change [19] from pre- contemplation or contemplation toward action or maintenance of future health.
Interestingly, lifestyle factors were the most frequently mentioned topic in response to the open-ended question on top health or healthcare concerns. Each of these factors (diet, fitness, weight, preventive care) require action on the part of the individual, and is further evidence that BodyWorlds, in conjunction with the OHSU thematic research exhibits, may have had an impact on health behavior. The mechanism is as yet unclear, although it may be a combination of fear (seeing real-world anatomical examples of the negative effects of unhealthy choices) and empowerment that comes from a better understanding of the body. Further research could aid in elucidating the process through which exhibits of this sort move people along the continuum of health behavior change.
Why is participants’ knowledge about and interest in health research important? The NIH has funded research at academic institutions for decades that have made little difference in most health indices, such as morbidity and mortality. The NIH’s CTSA program is designed to improve the translation of research from “bench to bedside” and beyond into public health and community-based clinical practice [4]. To do this successfully will require academic institutions to actively partner with community-based agencies and organizations. While this has occurred in the past, efforts need to increase rapidly and in many ways be different than they have over the past decades. It was sometimes difficult to recruit active NIH-researchers to leave their labs and come down to the local science museum to talk with the public. The themse listed arose from those groups willing to make such a commitment and to spend time developing explanatory posters and mechanisms for demonstrations. The program was designed so that visitors of the exhibit would emerge from the BodyWorlds exhibit and then directly enter the OHSU health research exhibits. Evaluations were conducted for both the general public visitors (age 18 and older) and for school groups, the latter of which involved the “Science in the City” Program (age 10–18). Specific methods and findings from the child portion of the project are reported elsewhere [20]. Past and present employees of OHSU were excluded from the study.
In prior studies, the academic institution received all or most of the funding for the research and community members volunteered their time and resources. More recently, community-based participatory research (CBPR) approaches have emerged and have been used in studies ranging from smoking cessation behavior to overcoming health disparities [21–24]. Ideally, CBPR is a collaborative approach to research that equitably involves all partners in the research process and recognizes the unique strengths that each brings [25]. CBPR has been associated with enhanced recruitment to research studies [26], and is particularly important for studies on culturally diverse populations [27, 28]. Clearly, the traditional scope of public health must be broadened to advance a new vision for improving community health and wellness.
In addition, accrual of patients to both clinical trials for disease treatment as well as studies to promote health among all population age groups can be challenging, especially in underserved populations [29]. If the type of program we conducted could improve interest in research, accrual could potentially become easier.
Answers to the open-ended question about what visitors to the thematic week exhibits learned from the displays also suggest that a sizable number increased their understanding of the scope of research conducted at OHSU, as well as the inherent value of health research. Respondents also indicated an appreciation for the fact that OHSU was involved with the community and was dedicated to sharing information with the public. As one person said, they are “trying to get information to the public, not just to [the] academic community.”
We were surprised to learn that we made a nearly 50% improvement in a well educated sample’s understanding that NIH research is funded by U.S. tax dollars. We expected that more participants, given the demographic characteristics of our participants having attended or graduated from college, would understand how NIH is funded. We were also surprised that this population appeared somewhat reluctant to speak with many of the physician or scientists who served in the role of experts for both the BodyWorlds and OHSU research exhibits. It may be that the public, in general, are intimidated by individuals with advanced training or perhaps those with advanced training do not appear open or welcoming to the public. More research is needed to understand this issue fully. If physicians and scientists are to be “stewards” of the health of the nation, successfully achieving appropriate interactions will be important.
A strength of our study is that we achieved a sample of nearly 1,000 respondents, which when compared to OMSI’s evaluation of characteristics of those who attended the exhibit were very similar. This suggests that our respondents were fairly typical of the type of community member who would attend this type of program.
Our study has some important limitations. Respondents took part in a post exhibit survey that was administered orally by trained research assistants. Though careful training and monitoring of collection procedures occurred, the study design as an observational post-test is limited. The evaluation sub-committee spent significant efforts attempting to implement a pre-post test design to more accurately capture changes in knowledge, attitudes and intended health changes, but the logistics of enrolling at the pre-period and capturing follow-up data following a very intense experience of examining closely human cadavers was not feasible. In addition, our design did not allow for a comparison group, which might have been possible if another exhibit on a different area had been available, but this was not the case. Despite these limitations, it is important to share findings in the published literature to provide a foundation of research on engaging the public and improving their understanding of and interest in health-related research.
In conclusion, research partnerships between academic institutions and community-based museums appear to be viable ways to inform the public about NIH research, stimulate their interest as future participants, and possibly influence their intention to improve health behaviors.
Acknowledgments
This work was supported by the Oregon Clinical and Translational Research Institute (NCRR # U54 RR023424, Eric Orwoll, MD, PI) and SEPA (NCRR #20443; William Cameron, PhD, PI). We would like to acknowledge the staff at the Oregon Museum of Science and Industry for their work on the BodyWorlds Exhibit.
References
- 1.Centers for Disease Control and Prevention (CDC) Behavioral risk factor surveillance system prevalence data. 1998 http://ww2.cdc.gov/nccdphp/brfss/index.asp.
- 2.Health Care Financing and Administration Department of Health and Human Services Fiscal Year. Freedom of Information Annual Report. [Accessed April 3, 2008];2000 ( http://www.hhs.gov/foia/reports/00anlrpt.html)
- 3.Navarro AM, Voetsch KP, Liburd LC, Giles HW, Collins JL National Expert Panel on Community Health Promotion. Charting the future of community health promotion: Recommendations from the National Expert Panel on Community Health Promotion. Preventing Chronic Disease. 2007;4(3):A68. [PMC free article] [PubMed] [Google Scholar]
- 4. [Accessed September 7, 2008];Office of Portfolio Analysis and Strategic Initiatives. ( http://nihroadmap.nih.gov/)
- 5.Ivanitskaya L, O’Boyle I, Casey AM. Health information literacy and competencies of information age students: Results from the interactive online Research Readiness Self-Assessment (RRSA) Journal of Medical Internet Research. 2006;8(2):e6. doi: 10.2196/jmir.8.2.e6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Logan RA, Tse T. A multidiscipline conceptual framework for consumer health informatics. Medinfo. 2007;12(2):1169–1173. [PubMed] [Google Scholar]
- 7.Potts HW. Is e-health progressing faster than e-health research? Journal of Medical Internet Research. 2006;8(3):3–24. doi: 10.2196/jmir.8.3.e24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Resnick B, Vogel A, Luisi D. Motivating minority older adults to exercise. Cultural Diversity & Ethnic Minority Psychology. 2006;12(1):17–29. doi: 10.1037/1099-9809.12.1.17. [DOI] [PubMed] [Google Scholar]
- 9.Hughes SL, Williams B, Molina LC, Bayles C, Bryant LL, Harris JR, et al. Characteristics of physical activity programs for older adults: Results of a multisite survey. Gerontologist. 2005;45(5):667–675. doi: 10.1093/geront/45.5.667. [DOI] [PubMed] [Google Scholar]
- 10.Zahuranec DB, Morgenstern LB, Garcia NM, Conley KM, Lisabeth LD, Rank GS, et al. Stroke health and risk education (SHARE) pilot project: Feasibility and need for church-based stroke health promotion in a biethnic community. Stroke. 2008;39(5):1583–1585. doi: 10.1161/STROKEAHA.107.503557. [DOI] [PubMed] [Google Scholar]
- 11.Campbell MK, Resnicow K, Carr C, Wang T, Williams A. Process evaluation of an effective church-based diet intervention: Body & Soul. Health Education & Behavior. 2007;34(6):864–880. doi: 10.1177/1090198106292020. [DOI] [PubMed] [Google Scholar]
- 12.Bopp M, Lattimore D, Wilcox S, Laken M, McClorin L, Swinton R, et al. Understanding physical activity participation in members of an African American church: A qualitative study. Health Education Research. 2007;22(6):815–826. doi: 10.1093/her/cyl149. [DOI] [PubMed] [Google Scholar]
- 13. [Accessed September 7, 2008];Body Worlds (German title: Körperwelten) ( http://en.wikipedia.org/wiki/Body_Worlds#cite_ref-0.
- 14. [Accessed July 9, 2008]; http://biz.yahoo.com/prnews/080429/aqtu508a.html?.v=2.
- 15.Channel M No Smoking Day, March. 12:2008. http://link.brightcove.com/services/link/bcpid1213934526/bctid1454906724.
- 16.MacQueen KM, McLellan E, Kay K, Milstein B. Codebook development for team-based qualitative analysis. Cultural Anthropology Methods. 1998;10(2):31–36. [Google Scholar]
- 17.White KM, Robinson NG, Young RM, Anderson PJ, Hyde MK, Greenbank S, et al. Testing an extended theory of planned behaviour to predict young people’s sun safety in a high risk area. British Journal of Health Psychology. 2008;13(3):435–448. doi: 10.1348/135910707X210004. [DOI] [PubMed] [Google Scholar]
- 18.Sioberg S, Kim K, Reicks M. Applying the theory of planned behavior to fruit and vegetable consumption by older adults. Journal of Nutrition and the Elderly. 2004;23(4):35–46. doi: 10.1300/J052v23n04_03. [DOI] [PubMed] [Google Scholar]
- 19.Prochaska JO, DiClementa CC. Toward a comprehensive model of change. In: Miller WR, Healther N, editors. Treating addictive behaviors: process of change. New York: Plenum Press; 1986. pp. 3–27. [Google Scholar]
- 20.Bunce AE, Griest S, Howarth LC, Beemsterboer P, Perrin N, Cameron WE, Carney PA. Educating youth about research funded by the National Institutes of Health Using a Partnership between an Academic Medical Center and Community-based Science Museum. doi: 10.1007/s10900-009-9150-z. (In Review) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Andrews JO, Bentley G, Crawford S, Pretlow L, Tingen MS. Using community-based participatory research to develop a culturally sensitive smoking cessation intervention with public housing neighborhoods. Ethnicity & Disease. 2007;17(2):331–337. [PubMed] [Google Scholar]
- 22.Pazoki R, Nabipour I, Seyednezami N, Imami SR. Effects of a community-based healthy heart program on increasing healthy women’s physical activity: A randomized controlled trial guided by Community-based Participatory Research (CBPR) BMC Public Health. 2007;7:216. doi: 10.1186/1471-2458-7-216. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Fielden SJ, Rusch ML, Masinda MT, Sands J, Frankish J, Evoy B. Key considerations for logic model development in research partnerships: A Canadian case study. Evaluation & Program Planning. 2007;30(2):115–124. doi: 10.1016/j.evalprogplan.2007.01.002. [DOI] [PubMed] [Google Scholar]
- 24.Moreno-John G, Fleming C, Ford ME, Lichtenberg P, Mangione CM, Perez-Stable EJ, et al. Mentoring in community-based participatory research: the RCMAR experience. Ethnicity & Disease. 2007;17(1 Suppl 1):S33–S43. [PubMed] [Google Scholar]
- 25.Norris KC, Brusuelas R, Jones L, Miranda J, Duru OK, Mangione CM. Partnering with community-based organizations: an academic institution’s evolving perspective. Ethnicity & Disease. 2007;17(1 Suppl 1):S27–S32. [PubMed] [Google Scholar]
- 26.Noe TD, Manson SM, Croy C, McGough H, Henderson JA, Buchwald DS. The influence of community-based participatory research principles on the likelihood of participation in health research in American Indian communities. Ethnicity & Disease. 2007;17(1 Suppl 1):S6–S14. [PubMed] [Google Scholar]
- 27.Chung PJ, Travis R, Jr, Kilpatrick SD, Elliott MN, Lui C, Khandwala SB, et al. Acculturation and parent-adolescent communication about sex in Filipino-American families: A community-based participatory research study. The Journal of Adolescent Health. 2007;40(6):543–550. doi: 10.1016/j.jadohealth.2007.01.004. [DOI] [PubMed] [Google Scholar]
- 28.Boyer BB, Mohatt GV, Pasker RL, Drew EM, McGlone KK. Sharing results from complex disease genetics studies: A community based participatory research approach. International Journal of Circumpolar Health. 2007;66(1):19–30. doi: 10.3402/ijch.v66i1.18221. [DOI] [PubMed] [Google Scholar]
- 29.Mapstone J, Elbourne D, Roberts I. Strategies to improve recruitment to research studies. Cochrane Database of Systematic Reviews. 2007;(2):MR000013. doi: 10.1002/14651858.MR000013.pub3. [DOI] [PubMed] [Google Scholar]