

Overview
Exercise intolerance is the primary symptom of chronic diastolic heart failure. It is part of the definition of heart failure and is intimately linked to its pathophysiology. Further, exercise intolerance affects the diagnosis and prognosis of heart failure. In addition, understanding the mechanisms of exercise intolerance can lead to developing and testing rationale treatments for heart failure. This chapter will focus on the fundamental principles of exercise physiology and the assessment, pathophysiology, and potential treatment of exercise intolerance in diastolic heart failure.
Importance of Exercise Intolerance
Heart failure is defined as a syndrome in which cardiac output is insufficient to meet metabolic demands. This implies that insufficient cardiac output will be expressed symptomatically. Heart failure may often manifest by occasional episodes of acute decompensation with overt systemic volume overload and pulmonary edema.(1;2) However, the primary chronic symptoms in outpatients, even when well compensated and non-edematous, and whether associated with reduced or normal ejection fraction, are exertional fatigue and dyspnea.(3) In addition, these symptoms and other consequences of exercise intolerance are potent determinants of health-related quality of life in heart failure patients. Several investigators have reported that objective measures, and even subjective estimates, of exercise tolerance predictor survival.(4;5)
Exercise intolerance can be objectively quantified using semiquantitative assessments, such as interview (New York Heart Association classification) and surveys (Minnesota Living with Heart Failure or Kansas City Cardiomyopathy questionnaires), and quantitative methods, including timed walking tests (6 minute walk distance) and graded exercise treadmill or bicycle exercise tests. Cardiopulmonary exercise testing on a treadmill or a bicycle ergometer provides the most accurate, reliable, and reproducible assessments of exercise tolerance, and yields multiple important outcomes, including METS, exercise time, exercise workload, blood pressure and heart rate responses, and rate-pressure product. Using commercially available instruments that perform automated expired gas analysis, for both concentration and volume, one can assess at both rest and during exercise, simultaneous measures of oxygen consumption (VO2), carbon dioxide generation, and ventilatory response. Patient effort is an important modifier of data quality, and can itself be assessed simultaneously and objectively by expired gas analysis as the respiratory exchange ratio, and by the somewhat subjective but more easily obtained measures of perceived effort by the Borg scale and percent age-predicted maximal heart rate.
Submaximal exercise is in some ways a more important outcome variable than peak exercise capacity because it is more applicable to everyday life and is relatively effort independent. Submaximal exercise capacity can be assessed as the ventilatory anaerobic threshold by expired gas analysis, using either the Wasserman-Whipp or the V-slope method. Cardiopulmonary exercise testing measurements and expired gas analysis with automated, commercially available instruments provides measure of both peak oxygen consumption and ventilatory anaerobic threshold that are valid and highly reproducible in elderly patients with diastolic as well as systolic heart failure (Figure 1). Another variable provided by these methods, VE/VCO2 slope, is a strong predictor of survival, independent of VO2.(6) We have shown that VE/VCO2 slope is abnormal in patients with DHF, though not as abnormal as in those with systolic heart failure.(7)
Figure 1.

Excellent reproducibility of peak exercise VO2 in older heart failure patients, including those with LV ejection fraction. Group data shown in top panel; representative patient with 15 second averaged data shown in bottom. From Marburger et al, Am J. Cardiol 1998;82:905–909.
Submaximal exercise performance can also be assessed by timed and distance walk tests. These are simple to perform and are widely available. We have shown six-minute walk distance is considerably decreased in elderly patients with DHF. In group data, the reduction is in proportion to both peak exercise oxygen consumption and ventilatory anaerobic threshold. However, our published studies suggest that 6 minute walk testing has only modest accuracy for predicting peak exercise capacity in individual patients compared with direct measurement with cardiopulmonary exercise testing with expired gas analyses, and is also not as reproducible.(8)
Pathophysiology of Exercise Intolerance
In order to understand the pathophysiology of exercise intolerance in DHF, we performed a comparative study of maximal exercise testing with expired gas in 119 older subjects in 3 distinct, well-defined groups: heart failure with severe LV systolic dysfunction (mean EF 30%); isolated diastolic heart failure (EF ≥ 50% and no significant coronary, valvular, pericardial, or pulmonary disease and no anemia); and age-matched controls.(3) In comparison to the controls, peak exercise oxygen consumption (VO2) was severely reduced in the patients with DHF and to a similar degree as those with SHF (Fig. 2).(3) submaximal exercise capacity, as measured by the ventilatory anaerobic threshold, was similarly reduced in DHF vs. SHF patients. This was accompanied by reduced health-related quality of life.(3)
Figure 2.

Exercise oxygen consumption (VO2) during peak exhaustive exercise (left panel) and during submaximal exercise at the ventilatory anaerobic threshold (right panel) in age matched normal subjects (NO), elderly patients with heart failure due to systolic dysfunction (SD), and elderly patients with heart failure with normal systolic function, presumed diastolic dysfunction (DD). Exercise capacity is severely reduced in patients with diastolic heart failure compared to normals (p<0.001) and to a similar degree as in those with systolic heart failure. Overall, peak exercise VO2 was 33% lower in the women compared to the men (not shown). Data from Kitzman DW, Little WC, Brubaker PH, Anderson RT, Hundley WG, Marburger CT et al. Pathophysiological characterization of isolated diastolic heart failure in comparison to systolic heart failure. JAMA 2002; 288(17):2144–2150.
By the Fick equation, peak VO2 during exercise is the product of cardiac output and arteriovenous oxygen (A-VO2) difference, indicating that exercise intolerance will be related to one or both of these factors and to the variables that influence them. Measurement of peak exercise VO2 and at least one of these other 2 factors (cardiac output or arteriovenous oxygen difference) allows one to calculate the remaining unknown factor and begin to isolate specific factors that contribute to exercise intolerance within individual patients and groups.(Figure 3).
Figure 3.

Potential mechanisms of exercise intolerance from the factors of the Fick Equation.
Central cardiac response to exercise
These principles were utilized in order to examine the determinants of exercise performance in normal humans and in patients with heart failure. A series of cardiopulmonary exercise studies was performed using symptom limited upright bicycle exercise with indwelling pulmonary artery and brachial artery catheters, and simultaneous expired gas analysis and radionuclide ventriculography.(9–17) Cardiac output was determined by the Fick principle for oxygen, and left ventricular end-diastolic volume and end-systolic volume were calculated from the Fick stroke volume and the radionuclide ejection fraction (LVEF).
In healthy young and middle-aged male and female volunteers during upright bicycle exercise, VO2 increases 7.7-fold from rest to peak exercise,(9) (14) and this is achieved by a 3.2-fold increase in cardiac output and a 2.5-fold increase in A-V O2 difference. The increase in cardiac output results from a 2.5-fold increase in heart rate and a 1.4-fold increase in stroke volume. Stroke volume increases during low levels of exercise via the Frank-Starling mechanism and during higher levels of exercise, stroke volume increases predominantly due to increased contractility, and may even decline slightly due to tachycardia and limited filling time.
Aging is known to be accompanied by reduced peak exercise VO2 and this is due to an age-related declines in peak exercise cardiac output, heart rate, stroke volume and left ventricular ejection fraction.(10;13) Thus, stroke volume and end diastolic volume response are important contributors to the increase in VO2 and cardiac output during upright exercise in normal subjects and are altered by normal aging but not gender.
This information regarding the physiology of exercise in normal persons and with aging provides background for a series of studies we’ve performed to the understand the cardiovascular and peripheral mechanisms of the reduced exercise capacity in patients with diastolic heart failure. Invasive cardiopulmonary exercise testing was performed in 7 patients with severe but stable chronic heart failure, 6 of whom had had at least one episode of clinically and radiographically documented pulmonary edema.(15) Patients had no significant coronary artery disease angiography, normal left ventricular ejection fraction (≥50%), no wall motion abnormalities, and no evidence of valvular or pericardial disease. Most but not all patients had a history of hypertension and increased LV mass. Ten age-matched and gender-matched healthy volunteers served as normal controls.
The diastolic heart failure patients had marked exercise intolerance and a 48% reduction in peak oxygen consumption. In patients and normal subjects, exercise was limited primarily by leg fatigue, and dyspnea was also frequently reported.(15) The peak respiratory exchange ratio was > 1.10 and similar in patients compared to normal subjects, suggesting good exercise effort in both groups. In both groups, arterial lactate concentration increased several fold from rest to peak exercise and during submaximal exercise at 50 watts where oxygen consumption was similar in patients and normals, lactate concentration tended to be increased in the patients compared to the normal subjects (2.2±1.1 vs. 1.4±0.7 mmol/liter).
At rest, there were no intergroup differences at rest in cardiac output, central A-V O2 difference, stroke volume, or heart rate between the two groups. However, cardiac output was significantly reduced in the patients at submaximal workloads and was severely reduced by 41% at peak exercise (Fig. 4A). Central A-V O2 difference was increased by approximately 10% in the patients during the submaximal exercise, partially compensating for the reduced cardiac index (Fig. 4B). However, at peak exercise, this mechanism was outstripped, and A-V O2 difference was reduced by 13%. In the patients, the change in cardiac output from rest to peak exercise correlated closely with the increase in VO2 during exercise (r=0.81, P<0.03).
Figure 4.

Cardiovascular function assessed by invasive cardiopulmonary exercise testing in patients with heart failure and normal systolic function (open boxes) and age-matched normals (closed boxes). The primary components of the Fick equation for oxygen consumption, cardiac output and arteriovenous oxygen difference, are shown in panels A and B, respectively. The components of cardiac output, stroke volume and heart rate, are shown in panels C and D. The X-axis is exercise workload in kpm/min; 150 kpm/min is equivalent to 25 watts. From Kitzman DW, Higginbotham MB, Cobb FR, Sheikh KH, Sullivan M. Exercise intolerance in patients with heart failure and preserved left ventricular systolic function: failure of the Frank-Starling mechanism. J Am Coll Cardiol 1991; 17:1065–1072.
Stroke volume was reduced in the patients during submaximal exercise and was markedly reduced (−26%) at peak exercise.(Fig. 4C)(15) Likewise, heart rate was reduced by 18% in patients compared to controls at peak exercise (Fig. 4D). The change in stroke volume correlated well with the increase in cardiac output during exercise, suggesting that in the diastolic heart failure patients, reduced stroke volume was the primary factor for reduced cardiac output and the 48% reduction in peak VO2.
There are a number of possible factors that could contribute to the abnormal stroke volume response in the patients, and these are shown in Figures 5A–D. The left ventricular ejection fraction and end-systolic volume index during rest and exercise were not different from the normal subjects (Fig. 5A and 5B), confirming that systolic function was within normal limits (Fig. 5B). End-diastolic volume, in contrast, was reduced markedly during exercise, resulting in a flattened curve that was similar to the abnormal stroke volume response (Fig. 5C). In the patients, the change in end-diastolic volume from rest to peak exercise correlated strongly with the change in stroke volume and in cardiac output.(15)
Figure 5.
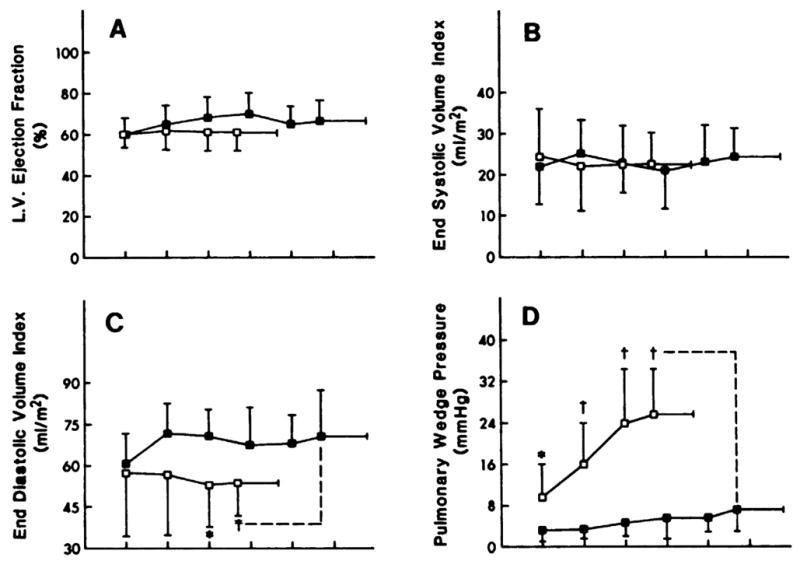
The components of the LV stroke volume response during exercise, LV ejection fraction, end-systolic volume, end-diastolic volume, and LV filling pressure, are shown in panels A–D. Not shown are systolic and mean arterial pressure, which was not different between groups. Key is same as for Figure 4. From Kitzman DW, Higginbotham MB, Cobb FR, Sheikh KH, Sullivan M. Exercise intolerance in patients with heart failure and preserved left ventricular systolic function: failure of the Frank-Starling mechanism. J Am Coll Cardiol 1991; 17:1065–1072.
Pulmonary wedge pressure as an estimate of LV filling pressure was mildly increased in the patients at rest and became severely increased during exercise (Fig. 5D). Notably, however, the change in pulmonary wedge pressure from rest to peak exercise did not correlate significantly with the change in stroke volume or the increase in VO2 during exercise. The left ventricular end-diastolic pressure-volume ratio tended to be elevated in the patients at rest and during exercise became markedly increased. The upward, left-shifted left ventricular diastolic pressure-volume relationship in the DHF patients is shown in Figure 6 (15) and indicates that the patients did not utilize the Frank-Starling mechanism, likely primarily due to diastolic LV dysfunction. This is in contrast to patients with heart failure and reduced systolic function who have an operating pressure volume relationship that is shifted upward and to the right during exercise.(18)
Figure 6.
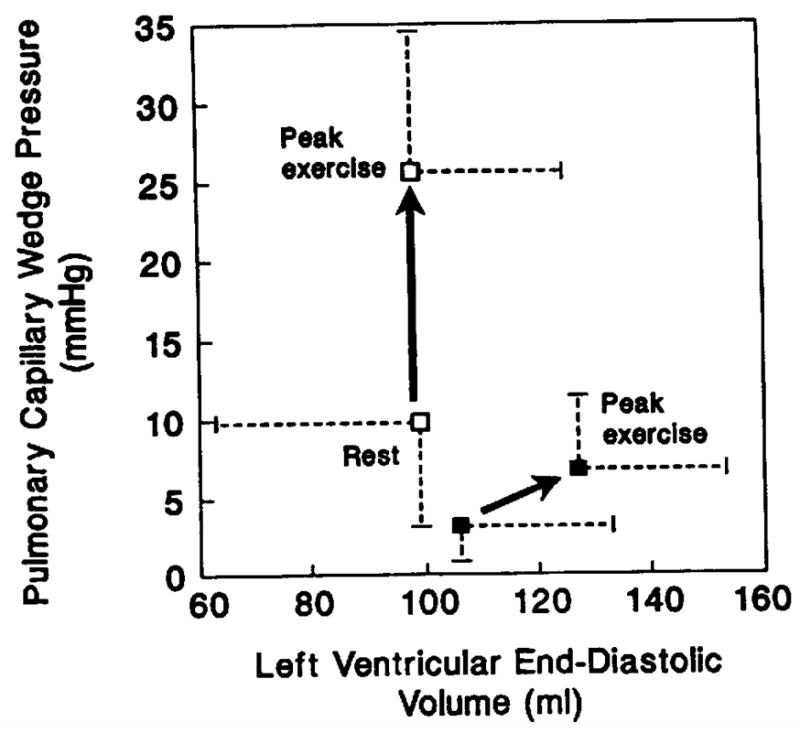
LV diastolic function assessed by invasive cardiopulmonary exercise testing. Key is the same as for Figure 4. The pressure-volume relation was shifted upward and leftward at rest. In the patients with exercise, LV diastolic volume did not increase despite marked increase in diastolic (pulmonary wedge) pressure. Due to diastolic dysfunction, failure of the Frank-Starling mechanism resulted in severe exercise intolerance. From Kitzman DW, Higginbotham MB, Cobb FR, Sheikh KH, Sullivan M. Exercise intolerance in patients with heart failure and preserved left ventricular systolic function: failure of the Frank-Starling mechanism. J Am Coll Cardiol 1991; 17:1065–1072.
Although these invasively assessed left ventricular filling pressures offers key insights into exercise intolerance, their invasive nature limits their overall utility. Noninvasive Doppler mitral filling indices can give insight to LV diastolic function, particularly the more recently developed tissue Doppler indices. The time constant of isovolumic pressure decline (τ) can be estimated non-invasively by measuring the early diastolic velocity of the mitral annulus (E′).(19) Furthermore, the ratio of early left ventricular diastolic filling velocity (E) to E′ correlates well with invasively measured left ventricular end diastolic pressures.(20) Notably, an increased E/E′ ratio at rest has been correlated with maximal and submaximal exercise intolerance.(21;22) In addition, an increase in E/E′ during exercise correlates with exercise intolerance.(23)
Comparison of the exercise cardiovascular responses in the 2 different groups of heart failure patients (those with normal ejection fractions (15) and those with reduced ejection fractions(11;13;15)) can be instructive. Both had severe exertional symptoms and objective evidence of exercise intolerance, as well as markedly reduced peak cardiac output and stroke volume, mildly reduced peak heart rate, and slightly reduced peak A-V O2 difference (Figure 7). Both groups also had mildly increased resting and markedly elevated exercise mean pulmonary capillary wedge pressures. However, the means by which LV stroke volume was reduced differed. In one group,(11;13) patients had profound systolic contractile dysfunction and were able to utilize markedly increased LV filling pressure to produce greater than normal use of the Frank-Starling mechanism to partially compensate and maintain an increase in exercise stroke volume. In the other group, despite normal systolic contractile function and markedly increased LV filling pressure,(15) patients had an inability to use the Frank-Starling mechanism to increase stroke volume during exercise.(Figure 7).(24)
Figure 7.

Comparison of characteristic central and peripheral cardiovascular response to exercise in patients with heart failure associated with severe LV systolic dysfunction versus normal LV ejection fraction. See text for discussion.
Heart rate response to exercise
Decreased heart rate response also contributes to the reduced peak exercise cardiac output and thence reduced peak exercise VO2. Indeed, chronotropic incompetence has been a frequent finding during cardiopulmonary exercise studies in systolic heart failure. However, there had been no information available in older patients and particularly those with normal ejection fraction. Therefore, we examined heart rate and expired gas analyses responses in elderly DHF patients in comparison to a group of age and gender matched SHF patients and healthy normal controls. Utilizing the most standard definition of chronotropic incompetence, we found that this was present in 20–25% of older heart failure patients, that the prevalence was similar in DHF compared to SHF, and that the presence of chronotropic incompetence was a significantly contributor to the degree of exercise intolerance, measured as maximal oxygen consumption, and that this was independent of medications, including beta-adrenergic antagonists (Fig. 8).(25) The important contribution of chronotropic incompetence to exercise intolerance in patients with DHF was confirmed by Borlaug et al. studied a cohort of primarily elderly, African American women with hypertension and heart failure with a preserved ejection fraction. The reported significant reductions in the rate of heart rate increase during exercise which was a primary contributor to reduced peak cardiac index and maximal exercise oxygen consumption (Fig. 9).(26) The implication of this finding may merits further investigation, and has therapeutic implications.
Figure 8.
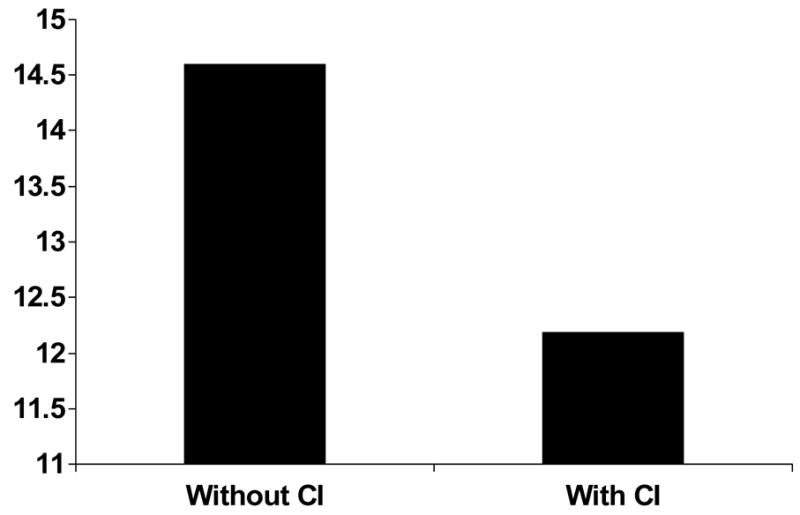
Peak exercise oxygen consumption (y-axis, in ml/kg/min) in heart failure patients with and without chronotropic incompetence (CI). Those with chronotropic incompetence have more severe exercise intolernace, suggesting a contributory role for CI. Adapted from Brubaker et al, J Cardiopulm Rehab, 2006;26:86–89.
Figure 9.
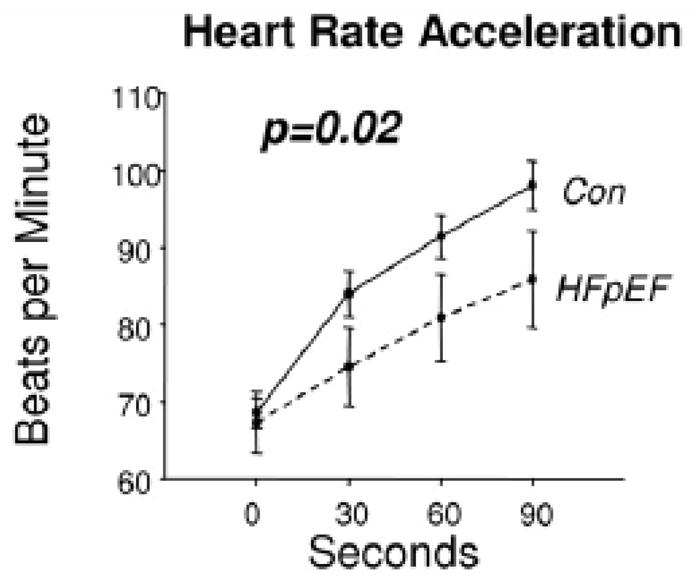
Heart rate acceleration during exercise in controls (CON) and patients with heart failure and preserved ejection fraction (HFPEF). From Kass et al; Circulation 2006;114:2138–2147.
Central and peripheral vascular contributions to exercise intolerance
Abnormal afterload and abnormal ventricular-vascular coupling may contribute to the abnormal Frank-Starling response seen in the diastolic heart failure patients. Nearly all (88%) of such patients have a history of chronic systemic hypertension.(27;28;28;29) In animal models, diastolic dysfunction develops early in systemic hypertension, and LV diastolic relaxation is sensitive to increased afterload, (30;31;31;32;32–35) which can impair relaxation, leading to increased LV filling pressures, decreased stroke volume, and could lead to symptoms of dyspnea and congestion.(1;2;33)
In animal models and humans, chronic systolic hypertension accelerates and magnifies the age-related increase in fibrotic thickening of the aortic wall and resultant increase in aortic stiffness, which is a major determinant of LV afterload and ventricular-vascular coupling.(36;37) To determine whether abnormally decreased aortic distensibility contributes to the severe exercise intolerance in heart failure with normal EF we performed magnetic resonance imaging and maximal exercise testing with expired gas analysis in a group of elderly patients with isolated DHF, as defined above, and in young healthy subjects and age-matched healthy subjects as normal controls. The patients with DHF had severe exercise intolerance, and this was associated with increased pulse pressure and concentric hypertrophic LV remodeling. Thoracic aortic wall thickness was increased 50% and there was markedly decreased aortic distensibility (Fig. 10). In univariate analysis, decreased aortic distensibility correlated closely with their severely decreased peak exercise oxygen consumption (Fig. 11).(38) In multivariate analysis, decreased aortic distensibility was the strongest independent predictor of reduced exercise capacity. These data support a potentially important role of increased aortic stiffness, due to underlying aging and amplified by chronic hypertension, in the pathophysiology of chronic heart failure symptoms. (39)
Figure 10.

Data and images from representative subjects from healthy young, healthy elderly, and elderly patients with diastolic heart failure. Maximal exercise oxygen consumption (V02max), aortic distensibility at rest, and left ventricular mass:volume ratio. Patients with diastolic heart failure have severely reduced exercise tolerance (V02max) and aortic distensibility and increased aortic wall thickness. Adapted from Hundley WG, Kitzman DW, Morgan TM, Hamilton CA, Darty S.N., Stewart KP et al. Cardiac cycle dependent changes in aortic area and aortic distensibility are reduced in older patients with isolated diastolic heart failure and correlate with exercise intolerance. J Am Coll Cardiol 2001; 38(3):796–802.
Figure 11.

There is a close relationship between peak exercise VO2 (horizontal axis) and proximal aortic distensibility (vertical axis) in a group of 30 subjects (10 healthy young, 10 healthy old, and 10 elderly DHF patients). Each symbol represents the data from 1 participant. From Hundley WG, Kitzman DW, Morgan TM, Hamilton CA, Darty S.N., Stewart KP et al. Cardiac cycle dependent changes in aortic area and aortic distensibility are reduced in older patients with isolated diastolic heart failure and correlate with exercise intolerance. J Am Coll Cardiol 2001; 38(3):796–802.
Peripheral arteries must dilate early during exercise in order to accommodate and facilitate the conveyance of increased nutritive blood flow to working skeletal muscle. Multiple lines of evidence suggest that in patients with systolic heart failure, this response is impaired, and contributes to exercise intolerance, and that this is modifiable with exercise training and other interventions.(40–43) We examined the flow-mediated arterial dilation (FMAD) response to ischemia induced but 3–5 minute cuff inflation in the femoral artery in elderly patients with DHF, patients with SHF, and normal age-matched controls using phase contrast magnetic imaging. We also performed cardiopulmonary exercise testing with expired gas analysis.(44) The latter again demonstrated severe exercise intolerance in the patients with DHF that was similar in degree to patients with SHF. The patients with SHF had severely reduced femoral FMAD compared to normal subjects. However, in DHF patients, FMAD was relatively preserved, and not significantly different from normals (Fig. 12). Thus, we concluded that abnormal FMAD was not present in DHF and was not a significant contributor to the severe exercise intolerance in these patients.
Figure 12.

Flow mediated arterial dilation (FMAD) of the femoral artery by phase contrast magnetic resonance imaging in normal subjects, elderly patients with heart failure and normal ejection fraction (HFNEF) and patients with heart failure and reduced ejection fraction (HFREF). FMAD is severely reduced in HFREF but is relatively preserved in HFNEF compared to age matched healthy normal subjects. From Hundley WG, Bayram E, Hamilton CA, Hamilton EA, Morgan TM, Darty SN et al. Leg flow-mediated arterial dilation in elderly patients with heart failure and normal left ventricular ejection fraction. Am J Physiol Heart Circ Physiol 2007; 292(3):H1427–H1434.
Primary cause of symptoms of exercise intolerance; skeletal muscle; other factors
Despite the many exercise physiological studies that have been performed in heart failure patients, there remains uncertainty regarding the final stimulus that causes heart failure patients to stop exercising at lower workloads than healthy subjects.(45–48) It had been thought that increased exercise pulmonary wedge pressure and stimulation of pulmonary J-receptors cause reflex hyperventilation and hypoxia leading to the sensation of severe dyspnea, causing the patient to stop exercise prematurely. However, about 50% of heart failure patients, whether systolic or diastolic, discontinue exercise primarily due to general fatigue or leg fatigue rather than dyspnea. In addition, investigators (16;49) have demonstrated that arterial hypoxia does not occur during exercise in heart failure patients, and that excess ventilation is related to pulmonary hypoperfusion and reduced cardiac output rather than elevated LV filling pressures. Furthermore, exercise intolerance, as measured objectively by peak oxygen consumption, is unrelated to invasively measure pulmonary capillary wedge pressures, including in patients with DHF.(15) The decreased exercise cardiac output likely causes skeletal muscle hypoperfusion, a potent stimulus for early anaerobic metabolism, and subsequent generation of muscle lactate and other metabolites which could produce the sensation of peripheral and central fatigue.(50;51) Indeed, in the studies where lactate production during exercise has been reported, it has been abnormal compared to normals.(3;15)
Based on the extensive experience in seeking to understand exercise intolerance in patients with systolic heart failure, it is likely that several factors in addition to those discussed above may contribute to exercise intolerance in patients with DHF, including: anemia (which is highly prevalent in DHF as it is in SHF),(52) and skeletal muscle bulk, fiber type, and function. (11;42;53–61) There have been particularly compelling findings regarding skeletal muscle in SHF.(11;56;62–73) Despite this, there has been no information regarding skeletal muscle in DHF. This could be even more relevant in DHF given increasing data regarding the role of skeletal muscle atrophy and dysfunction in older patients with a variety of disabling chronic syndromes, this appears a particularly promising area for future investigation.(74–78) In addition, the degree of adipose between skeletal muscle bundles appears to be a potential modifier of skeletal muscle function and exercise capacity as well. This will likely be a fruitful area for future research, particularly since skeletal muscle bulk and function appear potentially modifiable through nutrition and exercise interventions.(79)
Interventions to Improve Exercise Tolerance
During exercise in normal subjects, systolic and pulse pressure increase substantially, and this response is magnified by increased arterial stiffness. Data from animal models suggest that the exercise related increase in systolic blood pressure is mediated, in part, by exercise-induced increases in circulating angiotensin-II. Indeed, in a randomized, double-blind, placebo-controlled cross-over trial, angiotensin receptor blockade reduced the exaggerated exercise increase in systolic and pulse pressures, resulting in significantly improved exercise treadmill time and quality of life (Fig. 13). (80)
Figure 13.

Plots of peak systolic blood pressure and exercise duration during baseline, during placebo, and during losartan in a randomized, controlled, cross-over trial. Treatment with the angiotensin-II antagonist losartan increased exercise time. From Warner JG, Metzger C, Kitzman DW, Wesley DJ, Little WC. Losartan improves exercise tolerance in patients with diastolic dysfunction and a hypertensive response to exercise. J Am Coll Cardiol 1999; 33:1567–1572.
Aronow et al showed in a group of NYHA class III HF patients and presumed diastolic dysfunction (EF >50%) that the ACE inhibitor enalapril significantly improved functional class, exercise duration, ejection fraction, diastolic filling, and left ventricular mass.(81)
In hypertrophic cardiomyopathy, a disorder in which diastolic dysfunction is common, verapamil appears to improve symptoms and objectively measured exercise capacity.(82–85) This agent also improves ventricular vascular coupling and exercise performance in aged individuals with hypertension.(86) In laboratory animal models calcium antagonists, particularly dihydropyridines, prevent ischemia-induced increases in LV diastolic stiffness(87) and in improve diastolic performance in pacing-induced HF.(88–90) However, negative inotropic calcium antagonists significantly impair early relaxation, (90–94) and have in general shown a tendency toward adverse outcome in patients with systolic HF.(90) Despite this, Setaro examined 22 men (mean age 65) with clinical HF despite ejection fraction >45% in a randomized, double-blind, placebo-controlled crossover trial of verapamil.(95) There was a 33% improvement in exercise time and significant improvements in clinicoradiographic HF scoring and peak filling rate.
Little et al compared the calcium channel antagonist verapamil in a randomized, cross-over, blinded trial to the angiotensin receptor antagonist candesartan with the outcomes of peak exercise blood pressure, exercise time and quality of life.(96) While both agents blunted the peak systolic blood pressure response to exercise, only candesartan, and not verapamil, improved exercise time and quality of life.(96)
A subsequent trial with similar randomized, cross-over, blinded design, the diuretic hydrochlorothiazide was compared with the angiotensin receptor antagonist losartan on the outcomes of peak exercise blood pressure, exercise time and quality of life.(97) While both agents blunted the peak systolic blood pressure response to exercise, only losartan, but not hydrochlorothiazide, improved exercise time and quality of life.(97)
The addition of low dose spironolactone (12.5–50 mg daily) to standard therapy has been shown to improve exercise tolerance in patients with severe SHF. Aldosterone antagonism has numerous potential benefits in patients with DHF, including LV remodeling, reversal of myocardial fibrosis, and improved LV diastolic function and vascular function.(98–100) However few data are presently available regarding aldosterone antagonism in DHF. In one small study, low dose spironolactone was well tolerated and appeared to improve exercise capacity and quality of life in older women with isolated DHF.(101) In another, spironolactone improved measures of myocardial function in hypertensive patients with diastolic heart failure.(102)
Glucose cross-links increase with aging and diabetes, and cause increased vascular and myocardial stiffness. Alagebrium, a novel cross-link breaker, improved vascular and LV stiffness in dogs. In a small, open label, 4-month trial of this agent in elderly patients, LV mass, quality of life, and tissue Doppler diastolic function indexes improved,(Fig. 14) but there were no significant improvements in exercise capacity or aortic distensibility, the primary outcomes of the trial.(103) A variety of other agents and strategies are currently being evaluated or under consideration for this syndrome, including a selective endothelin antagonist.
Figure 14.
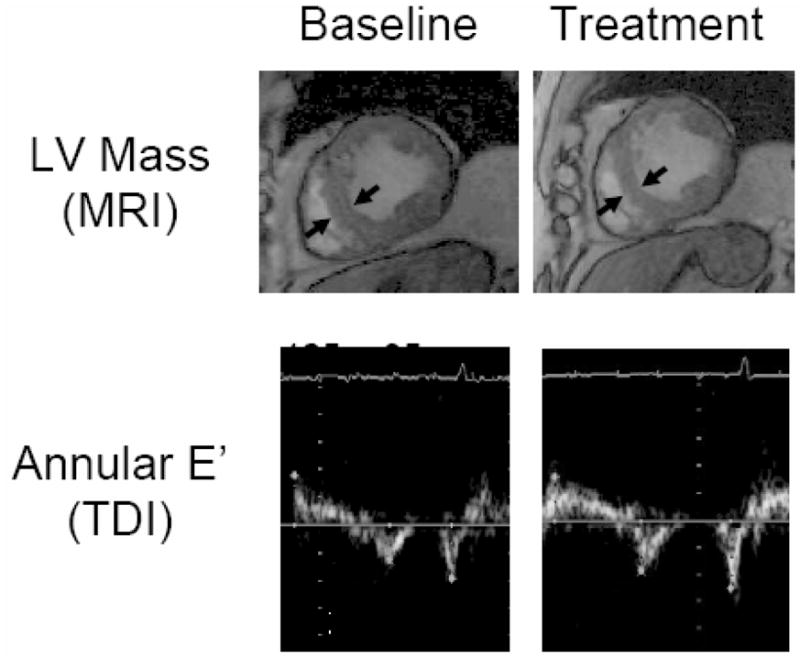
Effect of alegebrium on left ventricular mass (top panel) and tissue Doppler early diastolic velocity at the mitral annulus in older patients with diastolic heart failure. From Little WC, Zile MR, Kitzman DW, Hundley WG, O’Brien T.X., deGroof RC. The Effect of Alagebrium Chloride (ALT-711), a Novel Glucose Cross-Link Breaker, in the Treatment of Elderly Patients with Diastolic Heart Failure. J Card Fail 2005 5 A.D.; 11(3):191–195.
The substantial chronotropic incompetence seen in DHF patients and its correlation with reduced exercise capacity described above provides a rationale for electronic pacing interventions to improve exercise capacity. Indeed, one modest sized single-center study used such a strategy in selected patients with hypertensive left ventricular hypertrophy with supranormal systolic ejection and distal cavity obliteration who had debilitating exertional fatigue and dyspnea and demonstrated substantially improved exercise performance.(104) These data merit confirmation in larger, multicenter randomized controlled trials.
Thus, a variety of pharmacological and other interventions in small studies have shown improvements in exercise tolerance with verapamil,(95) enalapril,(81) angiotensin receceptor antagonism (80;96), and aldosterone antagonism.(101) It should be remembered that in patients with systolic heart failure, some types of pharmacological interventions that improve exercise tolerance have had paradoxical effects on long-term survival.(105;106) Because of this, VE/VCO2 slope during exercise, which is a powerful predictor of survival independent of VO2, should be included in future intervention trials of exercise tolerance.(6)
Aerobic exercise training has the potential to improve a variety of key abnormalities in patients with heart failure and normal ejection fraction, including LV diastolic compliance, aortic distensibility, blood pressure, and skeletal muscle function.(72;107;108) Indeed, in systolic heart failure, aerobic exercise training has been shown to improve exercise tolerance, likely via favorable effects on multiple factors.(17;109;110) A recent report indicates that LV diastolic compliance is preserved in older masters athletes compared to their age matched and young counterparts, suggesting that exercise training may be beneficial in diastolic heart failure as well.(111) A preliminary report indicates that exercise training improves exercise tolerance and quality of life in older patients with heart failure and normal ejection fraction.(112) A recent report from a clinical exercise rehabilitation program suggests that exercise training may also benefit patients with DHF.(113) Although the role of exercise training in the clinical management of this syndrome remains to be defined, as is the accepted practice in systolic heart failure, it would seem prudent to recommend regular, moderate physical activity as tolerated. The effect of exercise training on survival in systolic heart failure patients is being examined in a large, NIH-sponsored, multicenter, randomized, controlled trial (HF-ACTION). Presently, there is no trial examining mortality and exercise training in patients with heart failure and normal ejection fraction.
Conclusion
Even when stable and non-edematous, patients with heart failure and normal ejection fraction have severe, chronic exercise intolerance. The pathophysiology of exercise intolerance in this syndrome is incompletely understood, but is likely multifactorial. Presently available data suggest that important contributors include decreased LV diastolic compliance, decreased aortic distensibility, exaggerated exercise systolic blood pressure, relative chronotropic incompetence, and possibly anemia and skeletal muscle remodeling. Because it is a primary determinant of quality of life, can be quantified objectively, is reproducible, and is modifiable, exercise intolerance is an attractive therapeutic target. A number of pharmacological and other interventions appear to improve exercise intolerance in DHF. Although it is unknown whether these will be accompanied by improved survival, the parallel outcomes of improved quality of life support the clinical relevance of exercise performance outcomes.
Acknowledgments
Supported in part by National Institute on Aging Grants, R37-AG18915 (MERIT), Dennis Jahnigen Career Development and Paul Beeson Award (K08-AG026764) and Claude D. Pepper Older Americans Independence Center (P30 AG21332)
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Reference List
- 1.Gandhi SK, Powers JE, Fowle KM, Rankin KM, Nomeir AM, Kitzman DW, et al. The Pathogenesis of Acute Pulmonary Edema Associated with Hypertension. N Engl J Med. 2000;344(1):17–22. doi: 10.1056/NEJM200101043440103. [DOI] [PubMed] [Google Scholar]
- 2.Powers JE, Gandhi SK, Kramer RK, Fowle KM, Kitzman DW, Little WC. Predictors of Poor Outcome in Patients with Hypertensive Pulmonary Edema. J Am Coll Cardiol. 2004;43(5A):227A. [Google Scholar]
- 3.Kitzman DW, Little WC, Brubaker PH, Anderson RT, Hundley WG, Marburger CT, et al. Pathophysiological characterization of isolated diastolic heart failure in comparison to systolic heart failure. JAMA. 2002;288(17):2144–2150. doi: 10.1001/jama.288.17.2144. [DOI] [PubMed] [Google Scholar]
- 4.Bol E, de Vries WR, Mosterd WL, Wielenga RP, Coats A. Cardiopulmonary exercise parameters in relation to all-cause mortality in patients with chronic heart failure. Int J Cardiol. 2000;72:255–263. doi: 10.1016/s0167-5273(99)00195-3. [DOI] [PubMed] [Google Scholar]
- 5.Jones RC, Francis GS, Lauer MS. Predictors of mortality in patients with heart failure and preserved systolic function in the Digitalis Investigation Group trial. J Am Coll Cardiol. 2004;44(5):1025–1029. doi: 10.1016/j.jacc.2004.05.077. [DOI] [PubMed] [Google Scholar]
- 6.Francis DP, Shamin W, Davies LC, Piepoli M, Ponikowski P, Anker SD, et al. Cardiopulmonary exercise testing for prognosis in chronic heart failure: continuous and independent prognostic value from VE/VCO2 slope and peak VO2. Eur Heart J. 2000;21:154–161. doi: 10.1053/euhj.1999.1863. [DOI] [PubMed] [Google Scholar]
- 7.Moore B, Brubaker PH, Stewart KP, Kitzman DW. VE/VCO2 Slope in Older Heart Failure Patients With Normal Versus Reduced Ejection Fraction Compared With Age-Matched Healthy Controls. Journal of Cardiac Failure. 2007;13(4):259–262. doi: 10.1016/j.cardfail.2006.12.005. [DOI] [PubMed] [Google Scholar]
- 8.Maldonado-Martin S, Brubaker PH, Kaminsky LA, Moore JB, Stewart KP, Kitzman DW. The relationship of a 6-min walk to VO(2 peak) and VT in older heart failure patients. Med Sci Sports Exerc. 2006;38(6):1047–1053. doi: 10.1249/01.mss.0000222830.41735.14. [DOI] [PubMed] [Google Scholar]
- 9.Higginbotham MB, Morris KG, Williams RS, McHale PA, Coleman RD, Cobb FR. Regulation of stroke volume during submaximal and maximal upright exercise in normal man. Circ Res. 1986;58:281–291. doi: 10.1161/01.res.58.2.281. [DOI] [PubMed] [Google Scholar]
- 10.Higginbotham MB, Morris KG, Williams RS, et al. Physiologic basis for the age-related decline in aerobic work capacity. Am J Cardiol. 1986;57:1374–1379. doi: 10.1016/0002-9149(86)90221-3. [DOI] [PubMed] [Google Scholar]
- 11.Sullivan M, Knight JD, Higginbotham MB, Cobb FR. Relation between central and peripheral hemodynamics during exercise in patients with chronic heart failure: muscle blood flow is reduced with maintenance of arterial perfusion pressure. Circulation. 1989;80:769–781. doi: 10.1161/01.cir.80.4.769. [DOI] [PubMed] [Google Scholar]
- 12.Higginbotham MB, Sullivan M, Coleman RE, Cobb FR. Regulation of stroke volume during exercise in patients with severe left ventricular dysfunction: importance of Starling mechanism. J Am Coll Cardiol. 1987;9:58A. [Google Scholar]
- 13.Kitzman DW, Sullivan M, Cobb FR, Higginbotham MB. Exercise cardiac output declines with advancing age in normal subjects. J Am Coll Cardiol. 1989;13(2):241A. [Google Scholar]
- 14.Sullivan M, Cobb FR, Knight JD, Higginbotham MB. Stroke volume increases by similar mechanisms in men and women. Am J Cardiol. 1991;67:1405–1412. doi: 10.1016/0002-9149(91)90472-w. [DOI] [PubMed] [Google Scholar]
- 15.Kitzman DW, Higginbotham MB, Cobb FR, Sheikh KH, Sullivan M. Exercise intolerance in patients with heart failure and preserved left ventricular systolic function: failure of the Frank-Starling mechanism. J Am Coll Cardiol. 1991;17:1065–1072. doi: 10.1016/0735-1097(91)90832-t. [DOI] [PubMed] [Google Scholar]
- 16.Sullivan M, Higginbotham MB, Cobb FR. Increased exercise ventilation in patients with chronic heart failure: intact ventilatory control despite hemodynamic and pulmonary abnormalities. Circulation. 1988;77:552–559. doi: 10.1161/01.cir.77.3.552. [DOI] [PubMed] [Google Scholar]
- 17.Sullivan M, Higginbotham MB, Cobb FR. Exercise training in patients with chronic heart failure delays ventilatory anaerobic threshold and improves submaximal exercise performance. Circulation. 1989;79:324–329. doi: 10.1161/01.cir.79.2.324. [DOI] [PubMed] [Google Scholar]
- 18.Sullivan M, Cobb FR. Central hemodynamic response to exercise in patients with chronic heart failure. Chest. 1992;101:340S–346S. doi: 10.1378/chest.101.5_supplement.340s. [DOI] [PubMed] [Google Scholar]
- 19.Nagueh SF, Middleton KJ, Kopelen HA, Zoghbi WA, Quinones MA. Doppler tissue imaging: a noninvasive technique for evaluation of left ventricular relaxation and estimation of filling pressures. J Am Coll Cardiol. 1997;30(6):1527–1533. doi: 10.1016/s0735-1097(97)00344-6. [DOI] [PubMed] [Google Scholar]
- 20.Ommen SR, Nishimura RA, Appleton CP, Miller FA, Oh JK, Redfield MM, et al. Clinical utility of Doppler echocardiography and tissue Doppler imaging in the estimation of left ventricular filling pressures: A comparative simultaneous Doppler-catheterization study. Circulation. 2000;102(15):1788–1794. doi: 10.1161/01.cir.102.15.1788. [DOI] [PubMed] [Google Scholar]
- 21.Hadano Y, Murata K, Yamamoto T, Kunichika H, Matsumoto T, Akagawa E, et al. Usefulness of Mitral Annular Velocity in Predicting Exercise Tolerance in Patients With Impaired Left Ventricular Systolic Function. The American Journal of Cardiology. 2006;97(7):1025–1028. doi: 10.1016/j.amjcard.2005.10.044. [DOI] [PubMed] [Google Scholar]
- 22.Skaluba SJ, Litwin SE. Mechanisms of Exercise Intolerance: Insights From Tissue Doppler Imaging. Circulation. 2004;109(8):972–977. doi: 10.1161/01.CIR.0000117405.74491.D2. [DOI] [PubMed] [Google Scholar]
- 23.Ha JW, Oh JK, Pellikka PA, Ommen SR, Stussy VL, Bailey KR, et al. Diastolic stress echocardiography: A novel noninvasive diagnostic test for diastolic dysfunction using supine bicycle exercise Doppler echocardiography. Journal of the American Society of Echocardiography. 2005;18(1):63–68. doi: 10.1016/j.echo.2004.08.033. [DOI] [PubMed] [Google Scholar]
- 24.Kitzman DW, Sullivan M. Exercise intolerance in patients with heart failure: Role of diastolic dysfunction. In: Grossman W, editor. Diastolic Relaxation of the Heart. Boston: Kluwer Academic Publishers; 1994. pp. 295–302. [Google Scholar]
- 25.Brubaker PH, Joo KC, Stewart KP, Fray B, Moore B, Kitzman DW. Chronotropic incompetence and its contribution to exercise intolerance in older heart failure patients. J Cardiopulm Rehabil. 2006;26(2):86–89. doi: 10.1097/00008483-200603000-00007. [DOI] [PubMed] [Google Scholar]
- 26.Borlaug BA, Melenovsky V, Russell SD, Kessler K, Pacak K, Becker LC, et al. Impaired Chronotropic and Vasodilator Reserves Limit Exercise Capacity in Patients With Heart Failure and a Preserved Ejection Fraction. Circulation. 2006;114(20):2138–2147. doi: 10.1161/CIRCULATIONAHA.106.632745. [DOI] [PubMed] [Google Scholar]
- 27.Kitzman DW, Gardin JM, Gottdiener JS, Arnold AM, Boineau R, Aurigemma GP, et al. Importance of heart failure with preserved systolic function in patients > or = 65 Years of Age. CHS Research Group. Cardiovascular Health Study. Am J Cardiol. 2001;87(4):413–419. doi: 10.1016/s0002-9149(00)01393-x. [DOI] [PubMed] [Google Scholar]
- 28.Iriarte M, Murga N, Morillas M, Salcedo A, Etxebeste J. Congestive heart failure from left ventricular diastolic dysfunction in systemic hypertension. Am J Cardiol. 1993;71:308–312. doi: 10.1016/0002-9149(93)90796-f. [DOI] [PubMed] [Google Scholar]
- 29.Iriarte MM, Perez OJ, Sagastagoitia D, Molinero E, Murga N. Congestive heart failure due to hypertensive ventricular diastolic dysfunction. Am J Cardiol. 1995;76(13):43D–47D. doi: 10.1016/s0002-9149(99)80491-3. [DOI] [PubMed] [Google Scholar]
- 30.Little WC. Enhanced load dependence of relaxation in heart failure: clinical implications. Circulation. 1992;85(6):2326–2328. doi: 10.1161/01.cir.85.6.2326. [DOI] [PubMed] [Google Scholar]
- 31.Gelpi RJ. Changes in diastolic cardiac function in developing and stable perinephritic hypertension in conscious dogs. Circ Res. 1991;68:555–567. doi: 10.1161/01.res.68.2.555. [DOI] [PubMed] [Google Scholar]
- 32.Shannon RP, Komamura K, Gelpi RJ, Vatner SF. Altered load: an important component of impaired diastolic function in hypertension and heart failure. In: Lorell BH, Grossman W, editors. Diastolic Relaxation of the Heart. Norwell, Massachusetts: Kluwer Academic Publishers; 1994. pp. 177–185. [Google Scholar]
- 33.Little WC, Braunwald E. Assessment of cardiac performance. In: Braunwald E, editor. Heart Disease. Philadelphia: W.B. Saunders Company; 1999. [Google Scholar]
- 34.Hoit BD, Walsh RA. Diastolic dysfunction in hypertensive heart disease. In: Gaasch WH, LeWinter MM, editors. Left ventricular diastolic dysfunction and heart failure. Philadelphia: Lea & Febiger; 1994. pp. 354–372. [Google Scholar]
- 35.Little WC, Ohno M, Kitzman DW, Thomas JD, Cheng CP. Determination of left ventricular chamber stiffness from the time for deceleration of early left ventricular filling. Circulation. 1995;92:1933–1939. doi: 10.1161/01.cir.92.7.1933. [DOI] [PubMed] [Google Scholar]
- 36.Lakatta E. Cardiovascular aging research: The next horizons. J Am Geriatr Soc. 1999;47:613–625. doi: 10.1111/j.1532-5415.1999.tb02579.x. [DOI] [PubMed] [Google Scholar]
- 37.Lakatta EG, Levy D. Arterial and cardiac aging: major shareholders in cardiovascular disease enterprises: Part I: aging arteries: a “set up” for vascular disease. Circulation. 2003;107(1):139–146. doi: 10.1161/01.cir.0000048892.83521.58. [DOI] [PubMed] [Google Scholar]
- 38.Hundley WG, Kitzman DW, Morgan TM, Hamilton CA, Darty SN, Stewart KP, et al. Cardiac cycle dependent changes in aortic area and aortic distensibility are reduced in older patients with isolated diastolic heart failure and correlate with exercise intolerance. J Am Coll Cardiol. 2001;38(3):796–802. doi: 10.1016/s0735-1097(01)01447-4. [DOI] [PubMed] [Google Scholar]
- 39.Rerkpattanapipat P, Hundley WG, Link KM, Brubaker PH, Hamilton CA, Darty SN, et al. Relation of Aortic Distensibility Determine by Magnetic Resonance Imaging in patients =60 Years of Age to Systolic Heart Failure and Exercise Capacity. Am J Cardiol. 2002;90(11):1221–1225. doi: 10.1016/s0002-9149(02)02838-2. [DOI] [PubMed] [Google Scholar]
- 40.Drexler H, Hayoz D, Monzel T, Hornig B, Just H, Brunner HR, et al. Endothelial function in chronic congestive heart failure. Am J Cardiol. 1992;69:1596–1601. doi: 10.1016/0002-9149(92)90710-g. [DOI] [PubMed] [Google Scholar]
- 41.Hayoz D, Drexler H, Munzel T, Hornig B, Zeiher AM, Just H, et al. Flow-mediated arterial dilation is abnormal in congestive heart failure. Circulation. 1993;87:VII-92–VII-96. [Google Scholar]
- 42.Hornig B, Maier V, Drexler H. Physical training improves endothelial function in patients with chronic heart failure. Circulation. 1996;93(2):210–214. doi: 10.1161/01.cir.93.2.210. [DOI] [PubMed] [Google Scholar]
- 43.Hornig B, Arakawa N, Haussmann D, Drexler H. Differential effects of quinaprilat and enalaprilat on endothelial function of conduit arteries in patients with chronic heart failure. Circulation. 1998;98(25):2842–2848. doi: 10.1161/01.cir.98.25.2842. [DOI] [PubMed] [Google Scholar]
- 44.Hundley WG, Bayram E, Hamilton CA, Hamilton EA, Morgan TM, Darty SN, et al. Leg flow-mediated arterial dilation in elderly patients with heart failure and normal left ventricular ejection fraction. Am J Physiol Heart Circ Physiol. 2007;292(3):H1427–H1434. doi: 10.1152/ajpheart.00567.2006. [DOI] [PubMed] [Google Scholar]
- 45.Myers J, Froelicher V. Hemodynamic determinants of exercise capacity in chronic heart failure. Ann Intern Med. 1991;115:377–386. doi: 10.7326/0003-4819-115-5-377. [DOI] [PubMed] [Google Scholar]
- 46.Franciosa JA. Role of ventricular function in determining exercise capacity in patients with chronic left ventricular failure. Adv Cardiol. 1986;34:170–8. doi: 10.1159/000413049. 170–178. [DOI] [PubMed] [Google Scholar]
- 47.Wilson JR, Rayos G, Yeoh TK, Gothard P, Bak K. Dissociation between exertional symptoms and circulatory function in patients with heart failure. Circulation. 1995;92(1):47–53. doi: 10.1161/01.cir.92.1.47. [DOI] [PubMed] [Google Scholar]
- 48.Clark AL, Sparrow JL, Coats AJ. Muscle fatigue and dyspnoea in chronic heart failure: two sides of the same coin? Eur Heart J. 1995;16(1):49–52. doi: 10.1093/eurheartj/16.1.49. [DOI] [PubMed] [Google Scholar]
- 49.Fink LI, Wilson JR, Ferraro N. Exercise ventilation and pulmonary artery wedge pressure in chronic stable congestive heart failure. Am J Cardiol. 1966;57:249–253. doi: 10.1016/0002-9149(86)90900-8. [DOI] [PubMed] [Google Scholar]
- 50.Sullivan M, Cobb FR. The anaerobic threshold in chronic heart failure. Circulation. 1990;81:II-47–II-58. [PubMed] [Google Scholar]
- 51.Green HJ. Manifestations and sites of neuromuscular fatigue. Biochem Exercise. 1990;VII:13–35. [Google Scholar]
- 52.Brucks S, Little WC, Chao T, Rideman RL, Upadhya B, Wesley-Farrington D, et al. Relation of anemia to diastolic heart failure and the effect on outcome. Am J Cardiol. 2004;93(8):1055–1057. doi: 10.1016/j.amjcard.2003.12.062. [DOI] [PubMed] [Google Scholar]
- 53.Deedwania PC, Gottlieb S, Ghali JK, Waagstein F, Wikstrand JC. Efficacy, safety and tolerability of beta-adrenergic blockade with metoprolol CR/XL in elderly patients with heart failure. Eur Heart J. 2004;25(15):1300–1309. doi: 10.1016/j.ehj.2004.05.022. [DOI] [PubMed] [Google Scholar]
- 54.Sanders P, Kistler PM, Morton JB, Spence SJ, Kalman JM. Remodeling of sinus node function in patients with congestive heart failure: reduction in sinus node reserve. Circulation. 2004;110(8):897–903. doi: 10.1161/01.CIR.0000139336.69955.AB. [DOI] [PubMed] [Google Scholar]
- 55.Nagaya N, Moriya J, Yasumura Y, Uematsu M, Ono F, Shimizu W, et al. Effects of Ghrelin Administration on Left Ventricular Function, Exercise Capacity, and Muscle Wasting in Patients With Chronic Heart Failure. Circulation. 2004;110(24):3674–3679. doi: 10.1161/01.CIR.0000149746.62908.BB. [DOI] [PubMed] [Google Scholar]
- 56.Sullivan JJ, Green HJ, Cobb FR. Skeletal muscle biochemistry and histology in ambulatory patients with long-term heart failure. Circulation. 1990;81:518–527. doi: 10.1161/01.cir.81.2.518. [DOI] [PubMed] [Google Scholar]
- 57.Adamopoulos S, Coats A, Brunotte F, Arnolda L, Meyer TE, Thompson CH, et al. Physical training improves skeletal muscle metabolism in patients with chornic heart failure. J Am Coll Cardiol. 1993;21:1101–1106. doi: 10.1016/0735-1097(93)90231-o. [DOI] [PubMed] [Google Scholar]
- 58.Stratton J, Dunn JF, Adamopoulos S, Kemp GJ, Coats A, Rajagopalan B. Training partially reverses skeletal muscle metabolic abnormalities during exercise in heart failure. J Appl Physiol. 1994;76:1575–1582. doi: 10.1152/jappl.1994.76.4.1575. [DOI] [PubMed] [Google Scholar]
- 59.Kouba EJ, Hundley WG, Brubaker PH, Brosnihan B, Nickolas B, Kitzman DW. Skeletal Muscle Remodeling and Exercise Intolerance in Elderly Patients with Diastolic Heart Failure. Am J Geriatr Cardiol. 2003;12(2):135. [Google Scholar]
- 60.Felker GM, Adams KF, Jr, Gattis WA, O’Connor CM. Anemia as a risk factor and therapeutic target in heart failure. J Am Coll Cardiol. 2004;44(5):959–966. doi: 10.1016/j.jacc.2004.05.070. [DOI] [PubMed] [Google Scholar]
- 61.Adams V, Jiang H, Yu J, Mobius-Winkler S, Fiehn E, Linke A, et al. Apoptosis in skeletal myocytes of patients with chronic heart failure is associated with exercise intolerance. J Am Coll Cardiol. 1999;33(4):959–965. doi: 10.1016/s0735-1097(98)00626-3. [DOI] [PubMed] [Google Scholar]
- 62.Wilson JR, Fink L, Maris J, Ferraro N, Power-Vanwart J, Eleff S, et al. Evaluation of energy metabolism in skeletal muscle of patients with heart failure with gated phosphorus-31 nuclear magnetic resonance. Circulation. 1985;71(1):57–62. doi: 10.1161/01.cir.71.1.57. [DOI] [PubMed] [Google Scholar]
- 63.Minotti JR, Johnson EC, Hudson TL, Zuroske G, Murata GH, Fukushima E, et al. Skeletal muscle response to exercise training in congestive heart failure. J Clin Invest. 1990;86:751–758. doi: 10.1172/JCI114771. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Minotti JR, Christoph I, Oka R, Weiner MW, Wells L, Massie BM. Impaired skeletal muscle function in patients with congestive heart failure. J Clin Invest. 1991;88:2077–2082. doi: 10.1172/JCI115537. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Mancini DM, Walter G, Reichek N, Lenkinski R, McCully KK, Mullen JL, et al. Contribution of skeletal muscle atrophy to exercise intolerance and altered muscle metabolism in heart failure. Circulation. 1992;85:1364–1373. doi: 10.1161/01.cir.85.4.1364. [DOI] [PubMed] [Google Scholar]
- 66.Minotti JR, Christoph I, Massie BM. Skeletal muscle function, morphology, and metabolism in patients with congestive heart failure. Chest. 1992;101:333S–339S. doi: 10.1378/chest.101.5_supplement.333s. [DOI] [PubMed] [Google Scholar]
- 67.Wilson JR, Mancini DM. Skeletal muscle metabolic dysfunction. Implications for exercise intolerance in heart failure. Circulation. 1993;87:VII-104–VII-109. [Google Scholar]
- 68.Minotti JR, Pillay P, Oka R, Wells L, Christoph I, Massie BM. Skeletal muscle size: relationship to muscle function in heart failure. J Appl Physiol. 1993;75(1):373–381. doi: 10.1152/jappl.1993.75.1.373. [DOI] [PubMed] [Google Scholar]
- 69.Kao W, Helpern JA, Goldstein S, Gheorghiade M, Levine B. Abnormalities of skeletal muscle metabolism during nerve stimulation determined by 31P nuclear magnetic resonance spectroscopy in severe congestive heart failure. Am J Cardiol. 1995;76(8):606–609. doi: 10.1016/s0002-9149(99)80166-0. [DOI] [PubMed] [Google Scholar]
- 70.Lang CC, Chomsky DB, Rayos G, Keoh TK, Wilson JR. Skeletal muscle mass and exercise performance in stable ambulatory patients with heart failure. J Appl Physiol. 1997;82:257–261. doi: 10.1152/jappl.1997.82.1.257. [DOI] [PubMed] [Google Scholar]
- 71.Harrington D, Anker SD, Chua TP, Webb-Peploe KM, Ponikowski PP, Poole-Wilson PA, et al. Skeletal muscle function and its relation to exercise tolerance in chronic heart failure. J Am Coll Cardiol. 1997;30(7):1758–1764. doi: 10.1016/s0735-1097(97)00381-1. [DOI] [PubMed] [Google Scholar]
- 72.Peters DG, Mitchell HL, McCune SA, Park S, Williams JH, Kandarian SC. Skeletal muscle sarcoplasmic reticulum Ca(2+)-ATPase gene expression in congestive heart failure. Circ Res. 1997;81(5):703–710. doi: 10.1161/01.res.81.5.703. [DOI] [PubMed] [Google Scholar]
- 73.Vescovo G, Volterrani M, Zennaro R, Sandri M, Ceconi C, Lorusso R, et al. Apoptosis in the skeletal muscle of patients with heart failure: investigation of clinical and biochemical changes [see comments] Heart. 2000;84(4):431–437. doi: 10.1136/heart.84.4.431. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Grimby G. Physical activity and effects of muscle training in the elderly. Annals Clin Res. 1988;20:62–66. [PubMed] [Google Scholar]
- 75.Fleg JL, Lakatta EG. Role of muscle loss in the age-associated reduction in VO2 max. J Appl Physiol. 1988;65(3):1147–1151. doi: 10.1152/jappl.1988.65.3.1147. [DOI] [PubMed] [Google Scholar]
- 76.Rice CL, Cunningham DA, Paterson DH, Lefcoe MS. Arm and leg composition determined by computed tomography in young and elderly men. Clin Physiol. 1989;9(3):207–220. doi: 10.1111/j.1475-097x.1989.tb00973.x. [DOI] [PubMed] [Google Scholar]
- 77.Kallman DA, Plato CC, Tobin JD. The role of muscle loss in the age-related decline of grip strength: cross-sectional and longitudinal perspectives. J Gerontol. 1990;45:M82–88. doi: 10.1093/geronj/45.3.m82. [DOI] [PubMed] [Google Scholar]
- 78.Buchner D, deLateur B. The importance of skeletal muscle strength to physical function in older adults. Behav Med Annals. 1991;13:4206–4214. [Google Scholar]
- 79.Menshikova EV, Ritov VB, Toledo FGS, Ferrell RE, Goodpaster BH, Kelley DE. Effects of weight loss and physical activity on skeletal muscle mitochondrial function in obesity. Am J Physiol Endocrinol Metab. 2005;288(4):E818–E825. doi: 10.1152/ajpendo.00322.2004. [DOI] [PubMed] [Google Scholar]
- 80.Warner JG, Metzger C, Kitzman DW, Wesley DJ, Little WC. Losartan improves exercise tolerance in patients with diastolic dysfunction and a hypertensive response to exercise. J Am Coll Cardiol. 1999;33:1567–1572. doi: 10.1016/s0735-1097(99)00048-0. [DOI] [PubMed] [Google Scholar]
- 81.Aronow WS, Kronzon I. Effect of enalapril on congestive heart failure treated with diuretics in elderly patients with prior myocardial infarction and normal left ventricular ejection fraction. Am J Cardiol. 1993;71:602–604. doi: 10.1016/0002-9149(93)90520-m. [DOI] [PubMed] [Google Scholar]
- 82.Vandenberg VF, Rath LS, Stuhlmuller P, Melton H, Skorton DJ. Estimation of left ventricular cavity area with on-line, semiautomated echocardiographic edge detection system. Circulation. 1992;86:159–166. doi: 10.1161/01.cir.86.1.159. [DOI] [PubMed] [Google Scholar]
- 83.Bonow RO, Leon MB, Rosing DR, Kent K, Lipson LC, Bacharach SL, et al. Effects of verapamil and propranolol on left ventricular systolic function and diatsolic filling in patients with coronary artery disease: radionuclide angiographic studies at rest and during exercise. Circulation. 1981;65:1337–1350. doi: 10.1161/01.cir.65.7.1337. [DOI] [PubMed] [Google Scholar]
- 84.Bonow RO, Dilsizian V, Rosing DR, Maron BJ, Bacharach SL, Green MV. Verapamil-induced improvement in left ventricular diastolic filling and increased exercise tolerance in patients with hyprertrophic cardiomyopathy: short- and long-term effects. Circulation. 1985;72:853–864. doi: 10.1161/01.cir.72.4.853. [DOI] [PubMed] [Google Scholar]
- 85.Udelson J, Bonow RO. Left ventricular diastolic function and calcium channel blockers in hypertrophic cardiomyopathy. In: Gaasch WH, editor. Left Ventricular Diastolic Dysfunction and Heart Failure. Malvern, Pennsylvania: Lea & Febiger; 1996. pp. 465–489. [Google Scholar]
- 86.Chen CH, Nakayama M, Talbot M, Nevo E, Fetics B, Gerstenblith G, et al. Verapamil acutely reduces ventricular-vascular stiffening and improves aerobic exercise performance in elderly individuals. J Am Coll Cardiol. 1999;33:1602–1609. doi: 10.1016/s0735-1097(99)00052-2. [DOI] [PubMed] [Google Scholar]
- 87.Serizawa T, Shin-Ichi M, Nagai Y, Ogawa T, Sato T, Nezu Y, et al. Diastolic abnormalities in low-flow and pacing tachycardia-induced ischemia in isolated rat hearts-modification by calcium antagonists. In: Lorell BH, Grossman W, editors. Diastolic Relaxation of the Heart. Norwell, Massachusetts: Kluwer Academic Publishers; 1996. pp. 266–274. [Google Scholar]
- 88.Cheng CP, Pettersson K, Little WC. Effects of felodipine on left ventricular systolic and diastolic performance in congestive heart failure. J Pharma and Exper Thera. 1994;271:1409–1417. [PubMed] [Google Scholar]
- 89.Cheng CP, Noda T, Ohno M, Little WC. Differential effects of enalaprilat and felodipine on diastolic function during exercise in dogs with congestive heart failure. Circulation. 1993;88(4):I-294. [Google Scholar]
- 90.Little WC, Cheng CP, Elvelin L, Nordlander M. Vascular selective calcium entry blockers in the treatment of cardiovascular disorders: Focus on felodipine. Cardiovasc Drugs Ther. 1995;9(5):657–663. doi: 10.1007/BF00878548. [DOI] [PubMed] [Google Scholar]
- 91.Ten Cate FJ, Serruys PW, Mey S, Roelandt JR. Effects of short-term administration of verapamil on left ventricular filling dynamics measured by a combined hemodynamic-ultrasonic technique in patients with hypertrophic cardiomyopathy. Circulation. 1983;68(6):1274–1279. doi: 10.1161/01.cir.68.6.1274. [DOI] [PubMed] [Google Scholar]
- 92.Hess OM, Murakami T, Krayenbuehl HP. Does verapamil improve left ventricular relaxation in patients with myocardial hypertrophy? Circulation. 1996;74:530–543. doi: 10.1161/01.cir.74.3.530. [DOI] [PubMed] [Google Scholar]
- 93.Brutsaert DL, Rademakers F, Sys SU, Gillebert TC, Housmans PR. Analysis of relaxtion in the evaluation of ventricular function of the heart. Prog Cardiovasc Dis. 1985;28:143–163. doi: 10.1016/0033-0620(85)90022-2. [DOI] [PubMed] [Google Scholar]
- 94.Brutsaert DL, Sys SU, Gillebert TC. Diastolic Failure: Pathophysiology and Therapeutic Implications. J Am Coll Cardiol. 1993;22:318–325. doi: 10.1016/0735-1097(93)90850-z. [DOI] [PubMed] [Google Scholar]
- 95.Setaro JF, Zaret BL, Schulman DS, Black HR. Usefulness of verapamil for congestive heart failure associated with abnormal left ventricular diastolic filling and normal left ventricular systolic performance. Am J Cardiol. 1990;66:981–986. doi: 10.1016/0002-9149(90)90937-v. [DOI] [PubMed] [Google Scholar]
- 96.Little WC, Wesley-Farrington DJ, Hoyle J, Brucks S, Robertson S, Kitzman DW, et al. Effect of candesartan and verapamil on exercise tolerance in diastolic dysfunction. J Cardiovasc Pharmacol. 2004;43(2):288–293. doi: 10.1097/00005344-200402000-00019. [DOI] [PubMed] [Google Scholar]
- 97.Little WC, Zile MR, Klein AL, Appleton CP, Kitzman DW, Wesley-Farrington DJ. Effect of Losartan and Hydrochlorothiazide on Exercise Tolerand in Exertional Hypertension and Diastolic Dysfunction. Am J Cardiol. 2006;98(3):383–385. doi: 10.1016/j.amjcard.2006.01.106. [DOI] [PubMed] [Google Scholar]
- 98.Pitt B, Reichek N, Willenbrock R, Zannad F, Phillips RA, Roniker B, et al. Effects of eplerenone, enalapril, and eplerenone/enalapril in patients with essential hypertension and left ventricular hypertrophy: the 4E-left ventricular hypertrophy study. Circulation. 2003;108(15):1831–1838. doi: 10.1161/01.CIR.0000091405.00772.6E. [DOI] [PubMed] [Google Scholar]
- 99.Rajagopalan S, Pitt B. Aldosterone as a target in congestive heart failure. Med Clin North Am. 2003;87(2):441–457. doi: 10.1016/s0025-7125(02)00183-9. [DOI] [PubMed] [Google Scholar]
- 100.Zannad F, Alla F, Dousset B, Perez A, Pitt B. Limitation of excessive extracellular matrix turnover may contribute to survival benefit of spironolactone therapy in patients with congestive heart failure: insights from the randomized aldactone evaluation study(RALES). Rales Investigators. Circulation. 2000;102(22):2700–2706. doi: 10.1161/01.cir.102.22.2700. [DOI] [PubMed] [Google Scholar]
- 101.Daniel KR, Wells GL, Fray B, Stewart KP, Kitzman DW. The effect of spironolactone on exercise tolerance and quality of life in elderly women with diastolic heart failure. Am J Geriatr Cardiol. 2003;12(2):131. [Google Scholar]
- 102.Mottram PM, Haluska B, Leano R, Cowley D, Stowasser M, Marwick TH. Effect of aldosterone antagonism on myocardial dysfunction in hypertensive patients with diastolic heart failure. Circulation. 2004;110(5):558–565. doi: 10.1161/01.CIR.0000138680.89536.A9. [DOI] [PubMed] [Google Scholar]
- 103.Little WC, Zile MR, Kitzman DW, Hundley WG, O’Brien TX, deGroof RC. The Effect of Alagebrium Chloride(ALT-711), a Novel Glucose Cross-Link Breaker, in the Treatment of Elderly Patients with Diastolic Heart Failure. J Card Fail 5 AD. 11(3):191–195. doi: 10.1016/j.cardfail.2004.09.010. [DOI] [PubMed] [Google Scholar]
- 104.Kass DA, Chen CH, Talbot MW, Rochitte CE, Lima JA, Berger RD, et al. Ventricular pacing with premature excitation for treatment of hypertensive-cardiac hypertrophy with cavity-obliteration. Circulation. 1999;100(8):807–812. doi: 10.1161/01.cir.100.8.807. [DOI] [PubMed] [Google Scholar]
- 105.Packer M, Carver JR, Chesebro J, et al. Effect of oral milrinone on mortality in severe chronic heart failure: The Prospective Randomized Milrinone Survival Evaluation(PROMISE) N Engl J Med. 1991;325:1468–1475. doi: 10.1056/NEJM199111213252103. [DOI] [PubMed] [Google Scholar]
- 106.Creager MA, Massie BM, Faxon DP, Friedman SD, Kramer BL, Weiner DA, et al. Acute and long-term effects of enalapril on the cardiovascular response to exercise and exercise tolerance in patients with congestive heart failure. J Am Coll Cardiol. 1985;6(1):163–173. doi: 10.1016/s0735-1097(85)80269-2. [DOI] [PubMed] [Google Scholar]
- 107.Sullivan M. Role of exercise conditioning in patients with severe systolic left ventricular dysfunction. In: Fletcher GF, editor. Cardiovascular Response to Exercise. Mount Kisco: Futura Publishing Company; 1994. pp. 359–372. [Google Scholar]
- 108.Vaitkevicius PV, Fleg J, Engel JH, O’Connor VC, Wright JG, Kalatta LE, et al. Effects of age and aerobic capacity on arterial stiffness in healthy adults. Circulation. 1993;88(5):1456–1462. doi: 10.1161/01.cir.88.4.1456. [DOI] [PubMed] [Google Scholar]
- 109.Pina IL, Apstein CS, Balady GJ, Belardinelli R, Chaitman BR, Duscha BD, et al. Exercise and heart failure: A statement from the American Heart Association Committee on exercise, rehabilitation, and prevention. Circulation. 2003;107(8):1210–1225. doi: 10.1161/01.cir.0000055013.92097.40. [DOI] [PubMed] [Google Scholar]
- 110.Coats A, Adamopoulos S, Radaelli A, McCance A, Meyer TE, Bernardi L, et al. Controlled trial of physical training in chronic heart failure. Circulation. 1992;85:2119–2131. doi: 10.1161/01.cir.85.6.2119. [DOI] [PubMed] [Google Scholar]
- 111.Arbab-Zadeh A, Dijk E, Prasad A, Fu Q, Torres P, Zhang R, et al. Effect of aging and physical activity on left ventricular compliance. Circulation. 2004;110(13):1799–1805. doi: 10.1161/01.CIR.0000142863.71285.74. [DOI] [PubMed] [Google Scholar]
- 112.Kitzman DW, Brubaker PH, Abdelahmed A, Stewart KP. Effect of Exercise Training on Exercise Capacity, Quality of Life, and Flow-Mediated Arterial Dilation in Elderly Patients with Diastolic Heart Failure. J Am Coll Cardiol. 2004;110(17):III-558. [Google Scholar]
- 113.Smart N, Haluska B, Jeffriess L, Marwick TH. Exercise training in systolic and diastolic dysfunction: Effects on cardiac function, functional capacity, and quality of life. American Heart Journal. 2007;153(4):530–536. doi: 10.1016/j.ahj.2007.01.004. [DOI] [PubMed] [Google Scholar]