

Abstract
The aim of this study was to assess whether automated torque-based stimulator triggering could improve precision in delivering stimuli near peak torque during voluntary activation tests. The quadriceps activation test was used as a test model in eleven volunteers. Automated torque-based triggering reduced stimulus delivery timing errors by 75% when compared with conventional automated time-based triggering. Torque-based stimulator triggering is recommended as an alternative to automated time-based triggering in voluntary activation tests, as torque-based triggering improves stimulus timing precision and thereby reduces measurement error.
Keywords: Central activation, Voluntary activation, Strength testing, ITT, CAR
Introduction
Voluntary muscle activation is commonly estimated using the interpolated twitch (ITT) or burst superimposition techniques.14 In these techniques, an electrical stimulus is introduced during a maximal voluntary isometric contraction (MVIC) with the goal of activating motor units that are inactive or firing sub-maximally. The torque increment associated with the electrical stimulus is then used to assess the completeness of voluntary activation.7 Electrical stimuli are conventionally delivered by one of two methods: 1) manually by visually inspecting the torque curve and triggering the stimulator at the point perceived to be peak torque/force2,5, or 2) automatically at a set time-point following the onset of volitional contraction.3,11,17 It is rare, however, for the stimulus to be delivered at peak torque with these approaches.12,14 Hence, some measurement error is introduced to the estimation of voluntary activation. The difficulty in delivering the stimulus at or near peak torque is recognized as one of the shortcomings of these voluntary activation tests.12,14 Triggering the stimulator using feedback from real-time torque signals has been suggested as a method that may improve the likelihood of delivering stimuli close to peak torque.1,14 However, to our knowledge the validity of this suggested approach has not been verified through investigation. Therefore, the aim of this study was to test the hypothesis that automated torque-based stimulator triggering would deliver electrical stimuli significantly closer to peak torque than was achieved by a conventional automated time-based stimulator triggering approach in which the stimulator was triggered three seconds after the onset of an MVIC.
Materials & Methods
Eleven young people (6 males, 5 females) with no history of serious lower extremity injuries participated in this study. Subjects refrained from strenuous activity for 24 hours prior to participation. All subjects provided written informed consent to participation using a form approved by the University of Iowa Human Subjects Research Institutional Review Board.
After a routine “warm-up” on a stationary bicycle, subjects were positioned on an isokinetic dynamometer (HUMAC NORM Testing and Rehabilitation System, Computer Sports Medicine, Inc., Stoughton, MA, USA) with their knees and hips fixed at 90° of flexion. Subjects were tightly secured to the test system chair using a waist strap, chest straps, and a thigh strap according to the manufacturer’s guidelines. Four sub-maximal trials (50% to 85% of perceived maximum effort) and one 5-second maximal voluntary isometric contraction (MVIC) were performed to prepare the thigh muscles for testing and orient the subjects to the testing procedures. After 3-minutes of rest, three 5-second MVICs were performed with 3-minutes of rest between each trial. The test system software was used to control the dynamometer and to signal the start and end of each trial and rest period. A computer program written in LabVIEW (v. 7.0, National Instruments Corp., Austin, TX, USA) was used to administer the test and record data. Torque signals were sampled using a PC with a 16-bit A-to-D conversion board (NI PCI-6032E, National Instruments Corp., Austin, TX, USA), which provided a resolution of 0.012 N·m. During the three MVICs, two lines were projected to a LCD monitor placed in front of the subjects. One was a torque threshold line that provided the test administrator with real-time feedback related to when the stimulator would trigger. For the first MVIC trial, this line was set at the peak torque value the subject obtained during the practice MVIC. For subsequent trials, the torque threshold lines were set at torque values that were slightly below (3%) the peak torque value obtained in the preceding trials. The automated stimulator triggering process was automatically initiated when the exerted torque exceeded this value. Including this threshold ensured that electrical stimuli were not delivered when torque levels were clearly below a subject’s maxima. Setting the initial torque threshold based on the peak torque recorded in the practice MVIC is a reasonable approach. It is very rare for subjects to reach peak torque on their first trial, and the approach yields a value close to the subject’s peak torque. The second line was a target torque line that the subjects were instructed to attempt to surpass by as much as possible during their MVIC trials. This torque target line was set at a torque magnitude that was 10% higher than the torque threshold. Maximal effort was facilitated using visualization of the subjects’ real-time torque signals, the target torque line, and loud verbal encouragement.
Real-time torque data recorded during the MVICs were used as feedback in the automated stimulus delivery program. Several case structures (True or False) and logical gates (e.g., AND gate, OR gate) were incorporated into the program so that the TTL pulse used to trigger the high voltage constant current stimulator (model DS7AH, Digitimer Ltd., Hertfordshire, England) would only be generated when the torque exerted by the subject exceeded the torque threshold and subsequently dropped by 1 N·m. The 1 N·m trigger value was selected based on pilot testing performed in our laboratory. The case structures and logical gates further ensured that the stimulator was only triggered once in each MVIC trial. An output signal from the constant current stimulator was simultaneously sampled along with the torque signals so that stimulus delivery was clearly identified. The sampling frequency was 1000 Hz. Although the stimulator was triggered during each MVIC, the intensity of the stimulus was set so that no current was delivered to the subjects’ thigh muscles. This approach was used, because our primary aim was to assess and compare the precision of the two triggering approaches in delivering stimuli near peak torque. The known aftereffects of stimulus superimposition on torque generation would have confounded this analysis.
Data Analysis
The stimulus delivery precision of the two triggering methods was assessed by calculating the percent error associated with the difference in torque between what was recorded at the time of stimulus delivery and the peak torque value recorded during the MVIC trials:
| [1] |
The trial that produced the highest voluntary peak torque was used in analyses, as it is customary to use the trial that produced highest voluntary torque when estimating voluntary activation deficits.9,13,10,17 The Wilcoxon Signed Ranks Test was used to determine significant differences between the two techniques. A significance level of α = 0.05 was used.
Results
The automated torque-based stimulator triggering method was significantly (P = 0.016) more precise in delivering stimuli near peak torque than the conventional time-based triggering method (Figure 1). The conventional time-based method delivered the stimulus when the exerted torque was on average, 5.1% (standard deviation: ± 4.9%) less than peak torque, whereas the torque-based method delivered the stimulus when the exerted torque was on average, 1.2% (± 0.8%) less than peak torque. Hence, the torque-based triggering approach reduced error by approximately 75%.
Figure 1.
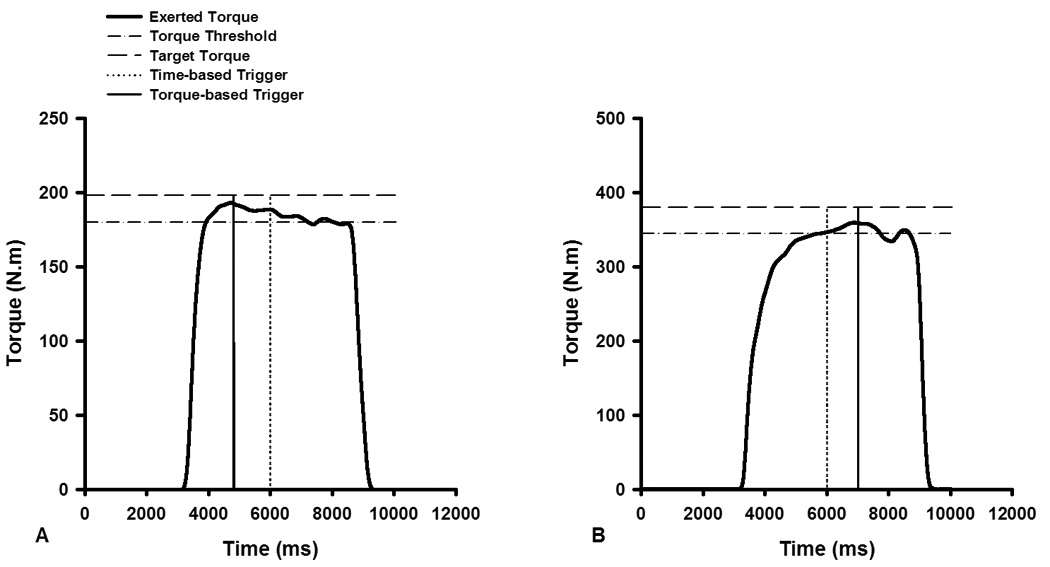
Two representative examples that demonstrate the precision of automated torque-based stimulator triggering in delivering stimuli near-peak torque. The first example (A) is from a female subject, and the second (B) is from a male subject. The torque threshold line represents the torque required to initiate the automated stimulator triggering process. The magnitude of this threshold was set using the peak torque values obtained during preceding MVIC trials. The target torque line established a target that the subjects were instructed to attempt to surpass by as much as possible during their MVIC trials. This was set 10% above the threshold torque value. With the torque-based triggering method (solid vertical lines) a stimulator was triggered when the torque exerted by the subject exceeded the torque threshold and subsequently dropped by 1 N·m. With the conventional time-based triggering method (broken vertical lines) the stimulator was triggered approximately 3 seconds after the onset of contraction. Note that in both examples the torque-based approach triggered the stimulator very close to peak torque, whereas the automated time-based approach triggered the stimulator after peak torque in (A) and before peak torque in (B).
Discussion
The inability to precisely introduce stimuli at peak torque/force is recognized as a source of error in the ITT and burst superimposition methods of testing voluntary activation.12,14 The results of this study clearly indicate that automated torque-based stimulator triggering significantly improves the precision of stimulus delivery when compared to the conventional time-based triggering approach. This finding was consistent in the sample studied; only one subject had less error with the automated time-based triggering approach.
We chose an automated time-based stimulator triggering approach as a comparison for the torque-based approach for the following reasons: 1) pilot-testing with 6 subjects in our laboratory indicated that there was no significant difference in the precision of stimulus delivery between automatic time-based triggering and manual triggering (error in automatic time-based triggering = 6.0%, error in manual triggering = 6.2%), 2) analysis of data reported in the literature from studies on quadriceps activation verified our own pilot study results, as similar stimulus delivery precision was present with automatic and manual triggering (automatic triggering error = 2.9%, manual triggering error = 3.1%),11,12, and 3) the automatic triggering approach has been the most commonly reported approach in studies published during the last 10 years. Based on our results from pilot study and analysis of data in the literature, it is expected that the advantages in stimulus timing precision associated with torque-based triggering would be similar whether the approach was compared with manual triggering of the stimulator or the automated time-based triggering approach tested in the present study. It is acknowledged, however, that a direct comparison of torque-based and manual stimulator triggering would be required to confirm this expectation. A valid head-to-head comparison of the three approaches was in our opinion impractical and unwarranted based on our preliminary analyses.
This study was designed so that no current was delivered to the subjects’ muscles when the stimulator was triggered, because our goal was to accurately assess stimulus timing precision of the two triggering approaches. The aftereffects of a supramaximal stimulus on the subjects’ torque curves would have confounded our analysis. Although this design was successful in enabling us to achieve our primary aim, it prevented us from defining how the improved stimulus timing observed with the torque-based triggering affects estimates of voluntary activation. Our experience to date using the torque-based triggering method when assessing voluntary activation in both healthy people and in patients indicates that the torque-based triggering approach does in fact reduce error in voluntary activation tests.
While automated torque-based triggering can significantly improve stimulus timing precision, this approach is dependent on the user’s selection of torque thresholds. Inappropriate selection of torque thresholds may lead to the stimulator triggering before peak torque. This is especially true when testing populations in which torque curve unsteadiness is common, such as the elderly and those who have sustained joint trauma.6,8 With appropriate selection of torque thresholds, instruction on generating a torque curve that builds to a plateau, and the inclusion of a series of preparatory isometric contractions prior to testing, stimulus delivery should be delivered consistently after peak torque. We recommend that readers start with the pre-testing routine and torque threshold selection approach described in this report and then modify the torque triggering parameters as necessary based on the results obtained with their own test systems.
We used a quadriceps activation testing model, as this is a common test that is reported in the literature and used in clinical settings; however, the results of this study are expected to apply to activation tests in other regions of the body. The findings are also expected to be applicable to voluntary activation tests that utilize other stimulation methods such as transcranial magnetic stimulation. The results of this study will be meaningful to scientists who use voluntary activation tests in research related to the effects and treatment of knee and other joint pathologies in which voluntary activation failure is often profound.4,9,15–17
Acknowledgements
This work was supported in part by NIH-NCMRR Grant # 1 K12 HD055931.
Abbreviations
- ITT
Interpolated Twitch Technique
- MVIC
Maximal Voluntary Isometric Contraction
- TTL
Transistor-Transistor Logic
References
- 1.Allen GM, Gandevia SC, McKenzie DK. Reliability of measurements of muscle strength and voluntary activation using twitch interpolation. Muscle Nerve. 1995;18(6):593–600. doi: 10.1002/mus.880180605. [DOI] [PubMed] [Google Scholar]
- 2.Bampouras TM, Reeves ND, Baltzopoulos V, Maganaris CN. Muscle activation assessment: effects of method, stimulus number, and joint angle. Muscle Nerve. 2006;34(6):740–746. doi: 10.1002/mus.20610. [DOI] [PubMed] [Google Scholar]
- 3.Behm D, Power K, Drinkwater E. Comparison of interpolation and central activation ratios as measures of muscle inactivation. Muscle Nerve. 2001;24(7):925–934. doi: 10.1002/mus.1090. [DOI] [PubMed] [Google Scholar]
- 4.Berth A, Urbach D, Neumann W, Awiszus F. Strength and voluntary activation of quadriceps femoris muscle in total knee arthroplasty with midvastus and subvastus approaches. J Arthroplasty. 2007;22(1):83–88. doi: 10.1016/j.arth.2006.02.161. [DOI] [PubMed] [Google Scholar]
- 5.De Serres SJ, Enoka RM. Older adults can maximally activate the biceps brachii muscle by voluntary command. J Appl Physiol. 1998;84(1):284–291. doi: 10.1152/jappl.1998.84.1.284. [DOI] [PubMed] [Google Scholar]
- 6.Enoka RM, Christou EA, Hunter SK, Kornatz KW, Semmler JG, Taylor AM, Tracy BL. Mechanisms that contribute to differences in motor performance between young and old adults. J Electromyogr Kinesiol. 2003;13(1):1–12. doi: 10.1016/s1050-6411(02)00084-6. [DOI] [PubMed] [Google Scholar]
- 7.Herbert RD, Gandevia SC. Twitch interpolation in human muscles: mechanisms and implications for measurement of voluntary activation. J Neurophysiol. 1999;82(5):2271–2283. doi: 10.1152/jn.1999.82.5.2271. [DOI] [PubMed] [Google Scholar]
- 8.Hortobagyi T, Garry J, Holbert D, Devita P. Aberrations in the control of quadriceps muscle force in patients with knee osteoarthritis. Arthritis Rheum. 2004;51(4):562–569. doi: 10.1002/art.20545. [DOI] [PubMed] [Google Scholar]
- 9.Hurley MV, Scott DL, Rees J, Newham DJ. Sensorimotor changes and functional performance in patients with knee osteoarthritis. Ann Rheum Dis. 1997;56(11):641–648. doi: 10.1136/ard.56.11.641. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Jayaraman A, Shah P, Gregory C, Bowden M, Stevens J, Bishop M, Walter G, Behrman A, Vandenborne K. Locomotor training and muscle function after incomplete spinal cord injury: case series. J Spinal Cord Med. 2008;31(2):185–193. doi: 10.1080/10790268.2008.11760710. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Krishnan C, Williams GN. Hamstrings Activity during Knee Extensor Strength Testing: Effects of Burst Superimposition. The Iowa Orthopaedic Journal. 2008;28:36–41. [PMC free article] [PubMed] [Google Scholar]
- 12.Miller M, Holmback AM, Downham D, Lexell J. Voluntary activation and central activation failure in the knee extensors in young women and men. Scand J Med Sci Sports. 2006;16(4):274–281. doi: 10.1111/j.1600-0838.2005.00479.x. [DOI] [PubMed] [Google Scholar]
- 13.Mizner RL, Petterson SC, Stevens JE, Vandenborne K, Snyder-Mackler L. Early quadriceps strength loss after total knee arthroplasty. The contributions of muscle atrophy and failure of voluntary muscle activation. J Bone Joint Surg Am. 2005;87(5):1047–1053. doi: 10.2106/JBJS.D.01992. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Shield A, Zhou S. Assessing voluntary muscle activation with the twitch interpolation technique. Sports Med. 2004;34(4):253–267. doi: 10.2165/00007256-200434040-00005. [DOI] [PubMed] [Google Scholar]
- 15.Suter E, Herzog W, Bray RC. Quadriceps inhibition following arthroscopy in patients with anterior knee pain. Clin Biomech (Bristol, Avon) 1998;13(4–5):314–319. doi: 10.1016/s0268-0033(98)00098-9. [DOI] [PubMed] [Google Scholar]
- 16.Urbach D, Berth A, Awiszus F. Effect of transcranial magnetic stimulation on voluntary activation in patients with quadriceps weakness. Muscle Nerve. 2005;32(2):164–169. doi: 10.1002/mus.20353. [DOI] [PubMed] [Google Scholar]
- 17.Williams GN, Buchanan TS, Barrance PJ, Axe MJ, Snyder-Mackler L. Quadriceps weakness, atrophy, and activation failure in predicted noncopers after anterior cruciate ligament injury. Am J Sports Med. 2005;33(3):402–407. doi: 10.1177/0363546504268042. [DOI] [PubMed] [Google Scholar]