

Abstract
AIM: To determine p16 promoter hypermethylation in gastric tumoral tissue and serum samples, its impact on p16-protein expression, and correlation with clinical and histological features.
METHODS: Samples were obtained from 52 histologically confirmed cases of gastric adenocarcinoma. Gastric tissue and serum of 50 age- and sex-matched individuals with normal gastroscopy and biopsy were obtained as control samples. Methylation-specific polymerase chain reaction (MSP) was used to evaluate methylation status of p16 promoter. p16-protein expression was analyzed by immunohistochemical staining on paraffin-embedded sections.
RESULTS: Methylation was detected in 44.2% (23/52) of tumoral tissues. 60.9% of them were also methylated in serum, i.e., 26.9% of all patients (14/52). Methylation was not detected in tissue and sera of control samples. p16-protein expression was decreased in 61.5% of cases (32/52), and was significantly associated with promoter hypermethylation (P < 0.001). Methylation was significantly more frequent in higher pathological grades (P < 0.05). Methylation was not associated with other clinicopathological features and environmental factors including H pylori infection and smoking.
CONCLUSION: p16 promoter hypermethylation is an important event in gastric carcinogenesis. It is the principle mechanism of p16 gene silencing. It is related to malignant tumor behavior. Detection of DNA methylation in serum may be a biomarker for early detection of gastric cancer.
Keywords: Gastric cancer, p16, Hypermethylation, Methylation specific PCR
INTRODUCTION
Gastric cancer is one of the most widespread cancers and the second leading cause of cancer-related death worldwide[1]. It is estimated that gastric cancer is the most common cancer in Iran (Age Standardized Rate = 26.1 per 105), and the incidence rate is higher than the world average[2]. Several genetic and epigenetic alterations have been suggested to play important roles in the carcinogenesis pathway, affecting oncogenes, tumor suppressor genes, apoptosis-regulating or mismatch repair genes[3]. Repression of genes by CpG island methylation in the promoter region, which is normally unmethylated, is the most frequent epigenetic alteration, in which the DNA structure is affected while the genetic code remains intact[4]. Thus, an increasing number of genes, methylated at the promoter region, are targeted as possible tumor markers for different purposes such as early detection, classification and tumor prognosis, therapeutic strategies and patient follow up[5–9].
Detection of circulating tumoral DNA was first reported about three decades ago[10]. Free DNA is thought to originate from apoptotic and necrotic tumoral cells[11]. More recently, detection of promoter hypermethylation in serum of patients has been reported in some malignancies such as colorectal or esophageal cancer[12,13]. Correlation of clinicopathological features with methylation patterns, which help to predict patient outcome, has been indicated in several studies[14–18].
p16 is a cell-cycle regulator that induces G1-phase arrest by inhibition of cyclin D-dependent protein kinase 4 (CDK4) and 6 (CDK6), thus interfering with phosphorylation of the retinoblastoma protein (pRb) and further inhibition of transcription of proteins that promote passage of the cell through the restriction point of the G1 stage[19]. p16 inactivation breaks down the regulatory mechanism of the cell cycle. As a tumor suppressor gene, being silenced by any mechanism will promote carcinogenesis. This study was conducted to assess the methylation of p16 promoter in gastric tumoral tissue and serum samples and its impact on gene expression, and correlation with clinical and histological features for the first time in the Iranian population.
MATERIALS AND METHODS
Sample collection and DNA preparation
Tumoral tissue and corresponding serum samples were obtained from 52 consecutive histologically confirmed gastric adenocarcinoma patients. Patients undergoing any therapeutic intervention were excluded. Tumoral tissues were obtained by gastrectomy or endoscopy in unresectable metastatic cases, formalin-fixed and paraffin-embedded. Tumors were histologically verified as gastric adenocarcinoma and subtyped into intestinal, diffuse, or mixed type, as suggested by Lauren[20]. Grading was also determined and staging was performed using tumor, node and metastasis (TNM) classification, sixth edition. Fifty age- and sex-matched individuals, with normal gastroscopy and biopsy, were included as a control group. Paraffin-embedded tissue and corresponding serum samples were taken as well. All patients and control individuals gave informed consent according to institutional guidelines, and the study was approved by the research ethics committee of Mashhad University of Medical Sciences. Paraffin-embedded tissues were retrieved by using xylene and alcohol, digested by proteinase K, extracted with phenol/chloroform/isoamyl alcohol, and precipitated in ethanol. Serum samples were isolated by DNA extraction kit (QIAamp DNA mini kit, QIAGEN, Canada). H pylori infection was detected and double checked in serum with an ELISA (Trinity H pylori kit, Ireland). None of the patients had a history of H pylori eradication.
DNA modification (bisulfite treatment)
DNA modification with sodium bisulfite causes unmethylated cytosine bases to convert to uracil, while methylated cytosine is resistant and remains unchanged. After treatment, methylated alleles have a different sequence as compared with unmethylated alleles, which can be used to design allele-specific PCR primers, and methylation-specific PCR (MSP) takes advantage of this fact[21]. Two micrograms of genomic DNA was first denatured by heating (97°C for 10 min followed by chilling on ice at 0°C for 5 min), and incubated for 20 min at 48°C after adding 3 mol/L NaOH (2 μL). Bisulfite solution (2.5 mol/L sodium metabisulfite and 125 mmol/L hydroquinone) was added and incubated for 12 h at 48°C in the dark, for modification. Modified DNA was purified by using Wizard DNA purification resin (DNA Cleanup Kit; Promega, Madison, WI, USA) according to the manufacturer’s instructions. Modified DNA was treated with 3 mol/L NaOH (5 μL) in 37°C for 10 min and precipitated with ammonium acetate 5 mol/L (75 μL), 2.5 volumes 100% ethanol and 2 μL glycogen (20 mg/mL; Fermentase; UAB, Lithuania) and dissolved in 20 μL 5 mmol/L Tris (pH 8.0).
MSP
Specific primer sets for unmethylated (p16U) and methylated (p16M) DNAs, described by Herman et al[21], were utilized (Table 1). The PCR mixture contained 1 × buffer (Finzymes OY, Finland) with 2 mmol/L MgCl2, 500 nmol/L each primer, 0.2 mmol/L dNTPs, 1 U Hot Start Taq polymerase (Finzymes OY, Finland). The PCR amplification of the modified DNA samples consisted of one cycle of 95°C for 10 min, 40 cycles of 94°C for 45 s, 60°C for 45 s, and 72°C for 1 min; then one cycle of 72°C for 10 min. DNA from L132 (embryonic lung cell line) cells was used as a positive control for unmethylated DNA. In order to make a positive control for methylated DNA, normal lymphocyte DNA was treated with M.Sss1 CpG methyltransferase (New England BioLabs, USA) before bisulfite treatment. Six microliters of amplified PCR products were loaded onto 2.5% agarose gels and non-denaturing 8% polyacrylamide gels, stained with ethidium bromide, and directly visualized under UV illumination.
Table 1.
Primer sets used in MSP
| Primer sets | Sense primer: 5’-3’ | Antisense primer: 5’-3’ | Size (bp) |
| p16-W | CAGAGGGTGGGGCGGACCGC | CGGGCCGCGGCCGTGG | 140 |
| p16-M | TTATTAGAGGGTGGGGCGGATCGC | GACCCCGAACCGCGACCGTAA | 150 |
| p16-U | TTATTAGAGGGTGGGGTGGATTGT | CAACCCCAAACCACAACCATAA | 151 |
W: Unmodified or wild-type primers; M: Methylated-specific primers; U: Unmethylated-specific primers.
Immunohistochemical staining
Immunohistochemical staining was performed using the CINtec p16INK4A Histology Kit, clone E6H4 (Dako, Carpinteria, CA, USA) and the DakoCytomation Autostainer Instrument, according to the manufacturer’s instructions. Briefly, 4-μm-thick formalin-fixed, paraffin-embedded sections were dewaxed, rehydrated and boiled in Target Retrieval Solution of Dako in a microwave oven for 40 min. After endogenous peroxidase blocking, the slides were incubated with primary p16INK4A antibody (clone E6H4) at 1:25 dilutions for 30 min. The antigen-antibody reaction was visualized by 3,3'-diaminobenzidine (DAB) chromogen for 10 min, followed by acidified hematoxyline counterstaining for 1 min. p16-positive cervical squamous cell carcinoma was used as an external positive control, and non-neoplastic stromal cells served as internal positive controls for p16 in every tumor section.
Statistical analysis
Statistical analysis was performed using SPSS software (ver. 11.5). The correlation between two variables was evaluated using Pearson’s χ2 and Fisher’s exact test. Statistical significance was defined as P < 0.05.
RESULTS
The studied population consisted of 38 men and 14 women. The median age was 64.5 and the average was 63.7 years (range, 38-81). Hypermethylation of p16 promoter was detected in 44.2% of tumoral gastric tissue (23/52), while normal gastric samples were all unmethylated. MSP analysis of the p16 promoter in gastric cancer is shown in Figure 1. Corresponding serum samples were also examined. Among the patients with methylated gastric tissue, 60.9% were also methylated in their corresponding serum, i.e., 26.9% of all cases (14/52). All normal individuals in the control group were unmethylated in their sera (Table 2).
Figure 1.
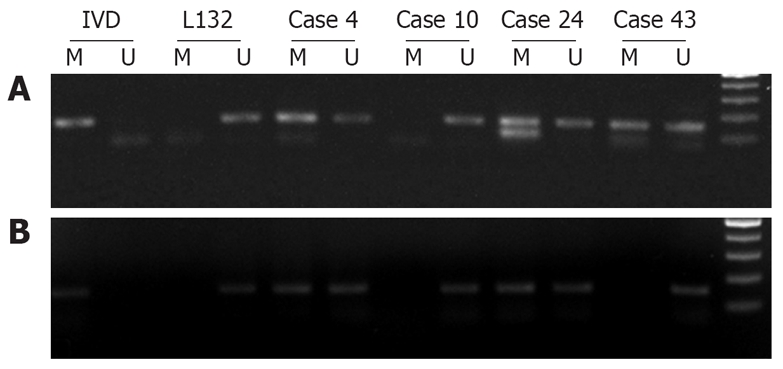
Analysis of p16 promoter hypermethylation in tissue and corresponding serum of patients. (A) MSP analysis. IVD served as a positive control for hypermethylated DNA and L132 as a positive control for unmethylated DNA. Patients 4, 24 and 43 were hypermethylated, which revealed 150 bp bands with hypermethylated primers. Patient 10 was not methylated. (B) MSP analysis in corresponding sera of samples depicted in A. Patients 4 and 24 were hypermethylated in serum as well. Patients 43 and 10 were not methylated.
Table 2.
Results of methylation in tumoral tissue and corresponding serum
| Tissue (+) | Tissue (-) | |
| Serum (+) | 14 | 0 |
| Serum (-) | 9 | 29 |
(+): Methylated; (–): Unmethylated.
Clinicopathological features of p16 promoter hypermethylation are tabulated in Table 3. There was no association between gender and promoter hypermethylation. Methylation had higher frequency in older patients (P = 0.051). Methylation was significantly lower in well-differentiated tumors as compared with higher pathological grades (P < 0.05). There was no significant difference in methylation status between intestinal and diffuse types. However, it was observed that 4/5 mixed type tumors were methylated, and all five were negative for p16 protein expression. Methylation was more frequent in non-cardiac type of tumor as compared with cardiac type (68.2% vs 31.8%), without statistical significance. p16 promoter methylation had no correlation with distant metastasis. No association was observed between methylated circulating DNA and lymph node metastasis.
Table 3.
Clinicopathological features of p16 promoter hypermethylation
| Variable | n (%) | Methylated | Unmethylated | P value |
| Total | 23 | 29 | ||
| Gender | ||||
| Male | 38 (73.1) | 17 | 21 | 0.904 |
| Female | 14 (26.9) | 6 | 8 | |
| Age (yr) | ||||
| < 64 | 26 (50.0) | 8 | 18 | 0.051 |
| > 64 | 26 (50.0) | 15 | 11 | |
| Pathological grade | ||||
| 1 | 20 (39.2) | 5 | 15 | < 0.05 |
| 2 | 11 (21.6) | 7 | 4 | |
| 3 | 20 (39.2) | 10 | 10 | (1 vs 2&3) |
| Pathological type | ||||
| Intestinal | 27 (62.7) | 13 | 14 | 0.754 (Intestinal vs Diffuse) |
| Diffuse | 14 (27.5) | 5 | 9 | 0.161 (Intestinal vs Mix) |
| Mixed | 5 (9.8) | 4 | 1 | 0.140 (Diffuse vs Mix) |
| Anatomical site | ||||
| Cardia | 22 (44.0) | 7 | 15 | 0.124 |
| Body | 15 (30.0) | 9 | 6 | |
| Pylorus | 13 (26.0) | 6 | 7 | (Cardia vs Noncardia) |
| Distant metastasis | ||||
| Absent | 39 (75.0) | 20 | 19 | 0.259 |
| Present | 13 (25.0) | 9 | 4 | |
| Smoking | ||||
| Yes | 9 (17.6) | 4 | 5 | 1.000 |
| No | 42 (82.4) | 19 | 23 | |
| H pylori infection | ||||
| Positive | 30 (60.0) | 11 | 19 | 0.201 |
| Negative | 20 (40.0) | 11 | 9 | |
Among environmental factors, we assessed H pylori infection and smoking. Sixty percent of patients (30/50) were infected with H pylori and 17.6% (9/51) were smokers. p16 promoter methylation had no correlation with smoking and H pylori infection.
Immunohistochemical staining of p16
Nuclear p16 immunostaining was positive for protein expression. Positive tumors varied in intensity of nuclear staining, with the proportion of cells ranging from 10% to 95%. In a few positive tumors, we observed marked heterogeneity in different areas with respect to p16 reactivity. Negative staining was observed in 61.5% of patients (32/52). Immunohistochemical staining is depicted in Figure 2. We assessed the correlation between immuno-histochemical staining and methylation status (Table 4). Among the p16-negative tumors, 62.5% were methylated, which showed strong correlation between negative immunostaining and promoter region hypermethylation (P < 0.001). There was significant correlation with pathological grade and mixed subtype, as well as methylation pattern, but no association was observed with other clinicopathological and demographic features and environmental factors.
Figure 2.

Immunohistochemical staining with monoclonal anti-p16 protein. (A) Nuclear reactivity showed expression of p16 protein (case 48). (B) p16-negative tumor (case 15) failed to stain due to decreased expression of p16 protein.
Table 4.
Results of methylation analysis in p16-positive and negative cases
| Immunohistochemistry | Methylated | Unmethylated |
| p16-positive | 3 | 17 |
| p16-negative | 20 | 12 |
DISCUSSION
Several genetic and epigenetic alterations play an important role in gastric carcinogenesis. Tumor suppressor and other tumor-related genes are the main targets. Aberrant alterations of p16, as a tumor suppressor gene, are important events in several tumors, including gastric cancer, and hypermethylation of CpG islands in the promoter region is responsible for a great proportion of tumors[22–25]. In this study, we demonstrated that 44.2% of tissues from gastric adenocarcinoma were methylated. The result was consistent with previous studies by Shim et al[26] and Ding et al[27] who reported 42% and 45% methylation of p16 promoter in gastric cancer.
Different mechanisms are suggested for decreased p16 protein expression, including homozygote deletion, point mutation and promoter methylation[28]. The first two mechanisms occur in < 10% of tumors[29,30]. We report that 61.5% of gastric adenocarcinomas were negative for p16 protein expression. Among p16-negative tumors, 62.5% were methylated in their promoter region, which was strongly correlated with decreased protein expression. We conclude that the principle mechanism for decreased p16-protein expression in gastric cancer is hypermethylation of the promoter region. There were three patients with normal protein expression despite promoter hypermethylation. All of these exhibited tumor heterogeneity, although partial methylation in one or both alleles might have been another possible reason. There were also twelve p16-negative patients with normal methylation status. Alternative mechanisms such as point mutation or homozygote deletion might be responsible for decreased protein expression.
Promoter hypermethylation was detected from sera of 60.9% of patients with tumor methylation, which accounted for 26.9% of all cases. This was similar to the study performed by Koike et al[31] who reported 27% methylated sera in gastric cancer patients. There are some interesting features that introduce p16 hypermethylation as a good serum marker for early detection of gastric cancer. As compared with other methods, serum markers are easier to use, less expensive and less invasive. Among serum markers, hypermethylation has some distinct features. It is a frequent event in cancer, while rare or absent in normal tissue, which leads to high specificity for the purpose of tumor diagnosis. Small specific regions of genome are affected, which make it easily detectable, in contrast with mutations. MSP is a sensitive technique that detects free circulating DNA even in small amounts[32]. Among many genes altered by methylation in gastric cancer, p16 promoter methylation is an early event in carcinogenesis[33]. We conclude that p16 is a good serum marker for early detection of gastric cancer.
In this study we showed that hypermethylation is less frequent in well-differentiated tumors. We conclude that p16 promoter hypermethylation is associated with tumor malignant behavior. There were no significant differences between intestinal and diffuse types in our population, but mixed subtype was strongly associated with silenced expression. However, there were only five cases with mixed type among our patients, and additional studies with a larger number of cases are needed to confirm the finding. In the population studied, 86.5% were at stage 3 and 4, which showed that gastric cancer was diagnosed in advanced stages, which necessitates early detection. We did not statistically compare patients at different stages, because of unbalanced distribution and the consequent bias. Methylation status in cardiac tumors was also compared with that of non-cardiac tumors. We know that cardiac tumors have different behavior from non-cardiac tumors. Methylation tends to occur more in distal tumors (more than two-fold higher), without statistical significance. We did not find any association between H pylori and methylation in our population, despite a few previous studies that suggested H pylori induces methylation[34,35]. Smoking, the other studied environmental factor, had no correlation with promoter hypermethylation. However, our patients consisted of only 17.6% (9/51) smokers, which was not sufficient to draw any strong conclusion. Promoter hypermethylation was not affected by gender, although it tended to occur more often in older patients. Precise matching and absence of promoter hypermethylation in the control individuals decreased the possibility of methylation induction by aging, unrelated to cancer. No association was observed between circulating methylated DNA and lymph node metastasis. This indicates that the origin of circulating methylated DNA is not from lymph node metastasis. Hypermethylation status in serum was not associated with other clinicopathological features either.
In conclusion, p16 promoter hypermethylation is an important event in gastric carcinogenesis. It is the principle mechanism of p16 gene silencing. It is associated with tumor malignant behavior. Detection of p16 hypermethylation in serum may be a useful biomarker for early detection of gastric cancer. Assessment of other serum markers may increase the sensitivity of screening in future studies. Moreover, promoter hypermethylation will regress after treatment. Further studies will determine whether promoter hypermethylation is a good surveillance marker for patient follow-up after treatment.
COMMENTS
Background
Gastric cancer is the second leading cause of cancer-related death worldwide. This is because most cases are diagnosed at an advanced stage, and there is no standard method for early detection. Several genetic and epigenetic alterations play important roles in gastric carcinogenesis. Methylation, the most important epigenetic alteration, influences gene repression without affecting genetic coding. Several recent studies have been conducted to assess the clinical implications of epigenetics in cancer. Free circulating, tumor-derived DNA is a good target for early detection as a serum marker. p16 is a tumor suppressor gene, which acts as a cell-cycle regulator. It is silenced in early stages of gastric carcinogenesis.
Research frontiers
P16 promoter hypermethylation related to clinicopathological features and early detection of gastric cancer.
Innovations and breakthroughs
A thorough analysis of p16 promoter hypermethylation, correlations with demographic and clinicopathological features and environmental factors, and implications as an early diagnostic marker were performed for the first time in the Iranian population.
Applications
Although p16 promoter hypermethylation is very specific for early detection of gastric cancer, further assessment of other genes will be useful to raise the sensitivity and provide a panel of serum markers for the purpose.
Peer review
This was a very interesting study. It examined p16 promoter hypermethylation in gastric adenocarcinoma and free DNA. Methylation was detected in 44% of tumors, and in 26.9% of serum. p16 promoter hypermethylation in serum was closely correlated with that in gastric tissue. Methylation was significantly associated with pathological grade.
Acknowledgments
We would like to thank Dr. Velayati, Dr. Gholamin and Mrs. Asadi for their technical assistance and Miss hoseinnezhad for her help in collecting gastric cancer specimens.
Supported by A grant offered by Mashhad University of Medical Sciences, No. 84129
Peer reviewer: Shingo Tsuji, Professor, Department of Internal Medicine and Therapeutics, Osaka University Graduate School of Medicine (A8), 2-2 Yamadaoka, Suita, Osaka 565-0871, Japan
S- Editor Li DL L- Editor Kerr C E- Editor Lu W
References
- 1.Munoz N, Franceschi S. Epidemiology of gastric cancer and perspectives for prevention. Salud Publica Mex. 1997;39:318–330. doi: 10.1590/s0036-36341997000400010. [DOI] [PubMed] [Google Scholar]
- 2.Sadjadi A, Nouraie M, Mohagheghi MA, Mousavi-Jarrahi A, Malekezadeh R, Parkin DM. Cancer occurrence in Iran in 2002, an international perspective. Asian Pac J Cancer Prev. 2005;6:359–363. [PubMed] [Google Scholar]
- 3.El-Rifai W, Powell SM. Molecular biology of gastric cancer. Semin Radiat Oncol. 2002;12:128–140. doi: 10.1053/srao.2002.30815. [DOI] [PubMed] [Google Scholar]
- 4.Strathdee G, Brown R. Aberrant DNA methylation in cancer: potential clinical interventions. Expert Rev Mol Med. 2002;4:1–17. doi: 10.1017/S1462399402004222. [DOI] [PubMed] [Google Scholar]
- 5.Abbaszadegan MR, Tavasoli A, Velayati A, Sima HR, Vosooghinia H, Farzadnia M, Asadzedeh H, Gholamin M, Dadkhah E, Aarabi A. Stool-based DNA testing, a new noninvasive method for colorectal cancer screening, the first report from Iran. World J Gastroenterol. 2007;13:1528–1533. doi: 10.3748/wjg.v13.i10.1528. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Toyota M, Ahuja N, Suzuki H, Itoh F, Ohe-Toyota M, Imai K, Baylin SB, Issa JP. Aberrant methylation in gastric cancer associated with the CpG island methylator phenotype. Cancer Res. 1999;59:5438–5442. [PubMed] [Google Scholar]
- 7.Lee TL, Leung WK, Chan MW, Ng EK, Tong JH, Lo KW, Chung SC, Sung JJ, To KF. Detection of gene promoter hypermethylation in the tumor and serum of patients with gastric carcinoma. Clin Cancer Res. 2002;8:1761–1766. [PubMed] [Google Scholar]
- 8.Cheng JC, Yoo CB, Weisenberger DJ, Chuang J, Wozniak C, Liang G, Marquez VE, Greer S, Orntoft TF, Thykjaer T, et al. Preferential response of cancer cells to zebularine. Cancer Cell. 2004;6:151–158. doi: 10.1016/j.ccr.2004.06.023. [DOI] [PubMed] [Google Scholar]
- 9.Abbaszadegan MR, Raziee HR, Ghafarzadegan K, Shakeri MT, Afsharnezhad S, Ghavamnasiry MR. Aberrant p16 methylation, a possible epigenetic risk factor in familial esophageal squamous cell carcinoma. Int J Gastrointest Cancer. 2005;36:47–54. doi: 10.1385/IJGC:36:1:047. [DOI] [PubMed] [Google Scholar]
- 10.Shapiro B, Chakrabarty M, Cohn EM, Leon SA. Determination of circulating DNA levels in patients with benign or malignant gastrointestinal disease. Cancer. 1983;51:2116–2120. doi: 10.1002/1097-0142(19830601)51:11<2116::aid-cncr2820511127>3.0.co;2-s. [DOI] [PubMed] [Google Scholar]
- 11.Jahr S, Hentze H, Englisch S, Hardt D, Fackelmayer FO, Hesch RD, Knippers R. DNA fragments in the blood plasma of cancer patients: quantitations and evidence for their origin from apoptotic and necrotic cells. Cancer Res. 2001;61:1659–1665. [PubMed] [Google Scholar]
- 12.Nakayama H, Hibi K, Taguchi M, Takase T, Yamazaki T, Kasai Y, Ito K, Akiyama S, Nakao A. Molecular detection of p16 promoter methylation in the serum of colorectal cancer patients. Cancer Lett. 2002;188:115–119. doi: 10.1016/s0304-3835(01)00839-4. [DOI] [PubMed] [Google Scholar]
- 13.Kawakami K, Brabender J, Lord RV, Groshen S, Greenwald BD, Krasna MJ, Yin J, Fleisher AS, Abraham JM, Beer DG, et al. Hypermethylated APC DNA in plasma and prognosis of patients with esophageal adenocarcinoma. J Natl Cancer Inst. 2000;92:1805–1811. doi: 10.1093/jnci/92.22.1805. [DOI] [PubMed] [Google Scholar]
- 14.Esteller M, Garcia-Foncillas J, Andion E, Goodman SN, Hidalgo OF, Vanaclocha V, Baylin SB, Herman JG. Inactivation of the DNA-repair gene MGMT and the clinical response of gliomas to alkylating agents. N Engl J Med. 2000;343:1350–1354. doi: 10.1056/NEJM200011093431901. [DOI] [PubMed] [Google Scholar]
- 15.Tang X, Khuri FR, Lee JJ, Kemp BL, Liu D, Hong WK, Mao L. Hypermethylation of the death-associated protein (DAP) kinase promoter and aggressiveness in stage I non-small-cell lung cancer. J Natl Cancer Inst. 2000;92:1511–1516. doi: 10.1093/jnci/92.18.1511. [DOI] [PubMed] [Google Scholar]
- 16.Roa JC, Anabalon L, Roa I, Tapia O, Melo A, Villaseca M, Araya JC. [Promoter methylation profile in gastric cancer. Rev Med Chil. 2005;133:874–880. [PubMed] [Google Scholar]
- 17.Leung WK, To KF, Chu ES, Chan MW, Bai AH, Ng EK, Chan FK, Sung JJ. Potential diagnostic and prognostic values of detecting promoter hypermethylation in the serum of patients with gastric cancer. Br J Cancer. 2005;92:2190–2194. doi: 10.1038/sj.bjc.6602636. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Vo QN, Geradts J, Boudreau DA, Bravo JC, Schneider BG. CDKN2A promoter methylation in gastric adenocarcinomas: clinical variables. Hum Pathol. 2002;33:1200–1204. doi: 10.1053/hupa.2002.130108. [DOI] [PubMed] [Google Scholar]
- 19.Sherr CJ. The Pezcoller lecture: cancer cell cycles revisited. Cancer Res. 2000;60:3689–3695. [PubMed] [Google Scholar]
- 20.Lauren P. The two histological main types of gastric carcinoma: diffuse and so-called intestinal-type carcinoma. Acta Pathol Microbiol Scand. 1965;64:31–49. doi: 10.1111/apm.1965.64.1.31. [DOI] [PubMed] [Google Scholar]
- 21.Herman JG, Graff JR, Myohanen S, Nelkin BD, Baylin SB. Methylation-specific PCR: a novel PCR assay for methylation status of CpG islands. Proc Natl Acad Sci USA. 1996;93:9821–9826. doi: 10.1073/pnas.93.18.9821. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Lee WH, Isaacs WB, Bova GS, Nelson WG. CG island methylation changes near the GSTP1 gene in prostatic carcinoma cells detected using the polymerase chain reaction: a new prostate cancer biomarker. Cancer Epidemiol Biomarkers Prev. 1997;6:443–450. [PubMed] [Google Scholar]
- 23.Belinsky SA, Nikula KJ, Palmisano WA, Michels R, Saccomanno G, Gabrielson E, Baylin SB, Herman JG. Aberrant methylation of p16(INK4a) is an early event in lung cancer and a potential biomarker for early diagnosis. Proc Natl Acad Sci USA. 1998;95:11891–11896. doi: 10.1073/pnas.95.20.11891. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Sato F, Meltzer SJ. CpG island hypermethylation in progression of esophageal and gastric cancer. Cancer. 2006;106:483–493. doi: 10.1002/cncr.21657. [DOI] [PubMed] [Google Scholar]
- 25.Zhao YF, Zhang YG, Tian XX, Juan Du, Jie Zheng. Aberrant methylation of multiple genes in gastric carcinomas. Int J Surg Pathol. 2007;15:242–251. doi: 10.1177/1066896907302117. [DOI] [PubMed] [Google Scholar]
- 26.Shim YH, Kang GH, Ro JY. Correlation of p16 hypermethylation with p16 protein loss in sporadic gastric carcinomas. Lab Invest. 2000;80:689–695. doi: 10.1038/labinvest.3780072. [DOI] [PubMed] [Google Scholar]
- 27.Ding Y, Le XP, Zhang QX, Du P. Methylation and mutation analysis of p16 gene in gastric cancer. World J Gastroenterol. 2003;9:423–426. doi: 10.3748/wjg.v9.i3.423. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Kamb A, Gruis NA, Weaver-Feldhaus J, Liu Q, Harshman K, Tavtigian SV, Stockert E, Day RS 3rd, Johnson BE, Skolnick MH. A cell cycle regulator potentially involved in genesis of many tumor types. Science. 1994;264:436–440. doi: 10.1126/science.8153634. [DOI] [PubMed] [Google Scholar]
- 29.Wu MS, Shun CT, Sheu JC, Wang HP, Wang JT, Lee WJ, Chen CJ, Wang TH, Lin JT. Overexpression of mutant p53 and c-erbB-2 proteins and mutations of the p15 and p16 genes in human gastric carcinoma: with respect to histological subtypes and stages. J Gastroenterol Hepatol. 1998;13:305–310. doi: 10.1111/j.1440-1746.1998.01560.x. [DOI] [PubMed] [Google Scholar]
- 30.Lee YY, Kang SH, Seo JY, Jung CW, Lee KU, Choe KJ, Kim BK, Kim NK, Koeffler HP, Bang YJ. Alterations of p16INK4A and p15INK4B genes in gastric carcinomas. Cancer. 1997;80:1889–1896. doi: 10.1002/(sici)1097-0142(19971115)80:10<1889::aid-cncr3>3.0.co;2-j. [DOI] [PubMed] [Google Scholar]
- 31.Koike H, Ichikawa D, Ikoma H, Tani N, Ikoma D, Otsuji E, Okamoto K, Ueda Y, Kitamura K, Yamagishi H. Comparison of serum aberrant methylation and conventional tumor markers in gastric cancer patients. Hepatogastroenterology. 2005;52:1293–1296. [PubMed] [Google Scholar]
- 32.Miyamoto K, Ushijima T. Diagnostic and therapeutic applications of epigenetics. Jpn J Clin Oncol. 2005;35:293–301. doi: 10.1093/jjco/hyi088. [DOI] [PubMed] [Google Scholar]
- 33.Kang GH, Lee S, Kim JS, Jung HY. Profile of aberrant CpG island methylation along the multistep pathway of gastric carcinogenesis. Lab Invest. 2003;83:635–641. doi: 10.1097/01.lab.0000067481.08984.3f. [DOI] [PubMed] [Google Scholar]
- 34.Perri F, Cotugno R, Piepoli A, Merla A, Quitadamo M, Gentile A, Pilotto A, Annese V, Andriulli A. Aberrant DNA methylation in non-neoplastic gastric mucosa of H. Pylori infected patients and effect of eradication. Am J Gastroenterol. 2007;102:1361–1371. doi: 10.1111/j.1572-0241.2007.01284.x. [DOI] [PubMed] [Google Scholar]
- 35.Ushijima T. Epigenetic field for cancerization. J Biochem Mol Biol. 2007;40:142–150. doi: 10.5483/bmbrep.2007.40.2.142. [DOI] [PubMed] [Google Scholar]