

Abstract
Disseminated signet ring cell carcinomas frequently arise from the stomach. However, primaries in the colon and rectum have also been reported. We present a 68 year old lady who presented with a change in her bowel habit. Colonoscopy showed a stenosing rectal tumour at 7 cm to 8 cm from the anal verge. Multiple scattered ulcers were also noted along the entire length of the colon. Biopsy of the lesions revealed signet ring cell adenocarcinoma. Gastroscopy showed multiple nodules with ulceration over several areas of the stomach which were similar in appearance to the colonic lesions. However, no primary tumour of the stomach was seen. Biopsy of the gastric lesions also showed signet ring cell adenocarcinoma. Computed tomography scan of the abdomen and pelvis revealed circumferential tumour at the rectosigmoid junction with possible invasion into the left ischiorectal fossa. The overall picture was that of a primary rectal signet ring cell carcinoma with peritoneal dissemination. The patient was referred for palliative chemotherapy in view of the disseminated disease. In the present report, we discuss this interesting pathological entity and review the role of various histolological techniques in helping to identify the primary tumor.
Keywords: Signet ring cell carcinoma, Colorectal tumour, Peritoneal dissemination, Gastric secondaries
INTRODUCTION
Primary colorectal signet ring cell carcinoma is a rare but distinctive malignancy of the large bowel. More than 96% of the signet ring cell carcinomas arise in the stomach, with the remainder arising from other sites, including colon, rectum, gallbladder, pancreas, urinary bladder and breast[1]. Therefore, metastasis to the colon and rectum must be excluded before a definite diagnosis of primary colorectal signet-ring cell carcinoma can be made.
CASE REPORT
A 68-year-old female patient with history of diabetes mellitus and hypertension presented with one month history of change in bowel habit. The patient complained of increased frequency of stools, with the passage of only small amounts of stools each time. There was no history of rectal bleeding, or loss of appetite or weight. Rectal examination revealed a hard mass about 6 cm from the anal verge.
Colonoscopy showed a hard stenosing rectal tumour at 7 cm to 10 cm from the anal verge (Figure 1A and B). Multiple scattered ulcers were found throughout the colon from the caecum to the sigmoid colon. Biopsy of the rectal tumour and the ulcers were performed. Transrectal ultrasound revealed a UT3N1 tumour of the mid-rectum.
Figure 1.

Colonoscopic pictures (A) and (B) show stenosing primary rectal tumour with multiple ulcerations; Gastroscopy (C) and (D) showed multiple ulcers in the stomach.
Carcino-embryonic antigen level was 10.7. Computed tomography of the abdomen and pelvis showed a circumferential tumour in the recto-sigmoid junction with no evidence of hepatic metastases or intrabdominal lymphadenopathy or a second primary.
Histopathology of the colonic ulcers and the rectal tumour showed large sheets and aggregates of signet ring cells with foamy cytoplasm and pleomorphic, hyper-chromatic eccentric nuclei (Figure 2A). The tumour cells infiltrated between the mucosal glands. Areas of ulceration and focal mucin pools were noted. These appearances were consistent with signet ring cell adenocarcinoma.
Figure 2.
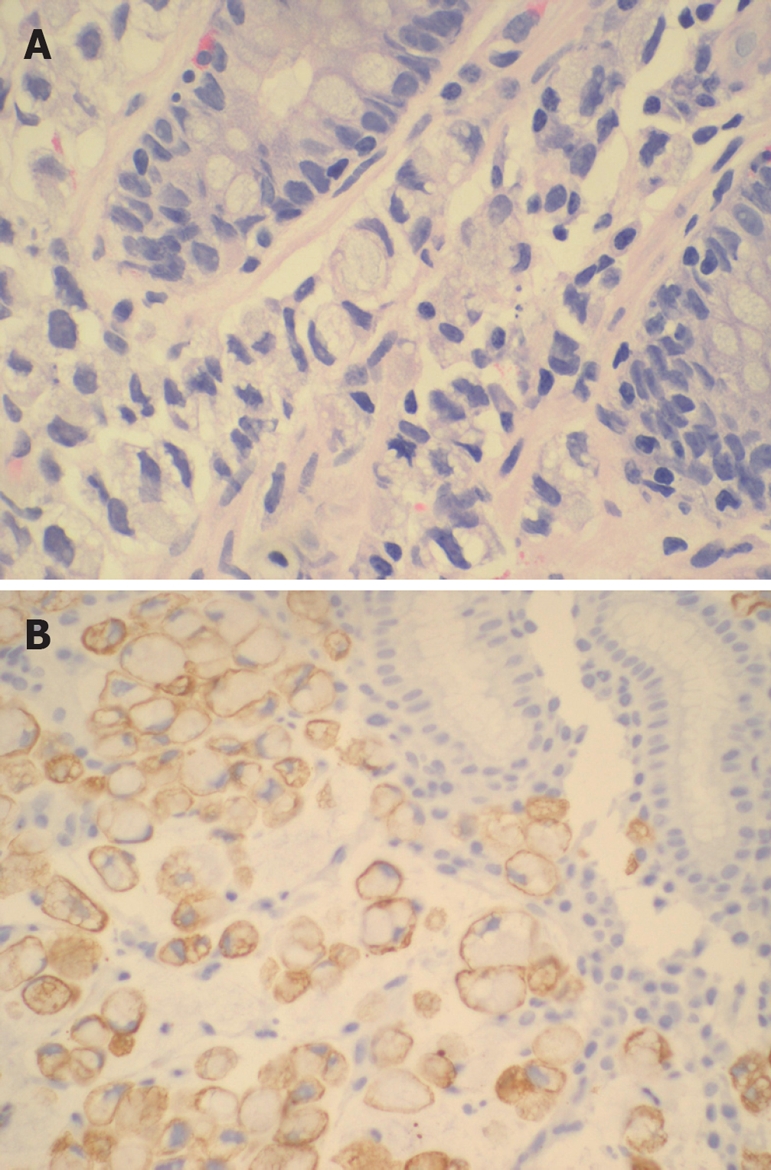
Photomicrograph A: normal colonic glands with signet ring cells within the lamina propria (HE); B: gastric mucosa with similar signet ring cells which were positive for CK 7.
In view of the histological finding of signet ring cell adenocarcinoma, gastroscopy was performed to exclude a gastric primary tumor. Gastroscopy revealed multiple nodules with ulceration scattered over body, incisura and antrum of the stomach (Figure 1C and D). No primary gastric tumour was found. Biopsy of the lesions showed signet ring cell adenocarcinoma similar to that found in the rectum and colon.
The clinical picture was that of a primary rectal signet ring cell adenocarcinoma with peritoneal dissemination and gastric metastasis. Immunohistochemical studies were performed to differentiate between a gastric and colonic primary tumor. Both specimens were positive for cytokeratin 7 (CK 7) (Figure 2B) and Cytokeratin 20 (CK 20).
In view of the disseminated peritoneal disease and minimal symptoms, the patient was not offered surgery. She received palliative chemoradiation and was clinically well at 6 mo follow-up.
DISCUSSION
Primary signet ring cell carcinoma of the colon and rectum is a rare variant of colorectal adenocarcinomas. The incidence of signet ring cell carcinoma is reported to range between 0.1% and 2.4%[2,3]. The diagnosis of primary colorectal signet ring cell carcinoma is often based on the histological appearance of the specimen with exclusion of a gastric primary.
Signet ring cell tumours have an aggressive clinical course and a poor prognosis[4–6]. There is high incidence of peritoneal metastases and relatively low incidence of hepatic metastases, a characteristic feature distinguishing colorectal signet-ring cell carcinoma from non-signet colorectal carcinoma.
According to Secco et al, the 5-year survival rate of primary colorectal signet ring cell carcinoma was 0% (median 15 mo) and disease recurrence was 100%. However, a local study from Singapore reported 5-year survival rate of 12%[7]. Generally, the prognosis of signet-ring cell carcinoma is worse than that of colorectal adenocarcinoma and most patients present at an advanced stage. It is important to identify disseminated peritoneal disease at the time of the initial diagnosis as these patients are unlikely to benefit from surgery, if the symptoms are minimal. It is important to obtain biopsy of lesions other than the primary tumour (as was done in this case) as it may provide diagnosis of disseminated peritoneal disease.
The histological appearance of the tumour is characterized by cells with abundant intracytoplasmic mucin, which pushes the nucleus to the periphery. The tumour cells may be arranged individually or in loose clusters, and may spread diffusely through the bowel wall. Mucin lakes containing small, primitive and abortive gland structures may be present[2,8].
Given the rarity of colon signet ring cell adeno-carcinomas, the question of a primary colon or metastatic gastric adenocarcinoma frequently arises when signet ring cell carcinoma is seen on colonoscopic biopsy.
Immunostaining profiles for CK7 and CK20 have been used to characterize and differentiate signet ring cell carcinomas of breast, stomach and colon[9,10]. CK20 is a low molecular weight cytokeratin that is normally expressed in the gastrointestinal epithelium, urothelium and in Merkel’s cells[11]. CK7 is expressed by tumours of the lung, ovary, endometrium and breast, but not of the lower gastrointestinal tract.
It has been suggested that when a signet ring cell adenocarcinoma is encountered on colon biopsy, the diagnosis of a colon primary is supported by the presence of CK7(-)/CK20(+) staining pattern in the neoplastic cells, while gastric primary is diagnosed if the cells have a CK7(+)/CK20(-) staining pattern.
However, in the present case, the colonic specimen was positive for both CK7 and CK20, making it difficult to determine whether the primary was gastric or colonic in origin.
To date, a primary rectal signet ring cell carcinoma with peritoneal dissemination and gastric secondaries had not been described. The present case illustrates the aggressive nature of signet ring cell carcinoma and the fact that immunohistochemistry may not be 100% accurate in predicting the primary source of the signet ring cell carcinoma.
Peer reviewer: Shotaro Nakamura, MD, Department of Medicine and Clinical Science, Kyushu University, Maidashi 3-1-1, Higashi-ku, Fukuoka 812-8582, Japan
S- Editor Li DL L- Editor Li M E- Editor Lu W
References
- 1.Tung SY, Wu CS, Chen PC. Primary signet ring cell carcinoma of colorectum: an age- and sex-matched controlled study. Am J Gastroenterol. 1996;91:2195–2199. [PubMed] [Google Scholar]
- 2.Laufman H, Saphir O. Primary linitis plastica type of carcinoma of the colon. AMA Arch Surg. 1951;62:79–91. doi: 10.1001/archsurg.1951.01250030082009. [DOI] [PubMed] [Google Scholar]
- 3.Chowdhury JR, Das K, Das KM. Primary linitis plastica of the colon: Report of a case and review of the literature. Dis Colon Rectum. 1975;18:332–338. doi: 10.1007/BF02587396. [DOI] [PubMed] [Google Scholar]
- 4.Amorn Y, Knight WA Jr. Primary linitis plastica of the colon: report of two cases and review of the literature. Cancer. 1978;41:2420–2425. doi: 10.1002/1097-0142(197806)41:6<2420::aid-cncr2820410648>3.0.co;2-l. [DOI] [PubMed] [Google Scholar]
- 5.Secco GB, Fardelli R, Campora E, Lapertosa G, Gentile R, Zoli S, Prior C. Primary mucinous adenocarcinomas and signet-ring cell carcinomas of colon and rectum. Oncology. 1994;51:30–34. doi: 10.1159/000227306. [DOI] [PubMed] [Google Scholar]
- 6.Giacchero A, Aste H, Baracchini P, Conio M, Fulcheri E, Lapertosa G, Tanzi R. Primary signet-ring carcinoma of the large bowel. Report of nine cases. Cancer. 1985;56:2723–2726. doi: 10.1002/1097-0142(19851201)56:11<2723::aid-cncr2820561137>3.0.co;2-n. [DOI] [PubMed] [Google Scholar]
- 7.Ooi BS, Ho YH, Eu KW, Seow Choen F. Primary colorectal signet-ring cell carcinoma in Singapore. ANZ J Surg. 2001;71:703–706. doi: 10.1046/j.1445-1433.2001.02269.x. [DOI] [PubMed] [Google Scholar]
- 8.Almagro UA. Primary signet-ring carcinoma of the colon. Cancer. 1983;52:1453–1457. doi: 10.1002/1097-0142(19831015)52:8<1453::aid-cncr2820520819>3.0.co;2-9. [DOI] [PubMed] [Google Scholar]
- 9.Goldstein NS, Long A, Kuan SF, Hart J. Colon signet ring cell adenocarcinoma: immunohistochemical characterization and comparison with gastric and typical colon adenocarcinomas. Appl Immunohistochem Mol Morphol. 2000;8:183–188. doi: 10.1097/00129039-200009000-00003. [DOI] [PubMed] [Google Scholar]
- 10.Tot T. The role of cytokeratins 20 and 7 and estrogen receptor analysis in separation of metastatic lobular carcinoma of the breast and metastatic signet ring cell carcinoma of the gastrointestinal tract. APMIS. 2000;108:467–472. doi: 10.1034/j.1600-0463.2000.d01-84.x. [DOI] [PubMed] [Google Scholar]
- 11.Varadhachary GR, Abbruzzese JL, Lenzi R. Diagnostic strategies for unknown primary cancer. Cancer. 2004;100:1776–1785. doi: 10.1002/cncr.20202. [DOI] [PubMed] [Google Scholar]