

Abstract
Introduction: Transverse myelitis is a very rare neurologic syndrome with an incidence per year of 1-5 per million population. We are presenting an interesting case of subacute transverse myelitis with its MRI (magnetic resonance imaging) and CSF (cerebrospinal fluid) findings.
Case: A 46-year-old African-American woman presented with decreased sensation in the lower extremities which started three weeks ago when she had a 36-hour episode of sore throat. She reported numbness up to the level just below the breasts. Lyme disease antibodies total IgG (immunoglobulin G) and IgM (immunoglobulin M) in the blood was positive. Antinuclear antibody profile was within normal limits. MRI of the cervical spine showed swelling in the lower cervical cord with contrast enhancement. Cerebrospinal fluid was clear with negative Borrelia Burgdorferi IgG and IgM. Herpes simplex, mycoplasma, coxiella, anaplasma, cryptococcus and hepatitis B were all negative. No oligoclonal bands were detected. Quick improvement ensued after she was given IV Ceftriaxone for 7 days. The patient was discharged on the 8th day in stable condition. She continued on doxycycline for 21 days.
Conclusions: Transverse myelitis should be included in the differential diagnosis of any patient presenting with acute or subacute myelopathy in association with localized contrast enhancement in the spinal cord especially if flu-like prodromal symptoms were reported. Lyme disease serology is indicated in patients with neurological symptoms keeping in mind that dissociation in Lyme antibody titers between the blood and the CSF is possible.
Keywords: transverse myelitis, Lyme disease
Abstract
Einleitung: Die transversale Myelitis ist eine seltene neurologische Erkrankung mit einer Häufigkeit von 1-5 pro 1 Mio. Bevölkerung und Jahr.
Wir stellen einen interessanten Fall einer subakuten transversalen Myelitis zusammen mit Magnetresonanztomographie und Liquorbefunden vor.
Fallbeschreibung: Eine 46-jährige Frau afrikanisch-amerikanischer Herkunft beklagte eine verminderte Sensibilität in den unteren Extremitäten, die drei Wochen vorher entstanden war, nachdem eine 36-stündige Phase mit trockenem Hals vorausgegangen war. Sie berichtete über Gefühllosigkeit bis hinauf im Brustbereich. Die Lyme-Antikörper IgG und IgM waren im Blut positiv. Die antinucleären Antikörper lagen im normalen Bereich. Die Magnetresonanztomographie des zervikalen Rückenmarks zeigte eine Anschwellung im unteren zervikalen Rückenmarkbereich mit erhöhtem Kontrast.
Der Liquor war klar, der Test auf Borrelia Burgdorferi IgG und IgM war negativ. Herpes simplex-, Mycoplasma-, Coxiella-, Anaplasma-, Cryptococcus- und Hepatits B-Tests waren alle negativ. Oligoklonale Banden konnten nicht nachgewiesen werden. Eine rasche Besserung erfolgte, als sie 7 Tage lang Ceftriaxon intravenös erhielt. Die Patientin wurde am 8. Tag entlassen in stabilisiertem Zustand. Über weitere 21 Tage nahm sie Doxycycline ein.
Schlussfolgerung: Die transversale Myelitis sollte in die Differenzialdiagnose bei Patienten einbezogen werden, die akute oder subakute Myelopathien in Verbindung mit lokalisierter Kontrastverstärkung im Rückenmark aufweisen, insbesondere wenn auch von grippeähnlichen Symptomen berichtet wird. Die Lyme-Serologie ist bei Patienten mit neurologischen Symptomen angezeigt, wobei zu bedenken ist, dass bei den Lyme-Antikörper-Titern Unterschiede zwischen Blut und Liquor auftreten können.
Introduction
Transverse myelitis is a very rare neurologic syndrome caused by inflammation of the spinal cord and occurs in both adults and children. Incidence per year varies from 1-5 per million population [1], [2]. Jeffery et al. [3] collected 33 cases in the Albuquerque area, NM, with a population base of 500,000 from 1960 through 1990 yielding an incidence of 4.6 per million per year. Berman et al. [4] gathered data on all Jewish patients with transverse myelitis throughout Israel for the period 1955 through 1975. Based on 62 patients who satisfied rigid diagnostic criteria, the average annual incidence rate was 1.34 per million population. No significant difference in incidence was noted between European/American-born and Afro/Asian-born populations. It is estimated that about 1400 new cases of transverse myelitis are diagnosed each year in the United States [5].
In the literature, a few cases of subacute transverse myelitis (SaTM) with their spinal MRI and cerebrospinal fluid (CSF) findings were reported [6]. We are presenting an interesting case of SaTM with its MRI and unusual CSF findings.
Case presentation
A 46-year old African-American woman presented with decreased sensation in the lower extremities. This started three weeks ago when she had a 36-hour bout of sore throat, cough and upper chest discomfort. At around the same time, she began to note a feeling of numbness of the right foot. Over the ensuing few days, this began to spread involving both legs up to the level of the knees. She reported hypersensitivity to touch in the lower extremities and described feeling as is she was walking on calluses. The sensation kept spreading up to the level of the buttocks and gradually up to the level just below the breasts bilaterally. Around that time, she began to have severe pain in the back involving the mid-thoracic region and interscapular area as well as the left scapular region. She was able to ambulate independently and was not aware of any weakness of the lower extremities. She had no upper extremity numbness, tingling or weakness. She noted decreased urination over the last two days, and when catheterized she was noted to have a post-void residual. She did not have a bowel movement for approximately 4 days. No prior similar episodes were reported.
She used to be in excellent health and exercised regularly. She did not use alcohol, cigarettes or illicit drugs and had no history of chronic medical problems. She had hysterectomy and bilateral salpingo-oophorectomy 25 years ago for fibroids. Her only medication was Premarin, but she had been using some Tylenol No.3 and/or Darvocet sparingly as needed for pain. Family history was negative for neurologic disease. She had had no tick bites, rash or fever. She denied headache, nausea or vomiting. Review of systems was otherwise negative.
Muscle strength was intact in the upper and lower extremities. Muscle tone was slightly increased in the lower limbs. There was no clonus. Deep tendon reflexes were traced in the upper extremities, 2+ at the knees, 2+ at the ankles. Toe signs were silent. There was no spine tenderness. Sensory examination revealed a sensory level to pin anteriorly at approximately T5 of T6. A level could not be determined over the back. Vibratory sense was absent at the ankles and reduced at the knees, but present over the upper extremities and sternum. Sensation was normal in the upper extremities.
White count 13,700/mm3, hemoglobin 13 g%, hematocrit 37%, platelets 289,000/mm3, VDRL (venereal disease research laboratory test), RPR (rapid plasma reagin test) and HIV (human immunodeficiency virus) were negative. ESR (erythrocyte sedimentation rate) was 28 mm/hr but CRP (C-reactive protein) was normal. TSH (thyroid stimulating hormone) was normal. Lyme disease total IgG and IgM in the blood was positive (>1.1 index). Antinuclear antibody profile was within normal limits.
MRI of the cervical and thoracic spine showed a diffuse, intramedullary abnormal signal extending from the medulla down to approximately the mid-thoracic level. There was swelling in portions of the spinal cord, particularly in the lower cervical cord where there was contrast enhancement (Figure 1 (Fig. 1), Figure 2 (Fig. 2), Attachment 1). The MRI of the brain was normal.
Figure 1. MRI of the cervical spine, sagittal view: contrast enhancement in the lower cervical cord.

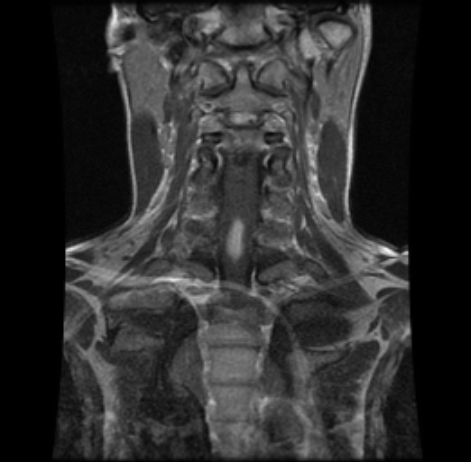
Figure 2. MRI of the cervical spine, coronal view: contrast enhancement in the lower cervical cord.
The impression was of subacute transverse myelitis. Multiple sclerosis and tumor were less likely. IV methylprednisolone was given. She had lumbar puncture and CSF studies done. CSF was clear. There were lymphocytes and monocytes with no malignant cells. Borrelia Burgdorferi IgG and IgM in the CSF were <0.80 index. No oligoclonal bands were detected. Herpes Simplex virus 1 and 2 DNA were <80 copies/mL. Mycoplasma, coxiella, anaplasma, cryptococcus and hepatitis B were all negative. Acyclovir ordered by the emergency doctor was discontinued the next day. She had a peripherally inserted central catheter (PICC) placed and was given IV ceftriaxone for 7 days and subsequently maintained on doxycycline for a 21-day course. No other processes were identified. Symptoms did seem to improve clinically. The patient stayed in hospital for 8 nights and was discharged in stable condition.
Discussion
The term transverse myelitis refers to nonspecific inflammation across one level of the spinal cord. Approximately one third of patients with transverse myelitis report a febrile illness (flu-like with fever) in close temporal relationship to the onset of neurologic symptoms. Transverse myelitis symptoms develop rapidly over several hours to several weeks. Approximately 45% of patients worsen maximally within 24 hours. Inflammation within the spinal cord interrupts neuronal pathways and causes the common presenting symptoms of transverse myelitis which include limb weakness, sensory disturbance, bowel and bladder dysfunction, and back/radicular pain.
Almost all patients develop leg weakness of varying degrees of severity. Sensation is diminished below the level of spinal cord involvement in the majority of patients. Some experience tingling or numbness in the legs. Pain and temperature sensation are diminished in the majority of patients. Vibration sensation and joint position sense may be decreased or spared. Bladder and bowel sphincter control are disturbed in the majority of patients. Patients sometimes report a tight banding or girdle-like sensation around the trunk that may be very sensitive to touch.
Transverse myelitis may occur in isolation (idiopathic) or in the setting of another illness. It may happen as a parainfectious, paraneoplastic or postvaccinal syndrome or as a complication of systemic autoimmune disease, multiple sclerosis or vasculopathy. Ropper AH and Poskanzer DC [7] followed 52 patients with acute and subacute transverse myelopathy at the Massachusetts General Hospital between 1955 and 1975. Nineteen had symptoms of a recent acute infectious illness, three had cancer, and one had undergone a recent operation. Jeffery et al. [3] had 45% of their 33 cases mentioned above categorized as parainfectious, 21% as associated with multiple sclerosis, 12% as associated with spinal cord ischemia, and 21% as idiopathic. Parainfectious transverse myelitis may be distinguishable from that associated with multiple sclerosis on the basis of presentation, findings on imaging, and the presence of cerebrospinal fluid oligoclonal bands. Patients with parainfectious transverse myelitis show evidence of spinal cord swelling, whereas patients with multiple sclerosis-associated transverse myelitis have spinal cord plaques on MRI but not swelling [3]. Oligoclonal bands are absent in patients with parainfectious transverse myelitis (as in our case) and present in the majority of patients with multiple sclerosis-associated transverse myelitis [3].
Acute myelitis accounts for 4 to 5 percent of all cases of neuroborreliosis [6]. In the study of Blanc et al. [6], Lyme serology was positive in CSF for all three reported cases. In our patient’s case, Lyme disease total IgG and IgM in the blood was positive (>1.1 index) however, Borrelia Burgdorferi IgG and IgM in the CSF were negative (<0.80 index). Lyme serology in CSF is indicated for any patients presenting with myelitis, particularly in endemic areas [6].
Transverse myelitis is generally a one-time occurrence and recuperation generally begins within 1 to 3 months with most patients showing good to fair recovery [4]. In the Ropper and Poskanzer study [7], an acute catastrophic onset was generally associated with back pain and led to a poor outcome in seven and a good outcome in only one of eleven patients. A subacute progressive onset over several days to four weeks (as in our case), generally with ascending paresthesias or leg weakness, was associated with a good outcome in 15 and fair outcome in 17 of 37 patients. The outcome seems to be correlated with the degree of cord enlargement, persistence of increased signal intensity and limited recovery. Atrophy and remaining high signal intensity are noted on late MRI in patients with poor outcome [8].
Although the patient, in our case, had negative Lyme titer in the CSF, the blood titer was positive and the patient responded quickly to ceftriaxone which was more consistent with transverse myelitis caused by borrelia burgdorferi. In addition to that, the high flu-like prodromal syndrome, high WBC (white blood cell count) and the detection of lymphocytes in the CSF pointed to infection-related process in the organism. IV ceftriaxone and oral doxycycline both were found to be effective, safe, and convenient for treatment of Lyme neuroborreliosis [9].
Conclusions
Transverse myelitis should be included in the differential diagnosis of any patient presenting with acute or subacute myelopathy in association with localized contrast enhancement in the spinal cord especially if flu-like prodromal symptoms were reported.
Lyme disease serology is indicated in patients with neurological symptoms keeping in mind that dissociation in Lyme antibody titers between the blood and the CSF is possible.
Notes
Conflicts of interest
None declared.
Supplementary Material
{kind=link}
References
- 1.Lynn J. Transverse myelitis: symptoms, causes and diagnosis. The Transverse Myelitis Association; c2006. [last modified 2007 Jul 17, cited 2008 Jan 29]. Available from: http://www.myelitis.org/tm.htm. [Google Scholar]
- 2.Lynn DJ, Newton HB, Rae-Grant A. The 5-minute Neurology Consult. Philadelphia, Pa.: Lippincott Williams & Wilkins; 2003. [Google Scholar]
- 3.Jeffery DR, Mandler RN, Davis LE. Transverse myelitis. Retrospective analysis of 33 cases, with differentiation of cases associated with multiple sclerosis and parainfectious events. Arch Neurol. 1993;50(5):532–535. doi: 10.1001/archneur.1993.00540050074019. [DOI] [PubMed] [Google Scholar]
- 4.Berman M, Feldman S, Alter M, Zilber N, Kahana E. Acute transverse myelitis: incidence and etiologic considerations. Neurology. 1981;31(8):966–971. doi: 10.1212/wnl.31.8.966. [DOI] [PubMed] [Google Scholar]
- 5.Transverse myelitis fact sheet. National Institute of Neurological Disorders and Stroke; [last updated 2007 Dec 11]. Available from: http://www.ninds.nih.gov/disorders/transversemyelitis/detail_transversemyelitis.htm. [Google Scholar]
- 6.Blanc F, Froelich S, Vuillemet F, Carré S, Baldauf E, de Martino S, Jaulhac B, Maitrot D, Tranchant C, de Seze J. Myelite aigue et neuroborreliose [Acute myelitis and Lyme disease] Rev Neurol (Paris) 2007;163(11):1039–1047. doi: 10.1016/s0035-3787(07)74176-0. [DOI] [PubMed] [Google Scholar]
- 7.Ropper AH, Poskanzer DC. The prognosis of acute and subacute transverse myelopathy based on early signs and symptoms. Ann Neurol. 1978;4(1):51–59. doi: 10.1002/ana.410040110. [DOI] [PubMed] [Google Scholar]
- 8.Holtås S, Basibüyük N, Fredriksson K. MRI in acute transverse myelopathy. Neuroradiology. 1993;35(3):221–226. doi: 10.1007/BF00588501. [DOI] [PubMed] [Google Scholar]
- 9.Borg R, Dotevall L, Hagberg L, Maraspin V, Lotric-Furlan S, Cimperman J, Strle F. Intravenous ceftriaxone compared with oral doxycycline for the treatment of Lyme neuroborreliosis. Scand J Infect Dis. 2005;37(6-7):449–454. doi: 10.1080/00365540510027228. [DOI] [PubMed] [Google Scholar]
- 10.Stone LA. Transverse myelitis. In: Rolak LA, Harati Y, editors. Neuroimmunology for the clinician. Boston, MA: Butterworth-Heinemann; 1997. pp. 155–165. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.