

Abstract
Background
Despite the prominence of comorbidity among substances and the recent attention focused on trajectory-based approaches to characterizing developmental change, little research in the substance use field has simultaneously considered both course and comorbidity.
Methods
Using nationally representative panel data from the Monitoring the Future Project (MTF; n = 32,087; 56% female; 82% Caucasian), we identified developmental courses of heavy drinking, smoking, and marijuana use using 4 waves of data spanning ages 18 to 26 in a multi-cohort young adult sample. Comorbidity was examined by cross-classifying group membership in substance use trajectories. Finally, the extent to which risk factors (sex, race, alcohol expectancies, delinquency, sensation seeking, depressive affect, religiosity, academic achievement, and parent education) accounted for combinations of comorbidity that occurred at a rate greater than chance was examined.
Results
For each substance, we identified 4 courses of substance use that were largely consistent with those found in the literature (chronic high use, late-onset use, developmentally limited use, and low-use), with a fifth moderate smoking group. Heavy drinking, smoking, and marijuana use were each highly associated, and distinct patterns of comorbidity were evident, with greatest agreement along the diagonal. All risk factors explained comorbidity to some degree, with delinquency, sensation seeking, alcohol expectancies, and religion in particular predicting combinations of comorbidity that were characterized by early onset and chronic high use.
Conclusions
Cross-substance trajectory concordance was high, with parallel changes in substance use over emerging adulthood. This suggests similar developmental timing of use, perhaps due to the experience of developmental transitions that have a common influence on use of different substances. Prediction of combinations of comorbidity characterized by early onset and persistently high use suggests that to some extent, individuals use multiple substances because of a common vulnerability to each, rather than directional relations among substances (e.g., cross-tolerance, cueing).
Keywords: Alcohol, Tobacco, Marijuana, Comorbidity, Trajectory, Developmental
IN NORTH AMERICA and many other industrialized societies, the transitional period from secondary school to young adulthood, spanning ages 18 to 25, has been referred to as “emerging adulthood” (Arnett, 2000). This is a time marked by frequent change and exploration and movement towards the assumption of adult roles and responsibilities; it is also a time during which the prevalence of alcohol use and related problems peaks (Arnett, 2000; Schulenberg and Maggs, 2002). For many individuals, onset of alcohol use occurs prior to leaving secondary school (Baer et al., 1995). However, peak use of alcohol typically occurs early on during emerging adulthood, as do associated alcohol problems. Although most emerging adults tend to “mature” out of alcohol involvement upon successfully negotiating developmental transitions associated with career and family (Bachman et al., 1997; Schulenberg and Maggs, 2002; Sher and Gotham, 1999), there are still many individuals who fail to moderate their alcohol consumption, which can have long-term effects on physical and psychological well-being (Schulenberg et al., 2003). There exists considerable individual heterogeneity in the timing and content of developmental milestones (Cohen et al. 2003; Schulenberg et al., 2004), including the use of substances such as alcohol, tobacco, and illicit drugs.
With the recent focus on charting developmental course of substance use afforded by methodological advances in mixture modeling techniques, some prototypical courses of substance use have emerged, including (but not limited to) a nonuser/stable low user course, an early onset persistent or chronic high use course, a “developmentally limited” course (transitioning or maturing out of substance use), and a late-onset increasing course. Studies assessing a sample across a broad developmental period tend to also identify a “fling” trajectory that, in studies using a younger or older sample, may manifest itself as an increasing or a developmentally limited course. In recent years, a great deal of work has been conducted on course of alcohol involvement (including but not limited to work by Chassin et al., 2002; Colder et al., 2002; Hill et al., 2000; Jackson and Sher, 2005; Oesterle et al., 2004; Schulenberg et al., 1996a,b; Tucker et al., 2003; Windle et al., 2005). Additional research has identified trajectories of tobacco use, showing an additional course characterized by experimental or moderate smoking, perhaps comprised of “chippers” who smoke during social situations (e.g., Abroms et al., 2005; Chassin et al., 2000; Colder et al., 2001; Orlando et al., 2005; Soldz and Cui, 2002; Stanton et al., 2004; Tucker, Ellickson, Orlando, & Klein, 2006; White et al., 2002; Wills, Resko, Ainette, & Mendoza, 2004). In addition, recent work has distinguished among courses of marijuana use (e.g., Brown et al., 2004; Ellickson et al., 2004; Kandel and Chen, 2000; Schulenberg et al., 2005; Windle and Wiesner, 2004).
Although high levels of comorbidity among substances have been demonstrated by a wealth of epidemiological (e.g., Donovan, 1996; Donovan and Jessor, 1985; Hays et al., 1987; Istvan and Matarazzo, 1984) and behavior genetic (e.g., Pickens et al., 1995; True et al., 1999) research, trajectory-based approaches largely focus on 1 substance at a time. Certainly the single-substance trajectories identified thus far have been shown to be associated with use of other substances. For example, trajectories of drinking are associated with poly-substance use (Chassin et al., 2002; Hill et al., 2000; Oesterle et al., 2004; Windle et al., 2005). In a similar fashion, trajectories of smoking are associated with alcohol use as well as with other drug use (Audrain-McGovern et al., 2004; Juon et al., 2002; Orlando et al., 2004; Soldz and Cui, 2002; Stanton et al., 2004; Tucker, Ellickson, Orlando, & Klein, 2006; White et al., 2002), with 1 study showing that marijuana use during adolescence very closely tracked smoking course (Soldz and Cui, 2002). Likewise, trajectories of marijuana use are associated with drinking (Brown et al., 2004; Schulenberg et al., 2005; Windle and Wiesner, 2004) and smoking (Kandel and Chen, 2000; Schulenberg et al., 2005; White et al., 2002; Windle and Wiesner, 2004).
Very few studies, however, have simultaneously considered both course and comorbidity. Using a group of youth during adolescence and young adulthood (approximate ages 11 to 30), Chassin et al. (2004) extracted 3 trajectories of alcohol and drug use as well as an a priori abstaining class and 4 trajectories of alcohol and drug dependence diagnoses as well as a nondiagnosing class. In general, the trajectories for use and dependence were characterized by absence versus presence of alcohol use and drug use as well as by level of severity (high or low). Using a treatment sample of adolescents (age 12 to 18), Chung, Maisto, Cornelius, and Martin (2004) identified short-term trajectories of abstinence for drinking and trajectories of abstinence for other drug use, and demonstrated moderately strong concordance between the 2 substances (Cohen's k = 0.49). Flory et al. (2004) independently derived separate trajectories of drinking and marijuana use among adolescents and young adults (approximate ages 11 to 21) and showed a strong association between them, with over half of the sample belonging to courses that were concordant with the corresponding course for the other substance. In addition, predictors of the 2 substances tended to be similar, suggesting that comorbidity may be accounted for by common mechanisms. Tucker et al. (2005) extracted individual trajectories for alcohol, tobacco, and marijuana use covering ages 13 through 23 and found overlap among classes with similar patterns of use across substances, particularly among abstainers but also among those characterized by increasing or early high use. Using the same sample as Tucker et al. (2005), Orlando et al. (2005) identified distinct courses of concurrent alcohol-tobacco use and found that for the most part, course of drinking paralleled change in smoking. Finally, in our own work, we identified 5 distinct courses of comorbid alcohol use disorders and tobacco dependence in a young adult sample (ages 18 to 24) (Jackson et al., 2000a). This work was followed by a study using a nationally representative young adult sample aged 18 to 26 (Jackson et al., 2005), in which we derived trajectories of smoking and drinking in a simultaneous modeling procedure. We identified distinct patterns of heavy drinking and smoking that could be differentiated by risk factors, and determined that the association between smoking and certain risk factors (delinquency, alcohol expectancies) appeared to exist by virtue of smoking's comorbidity with drinking. Although preliminarily analyses in that study identified trajectories of each single substance and characterized comorbidity between the two, describing and explaining comorbidity between the single-substance trajectories was not the focus of our earlier work.
We consider here several risk factors that to some degree may account for co-occurring substance use, including sex, race, alcohol expectancies, delinquency, sensation seeking, depressive affect, religiosity, academic achievement, and parent education. Indices of behavioral undercontrol such as novelty seeking and delinquency are associated with alcohol use (Elkins et al., 2006; Trull & Sher, 1994) and tobacco use (Bryant et al., 2000; Windle, 1990); this is consistent with a common trait of disinhibition that underlies use of alcohol, tobacco, and illicit drugs as well as other problem behaviors (McGue and Iacono, 2005; McGue et al., 2006). Although generally a less robust correlate than behavioral undercontrol, negative affect is associated with drug use (Degenhardt et al., 2003; Kassel et al., 2007). The association between drinking and alcohol expectancies is well established (see Jones et al., 2001), and expectancies for a given substance have been shown to be associated with other drug expectancies (Aarons, Brown, Coe, & Stice, 2001; Stacy et al., 1996). Men generally report greater alcohol consumption and marijuana use than women although, at least in recent cohorts, women are more likely to smoke (Johnston et al., 2007). In general, Whites are more likely to engage in substance use than Blacks, Hispanic, or Asians (Substance Abuse and Mental Health Services Administration (SAMHSA), 2007). Lower academic achievement is associated with increased risk for substance use (Bachman et al., 2008; Hallfors et al., 2006; Hawkins et al., 1992) and higher religiosity/conventionality appears to be protective against substance use (Miller, 1998; Rostosky et al., 2007; Wallace et al., 2007). Finally, low family socioeconomic status (SES) is associated with increased risk for substance use (Fothergill and Ensminger, 2006; Wills et al., 1995). In general, we expected to see courses characterized by greater comorbidity and high severity to exhibit the strongest associations with risk factors that correlate similarly with each substance on a univariate basis. For example, we might expect that negative affect is particularly associated with a course characterized by chronic high drinking and chronic high smoking. That is, not only will more severe courses be associated with more baseline risk factors, but these risk factors are expected to explain more comorbidity in conjoint trajectories.
The current study extends our previous work using Monitoring the Future (MTF) national panel data by exploring alcohol, tobacco, and marijuana use. As with our prior work on heavy drinking and smoking, we derive independent trajectories of each, and then characterize comorbidity among the 3 substances. In addition, using this modeling framework, we examine the extent to which comorbidity is accounted for by available important demographic and behavioral risk factors. Our sample is drawn from MTF panel data, a large national dataset that permits fairly broad generalizability to young adults in the U.S. The multiple-cohort nature of MTF controls for potential confounds between developmental change and secular change.
MATERIALS AND METHODS
Respondents and Procedure
Data were taken from the MTF project (e.g., Johnston et al., 2007), an ongoing national study of adolescents and young adults. Beginning in 1975, questionnaires were annually administered to approximately 17,000 high school seniors, using a multi-stage random sampling procedure (selection was based on geographic area, school, and classroom). Approximately 2,400 respondents from each cohort were randomly selected for biennial follow-up through mail surveys. These surveys begin 1 year post high school for one random half of each cohort and 2 years post high school for the other half; the 2 random halves were combined for these analyses. Study design and procedure are discussed in further detail in Bachman et al. (2002), in Johnston et al. (2007), and on the study web site (http://www.monitoringthefuture.org).
Panel data used in the present study are based on the follow-up data for senior year cohorts 1976 to 1997 (corresponding to birth year cohorts 1958 to 1979) collected at Waves 2 to 5 (henceforth termed Times 1 to 4). Respondents were on average 18 to 20 at Time 1, age 20 to 22 at Time 2, age 22 to 24 at Time 3, and age 24 to 26 at Time 4 (the sample was restricted to these modal ages due to the study's focus on developmental trajectories and the importance of retaining homogeneity in age). The sample used in the present study (n = 32,087) was primarily Caucasian (82%) and slightly less than half of the sample was male (44%). Respondents who reported heavy drug use at baseline were oversampled for follow-up. [We note here that in order to account for this selective probability of retention, we re-estimated trajectory models with a weight statement, down-weighting the heavy drug users. The pattern of trajectories was virtually identical, but the weighted results showed more individuals in the low-substance-using categories than the unweighted results (i.e., 68% vs. 63% for drinking; 73% vs. 69% for smoking; 86% vs. 80% for marijuana use). This is consistent with the over-sampling of the heavy drug users].
Measures
Substance use measures included frequency of heavy episodic (“binge”) drinking, quantity of cigarette smoking, and frequency of marijuana use (frequency of cigarette use was not available in these data). The Monitoring the Future substance use items have been used for decades in both the project's surveys and by other researchers. They have been shown to demonstrate excellent psychometric properties, and their reliability and validity have been reported and discussed extensively (e.g., Johnston and O'Malley, 1985; O'Malley et al., 1983). Although substance use variables as well as sex, race, age, parent education, academic achievement, and religion were assessed on all participants, some psychosocial scales (alcohol expectancies, delinquency, sensation seeking, depressive affect) were systematically given to random, nonoverlapping subsamples of the full respondent sample; analyses using these variables reflect this reduced sample size.
Heavy Alcohol Use
A single ordinal item assessed frequency of heavy drinking (operationalized as 5 or more drinks in a row) in the past 2 weeks. Item responses included 1 (never drink), 2 (once), 3 (twice), 4 (3 to 5 times), 5 (6 to 9 times), and 6 (10 or more times) (Time 1 M = 1.96). Figure 1 (upper left panel) presents the distribution of heavy drinking.
Fig. 1.

Prevalence of alcohol, tobacco, and marijuana use.
Tobacco Use
A single ordinal item assessing quantity of cigarettes smoked per day in the past 30 days was used. Item response categories included 1 (not at all), 2 (less than 1 cigarette per day), 3 (1 to 5 cigarettes per day), 4 (about 1/2 pack per day), 5 (about 1 pack per day) 6 (about 1 1/2 packs per day), and 7 (2 packs or more per day) (Time 1 M = 1.97). Figure 1 (upper right panel) presents the distribution of smoking.
Marijuana Use
A single ordinal item assessed the number of occasions the respondent used marijuana (grass, pot) or hashish in the past 30 days. Item response categories included 1 (0), 2 ( 1 to 2), 3 (3 to 5), 4 (6 to 9), 5 (10 to 19) 6 (20 to 39), and 7 (40 or more) (Time 1 M = 1.89). Figure 1 (bottom left panel) presents the distribution of marijuana use.
Demographic Characteristics
Age, sex (1 = male, 0 = female), and race were assessed at Wave 1 (Time 0). Race was coded broadly into 5 categories: White, Black, Hispanic, Asian, and Other (Native American, other ethnic minorities); for analysis, we used 4 dummy codes with White as reference group. Finally, parent education (a proxy for SES; also reported at Time 0) was computed by taking the mean of maternal and paternal education (inter-item r =0.55), which ranged from (1) completed grade school or less to (6) graduate or professional school after college. For respondents who reported on a single parent, SES reflected the education level for that parent. Unless otherwise noted, all risk factors were collected at Time 1. Table 1 presents descriptive information [n, means (SD) or proportion] for and correlations among the risk factors.
Table 1.
Descriptive Information and Inter-Correlations for Risk Factors
| Sex | Delinq | SS | NR Exp | PR Exp | Depr | Relig | Acad ach | SES | Asian | Black | Hispanic | n | M (SD) or % | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sex (% male) | 32,039 | 44.31% | ||||||||||||
| Delinquency | −0.24** | 7,821 | 1.17 (0.30) | |||||||||||
| Sensation seeking | −0.27** | 0.24** | 1,757 | 3.16 (1.20) | ||||||||||
| Neg reinforce expect | 0.03* | - | - | 4,826 | 0.19 (0.22) | |||||||||
| Pos reinforce expect | −0.09** | - | - | 0.32** | 4,826 | 0.28 (0.19) | ||||||||
| Depression | 0.00 | 0.14** | 0.07** | - | - | 1,757 | 1.77 (0.84) | |||||||
| Religiosity | 0.12** | −0.15** | −0.15** | −0.03* | −0.15** | −0.16** | 31,855 | 2.66 (0.90) | ||||||
| Acad ach | 0.13** | −0.12** | −0.14** | −0.06** | −0.14** | −0.13** | 0.12** | 31,327 | 5.93 (1.91) | |||||
| SES | −0.05** | 0.03** | 0.07** | −0.01 | 0.03* | −0.08** | −0.04** | 0.18** | 31,194 | 3.65 (1.18) | ||||
| Asiana | −0.02** | −0.01 | 0.02 | −0.04** | −0.04** | 0.07** | −0.03** | 0.06** | 0.05** | 31,837 | 1.94% | |||
| Blacka | 0.05** | −0.03** | −0.14** | −0.05** | −0.09** | −0.05 | 0.13** | −0.08** | −0.09** | −0.04** | 31,837 | 8.57% | ||
| Hispanica | 0.01 | −0.03* | −0.01 | −0.04** | −0.04** | 0.02 | 0.04** | −0.05** | −0.16** | −0.03** | −0.07** | 31,837 | 4.50% | |
| Othera | −0.01 | 0.03* | 0.03 | 0.03 | 0.00 | 0.04 | −0.01* | −0.06** | −0.05** | −0.03** | −0.06** | −0.04** | 31,837 | 3.39% |
Delinq, delinquency; SS, sensation seeking; NR exp, negative reinforcement expectancies; PR exp, positive reinforcement expectancies; Depr, depression; Relig, religiosity; Acad ach, academic achievement; Neg reinforcement expect, negative reinforcement expectancies; Pos Reinforcement expect, positive reinforcement expectancies.
p < 0.05
p < 0.01
Race was coded into 5 categories with White as reference group.
Risk Factors
Alcohol expectancies were assessed using 11 binary (yes/no) items that were preceded by the statement “What have been the most important reasons for your drinking alcoholic beverages.” From the set of 11 items, we created a negative expectancy scale and positive expectancy scale. Negative reinforcement expectancies (α = 0.59) were a mean across 5 items such as “To relax or relieve tension” and “To get away from my problems or troubles.” Positive reinforcement expectancies (α = 0.49) were a mean across 6 items such as “To have a good time with my friends” and “Because of boredom, nothing else to do.” These subscales parallel tension reduction and social facilitation expectancies for drinking (Jones et al., 2001). Although no expectancy items were available for smoking or marijuana, expectancies for a given substance may influence use of other substances, and different drug expectancies tend to correlate (Aarons et al., 2001). Past-year delinquency was the mean of 15 items ranging from (1) not at all to (5) 5 or more times, and included such items as “got in a serious fight in school or at work” and “been arrested and taken to a police station.” Internal consistency was good (α = 0.79). Sensation seeking was the mean of 2 items “I get a real kick out of doing things that are a little dangerous” and “I like to test myself every now and then by doing something a little risky” (r = 0.65). Depressive affect (α = 0.79) was assessed by taking the mean of the following 4 items: “Life often seems meaningless,” “The future often seems hopeless,” “I enjoy life as much as anyone,” and “It feels good to be alive” (with the last 2 items reverse scored).
Religiosity (important in its own right, as well as a proxy for conventionalism) was assessed using 2 items: importance of religion and attendance at religious services (inter-item r = 0.62). Importance of religion ranged from (1) not important to (4) very important, and attendance at religious services ranged from (1) never to (4) about once a week or more. Average high school grades, reported at Time 0, were used as an indicator of academic achievement; options ranged from (1) D (69 or below) to (9) A (93 to 100).
Analytic Procedure
To extract trajectories of substance use, we used a mixture modeling procedure (Muthén, 2001; Muthén and Shedden, 1999; Nagin, 1999; Nagin and Land, 1993). Growth mixture modeling is based on a latent growth modeling procedure. As with traditional growth models, growth is represented by latent growth factors (intercept, slope factors). However, whereas growth modeling has a parameter representing variability around the growth factor means, growth mixture modeling models variability with a latent (unobserved) categorical variable. This variable reflects discrete homogeneous classes of individuals who have similar responses on a given outcome (e.g., alcohol use). Classes were identified based on the mean of the growth factors alone because freeing the variances across classes typically resulted in model nonconvergence, consistent with other studies using this technique (e.g., Chassin et al., 2004; Colder et al., 2002; Tucker et al., 2003, 2005). Underlying latent growth models included an intercept and 2 slope factors (representing linear and quadratic growth) for the alcohol and marijuana use model; for the tobacco use model, the quadratic slope factor was eliminated due to convergence problems (possibly due to relatively stable levels of smoking). The intercept was centered at Time 1 (by virtue of a zero loading on the slope factors at Time 1) and the negative relation between the intercept factor and the slope factors was parameterized as a directional relation, rather than as a covariance, in order to address the phenomenon that when modeling negative growth, the higher an individual is at Time 1, the greater he/she falls over time (suggesting perhaps a floor effect for those low at Time 1).
Class prevalence is obtained for each trajectory, and each participant receives a probability of class membership for each class, ranging from 0 to 1.0. As recommended by Muthén (2004), model fit was evaluated using information criteria fit indices (Bayesian Information Criterion, BIC; Schwarz, 1978 and Akaike's Information Criterion, AIC; Akaike, 1987), for which low values are desired, as well as using the Vuong-Lo-Mendell-Rubin Likelihood Ratio test for k versus (k – 1) classes (Lo et al., 2001; Muthén et al., 2002) which tests whether k classes show improvement over (k – 1) classes. In addition, as these indices are a function of sample size (which would lead to an inflated number of significant model differences with the current sample size), we considered other criteria, including class interpretability (the extent to which an additional class provided unique information), class prevalence (preferring classes with 5% of the sample for improved replicability), and entropy (a measure of classification based on posterior probability values, with higher values representing better classification).
Given the multiple cohort design, we examined the effect of birth cohort on substance use and risk factors; linear, quadratic, and cubic trends were explored. Baseline drinking, smoking, and marijuana use linearly declined over cohort (η2 = 0.007, η2 = 0.015, and η2 = 0.046, respectively) (a finding consistent with other MTF analyses on these cohorts, Johnston et al., 2007). Birth cohort also had a significant linear effect such that later cohorts were more likely to be female (η2 = 0.001), to have lower delinquency (η2 = 0.001), to have higher negative reinforcement expectancies (η2 = 0.001) and lower positive reinforcement expectancies (η2 = 0.002), to have lower religiosity (η2 = 0.002), to have higher academic achievement (η2 = 0.01), to have higher SES (η2 = 0.02), and to be more likely to be Asian (η2 = 0.005) and Hispanic (η2 = 0.009) and less likely to be Black (η2 = 0.0002). Quadratic effects were also observed for smoking (η2 = 0.002), marijuana use (η2 = 0.007), negative reinforcement expectancies (η2 = 0.003) and race (η2 = 0.0001 for being Hispanic). Cubic effects were observed for drinking (η2 = 0.001), marijuana use (η2 = 0.002) sex (η2 = 0.0004), positive reinforcement expectancies (η2 = 0.003), religiosity (η2 = 0.001), and race (η2 = 0.0001 for being Hispanic). These quadratic and cubic trends reflect that over such a long time period, we see multiple secular trends occurring that are related to substance use, namely a tendency for substance use and the associated risk factors to generally decline over cohort but increase in recent cohorts. There was also significant age heterogeneity within cohort (in part due to the process of collecting follow-up data at biennial intervals). We controlled for birth cohort by treating it as an exogenous variable predicting Times 1 to 4 substance use variables (see Jackson et al., 2005). We used Mplus 4.10 (Muthén and Muthén, 1998−2004). Although retention rates for any one MTF follow-up survey averaged 75% to 80%, the listwise retention rate was 62%, so the model was estimated using full information maximum likelihood (FIML) which assumes that data are missing at random (MAR). A substantial majority of participants had at least 2 waves of data; 8% had data at only Time 1 and 0.5% had data from only 1 wave other than Time 1. Those retained in the longitudinal sample were more likely to be female, White, higher on high school GPA and parental education level, and lower on high school truancy and senior year substance use; see Schulenberg et al., 1996a,b, 2005). Finally, although the ordinal substance use variables were not normally distributed (see Figure 1), we treated them as continuous in the mixture modeling analyses. In general, analyses which treated these variables either as count or as censored variables failed to converge.
RESULTS
Findings from mixture models for heavy alcohol use, smoking, and marijuana use are presented, followed by a discussion of comorbidity between the 3 substances. Finally, we examine the extent to which risk factors account for comorbidity between the substances.
Mixture Modeling: Extracting Trajectories
For frequency of heavy alcohol use, we extracted 2-through 4-group solutions and found significant improvements in model fit up to 4 classes (and good entropy for all solutions, suggesting clear classification) (see Table 2). The model would not converge with 5 classes, suggesting that the data were most compatible with the 4-class solution. Figure 2 depicts estimated mean growth trajectories from Times 1 to 4 for frequency of heavy alcohol use by class, weighted by the probability of being in a given class. Based on the figure, the groups appear to include low heavy-drinkers (63%), chronic (CHR) heavy-drinkers (12%), developmentally limited (DV LTD), or decreasing, heavy-drinkers (16%), and late-onset (LATE), or increasing, heavy-drinkers (8%).
Table 2.
Mixture Models for Heavy Alcohol Use, for Smoking, and for Marijuana Use
| AIC | BIC | Entropy | Vuong-Lo-Mendell-Rubin LRT (p-value) | |
|---|---|---|---|---|
| Heavy drinking (n = 31,939) | ||||
| 2 classesa | 305657.94 | 305833.74 | 0.94 | <0.001 |
| 3 classes | 300408.64 | 300617.93 | 0.83 | <0.001 |
| 4 classes | 289682.53 | 289925.31 | 0.90 | <0.001 |
| Smoking (n = 31,952) | ||||
| 2 classes | 295847.47 | 295981.42 | 0.95 | <0.001 |
| 3 classes | 283840.21 | 283999.28 | 0.99 | <0.001 |
| 4 classes | 275359.47 | 275543.65 | 0.94 | <0.001 |
| 5 classes | 266864.32 | 267073.62 | 0.94 | <0.001 |
| 6 classesc | 265235.94 | 265235.94 | 0.70 | 0.49 |
| Marijuana use (n = 31,961) | ||||
| 2 classes | 306752.76 | 306928.58 | 0.99 | <0.001 |
| 3 classes | 290694.36 | 290903.67 | 0.97 | <0.001 |
| 4 classes | 275215.38 | 289160.32 | 0.97 | <0.001 |
| 5 classesb | 269909.77 | 270177.68 | 0.97 | <0.001 |
| 6 classesc | 266973.74 | 267283.52 | 0.69 | 0.50 |
LRT, likelihood ratio test.
This model had an improper solution (nonpositive definite residual covariance matrix) that could not be resolved. Although none of the growth factors had negative variances, it appears likely that the model which extracted 2 classes over-estimated the variance in the quadratic factor. However, given that it is an independence model against which to compare solutions with greater than 2 classes, we retain it in the Table for reference.
As this model had an improper solution (nonpositive definite residual covariance matrix), the Year 1 residual variance was constrained to zero.
This model had an improper solution (nonpositive definite first-order derivative matrix) that could not be resolved.
Fig. 2.
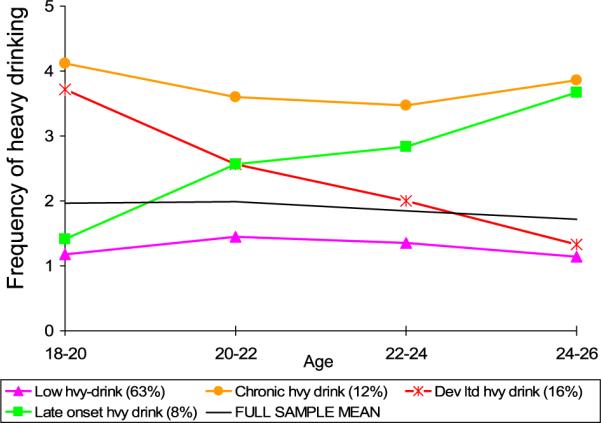
Mixture model for heavy drinking: Heavy drinking at Times 1 to 4 weighted by estimated class probabilities. Response values for frequency of heavy drinking (operationalized as 5 or more drinks in a row) in the past 2 weeks are 1 = never drink, 2 = once, 3 = twice, 4 = 3 to 5 times, 5 = 6 to 9 times, 6 = 10 or more times. AIC = 289682.53; BIC = 289925.31; Entropy = 0.90.
For smoking quantity, we tested 2- through 5-group solutions (the 6-group model would not converge on a proper solution) (see Table 2). We found significant improvements in model fit according to information criteria fit indices and the Vuong-Lo-Mendell-Rubin Likelihood Ratio test, a test for the number of components in a mixture, and good entropy up to 5 classes. Figure 3 depicts estimated mean growth trajectories for smoking quantity by class, weighted by estimated class probabilities. We extracted classes representing low-smokers (69%), CHR smokers (12%), LATE smokers (6%), DV LTD smokers (6%), and moderate (MOD) smokers (8%).
Fig. 3.
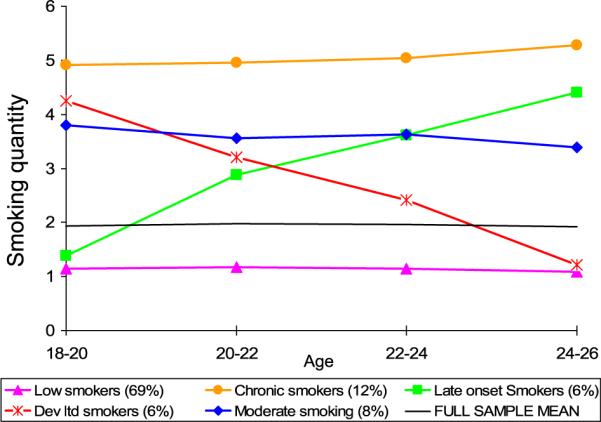
Mixture model for smoking: Smoking at Times 1 to 4 weighted by estimated class probabilities. Response values for quantity of cigarettes smoked per day in the past 30 days are 1 = not at all, 2 = less than 1 cigarette per day, 3 = 1 to 5 cigarettes per day, 4 = about 1.5 pack per day, 5 = about 1 pack per day, 6 = about 1 and 1.5 packs per day, 7 = 2 packs or more per day. AIC = 255436.56; BIC = 255704.46; Entropy = 0.99.
For frequency of marijuana use, we extracted 2- through 5-group solutions (again, the 6-group model failed to converge) and found significant improvements in model fit up to 5 classes (and good entropy for all solutions) (see Table 2). However, the fifth class was a combination of chronic and developmentally limited classes and included only 3% of the sample, and did not appear to represent an additional distinct class. Figure 4 depicts estimated mean growth trajectories from Times 1 to 4 for frequency of marijuana use by class for the 4-class solution, weighted by estimated class probabilities. Based on the figure, the groups appear to include low marijuana users (80%), CHR marijuana users (7%), DV LTD marijuana users (9%), and LATE marijuana users (4%).
Fig. 4.
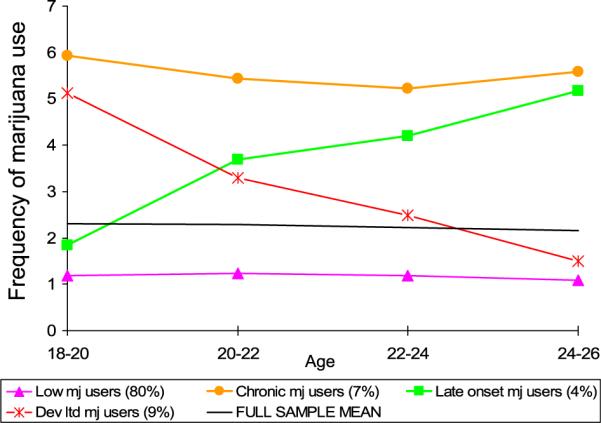
Mixture model for marijuana use: Marijuana use at Times 1 to 4 weighted by estimated class probabilities. Response options for number of occasions the respondent used marijuana (grass, pot) or hashish in the past 30 days are 1 = zero, 2 = 1 to 2, 3 = 3 to 5, 4 = 6 to 9, 5 = 10 to 19, 6 = 20 to 39, 7 = 40 or more. AIC = 275215.38; BIC = 275458.17; Entropy = 0.97.
Comorbidity
Alcohol and Tobacco Use
To evaluate comorbidity between alcohol and tobacco use, we examined a cross-tabulation of group membership for heavy drinking by smoking (i.e., a 4 × 5 table; see Table 3).1 We assigned group membership using posterior probabilities; that is, assigning an individual to the class to which he/she was most likely to belong. We also examined comorbidity using weighted estimates (weighted by probability of group membership in both groups). As might be expected by the clear classification in all models, estimates that were weighted by probability of group membership (which in most cases were close to 1.0) and corresponding tests of association were similar to findings using unweighted estimates. All subsequent analyses use the posterior probability approach, as parameters are more easily calculated in this approach than by hand-computing weighted scores.
Table 3.
Cross-Tabulations of Frequency (Cell Percentage) of Group Membership in Heavy Drinking Classes and Smoking Classes
| Tobacco |
||||||
|---|---|---|---|---|---|---|
| Low-smoker | Chronic | Dev. limited | Late onset | Moderate | ||
| Alcohol | 1 | 2 | 3 | 4 | 5 | Marginals |
| 1. Low heavy-drinker | 15,931 (50.0%)↑ | 1560 (4.9%) ↓ | 904 (2.8%) | 906 (2.8%) | 1229 (3.9%) | 20,530 (64.4%) |
| 2. Chronic | 1895 (6.0%)↓ | 890 (2.8%) ↑ | 288 (0.9%) | 295 (0.9%) | 496 (1.6%) ↑ | 3864 (12.1%) |
| 3. Developmentally limited | 2992 (9.4%)↓ | 917 (2.9%) ↑ | 573 (1.8%) ↑ | 242 (0.8%) | 538 (1.7%) | 5262 (16.5%) |
| 4. Late onset | 1216 (3.8%) | 371 (1.1%) | 78 (0.2%) | 291 (0.9%) ↑ | 241 (0.8%) | 2197 (6.9%) |
| Marginals | 22,034 (69.2%) | 3738 (11.7%) | 1843 (5.8%) | 1734 (5.4%) | 2504 (7.9%) | 31,853 |
Note. χ2(12, n = 31,853) = 2,474.41, p <0.001; Φ = 0.28; Cramer's V = 0.16. Numbers with up arrows (↑) indicate values that are significantly greater than what would be expected by chance ("types") and numbers with down arrows (↓) indicate values that are significantly less than what would be expected by chance ("antitypes") based on a conservative chi-square value of 100.
According to a Pearson chi-square test of association, drinking and smoking were moderately associated, χ2 (12, n = 31,853) = 2,474.41, p < 0.001; Φ = 0.28; Cramer's V = 0.16. Using a first-order configural frequency analysis technique (von Eye, 2002), we tested observed versus expected cell frequencies in the heavy drinking-smoking contingency table to determine “types” (i.e., configurations which occur more frequently than chance), and “antitypes” (i.e., configurations that occur less frequently than chance). We used Lehmacher's approximation to the binomial probability (with Küchenhof's correction for continuity cf. von Eye, 2002), with the significance criterion that cell misfit exceeds a chi-square value of 100. Significant types could be observed for cells along the diagonal (e.g., low heavy-drinker/low-smoker; chronic drinker/chronic smoker). In addition, a significant type was observed for the combination of CHR drinker (DRK) with MOD smoking (SMK), and for the combination of CHR SMK with DV LTD DRK. Correspondingly, we observed significant antitypes for the combination of the low heavy-drinker class and CHR SMK and for the combination of the low-smoker class and both CHR and DV LTD DRK classes. These types and antitypes are portrayed (using up and down arrows) in Table 3.
Finally, we also examined the association between heavy drinking and smoking only among those in the chronic high, later onset, developmentally limited, and (for smoking) moderate groups in order to determine the extent to which the alcohol-tobacco association was driven by low heavy-drinkers and low-smokers (that is, individuals who either abstain or were low users of both substances throughout). Analyses excluding the low using groups still showed a small-to-moderate association, χ2(6, n = 5,220) = 302.41, p < 0.001; Φ = 0.24; Cramer's V = 0.17.
Alcohol and Marijuana Use
Next, to evaluate comorbidity between alcohol and marijuana use, we computed a 4 × 4 cross-tabulation of group membership for heavy drinking by marijuana use (see Table 4). Drinking and marijuana use were also associated, χ2(9, n = 31,869) = 4,179.32, p < 0.001; Φ = 0.36; Cramer's V = 0.21; Cohen's k = 0.21. Significant types were evident for cells along the diagonal. In addition, significant types were observed for the combination of CHR DRK with DV LTD marijuana (MJ) and of CHR DRK with LATE MJ. Correspondingly, significant antitypes were observed for the combination of the low heavy-drinker class and both CHR and DV LTD MJ classes, and for the combination of the low marijuana using class and both CHR and DV LTD DRK classes.
Table 4.
Cross-Tabulations of Frequency (Cell Proportion) of Group Membership in Heavy Drinking Classes and Marijuana Use Classes
| Marijuana use |
|||||
|---|---|---|---|---|---|
| Low-user | Chronic | Dev. limited | Late onset | ||
| Alcohol | 1 | 2 | 3 | 4 | Marginals |
| 1. Low heavy-drinker | 18,469 (58.0%)↑ | 611 (1.9%)↓ | 999 (3.1%)↓ | 461 (1.4%) | 20,540 (64.4%) |
| 2. Chronic | 2062 (6.5%) ↓ | 828 (2.6%) ↑ | 718 (2.2%) ↑ | 259 (0.8%) ↑ | 3867 (12.1%) |
| 3. Developmentally limited | 3551 (11.1%) ↓ | 548 (1.7%) | 996 (3.1%) ↑ | 168 (0.5%) | 5263 (16.5%) |
| 4. Late onset | 1634 (5.1%) | 211 (0.7%) | 171 (0.5%) | 183 (0.6%) ↑ | 2199 (6.9%) |
| Marginals | 25,716 (80.7%) | 2198 (6.9%) | 2884 (9.0%) | 1071 (3.4%) | 31,869 |
Note. χ2(9, n = 31,869) = 4,179.32, p < 0.001; Φ = 0.36; Cramer's V = 0.21; Cohen's κ = 0.21. Numbers with up arrows (↑) indicate values that are significantly greater than what would be expected by chance ("types") and numbers with down arrows (↓) indicate values that are significantly less than what would be expected by chance ("antitypes"), based on a conservative chi-square value of 100.
We also examined the association between drinking and marijuana use among all participants except the consistent low users/abstainers. Analyses excluding the low using groups showed a small association, χ2(4, n = 9,742) = 296.52, p < 0.001; Φ = 0.17; Cramer's V = 0.12; although Cohen's k = −0.01, suggesting that virtually all of the agreement was due to the group of low heavy-drinkers and low marijuana users.
Marijuana and Tobacco Use
Finally, we computed a 4 × 5 cross-tabulation of group membership for smoking by marijuana use (see Table 5). Smoking and marijuana use were associated, χ2(12, n = 31,872) = 3,683.51, p < 0.001; Φ = 0.34; Cramer's V = 0.20. Significant types were evident for cells along the diagonal. In addition, a significant type was found for the combination of DV LTD MJ with both CHR SMK and MOD SMK, and a significant type was observed for CHR MJ and MOD SMK. Significant antitypes were observed for the combination of the low-smoking class and the 3 marijuana using classes, and for the combination of the low marijuana using class and CHR SMK. Analyses excluding the low marijuana and low-tobacco using groups still showed a small association between marijuana and tobacco, χ2(6, n = 8,400) = 169.91, p <0.001; Φ =0.14; Cramer's V = 0.10.
Table 5.
Cross-Tabulations of Frequency (Cell Percentage) of Group Membership in Marijuana Classes and Smoking Classes
| Tobacco |
||||||
|---|---|---|---|---|---|---|
| Low-smoker | Chronic | Dev. limited | Late onset | Moderate | ||
| Marijuana | 1 | 2 | 3 | 4 | 5 | Marginals |
| 1. Low-user | 19,589 (61.5%) ↑ | 2068 (6.5%) ↓ | 1190 (3.7%) | 1282 (4.0%) | 1593 (5.0%) | 25,722 (80.7%) |
| 2. Chronic | 774 (2.4%) ↓ | 746 (2.3%) ↑ | 220 (0.7%) | 129 (0.4%) | 325 (1.0%) ↑ | 2194 (6.9%) |
| 3. Developmentally limited | 1223 (3.8%) ↓ | 706 (2.2%) ↑ | 378 (1.2%) ↑ | 165 (0.5%) | 413 (1.3%) ↑ | 2885 (9.0%) |
| 4. Late onset | 466 (1.5%) ↓ | 223 (0.7%) | 56 (0.2%) | 156 (0.5%) ↑ | 170 (0.5%) | 1071 (3.4%) |
| Marginals | 22,052 (69.2%) | 3743 (11.7%) | 1844 (5.8%) | 1732 (5.4%) | 2501 (7.8%) | 31,872 |
Note. χ2(12, n = 31,872) = 3,683.51, p < 0.001; Φ = 0.34; Cramer's V = 0.20. Numbers with up arrows (↑) indicate values that are significantly greater than what would be expected by chance ("types") and numbers with down arrows (↓) indicate values that are significantly less than what would be expected by chance ("antitypes") based on a conservative chi-square value of 100.
Contributions to Comorbidity
Building on the identification of patterns of comordibity of smoking, heavy drinking, and marijuana use, we next turned to examining the extent to which risk factors accounted for comorbidity between the 3 substances, permitting us a window into the processes that contribute to the comorbidity. An important first step in these analyses was to consider whether the risk factors accounted for overall comorbidity (not by comorbid types). To do this in a straightforward manner, we used a series of least-squares analyses of variance that are appropriate for categorical data for each of our comorbid pairs. That is, we predicted the categorical heavy drinking class variable from the categorical smoking class variable, we predicted the heavy drinking class variable from the marijuana use class variable, and we predicted the marijuana use class variable from the smoking class variable. (We note that the converse associations, with the predictor and outcome variable switched, produced nearly identical results). We then included each risk factor in the model to determine the extent to which the association between heavy drinking and smoking diminished in the presence of the risk factor, the extent to which the association between heavy drinking and marijuana use diminished in the presence of the risk factor, and the extent to which the association between marijuana use and smoking diminished in the presence of the risk factor. This was conducted univariately due to the differing number of participants and nonoverlapping samples for each risk factor (as discussed previously, some risk factors were gathered on only random subgroups of the total sample). Table 6 portrays the associations in the presence of the risk factors (and, as comparison, the associations with no risk factor in the model). Comorbidity associations were reduced in the presence of the risk factors, particularly delinquency and positive reinforcement alcohol expectancies. All pairwise chi-square difference tests between the full model and the model excluding the covariate were significant at p < 0.001 with the following exceptions: depression, which was significant at p < 0.05 for the alcohol-tobacco association, was significant at p < 0.01 for the tobacco-marijuana association, and did not significantly reduce the alcohol-marijuana association, and parent education, which did not significantly reduce the alcohol-tobacco association.
Table 6.
Chi-Square Values Showing Prediction of Comorbidity Between Categorical Latent Class Substance Use Variables by Risk Factors
| Drinking and smokinga | Drinking and marijuana useb | Marijuana use and smokinga | |
|---|---|---|---|
| No covariates, total sample (n = 31,853 to 31,869) | 2328.05 | 3538.31 | 3205.63 |
| No covariates, subsample with delinquency (n = 7,771 to 7,777) | 664.35 | 844.22 | 854.39 |
| No covariates, subsample with alcohol expectancies (n = 4,788 to 4,793) | 259.90 | 490.62 | 442.99 |
| No covariates, subsample with depressive affect and sensation seeking (n = 1,742 to 1,747) | 143.67 | 140.04 | 199.66 |
| Sex (n = 31,804 to 31,823) | 2454.15 | 3073.48 | 3265.70 |
| Delinquency (n = 7,771 to 7,777) | 552.07 | 582.11 | 738.19 |
| Sensation seeking (n = 1,742 to 1,747) | 119.12 | 116.70 | 183.29 |
| Neg reinforce alcohol expect (n = 4,788 to 4,793) | 231.82 | 476.06 | 426.95 |
| Pos reinforce alcohol expect (n = 4,788 to 4,793) | 173.84 | 332.94 | 341.20 |
| Depressive affect (n = 1,742 to 1,747) | 139.01 | 136.58 | 192.41 |
| Religion (n = 31,633 to 31,651) | 1910.35 | 2945.69 | 2637.51 |
| Academic achievement (n = 31,106 to 31,121) | 1964.67 | 3176.43 | 2665.68 |
| Parent education (n = 30,972 to 30,991) | 2326.47 | 3407.84 | 3127.60 |
| Race (n = 31,603 to 31,624) | 2133.26 | 3378.54 | 3047.61 |
Note. Chi-square values were obtained from least-squares analyses of variance for categorical data, with the first term predicted by the second term (e.g., in Column 1, smoking predicted drinking). Note that models with the converse associations yielded virtually identical values. All chi-square values are significant at p < 0.001. All pairwise chi-square difference tests between the full model and the model excluding the covariate are significant at p < 0.001 with the exception of parent education, which did not significantly reduce the alcohol-tobacco association, and depression, which was significant at p < 0.05 for the alcohol-tobacco association, was significant at p < 0.01 for the tobacco-marijuana association, and did not significantly reduce the alcohol-marijuana association.
df = 12
df = 9.
Although it is interesting to understand that a given risk factor can account for comorbidity between 2 substances, it is not informative if we wish to determine the risk factor's influence on specific combinations of comorbidity. Thus, in our second step, we sought to determine the extent to which risk factors accounted for significant types (i.e., combinations that occurred at a rate greater than chance) observed in Tables 3-5. For example, does delinquency explain the correspondence between chronic drinking and chronic smoking? Does it explain the correspondence between chronic drinking and moderate smoking? We specifically focused on types and did not examine antitypes because from our perspective, accounting for configurations that occur at a rate greater than chance would take care of those that occur at a rate less than chance.
The analytic approach to answering these questions is somewhat complex, given the nominal nature of the substance use trajectories. As such, we coded group membership as a binary variable reflecting the class of interest for each substance (e.g., chronic drinking versus all others; developmentally limited drinking versus all others; late onset drinking versus all others, and so on), because binary variables can be analyzed by relatively standard analytic strategies, whereas nominal variables are difficult to analyze (particularly when both predictor and outcome variables are nominal in nature). We predicted the binary outcome variables from the binary predictors (with no covariates) using a series of logistic regressions; this is referred to as the “null model.” Specifically, we predicted binary drinking variables from binary smoking variables (e.g., predicting the binary chronic drinking variable from the binary chronic smoking variable), we predicted binary drinking variables from binary marijuana use variables, and we predicted binary marijuana use variables from binary smoking variables. Not surprisingly, we observed significant odds ratios (see Table 7, top panel) for each of these models (e.g., chronic smoking indeed predicted chronic drinking; odds ratio = 4.38).
Table 7.
Reduction of Comorbidity When Controlling for Risk Factors, as Portrayed by Odds Ratio (and Standardized Logistic Beta) for the Prediction of a Given Substance Use Trajectory Class From Another Substance Use Trajectory Class
| Chronic drink, chronic smoke | Dev Ltd drink, Dev Ltd smoke | Late onset drink, late onset smoke | Chronic drink, moderate smoke | Dev Ltd drink, chronic smoke | ||
|---|---|---|---|---|---|---|
| Drinking and smoking No covariates | 4.38 (0.22) | 4.02 (0.15) | 4.77 (0.16) | 3.13 (0.14) | 3.02 (0.16) | |
| Sex | 4.79 (0.23) | 4.05 (0.15) | 4.73 (0.16) | 3.75 (0.16) | 3.01 (0.16) | |
| Delinquency | 3.10 (0.19)a | 3.36 (0.14) | 4.33 (0.17) | 1.99 (0.10)a | 2.08 (0.12)a | |
| Sensation seek | 2.47 (0.13)a | 3.42 (0.15) | 4.33 (0.18) | 3.29 (0.17) | 2.45 (0.13) | |
| Neg Alc expect | 3.20 (0.18)a | 3.27 (0.13) | 4.42 (0.16) | 2.91 (0.14) | 2.52 (0.15) | |
| Pos Alc expect | 2.95 (0.17)a | 3.07 (0.13) | 4.40 (0.16) | 2.83 (0.14) | 2.37 (0.14) | |
| Depress affect | 2.82 (0.15) | 3.58 (0.16) | 4.47 (0.18) | 3.45 (0.18) | 2.68 (0.14) | |
| Religion | 2.82 (0.17)a | 2.73 (0.12)a | 3.50 (0.15)a | 2.17 (0.11)a | 1.97 (0.11)a | |
| Academic achievement | 4.32 (0.22) | 3.99 (0.15) | 4.76 (0.16) | 3.08 (0.14) | 3.01 (0.16) | |
| Parent education | 4.57 (0.22) | 3.97 (0.15) | 4.67 (0.16) | 3.10 (0.14) | 3.07 (0.17) | |
| Race | 3.91 (0.20) | 3.78 (0.14) | 4.62 (0.16) | 3.11 (0.14) | 2.70 (0.15) |
| |
Chronic drink, chronic use |
Dev Ltd drink, Dev Ltd use |
Late onset drink, late onset use |
Chronic drink, Dev Ltd use |
Chronic drink, late onset use |
|
|---|---|---|---|---|---|---|
| Drinking and marijuana use No covariates | 8.62 (0.25) | 5.11 (0.21) | 4.67 (0.12) | 4.48 (0.20) | 3.89 (0.11) | |
| Sex | 7.86 (0.24) | 5.09 (0.21) | 4.47 (0.12) | 4.55 (0.20) | 3.74 (0.11) | |
| Delinquency | 5.28 (0.21)a | 3.19 (0.17)a | 3.13 (0.11) | 2.37 (0.12)a | 2.95 (0.10) | |
| Sensation seek | 4.79 (0.16) | 3.88 (0.16) | 2.70 (0.10) | 2.72 (0.12) | 4.10 (0.14) | |
| Neg Alc expect | 6.60 (0.24) | 4.08 (0.20) | 4.66 (0.13) | 4.01 (0.20) | 2.91 (0.09) | |
| Pos Alc expect | 5.50 (0.22)a | 3.62 (0.18)a | 4.63 (0.13) | 3.34 (0.17) | 2.80 (0.09) | |
| Depress affect | 5.44 (0.18) | 4.23 (0.17) | 2.81 (0.10) | 3.10 (0.14) | 4.33 (0.14) | |
| Religion | 5.43 (0.22)a | 3.37 (0.18)a | 3.38 (0.11)a | 2.89 (0.16)a | 2.64 (0.09)a | |
| Academic achievement | 8.42 (0.24) | 5.07 (0.21) | 4.65 (0.12) | 4.44 (0.19) | 3.83 (0.11) | |
| Parent education | 8.46 (0.24) | 4.99 (0.21) | 4.60 (0.12) | 4.42 (0.19) | 3.82 (0.11) | |
| Race | 8.04 (0.24) | 4.87 (0.21) | 4.52 (0.12) | 4.21 (0.19) | 3.69 (0.11) |
| Chronic use, chronic smoke | Dev Ltd use, Dev Ltd smoke | Late onset use, late onset Smoke | Chronic use, moderate smoke | Dev Ltd use, chronic smoke | Dev Ltd use, moderate smoke | |
|---|---|---|---|---|---|---|
| Marijuana use and smoking No covariates | 7.42 (0.29) | 4.54 (0.16 | 4.98 (0.16) | 3.52 (0.15 | 4.55 (0.22) | 3.48 (0.15) |
| Sex | 7.80 (0.30) | 4.60 (0.16) | 4.88 (0.16) | 3.88 (0.17) | 4.58 (0.22) | 3.56 (0.16) |
| Delinquency | 5.49 (0.28)a | 3.10 (0.13)a | 4.91 (0.19) | 2.04 (0.10)a | 3.46 (0.20) | 2.65 (0.14) |
| Sensation seek | 7.72 (0.29) | 2.67 (0.12) | 6.78 (0.23) | 2.09 (0.11) | 3.85 (0.19) | 4.18 (0.20) |
| Neg Alc expect | 6.38 (0.29) | 4.10 (0.16) | 4.45 (0.16) | 2.90 (0.14) | 3.78 (0.21) | 2.53 (0.12) |
| Pos Alc expect | 5.82 (0.28) | 3.75 (0.15) | 4.39 (0.16) | 2.75 (0.13) | 3.46 (0.20) | 2.42 (0.12) |
| Depress affect | 8.12 (0.30) | 2.81 (0.13) | 6.96 (0.24) | 2.14 (0.11) | 4.09 (0.20) | 4.31 (0.21) |
| Religion | 4.60 (0.25)a | 3.04 (0.13)a | 3.65 (0.15) | 2.46 (0.12)a | 2.89 (0.18)a | 2.42 (0.12)a |
| Academic Ach | 7.07 (0.29) | 4.33 (0.15) | 5.02 (0.17) | 3.44 (0.15) | 4.43 (0.22) | 3.42 (0.15) |
| Parent education | 7.51 (0.30) | 4.45 (0.16) | 5.07 (0.17) | 3.47 (0.15) | 4.60 (0.22) | 3.46 (0.15) |
| Race | 6.81 (0.29) | 4.29 (0.15) | 4.79 (0.16) | 3.47 (0.15) | 4.23 (0.21) | 3.47 (0.15) |
Note. Parameters with superscript indicate a model with a nonoverlapping 95% confidence interval (not shown) with the odds ratio for the model with no covariates.
Next, analogous logistic regressions were estimated with risk factors univariately controlled. Odds ratios (OR) and standardized betas were calculated (see Table 7), and 95% confidence intervals around the OR were computed (not shown). Confidence intervals that were nonoverlapping with the null model were identified and are portrayed in Table 7 using superscripts; these indicate that the OR for the model with the covariate was significantly different (in all cases, lower) than the OR for the null model. We believed this to be a conservative approach, given that they are separated by an interval reflecting 2 standard errors in 1 model and 2 standard errors on the other model.
For drinking and smoking, we had identified 5 types which occur at a rate more frequently than chance (CHR DR-CHR SMK; DV LTD DR-DV LTD SMK; LATE DR-LATE SMK, CHR DRK-MOD SMK; and DV LTD DRK-CHR SMK).The OR for CHR DR-CHR SMK was significantly reduced when the following risk factors were controlled: delinquency, sensation seeking, both positive and negative reinforcement alcohol expectancies, and religion. The ORs for CHR DRK-MOD SMK; DV LTD DRK-CHR SMK were significantly reduced when delinquency and religion were controlled. Finally, the ORs for DV LTD DR-DV LTD SMK and for LATE DR-LATE SMK were significantly reduced only when religion was controlled.
For drinking and marijuana use, we had identified 5 types (CHR DR-CHR MJ; DV LTD DR-DV LTD MJ; LATE DR-LATE MJ, CHR DRK-DV LTD MJ; and CHR DRK-LATE MJ). The OR for CHR DR-CHR MJ was significantly reduced when delinquency, positive reinforcement alcohol expectancies, and religion were controlled. The ORs for DV LTD DR-DV LTD MJ and CHR DRK-DV LTD MJ were significantly reduced when delinquency and religion were controlled. Finally, the ORs for LATE DR-LATE MJ and CHR DRK-LATE MJ were significantly reduced when religion was controlled.
For marijuana use and smoking, we had identified 6 types (CHR MJ-CHR SMK; DV LTD MJ-DV LTD SMK; LATE MJ-LATE SMK; CHR MJ-MOD SMK; DV LTD MJ-CHR SMK; and DV LTD MJ-MOD SMK). The ORs for CHR MJ-CHR SMK; DV LTD MJ-DV LTD SMK, and CHR MJ-MOD SMK were significantly reduced when delinquency and religion were controlled. The ORs for DV LTD MJ-CHR SMK; and DV LTD MJ-MOD SMK were significantly reduced when religion was controlled.
CONCLUSIONS
Longitudinal comorbidity is among the least understood aspects of etiology of substance use (Sher et al., 2005); this gap is especially apparent during the transition to adulthood when there is considerable change in various types of substance use. In this study, our purpose was to describe and explain the comorbidity among trajectories of cigarette, alcohol, and marijuana use based on national panel data spanning ages 18 to 26. For all 3 substances, we identified 4 courses of emerging adulthood substance use while controlling for secular changes occurring over 2 decades: (i) low users, (ii) chronic users, (iii) late-onset users, and (iv) developmentally limited users. For the smoking class only, we also extracted a “moderate” group. These courses of substance use are largely consistent with those found in the literature. For heavy drinking, the developmentally limited class was the largest drinking class, in support of literature documenting a “maturing out” effect in heavy drinking towards the culmination of emerging adulthood (Bachman et al., 2002). Likewise, the largest class reporting marijuana use was the developmentally limited class, although it was not notably larger than the chronic class. For smoking, however, the chronic high class had the highest prevalence among the smoking classes, attesting to the highly addictive nature of tobacco. We also characterized comorbidity in a longitudinal context, demonstrating moderate levels of comorbidity between each of the trajectories of substance use and particular subtypes that may benefit from targeted intervention. Finally, we examined the extent to which etiologically relevant risk factors explained combinations of comorbidity.
Comorbidity Among Substances
Our cross-classification of alcohol and tobacco use showed the 2 substances to be moderately-to-strongly related. As might be expected by research showing a dose-dependent relation between smoking and drinking (Madden et al., 2000), low heavy-drinkers were least likely to smoke and chronic drinkers were most likely to smoke. In addition, individuals who persistently drank heavily or who drank heavily during early young adulthood (but later remitted) were most likely to be chronic smokers, again supporting the extent to which smoking is highly addictive (more so than alcohol or marijuana use; Merline et al., 2004). We also showed that those who drank persistently had a greater likelihood than would be expected by chance of being moderate smokers, or “chippers,” who may be smoking only while drinking. Course of alcohol and marijuana use exhibited even stronger comorbidity than conjoint drinking and smoking. Cross-substance trajectory concordance (agreement reflected by cells along the diagonal; 64%) was high, consistent with findings by Flory et al. (2004), who, despite dissimilarity in trajectory shape, found similar concordance rates for men (61%) and women (50%). Also, like chronic marijuana users, both developmentally limited and late-onset users were more likely to be chronic heavy drinkers. The association between developmentally limited marijuana users and chronic drinkers may be due to the commonality across the 2 substances such that (unlike smoking), drinking and marijuana use are each used to attain a feeling of feeling intoxicated or high; however, environmental constraints that arise during young adulthood such as a full-time career, family, and physical or social access may constrain use of marijuana more so than heavy drinking.
Finally, concordance between trajectories of marijuana and tobacco use was somewhat surprisingly as high as (if not higher than) the association between alcohol and tobacco use. Developmentally limited marijuana users were more likely to be chronic smokers, again supporting the idea that logistical factors may constrain the use of illicit more so than licit substances in later emerging adulthood (ages 22 to 26). In addition, those who used marijuana early (and either continued to do so or matured out of marijuana use) were more likely to be moderate smokers; perhaps these 2 substances are enjoyed for their social benefits among this subgroup.
The high concordance of trajectories along the diagonal has implications for similar developmental timing of use for different substances, perhaps due to the experience of developmental transitions (e.g., living situation, traditional roles associated with a new career and family) that have a common influence on use of different substances. In addition, these findings suggest that prevention and treatment efforts might better be directed to poly-substance use rather than targeting single substances alone. Interestingly, although findings in the literature support alcohol and tobacco as “gateway” drugs to illicit drug use (Kandel, 2002; Kandel and Yamaguchi, 1993; Peele and Brodsky, 1997), we did not find evidence for the Gateway Hypothesis in this age range, consistent with Labouvie and White (2002), who found that trajectories of smoking and drinking failed to predict subsequent substance use disorders. We were able to examine the extent to which use of alcohol or tobacco led to subsequent marijuana use by exploring the combinations of chronic or developmentally limited alcohol or tobacco use with late onset marijuana use. In none of these instances (across all 4 combinations) was a significant type evident, suggesting for this age range, use of licit drugs did not set the stage for subsequent illicit drug use. Perhaps by the mid-twenties, the Gateway effect is secondary to more situational constraints. It would be important to see this addressed in a younger sample, however.
Prescott and Kendler (1995) raise the question of whether much of the genetic covariation between alcohol and tobacco use may be due to the large group of abstainers; they found that shared (genetic) variation between alcohol and tobacco use was much reduced when abstainers were removed. In the current study, we examined the extent to which removing low users from our sample diminished the association between drinking and smoking group membership and found that analyses excluding the low heavy-drinking and low-smoking groups still showed a small-to-moderate association, suggesting that the alcohol-tobacco association is not an artifact of imposed covariation due to common factors in abstention/low levels of substance use. This was true also for the marijuana-tobacco association, although the relation between alcohol and marijuana appeared to be driven strongly by low users.
Prediction of Comorbidity by Risk Factors
Membership in trajectory groups of alcohol, tobacco use, and marijuana use may share risk factors, suggesting that comorbidity between these substances may be in part due to common risk factors. We explicitly examined the extent to which risk factors predicted comorbidity. All risk factors examined herein (sex, delinquency, sensation seeking, depressive affect, alcohol expectancies, religiosity, academic achievement, parent education, and race) accounted for general comorbidity to some degree, with religiosity, delinquency, sensation seeking, and positive reinforcement alcohol expectancies appearing to be the strongest predictors.
Expectancies about the positive effects of alcohol contributed only to the most severe configurations of comorbid substance use; that is, chronic high drinkers are more likely to be both chronic high smokers and, for positive reinforcement expectancies only, chronic high marijuana users, in part due to their expectations about the positive effects of alcohol. Although there is some generality across expectancies (Aarons et al., 2001), alcohol expectancies did not explain the tendency for chronic high marijuana users to be chronic high smokers, supporting some drug specificity as well. Unfortunately we did not have measures of tobacco or marijuana expectancies to explicitly test this.
Past-year delinquency also was a risk factor for the most severe configurations of comorbid substance use (reflected by chronic high users of each substance). Although only the association between chronic high drinking and smoking was significantly reduced in the presence of sensation seeking, there were clear reductions in other configurations of comorbidity that were similar in magnitude to delinquency; the lack of significance here is likely due to the low sample size for the sensation seeking analyses. These findings are consistent with Chassin et al. (2004) who demonstrated that impulsivity, a temperamental trait that is highly correlated with sensation seeking and delinquency, predicted membership in a co-occurring heavy drinking/heavy drug use class as well as in a comorbid alcohol and drug dependence class. The extent to which a course of marijuana use that was characterized by remission over the young adult years tracked drinking and smoking was also in part explained by high delinquency at age 18. That delinquent behavior and sensation seeking account for combinations of comorbidity characterized by early onset and persistently high use suggests that to some extent, individuals use multiple substances because of a common genetic vulnerability to use of substances and behavioral undercontrol (e.g., McGue and Iacono, 2005; McGue et al., 2006; Slutske et al., 1998; Zucker, 2006), rather than because use of 1 substance leads to use of another (e.g., cross-tolerance between drinking and smoking). These vulnerable individuals may be more susceptible to an environment that promotes substance use during emerging adulthood but constrains heavy use as the individual matures. Combinations of substance use that were characterized by later onset use, however, were not explained by delinquency, in line with work by Babor et al. (1992) hypothesizing the existence of a later-onset alcoholic (“Type A” alcoholism) whose course is not marked by symptoms of conduct disorder.
Although the findings failed to reach significance, depressive affect appeared to explain combinations of comorbidity with marijuana use. Again, this may be due to reduced power with the smaller subsample size; alternately, the low magnitude of associations with depressive affect may be in part because we assessed global depression, rather than specific episodes or symptoms of depression (e.g., anxiety) that might be differentially associated with substance use. Religiosity, an important protective factor in its own right as well as a proxy for conventionality, was the most prominent protective factor across many combinations of comorbidity, particularly for courses of substance use that tracked one another. We note, however, that the power to detect an effect was much higher in the models with religiosity as a covariate (as well as those with gender, parent education, and race) than with alcohol expectancies or delinquency. The tendency for chronic drinkers to smoke moderately and to use marijuana in a time-delimited fashion (developmentally limited or late onset) was in part due to religiosity, as was the association between developmentally limited drinking and chronic smoking, developmentally limited marijuana use and chronic smoking, and developmentally limited marijuana use and moderate smoking. Finally, the association between chronic marijuana use and moderate smoking was in part due to religiosity.
Unlike Chassin et al. (2004) and Orlando et al. (2005), who both noted that courses of multiple substance use characterized by heavy drinking/heavy drug use were more likely to comprise men, we found no evidence for sex as a risk factor for combinations of substance use that occurred at a rate more frequently than chance. The current study found no evidence for either parent education or race as a risk factor for any comorbid combinations, despite marked variability along these dimensions in the present nationally representative sample. Finally, there was little support for academic achievement as a risk factor for comorbidity during emerging adulthood; although this may be due in part to the normative excessive drinking that often occurs during college (thus blurring relationships between achievement and substance use), it also suggests that there may be directional (perhaps causal) associations between academic achievement and substance use as opposed to a common underlying propensity to use substances and to exhibit poor academic outcomes (Bachman et al., 2008).
Strengths and Limitations
Unlike much extant research, the current study utilized multi-wave data from a very large, nationally representative sample with multiple cohorts, allowing us to control for secular effects and generalize across historic period. Large representative samples permit identification of relatively rare subgroups reflecting unique comorbidity patterns, which is essential to advancing our understanding of the etiology and comorbidity of substance use. However, characteristics of the dataset also presented some limitations. Due to the heterogeneity in age, there was some overlap in age in adjacent waves (e.g., Time 1 includes 18 to 20 year olds, and Time 2 includes 20 to 22 year olds), so the results are not strictly interpretable by age. As is typical in longitudinal studies of substance use, attrition was differential with respect to variables important in this analysis such that those who were retained had lower high school substance use. This suggests that our findings reflect a more conservative population in terms of substance use. In addition, our sample over-represented females, Whites, and those with higher SES. Also, we were limited to risk factors that were available in the dataset (some of which had low-to-moderate reliability), and we were unable to examine risk factors in a multivariate fashion because the psychosocial scales were given to random, nonoverlapping subsamples of the full respondent sample. We caution that comorbidity between each of the substances may have been further reduced (explained) if other risk factors were considered (e.g., childhood life events, peer norms), and because of the need to conduct univariate analyses, a relatively large number of pair-wise comparisons were made without correction for multiple comparisons.
Although we applied a state-of-the-art analytic technique to characterize ordered trajectories of substance use, research suggests that this technique has drawbacks (Bauer and Curran, 2003; but see Muthén, 2003). We exercise caution in drawing conclusions from these data until the replicability of these findings is better established.
Describing the course of co-occurring behaviors is of recent interest to researchers in developmental psychopathology. Currently, 2 approaches have been taken: (i) models that simultaneously model multiple behaviors in a single multivariate analysis (dual trajectory model) and (ii) models that derive courses for each behavior separately and then model conjoint use by estimating concordance between each behavior (parallel process models). The first approach explicitly models comorbidity and its change over time. It may be more parsimonious; for example, whereas the 4 × 5 contingency tables presented here yield 20 combinations of comorbidity, fewer groupings may be sufficient (indeed, in our prior work examining trajectories of drinking and smoking using this technique, only 7 trajectories were identified). The second approach, however, provides estimates of comorbidity (i.e., concordance) that are similar to more traditional cross-sectional approaches (i.e., likelihood-based measures and measures of agreement such as Cohen's k). When considering 3 or more substances, we believe the univariate approach is more straightforward and more practicable. Finally, we struggled with the best way to identify factors that account for comorbidity. Categorical data such as nominal grouping variables often pose challenges, particularly when the data are nominal in nature.
In addition, we treated the ordinal substance use variables as pseudo-continuous in order to facilitate analysis. Although there are several ways to deal with nonnormal and categorical data in the area of latent growth modeling, including two-part growth modeling (Olsen and Schafer, 2001), the analytic techniques for trajectory modeling are still in their infancy and convergence problems are frequently encountered when estimating mixture models for count or censored variables. Finally, it is possible that the MAR assumption for modeling missing data in Mplus was not met, as previous attrition analyses with similar MTF panel samples have shown that those retained in the longitudinal sample were lower on senior year substance use than those who were excluded (e.g., Schulenberg et al., 1996a,b); unfortunately, there is no statistical test to determine if data are missing at random. Despite these limitations, the current study demonstrates the feasibility and substantive importance of modeling comorbidity and course within a person-centered approach to data analysis.
Acknowledgments
Portions of this paper were presented at the 112th Annual Convention of the American Psychological Association in Honolulu, HI. Preparation of the work was supported by National Institute on Alcohol Abuse and Alcoholism Grants AA12383 and AA13938 to Kristina M. Jackson. The Monitoring the Future project, from which the data were obtained, is funded by the National Institute on Drug Abuse Grant DA01411 to Lloyd D. Johnston. The findings and conclusions in this report are those of the authors and do not necessarily represent the views of the NIH.
Footnotes
We considered reporting a simultaneous cross-classification table but deemed it too burdensome, as it would consist of 80 cells (e.g., four 4 × 5 tables). We are unaware of any statistic that summarizes the association between 3 categorical variables.
REFERENCES
- Aarons GA, Brown SA, Stice E, Coe MT. Psychometric evaluation of the marijuana and stimulant effect expectancy questionnaires for adolescents. Addict Behav. 2001;26:219–236. doi: 10.1016/s0306-4603(00)00103-9. [DOI] [PubMed] [Google Scholar]
- Abroms L, Simons-Morton B, Haynie DL, Chen R. Psychosocial predictors of smoking trajectories during middle and high school. Addiction. 2005;100:852–861. doi: 10.1111/j.1360-0443.2005.01090.x. [DOI] [PubMed] [Google Scholar]
- Akaike H. Factor analysis and AIC. Psychometrika. 1987;52:317–332. [Google Scholar]
- Arnett JJ. Emerging adulthood: a theory of development from late teens through the twenties. Am Psychol. 2000;55:469–480. [PubMed] [Google Scholar]
- Audrain-McGovern J, Rodriguez D, Tercyak KP, Cuevas J, Rodgers K, Patterson F. Identifying and characterizing adolescent smoking trajectories. Cancer Epidemiol Biomarkers Prev. 2004;13:2023–2034. [PubMed] [Google Scholar]
- Babor TF, Hofmann M, Del Boca F, Hesselbrock V, Meyer R, Dolinsky Z, Rounsaville B. Types of alcoholics, I: evidence for an empirically-derived typology based on indicators of vulnerability and severity. Arch Gen Psychiatry. 1992;49:599–608. doi: 10.1001/archpsyc.1992.01820080007002. [DOI] [PubMed] [Google Scholar]
- Bachman JG, O'Malley PM, Schulenberg JE, Johnston LD, Bryant AL, Merline AC. The Decline of Substance Use in Young Adulthood: Changes in Social Activities, Roles, and Beliefs. Lawrence Erlbaum Associates; Mahwah, NJ: 2002. [Google Scholar]
- Bachman JG, O'Malley PM, Schulenberg JE, Johnston LD, Freedman-Doan P, Messersmith EE. The Education–Drug Use Connection: How Successes and Failures in School Relate to Adolescent Smoking, Drinking, Drug Use, and Delinquency. Lawrence Erlbaum Associates/Taylor & Francis; New York: 2008. [Google Scholar]
- Bachman JG, Wadsworth KN, O'Malley PM, Johnston LD, Schulenberg JE. Smoking, Drinking, and Drug Use in Young Adulthood: The Impacts of New Freedoms and New Responsibilities. Lawrence Erlbaum Associates; Mahwah, NJ: 1997. [Google Scholar]
- Baer JS, Kivlahan DR, Marlatt GA. High-risk drinking across the transition from high school to college. Alcohol Clin Exp Res. 1995;19:54–61. doi: 10.1111/j.1530-0277.1995.tb01472.x. [DOI] [PubMed] [Google Scholar]
- Bauer DJ, Curran PJ. Distributional assumptions of growth mixture models: implications for over-extraction of latent trajectory classes. Psychol Methods. 2003;8:338–363. doi: 10.1037/1082-989X.8.3.338. [DOI] [PubMed] [Google Scholar]
- Brown TL, Flory K, Lynam DR, Leukefeld C, Clayton RR. Comparing the developmental trajectories of marijuana use of African American and Caucasian adolescents: patterns, antecedents, and consequences. Exp Clin Psychopharmacol. 2004;12:47–56. doi: 10.1037/1064-1297.12.1.47. [DOI] [PubMed] [Google Scholar]
- Bryant AL, Schulenberg J, Bachman JG, O'Malley PM, Johnston LD. Understanding the links among school misbehavior, academic achievement, and cigarette use: A national panel study of adolescents. Prev Sci. 2000;1:71–87. doi: 10.1023/a:1010038130788. [DOI] [PubMed] [Google Scholar]
- Chassin L, Flora DB, King KM. Trajectories of alcohol and drug use and dependence from adolescence to adulthood: The effects of familial alcoholism and personality. J Abnorm Psychol. 2004;113:483–498. doi: 10.1037/0021-843X.113.4.483. [DOI] [PubMed] [Google Scholar]
- Chassin L, Pitts SC, Prost J. Binge drinking trajectories from adolescence to emerging adulthood in a high-risk sample: predictors and substance abuse outcomes. J Consult Clin Psychol. 2002;70:67–78. [PubMed] [Google Scholar]
- Chassin L, Presson CC, Pitts SC, Sherman SJ. The natural history of cigarette smoking from adolescence to adulthood in a Midwestern community sample: multiple trajectories and their psychosocial correlates. Health Psychol. 2000;19:223–231. [PubMed] [Google Scholar]
- Chung T, Maisto SA, Cornelius JR, Martin CS. Adolescents’ alcohol and drug use trajectories in the year following treatment. J Stud Alcohol. 2004;65:105–114. doi: 10.15288/jsa.2004.65.105. [DOI] [PubMed] [Google Scholar]
- Cohen P, Kasen S, Chen H, Hartmark C, Gordon K. Variations in patterns of developmental transmissions in the emerging adulthood period. Dev Psychol. 2003;39:657–669. doi: 10.1037/0012-1649.39.4.657. [DOI] [PubMed] [Google Scholar]
- Colder CR, Campbell RT, Ruel E, Richardson JL, Flay BR. A finite mixture model of growth trajectories of adolescent alcohol use: predictors and consequences. J Consult Clin Psychol. 2002;70:976–985. doi: 10.1037//0022-006x.70.4.976. [DOI] [PubMed] [Google Scholar]
- Colder CR, Mehta P, Balanda K, Campbell RT, Mayhew KP, Stanton WR, Pentz MA, Flay BR. Identifying trajectories of adolescent smoking: an application of latent growth mixture modeling. Health Psychol. 2001;20:127–135. doi: 10.1037//0278-6133.20.2.127. [DOI] [PubMed] [Google Scholar]
- Degenhardt L, Hall W, Lynskey M. Exploring the association between cannabis use and depression. Addiction. 2003;98:1493–1504. doi: 10.1046/j.1360-0443.2003.00437.x. [DOI] [PubMed] [Google Scholar]
- Donovan JE. Problem behavior theory and the explanation of adolescent marijuana use. J Drug Issues. 1996;26:375–401. [Google Scholar]
- Donovan JE, Jessor R. Structure of problem behavior in adolescence and young adulthood. J Consult Clin Psychol. 1985;53:890–904. doi: 10.1037//0022-006x.53.6.890. [DOI] [PubMed] [Google Scholar]
- Elkins IJ, King SM, McGue M, Iacono WG. Personality traits and the development of nicotine, alcohol, and illicit drug disorders: prospective links from adolescence to young adulthood. J Abnorm Psychol. 2006;115:26–39. doi: 10.1037/0021-843X.115.1.26. [DOI] [PubMed] [Google Scholar]
- Ellickson PL, Martino SC, Collins RL. Marijuana use from adolescence to young adulthood: multiple developmental trajectories and their associated outcomes. Health Psychol. 2004;23:299–307. doi: 10.1037/0278-6133.23.3.299. [DOI] [PubMed] [Google Scholar]
- von Eye A. Configural Frequency Analysis: Methods, Models, and Applications. Lawrence Erlbaum Associates; Mahwah, NJ: 2002. [Google Scholar]
- Flory K, Lynam D, Milich R, Leukefeld C, Clayton R. Early adolescent through young adult alcohol and marijuana use trajectories: early predictors, young adult outcomes, and predictive utility. Dev Psychopathol. 2004;16:193–213. doi: 10.1017/s0954579404044475. [DOI] [PubMed] [Google Scholar]
- Fothergill KE, Ensminger ME. Childhood and adolescent antecedents of drug and alcohol problems: a longitudinal study. Drug Alcohol Depend. 2006;82:61–76. doi: 10.1016/j.drugalcdep.2005.08.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hallfors D, Cho H, Brodish PH. Identifying high school students ‘at risk’ for substance use and other behavioral problems: implications for prevention. Subst Use Misuse. 2006;41:1–15. doi: 10.1080/10826080500318509. [DOI] [PubMed] [Google Scholar]
- Hawkins JD, Catalano RF, Miller JY. Risk and protective factors for alcohol and other drug problems in adolescence and early adulthood: implications for substance abuse prevention. Psychol Bull. 1992;112:64–105. doi: 10.1037/0033-2909.112.1.64. [DOI] [PubMed] [Google Scholar]
- Hays RD, Widaman KF, DiMatteo MR, Stacy AW. Structural-equation models of current drug use: are appropriate models so simple(x)? J Pers Soc Psychol. 1987;52:134–144. doi: 10.1037//0022-3514.52.1.134. [DOI] [PubMed] [Google Scholar]
- Hill KG, White HR, Chung I-J, Hawkins JD, Catalano RF. Early adult outcomes of adolescent binge drinking: person- and variable-centered analyses of binge drinking trajectories. Alcohol Clin Exp Res. 2000;24:892–901. [PMC free article] [PubMed] [Google Scholar]
- Istvan J, Matarazzo JD. Tobacco, alcohol, and caffeine use: a review of their relationships. Psychol Bull. 1984;95:301–326. [PubMed] [Google Scholar]
- Jackson KM, Sher KJ. Similarities and differences of longitudinal phenotypes across alternate indices of alcohol involvement: a methodologic comparison of trajectory approaches. Psychol Addict Behav. 2005;19:339–351. doi: 10.1037/0893-164X.19.4.339. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jackson KM, Sher KJ, Schulenberg JE. Conjoint developmental trajectories of young adult alcohol and tobacco use. J Abnorm Psychol. 2005;114:612–626. doi: 10.1037/0021-843X.114.4.612. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jackson KM, Sher KJ, Wood PK. Trajectories of conjoint substance use disorders: a developmental, typological approach to comorbidity. Alcohol Clin Exp Res. 2000a;24:902–913. [PubMed] [Google Scholar]
- Johnston LD, O'Malley PM. Issues of validity and population coverage in student surveys of drug use. In: Rouse BA, Kozel NJ, Richards LG, editors. Self-Report Methods of Estimating Drug Use: Meeting Current Challenges to Validity. National Institute on Drug Abuse; Washington, DC: 1985. pp. 31–54. NIDA Research Monograph No. 57. [PubMed] [Google Scholar]
- Johnston LD, O'Malley PM, Bachman JG, Schulenberg JE. Monitoring the Future National Survey Results on Drug Use, 1975−2006. Volume II: College Students and Adults Ages 19−45. National Institute on Drug Abuse; Bethesda, MD: 2007. NIH Publication No. 07−6206. [Google Scholar]
- Jones BT, Corbin W, Fromme K. A review of expectancy theory and alcohol consumption. Addiction. 2001;96:57–72. doi: 10.1046/j.1360-0443.2001.961575.x. [DOI] [PubMed] [Google Scholar]
- Juon H-S, Ensminger ME, Sydnor KD. A longitudinal study of developmental trajectories to young adult cigarette smoking. Drug Alcohol Depend. 2002;66:303–314. doi: 10.1016/s0376-8716(02)00008-x. [DOI] [PubMed] [Google Scholar]
- Kandel DB. Stages and Pathways of Drug Involvement: Examining the Gateway Hypothesis. Cambridge University Press; New York, NY: 2002. [Google Scholar]
- Kandel DB, Chen K. Types of marijuana users by longitudinal course. J Stud Alcohol. 2000;61:367–378. doi: 10.15288/jsa.2000.61.367. [DOI] [PubMed] [Google Scholar]
- Kandel D, Yamaguchi K. From beer to crack: developmental patterns of drug involvement. Am J Public Health. 1993;83:851–855. doi: 10.2105/ajph.83.6.851. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kassel JD, Veilleux JC, Wardle MC, Yates MC, Greenstein JE, Evatt DP, Roesch LL. Negative affect and addiction. In: al'Absi M, editor. Stress and Addiction: Biological and Psychological Mechanisms. Elsevier Academic Press; San Diego, CA: 2007. pp. 171–189. [Google Scholar]
- Labouvie E, White HR. Drug sequences, age of onset, and use trajectories as predictors of drug abuse/dependence in young adulthood. In: Kandel DB, editor. Stages and Pathways of Drug Involvement: Examining the Gateway Hypothesis. Cambridge University Press; New York, NY: 2002. pp. 19–41. [Google Scholar]
- Lo Y, Mendell N, Rubin DB. Testing the number of components in a normal mixture. Biometrika. 2001;88:767–778. [Google Scholar]
- Madden PAF, Bucholz KK, Martin NG, Heath AC. Smoking and the genetic contribution to alcohol-dependence risk. Alcohol Health Res World. 2000;24:209–214. [PMC free article] [PubMed] [Google Scholar]
- McGue M, Iacono WG. The association of early adolescent problem behavior with adult psychopathology. Am J Psychiatry. 2005;162:1118–1124. doi: 10.1176/appi.ajp.162.6.1118. [DOI] [PubMed] [Google Scholar]
- McGue M, Iacono WG, Krueger RF. The association of early adolescent problem behavior and adult psychopathology: a multivariate behavioral genetic perspective. Behav Genet. 2006;36:591–602. doi: 10.1007/s10519-006-9061-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Merline AC, O'Malley PM, Schulenberg JE, Bachman JG, Johnston LD. Substance use among adults 35 years of age: prevalence, adulthood predictors, and impact of adolescent substance use. Am J Public Health. 2004;94:96–102. doi: 10.2105/ajph.94.1.96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miller WR. Researching the spiritual dimensions of alcohol and other drug problems. Addiction. 1998;93:979–990. doi: 10.1046/j.1360-0443.1998.9379793.x. [DOI] [PubMed] [Google Scholar]
- Muthén B. Second-generation structural equation modeling with a combination of categorical and continuous latent variables: new opportunities for latent class-latent growth modeling. In: Collins LM, Sayer AG, editors. New Methods for the Analysis of Change. Decade of Behavior. American Psychological Association; Washington, DC: 2001. pp. 291–322. [Google Scholar]
- Muthén BO. Statistical and substantive checking in growth mixture modeling: comment on Bauer and Curran. Psychol Methods. 2003;8:369–377. doi: 10.1037/1082-989X.8.3.369. [DOI] [PubMed] [Google Scholar]
- Muthén B. Latent variable analysis: growth mixture modeling and related techniques for longitudinal data. In: Kaplan D, editor. Handbook of Quantitative Methodology for the Social Sciences. Sage Publications; Newbury Park, CA: 2004. pp. 345–368. [Google Scholar]
- Muthén B, Brown CH, Masyn K, Jo B, Khoo ST, Yang CC, Wang CP, Kellam SG, Carlin JB, Liao J. General growth mixture modeling for randomized preventive interventions. Biostatistics. 2002;3:459–475. doi: 10.1093/biostatistics/3.4.459. [DOI] [PubMed] [Google Scholar]
- Muthén LK, Muthén BO. Mplus User's Guide. 3rd ed. Mutheń and Muthén; Los Angeles, CA: 1998−2004. [Google Scholar]
- Muthén B, Shedden K. Finite mixture modeling with mixture outcomes using the EM algorithm. Biometrics. 1999;55:463–469. doi: 10.1111/j.0006-341x.1999.00463.x. [DOI] [PubMed] [Google Scholar]
- Nagin DS. Analyzing developmental trajectories: a semiparametric, group-based approach. Psychol Methods. 1999;4:139–157. doi: 10.1037/1082-989x.6.1.18. [DOI] [PubMed] [Google Scholar]
- Nagin D, Land K. Age, criminal careers, and population heterogeneity: specification and estimation of a nonparametric, mixed Poisson model. Criminology. 1993;31:327–362. [Google Scholar]
- O'Malley PM, Bachman JG, Johnston LD. Reliability and consistency of self-reports of drug use. Int J Addict. 1983;18:805–824. doi: 10.3109/10826088309033049. [DOI] [PubMed] [Google Scholar]
- Oesterle S, Hill KG, Hawkins JD, Guo J, Catalano RF, Abbott RD. Adolescent heavy episodic drinking trajectories and health in young adulthood. J Stud Alcohol. 2004;65:204–212. doi: 10.15288/jsa.2004.65.204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Olsen MK, Schafer JL. A two-part random effects model for semicontinuous longitudinal data. J Am Stat Assoc. 2001;96:730–745. [Google Scholar]
- Orlando M, Tucker JS, Ellickson PL, Klein DJ. Developmental trajectories of cigarette smoking and their correlates from early adolescence to young adulthood. J Consult Clin Psychol. 2004;27:400–410. doi: 10.1037/0022-006X.72.3.400. [DOI] [PubMed] [Google Scholar]
- Orlando M, Tucker JS, Ellickson PL, Klein DJ. Concurrent use of alcohol and cigarettes from adolescence to young adulthood: an examination of developmental trajectories and outcomes. Subst Use Misuse. 2005;40:1051–1069. doi: 10.1081/JA-200030789. [DOI] [PubMed] [Google Scholar]
- Peele S, Brodsky A. Gateway to nowhere: how alcohol came to be scapegoated for drug abuse. Addict Res. 1997;5:419–426. [Google Scholar]
- Pickens RW, Svikis DS, McGue M, LaBuda MC. Common genetic mechanisms in alcohol, drug, and mental disorder comorbidity. Drug Alcohol Depend. 1995;39:129–138. doi: 10.1016/0376-8716(95)01151-n. [DOI] [PubMed] [Google Scholar]
- Prescott CA, Kendler KS. Genetic and environmental influences on alcohol and tobacco dependence among women. In: Fertig JB, Allen JP, editors. Alcohol and Tobacco: From Basic Science to Clinical Practice. U.S. Department of Health and Human Services; Bethesda, MD: 1995. pp. 59–87. NIAAA Research Monograph No. 30. [Google Scholar]
- Rostosky SS, Danner F, Riggle EDB. Is religiosity a protective factor against substance use in young adulthood? Only if you're straight! J Adolesc Health. 2007;40:440–447. doi: 10.1016/j.jadohealth.2006.11.144. [DOI] [PubMed] [Google Scholar]
- Schulenberg JE, Bryant AL, O'Malley PM. Taking hold of some kind of life: how developmental tasks relate to trajectories of well-being during the transition to adulthood. Dev Psychopathol. 2004;16:1119–1140. doi: 10.1017/s0954579404040167. [DOI] [PubMed] [Google Scholar]
- Schulenberg JE, Maggs JL. A developmental perspective on alcohol use and heavy drinking during adolescence and the transition to young adulthood. J Stud Alcohol Suppl. 2002;14:54–70. doi: 10.15288/jsas.2002.s14.54. [DOI] [PubMed] [Google Scholar]
- Schulenberg JE, Maggs JM, O'Malley PM. How and why the understanding of developmental continuity and discontinuity is important: the sample case of long-term consequences of adolescent substance use. In: Mortimer JT, Shanahan MJ, editors. Handbook of the Life Course. Plenum Publishers; New York: 2003. pp. 413–436. [Google Scholar]
- Schulenberg J, Merline AC, Johnston LD, O'Malley PM, Bachman JG, Laetz VB. Trajectories of marijuana use during the transition to adulthood: the big picture based on national panel data. J Drug Issues. 2005;35:255–280. doi: 10.1177/002204260503500203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schulenberg J, O'Malley PM, Bachman JG, Wadsworth KN, Johnston LD. Getting drunk and growing up: trajectories of frequent binge drinking during the transition to young adulthood. J Stud Alcohol. 1996a;57:289–304. doi: 10.15288/jsa.1996.57.289. [DOI] [PubMed] [Google Scholar]
- Schulenberg J, Wadsworth KN, O'Malley PM, Bachman JG, Johnston LD. Adolescent risk factors for binge drinking during the transition to young adulthood: variable- and pattern-centered approaches to change. Dev Psychol. 1996b;32:659–674. [Google Scholar]
- Schwarz G. Estimating the dimension of a model. Ann Stat. 1978;6:461–464. [Google Scholar]
- Sher KJ, Gotham HJ. Pathological alcohol involvement: a developmental disorder of young adulthood. Dev Psychopathol. 1999;11:933–956. doi: 10.1017/s0954579499002394. [DOI] [PubMed] [Google Scholar]
- Sher KJ, Grekin ER, Williams NA. The development of alcohol use disorders. Annu Rev Clin Psychol. 2005;1:493–523. doi: 10.1146/annurev.clinpsy.1.102803.144107. [DOI] [PubMed] [Google Scholar]
- Slutske WS, Heath AC, Dinwiddie SH, Madden PAF, Bucholz KK, Dunne MP, Statham DJ, Martin NG. Common genetic risk factors for conduct disorder and alcohol dependence. J Abnorm Psychol. 1998;107:363–374. doi: 10.1037//0021-843x.107.3.363. [DOI] [PubMed] [Google Scholar]
- Soldz S, Cui X. Pathways through adolescent smoking: a 7-year longitudinal grouping analysis. Health Psychol. 2002;21:495–504. [PubMed] [Google Scholar]
- Stacy A, Galaif ER, Sussman S, Dent CW. Self-generated drug outcomes in high-risk adolescents. Psychol Addict Behav. 1996;10:18–27. [Google Scholar]
- Stanton WR, Flay BR, Colder CR, Mehta P. Identifying and predicting adolescent smokers’ developmental trajectories. Nicotine Tob Res. 2004;6:843–852. doi: 10.1080/14622200410001734076. [DOI] [PubMed] [Google Scholar]
- Substance Abuse and Mental Health Services Administration . Results from the 2006 National Survey on Drug Use and Health: National Findings. Substance Abuse and Mental Health Services Administration; Rockville, MD: 2007. (Office of Applied Studies, NSDUH Series H-32, DHHS Publication No. SMA 07−4293)
- True WR, Xian H, Scherrer JF, Madden PAF, Bucholz KK, Heath AC, Eisen SA, Lyons MJ, Goldberg J, Tsuang M. Common genetic vulnerability for nicotine and alcohol dependence in men. Arch Gen Psychiatry. 1999;56:655–661. doi: 10.1001/archpsyc.56.7.655. [DOI] [PubMed] [Google Scholar]
- Trull TJ, Sher KJ. Relationship between the five-factor model of personality and Axis I disorders in a nonclinical sample. J Abnorm Psychol. 1994;103:350–360. doi: 10.1037//0021-843x.103.2.350. [DOI] [PubMed] [Google Scholar]
- Tucker JS, Ellickson PL, Orlando M, Klein DJ. Cigarette smoking from adolescence to young adulthood: Women's developmental trajectories and associated outcomes. Wom Health Issues. 2006;16:30–37. doi: 10.1016/j.whi.2005.08.004. [DOI] [PubMed] [Google Scholar]
- Tucker JS, Ellickson PL, Orlando M, Martino SC, Klein DJ. Substance use trajectories from early adolescence to emerging adulthood: a comparison of smoking, binge drinking, and marijuana use. J Drug Issues. 2005;35:307–332. [Google Scholar]
- Tucker JS, Orlando M, Ellickson PL. Patterns and correlates of binge drinking trajectories from early adolescence to young adulthood. Health Psychol. 2003;22:79–87. doi: 10.1037//0278-6133.22.1.79. [DOI] [PubMed] [Google Scholar]
- Wallace JM, Jr, Yamaguchi R, Bachman JG, O'Malley PM, Schulenberg JE, Johnston LD. Religiosity and adolescent substance use: the role of individual and contextual influences. Soc Probl. 2007;54:308–327. [Google Scholar]
- White HR, Pandina RJ, Chen P. Developmental trajectories of cigarette use from early adolescence into young adulthood. Drug Alcohol Depend. 2002;65:167–178. doi: 10.1016/s0376-8716(01)00159-4. [DOI] [PubMed] [Google Scholar]
- Wills TA, McNamara G, Vaccaro D. Parental education related to adolescent stress-coping and substance use: development of a mediational model. Health Psychol. 1995;14:464–478. doi: 10.1037//0278-6133.14.5.464. [DOI] [PubMed] [Google Scholar]
- Wills TA, Resko JA, Ainette MG, Mendoza D. Smoking onset in adolescence: A person-centered analysis with time-varying predictors. Health Psychol. 2004;23:158–167. doi: 10.1037/0278-6133.23.2.158. [DOI] [PubMed] [Google Scholar]
- Windle M. A longitudinal study of antisocial behaviors in early adolescence as predictors of late adolescent substance use: Gender and ethnic group differences. J Abnorm Psychol. 1990;99:86–91. doi: 10.1037//0021-843x.99.1.86. [DOI] [PubMed] [Google Scholar]
- Windle M, Mun EY, Windle RC. Adolescent-to-young adulthood heavy drinking trajectories and their prospective predictors. J Stud Alcohol. 2005;66:313–322. doi: 10.15288/jsa.2005.66.313. [DOI] [PubMed] [Google Scholar]
- Windle M, Wiesner M. Trajectories of marijuana use from adolescence to young adulthood: predictors and outcomes. Dev Psychopathol. 2004;16:1007–1027. doi: 10.1017/s0954579404040118. [DOI] [PubMed] [Google Scholar]
- Zucker RA. Alcohol use and the alcohol use disorders: a developmental-biopsychosocial systems formulation covering the life course. In: Cicchetti D, Cohen DJ, editors. Developmental Psychopathology. 2nd ed Vol. 3. Wiley; Hoboken, NJ: 2006. pp. 620–656. Risk, Disorder, and Adaptation