

Abstract
Neuroendocrine tumors are rare entities which can arise in various sites of the body. The presence of both neural and endocrine elements in conjunction characterises these tumors pathologically. Most of these tumors are non secretory in nature, and arise in organs where there may not be any neuroendocrine elements. Carcinoid tumors are the most common entities reported in the kidney. There have been only a couple of case series of non-carcinoid neuroendocrine tumors of the kidney reported in literature. Surgical resection appears to be the best available treatment modality. Chemotherapy has been attempted with dismal results. The biological behaviour is determined by the occurrence of metastases to the liver or lung. We report a patient with a large cell neuroendocrine carcinoma of the kidney, who underwent radical resection and is doing well on follow-up. The diagnosis was confirmed by immune-histochemistry.
Keywords: Immuno histochemistry, kidney, neuroendocrine tumors
INTRODUCTION
Neuroendocrine neoplasms are uncommon tumors of the kidney that may arise in various organs and tissues, including in those that do not normally contain neuroendocrine cells.[1] These tumors are characterized by the presence of a neural and an epithelial component in conjunction with each other. The biological behavior of these tumors ranges over a spectrum, and can only be judged accurately by their metastatic tendency. There have been only a couple of series of such tumors of the kidney reported in literature. We report here a case of a large-cell neuroendocrine carcinoma (LCNEC) of the kidney with appropriate immunohistochemistry.
CASE REPORT
A 40-year-old lady presented with an asymptomatic right-sided renal mass. Imaging of the abdomen revealed a renal tumor, abutting the undersurface of the right lobe of the liver with a thrombus in the renal vein. The patient underwent a right radical nephrectomy after due preparations. Resection of a portion of the right diaphragmatic crus and of the renal vein thrombus was done. Gross examination revealed a lobulated, firm, grey-white tumor along with necrosis and a renal vein thrombus. Microscopy evidence indicated the composition of trabeculae, pseudorosettes, and strands of medium-to-large-sized tumor cells possessing moderate eosinophilic cytoplasm and vesicular nuclei in the tumor lobules. The nuclei had fine chromatin and prominent nucleoli and the cells were separated by a fibrovascular stroma. Mitotic count was >20 per 10 high-power fields [Figure 1].
Figure 1.
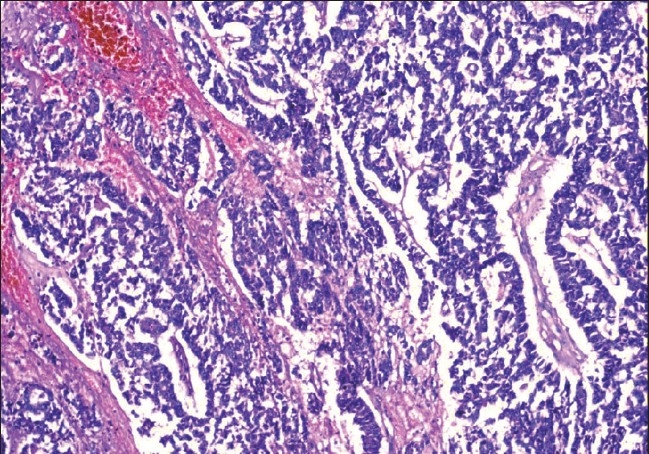
Ribbons and cords of tumor cells separated by stroma (H and E, ×10)
Immunohistochemistry revealed positive staining (>10 high-power fields) for cytokeratin, neuron-specific enolase (NSE), chromogranin A, and synaptophysin, and negative staining for vimentin [Figure 2].
Figure 2.
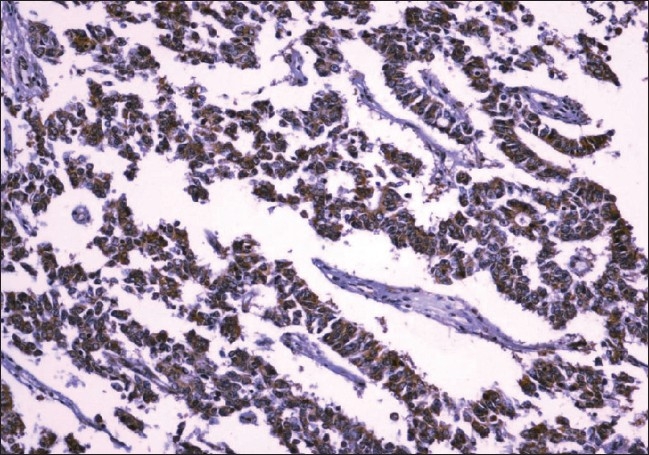
Tumor cells positive for chromogranin (IHC, ×40)
On the basis of these results, a diagnosis of LCNEC was made. The patient has completed one year of follow-up and remains disease-free at the time of this report.
DISCUSSION
The neuroendocrine tumors (NETs) represent a spectrum of diseases with varying aggressiveness. These tumors can be admixed with other histological types such as adenocarcinoma or squamous cell carcinoma. Neuroendocrine tumors of the kidney are rare with LCNEC being even more uncommon. There have been only a couple of series of renal LCNEC reported in the English literature.[2,3]
The nomenclature and classification of NETs at different sites (lung, GI tract), remains controversial. The recent WHO classification of NETs is as follows: well-differentiated NET (carcinoid), well-differentiated neuroendocrine carcinoma (atypical carcinoid), and poorly differentiated neuroendocrine carcinomas (small cell carcinoma) and LCNEC.[4] The histologic appearance combined with mitotic rate helps distinguish them from one another.
Renal NETs occur in older patients and show no sex predilection. The renal NET patients present with hematuria and abdominal pain, and the tumors are typically advanced at the time of diagnosis. Grossly, the tumor appears lobulated with a tan or grey cut surface. Focal necrosis and hemorrhage are common.[5]
Microscopically, LCNEC is composed of tumor cells that are arranged in organoid nests, trabeculae, rosette-like, and palisading patterns. The tumor cells are large with moderate-to-abundant cytoplasm. The nuclei are vesicular with granular chromatin and prominent nucleoli. Mitotic rate is usually ≥10 per 10 high-power fields.[5] Immunohistochemistry shows positivity for NSE, chromogranin A, synaptophysin, and Leu 7 (CD57).
An LCNEC can be mistaken for a high-grade renal cell carcinoma or urothelial carcinoma.[6] Immunohistochemistry comes to the rescue, with at least one of the neuroendocrine markers being positive.
In summary, the LCNEC entity's awareness and its occurrence in the kidney along with the appropriate usage of immunohistochemical techniques would enable the establishment of its diagnosis.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Oberg K. Neuroendocrine tumors of the gastrointestinal tract: Recent advances in molecular genetics, diagnosis and treatment. Curr Opin Oncol. 2005;17:386–91. doi: 10.1097/01.cco.0000167739.56948.a9. [DOI] [PubMed] [Google Scholar]
- 2.Lane BR, Chery F, Jour G, Sercia L, Magi-Galluzzi C, Novick AC, et al. Renal neuroendocrine tumors: A clinicopathologic study. BJU Int. 2007;100:1030–5. doi: 10.1111/j.1464-410X.2007.07116.x. [DOI] [PubMed] [Google Scholar]
- 3.Moukassa D, Leroy X, Bouchind'homme B, Saint F, Lemaître L, Gosselin B. Primary large cell neuroendocrine carcinoma of the kidney: Morphologic and immunohistochemical features of two cases. Ann Pathol. 2000;20:357–60. [PubMed] [Google Scholar]
- 4.De Lellis RA, Osamura RY. Neuroendocrine tumors: An overview. Pathol Case Rev. 2006;11:229–34. [Google Scholar]
- 5.Sahin A, Demirbas M, Ozen H, Sungur A, Küçükali T, Aygün N, et al. Primary carcinoid of the kidney. Scand J Urol Nephrol. 1996;30:325–7. doi: 10.3109/00365599609182316. [DOI] [PubMed] [Google Scholar]
- 6.Ricardo V Lloyd. The neuroendocrine and paracrine systems. In: Mills SE, editor. Sternberg's Diagnostic surgical pathology. 4th ed. Philadelphia: Lippincott Williams and Wilkins; 2004. pp. 507–19. [Google Scholar]