

Abstract
Pediatric Research Articles Ahead of Print
contains articles in unedited manuscript form that have been peer-reviewed and accepted for publication. As a service to our readers, we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting and review of the resulting proof before it is published in its final definitive form. Please note that during the production process errors may be discovered, which could affect the content, and all legal disclaimers that apply to the journal pertain.
Our goal was to determine how the actions of the thorax and the pelvis are organized and coordinated to achieve independent sitting posture in typically developing infants. The participants were ten typically developing infants that were evaluated longitudinally from first onset of sitting until sitting independence. Each infant underwent nine testing sessions. The first session included motor evaluation with the Peabody test. The other eight sessions occurred over a period of four months where sitting behavior was evaluated by angular kinematics of the thorax and the pelvis. A physical therapist evaluated sitting behavior in each session and categorized it according to five stages. The phasing relationship of the thorax and the pelvis was calculated and evaluated longitudinally using a one-way ANOVA. With development, the infants progressed from an in-phase (moving in the same direction) to an out-of-phase (moving in an opposite direction) coordinative relationship between the thorax and the pelvis segments. This change was significant for both the sagittal and frontal planes of motion. Clinically, this relationship is important because it provides a method to quantify infant sitting postural development, and can be used to assess efficacy of early interventions for pediatric populations with developmental motor delays.
During the acquisition of the simplest form of a skill, such as sitting, postural control is the primary goal to be successful. However, if we consider that postural control is the complex interaction of controlling and coordinating the numerous factors of the CNS, the task of sitting looks like an impossible skill to be acquired. Therefore, investigators have been interested in identifying how we actually develop this skill and several theories have been proposed to explain the development of postural control. These theories elicit hierarchical explanations, where skill is the outcome of mature executive function from the motor cortex, or a motor program located at the spinal cord or at the brainstem (1,2). However, these theories have not been successful in defining the relationship between the earlier and later forms of the behavior or explaining the synergistic action of the various cooperating components that contribute to the development of the behavior (3). The Dynamical Systems Theory (DST) provides an alternative approach to the development of posture control. According to DST, development of posture control, and generally movement skills, is a product not only of central and cognitive information, but arises from the synergistic organization of the neuromuscular system and the morphologic, biomechanical and environmental constraints (1,3). Utilizing this approach, Thelen and colleagues were able to explain stepping performance in newborns and identify that the “disappearance” of the newborn stepping response at about 2 mo is not due to changes in central processes but was due to the alterations that occur due to parallel development in body size and composition (4). Similarly, the same group has found that newborns can elicit adult-like steps when walking on a treadmill due to the mechanical backward stretch by the belt on the legs. This stretch practically provided the necessary hip strength needed for walking which is absent in newborns and eventually occurs due to development (5). Therefore, we anticipate that the DST framework can provide with similar insights for another motor milestone, the development of sitting posture, a skill that has not received much research attention.
From a DST perspective, the emergence of a movement behavior can be viewed as a path toward a stable attractor, which is the preferred behavioral state of the system (1,3). Attractors can be described quantitatively by evaluating the order parameter. In the studies mentioned above by Thelen and colleagues, interjoint and interlimb coordination have been used as order parameters (5,6). To elicit behavioral changes and explore how an order parameter differs from one attractor to another, the control parameter is used. In the studies mentioned above, hip strength as provided by a motorized treadmill or changes in gravity utilizing buoyancy have been used as control parameters. By scaling the control parameter, we can observe changes in behavior and we can describe the different attractors of the dynamical system in question. Previous studies that investigated standing postural control, used as the control parameter different support surfaces (7,8) and a suprapostural tracking task (9). Previous work has also demonstrated that relative phase, which describes the coordinative relationship between the segments of the lower extremity, is a suitable order parameter that can elucidate the collective states of the neuromuscular system during standing (7–9). Therefore, DST provides also the advantage of describing the dynamic state of the neuromuscular system by acknowledging a single variable, relative phase.
Even though the above theoretical framework can provide a basis for the exploration of infant sitting postural control, limited attention has been directed toward the understanding of the mechanisms involved in the postural control of sitting during development (10). Most of the existing literature on postural control of infants is focused on the examination of the development of postural adjustments during reaching (11–14). Only a few studies have investigated solely the development of sitting postural control in infants. In these investigations, kinematic and electromyographic analysis was used to describe sitting posture, while a movable platform was used to perturb postural control (15,16). Using a different paradigm, Harborne and Stergiou analyzed the development of sitting postural control in infants by exploring the variability of the center of pressure during infant sitting using a force platform (16). The development of posture was not approached as a process directed toward maximum balance resulting in a rigid and motionless body over the center of the base of support. On the contrary, variations present in the sitting postural sway during development were viewed not as noise that needs to be removed from the system, but as a basin rich in important environmental information. From this perspective, postural control develops as an ongoing process of improving sitting posture by managing available degrees of freedom. They also suggested that this process would enable the children at first to be fairly accurate in accessing the skill of sitting independently and then to explore more freely their environment. Importantly, they hypothesized that a significant component of gaining the ability to sit and coordinate the superincumbent body segments over the base of support includes the ability to control the thorax over the pelvis.
Therefore, the purpose of the present study was to implement the DST framework to examine the development of sitting postural control in typically developing infants by investigating the coordination of the thorax and pelvis segments. The motions of the thorax and the pelvis were evaluated longitudinally in terms of their relative phase relationship in typically developing infants from the first onset of sitting, and up to the point that they can sit independently. For the present study, change in the physiologic and neuromuscular systems (natural development) served as the control parameter. We hypothesized that through development, we will be able to discern a movement in the opposite direction (a more out-of-phase relationship) between the thorax and pelvis segment to achieve independent sitting. Clinically, the quantification of this relationship is important because it can provide with a method to evaluate infant sitting postural development and eventually to assess efficacy of early interventions for infants with developmental motor delays.
METHODS
Subjects
The participants in this study were 10 typically developing infants (Table 1). The infants were followed from the age of around five months to eight months, the time when infants are learning to sit independently. Infants were recruited from employee announcements at the campus of the University of Nebraska at Omaha and at the Munroe-Meyer Institute, University of Nebraska Medical Center.
Table 1.
Descriptive characteristics of the subjects at onset and conclusion of the study.
| Weight (kg) | Age (Weeks) | Gender | |||
|---|---|---|---|---|---|
| Subjects | Start | End | Start | End | |
| 1 | 8.26 | 9.48 | 22.14 | 35.00 | Male |
| 2 | 7.24 | 8.16 | 18.29 | 31.43 | Female |
| 3 | 6.42 | 7.55 | 22.29 | 38.43 | Female |
| 4 | 5.81 | 6.42 | 18.14 | 32.57 | Female |
| 5 | 7.85 | 8.87 | 20.29 | 32.43 | Female |
| 6 | 7.14 | 8.57 | 22.14 | 34.29 | Female |
| 7 | 7.24 | 8.06 | 22.29 | 34.43 | Female |
| 8 | 8.16 | 8.97 | 24.00 | 37.00 | Female |
| 9 | 7.34 | 7.85 | 18.29 | 30.29 | Female |
| 10 | 6.73 | 7.34 | 22.57 | 32.57 | Female |
| Mean | 7.22 | 8.13 | 21.04 | 33.84 | |
| SD | 0.76 | 0.90 | 2.13 | 2.51 | |
The inclusion criteria for entry into the study for the typically developing infants were: a) a score on the Peabody within 0.5 SD of the mean, b) age of about five months at the time of initial data collection, c) the ability of the child to hold up their head when supported at the thorax, d) beginning ability to reach for objects dangled in front of them in supported sitting or lying on their back, e) propping on their elbows when in prone for thirty seconds and f) propping on both arms to maintain sitting. The exclusion criteria were: a) a score on the Peabody of greater than 0.5 SD below the mean, b) diagnosed visual deficits, and c) diagnosed musculoskeletal problems. Before participation an informed consent form was signed by the parents of the infants. The study has been approved by the Institutional Review Board of the University of Nebraska Medical Center.
Experimental design
Each infant participated in nine sessions. The first session lasted for 45 min and was used to perform the Peabody. The Peabody is a norm-and criterion-referenced test that examines gross motor function in children from birth to 83 mo (17). The other eight sessions were distributed over a period of four months. The infants were tested twice in one week at each of the four months of the study. A physical therapist ranked each infant’s sitting behavior at each session according to five stages of sitting: 1) Prop sitting, 1.5) Transition-moves briefly out of prop sit, but goes back to it, 2) Variable, about 10 s of sitting, 2.5) Not solid stage 3, but longer than 10 s of sitting and 3) Sits upright all the time-doesn’t need hands. Stage identification was always performed by the same physical therapist (author RTH). Even though more than one session could be identified at the same stage of sitting, the three trials required by each infant for a specific stage were chosen from the same session. Stages of sitting were considered the appropriate independent variable of development, because of the wide variability of age at which the infants began to sit.
Protocol
For all sessions, the infants were allowed time to get used to the laboratory setting, and were at their parent’s side or on their lap for preparation. A standard set of infant toys was used for distraction and comfort, accompanied by a DVD player, which presented infant movies. All attempts were made to maintain a calm, alert state by allowing the infant to eat if hungry, be held by a parent for comforting, or adapt the temperature of the room to the infant’s comfort level.
After the child was undressed by the mother, two sets of triangles with one reflective marker in each corner were glued with a double face tape in two locations (Fig. 1A): around the spinous process at the level of the axilla, so as the upper side of the triangle was parallel to the shoulder’s mediolateral line and the second triangle was placed midway between the left and right posterior superior iliac spine so as one side of the triangle was parallel to the level of the pelvic crest. After positioning the reflective markers, the infants were placed by their parent on the top of a force plate that was covered with a special pad for warmth, which was securely adhered with tape on the force plate. The baby was held in the sitting position in the middle of the plate when calm and happy (Fig. 1B). The investigator and the parent remained at one side and in front of the infant respectively during all data collection to assure the infant does not fall or become insecure. The child was held at the thorax for support, and gradually the infant was guided into a sitting position while being distracted by toys presented by the parent, the investigator, or a DVD movie. Once the examiner could completely let go of the infant, data were collected continuously while the child maintained sitting (Fig. 1B). Data were collected until we had three trials that were acceptable for our criteria, or until the infants were indicating that they were done. If the child became irritated, the session was halted for comforting by the parent, or a chance of feeding, and then resumed only when the child was again in a calm state.
Figure 1.
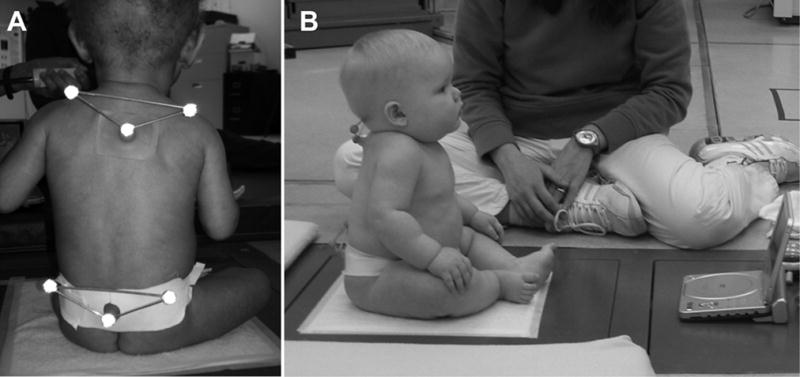
A. Rear view of the position of the infant during data collection. B. Side view of the position of the infant during data collection.
Data Analysis
Kinematic data were collected using a six camera motion analysis system (Vicon, Oxford Metrics Group, Oxford, UK) at a sampling rate of 60 Hz. The lightweight reflective markers (Fig. 1) were tracked by the system, and recorded in three-dimensional space. Specifically, the local coordinate systems (Fig. 2) defined the origin of each segment (pelvis and thorax), with respect to the global reference system of the laboratory. Thereafter, the angular kinematic data were calculated relative to the fixed global coordinate system of the laboratory. The movement patterns of the thorax and the pelvis were viewed as inverted pendulums. Furthermore, video of each trial was collected using two Panasonic video cameras (Model 5100 HS) and processed for split screen video imaging using a Panasonic Digital AV Mixer (Model WJ-MX30). The cameras were positioned to record a sagittal and a frontal view of the subject.
Figure 2.
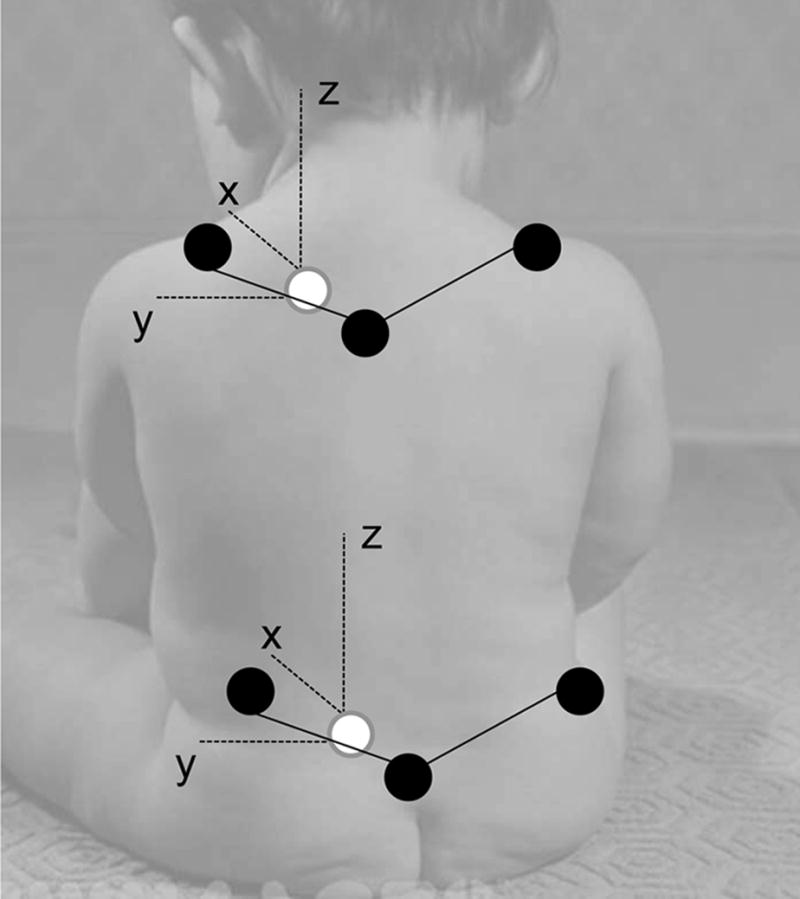
Schematic representation of the pelvis and the thorax segments.
Three acceptable trials of 8.3 s were selected from each testing session using the video record and the following criteria: a) infant did not move the arms (not reaching, holding an object, or flapping their arms), b) infant did not vocalize or cry, c) infant was not in the process of falling, d) thorax was not inclined more than 45 degrees to either side, e) not being touched, f) the arm position (propping or not propping) of the infants was noted during the entire trial and only trials that have the infant using consistent base of support was used. Test re-test reliability of trial identification was 0.99. Out of the 240 trials in total required to examine infant sitting posture across stages of sitting, we were able to identify 239 acceptable trials based on our criteria.
The six reflective markers attached in the form of two triangles, defined a two-segment model comprised of the pelvis and the thorax (Fig. 2). Coordination of these segments was examined in the sagittal and the frontal plane. The angular kinematic data acquired were used to examine the coordination pattern between the thorax and the pelvis. The data were filtered using a 0.5Hz low pass, second order Butterworth filter. The 0.5Hz as a cut-off frequency was selected based on power spectrum evaluation and phase portrait qualitative analysis.
To examine the coordination between the two segments, the phase portraits for the thorax and the pelvis were generated (Fig. 3), which is a plot of each segment’s position versus its velocity (18). The phase portrait analysis follows Rosen’s suggestion (18) that the behavior of a dynamical system may be captured by a variable and its first derivative with respect to time. Once the phase portraits were constructed, the resulting phase plane trajectories were transformed from Cartesian (x, y) to polar coordinates with a phase angle Φ = tan−1y/x and radius (19). Phase angle ranged from zero to ± 180 degrees. The phase angles of the segments’ trajectories were used to calculate relative phasing relationships between the actions of the two respective segments for the period of sitting. Relative phase represents the coordinative relationship between the actions of two segments at every point during a specific time domain. In other words, relative phase indicates how the two segments were coupled in their movements while performing the sitting task. Relative phase was calculated by subtracting the distal phase angle (thorax) from the proximal phase angle (pelvis). Relative phase values close to zero designated that the two segments were moving in similar fashion or in-phase, while values close to 180 indicated that the two segments moved exactly opposite or out-of-phase. Relative phase curves were not time normalized since the time lengths of all sitting trials selected were 8.3 s. The relative phase curves were also averaged and mean ensemble curves were generated from all infants and for each testing session (by averaging the three acceptable trials) for the evaluation of the postural control during sitting. Furthermore, the mean of the absolute values for all points of the relative phase (MARP) mean ensemble curve was calculated. This parameter captured in a single value the entire relative phase curve. Thus, MARP values close to zero designated that the two segments were moving in similar fashion or in-phase, while values close to 180 indicated that the two segments moved opposite or out-of-phase. All the above analysis was performed by custom written laboratory software in Matlab (The MathWorks, Natick, MA).
Figure 3.

Example of time series data for pelvis and thorax at the onset and end of the study as well as the corresponding phase portraits. Phase portraits provide a qualitative picture of the organization of the neuromuscular system. Solid line represents the pelvis while the dotted line represents the thorax.
Statistical Analysis
Based on the physical therapist’s evaluation of each session’s sitting behavior for each infant, five groups of sitting were formed and tested statistically. Group means and standard deviations were calculated for the MARP for each stage and for both planes. Because we had an unequal number of observations at each stage of sitting, we did not perform repeated measures ANOVA. Instead, one-way between stages of sitting ANOVA with a test for linear trend was performed on the subjects’ means for each parameter using the SPSS software. A Tukey multiple comparison post hoc analysis was also performed to identify the location of the significant differences for all tests resulting in a significant F-ratio. All statistical tests were evaluated at the 0.05 level for significance.
RESULTS
An example of time series data for pelvis and thorax at the onset and at the last stage of sitting, as well as the corresponding phase portraits, are presented in Fig. 3. Generally, the angular position of the thorax and the pelvis at the onset of sitting seems to be very similar. Alternatively, at the end of the study the angular positions of the two segments seems to be the opposite; when the angular position of the thorax decreases, the angular position of the pelvis increases and vice versa. The phase portraits demonstrated a cyclic movement by the formation of a closed cyclic path. Even though this pattern is not a perfect circle, we can reasonably conclude that pelvis and thorax segments have an oscillatory nature, which in DST phraseology this constitutes a limit cycle type of behavioral attractor (19).
MARP values at the onset and conclusion of the study are presented in Table 2 for each subject. MARP values in the sagittal plane significantly increased (F = 4.406, df = 4, p = 0.003), demonstrating a more out-of-phase relationship, as the infants improved their ability of sitting. The post hoc analysis test revealed significant differences between the first and the third stage of sitting with the latter presenting larger values (Fig. 4A). A significantly increasing linear trend (F = 15.743, p [lt] 0.001) was found for MARP in the sagittal plane from stage one to stage three (Fig. 4A).
Table 2.
MARP values in the sagittal and frontal planes at onset and conclusion of the study.
| MARP | ||||
|---|---|---|---|---|
| Start | End | |||
| Subjects | Sagittal | Frontal | Sagittal | Frontal |
| 1 | 115.9 | 74.0 | 137.8 | 119.6 |
| 2 | 133.7 | 158.3 | 151.6 | 126.5 |
| 3 | 85.0 | 75.5 | 79.4 | 117.5 |
| 4 | 66.7 | 85.3 | 128.4 | 93.7 |
| 5 | 58.7 | 63.4 | 105.4 | 83.4 |
| 6 | 121.4 | 127.9 | 127.2 | 118.6 |
| 7 | 92.5 | 127.5 | 152.4 | 96.4 |
| 8 | 52.7 | 100.7 | 88.0 | 78.4 |
| 9 | 40.1 | 59.7 | 88.1 | 72.6 |
| 10 | 61.3 | 70.9 | 114.7 | 134.7 |
| Mean | 82.8 | 94.3 | 117.3 | 104.1 |
| SD | 32.1 | 33.2 | 26.6 | 21.9 |
Figure 4.

A. Group mean values and SE for MARP in the sagittal plane. B. Group mean values and SE for MARP in the frontal plane. The dotted line indicates statistically significant linear trend. * indicates significant differences. The sample size for each stage was the following: Stage 1 (6), Stage1.5 (3), Stage 2 (4), Stage 2.5 (7), Stage 3 (10).
MARP in the frontal plane of motion significantly increased (F = 2.742, df = 4, p = 0.034). The post hoc analysis revealed significant differences between the first stage and the 2.5 stage, with 2.5 stage showing slightly larger values (Fig. 4B). A significantly increasing linear trend (F = 6.253, p = 0.014) for MARP in the frontal plane from stage one to stage three (Fig. 4B).
DISCUSSION
The purpose of this study was to examine and identify any changes in the coordination pattern of the thorax and the pelvis during sitting in infants that may take place with development. The DST was used as the theoretical platform to examine coordination.
Our results verified our hypotheses for both sagittal and frontal planes of motion. The preferred behavioral state of infant sitting postural control was an out-of-phase relationship between the thorax and the pelvis. This conclusion was made due to the fact that at the latter stages of sitting when the infants demonstrated the ability to sit independently for long periods of time, the values of relative phase were much higher than the first stages of sitting and closer to 180°. These values are indicative of an out-of-phase relationship and were also noticeable from the example presented in Fig. 3. Therefore, the DST framework was able to define the relationship between the earlier and later forms of the sitting behavior and explain the synergistic action of the various cooperating components that contribute to the development of the sitting posture.
In addition, we hypothesized that at the onset of sitting, we had a different behavioral state or attractor. Infants presented a more in-phase relationship between the two segments both in the sagittal and frontal planes. The value of MARP for stage 1 in the sagittal plane was approximately 75°. Even though the value is not 0°, to indicate an absolute in-phase relationship of thorax and pelvis at the onset of sitting, it can be concluded that it is a rather in-phase relationship at the onset of sitting behavior. Moreover, as the infants matured physiologically and became more experienced, the value of MARP increased and reached 120°, which is closer to 180° and rather an out-of-phase relationship of the two segments. This demonstrates a clear behavioral transition for the sagittal plane of movement. Similarly, in the frontal plane the values of MARP presented a significant trend to increase with development. However, the values of MARP for the frontal plane on the third stage of sitting dropped to approximately 105°, similar to stage two, while the range of change in MARP was not as large as in the sagittal plane. It can be speculated that at the onset of sitting skill infants were not able to control efficiently the thorax, the pelvis motion, and the activation of the postural muscles. In contrast, with development and experience infants accomplish to synergistically self-organize the most appropriate degrees of freedom and conclude to the appropriate sitting pattern. This result may be due to biomechanical and/or neuromuscular constraints, such as the fat tissue stored around the pelvis of the infants, which may limit the movement of the upper body in the frontal plane.
Theoretical mechanical aspects of sitting postural control should also be considered (20), regarding the results of the present study. To achieve independent sitting posture, the body center of mass must remain within the base of support. When there is an in-phase relationship between two segments, this will lead to an unstable behavioral state. This instability does not allow the system to counteract and keep the center of mass (COM) within the stability limits (Fig. 5). Specifically, when both the thorax and the pelvis move in the same direction, they move as one segment, which has its axis of rotation at the pelvis. Thus, as the gravity and the force produced from the neuromuscular system pushes the system in one direction, the center of mass steps out of the base of support, and falling occurs. The opposite holds true with an out-of-phase relationship, which is more stable behavioral state. Particularly, when the thorax and the pelvis move in the opposite direction, the axis of rotation is located between the two segments. Hence, as the gravity and the force produced from the neuromuscular system pushes the segments in the opposite direction, the center of mass is prohibited from stepping out of the base of support, and sitting occurs (Fig. 5). This synergistic action of the cooperating components contributes to the development of the sitting posture.
Figure 5.
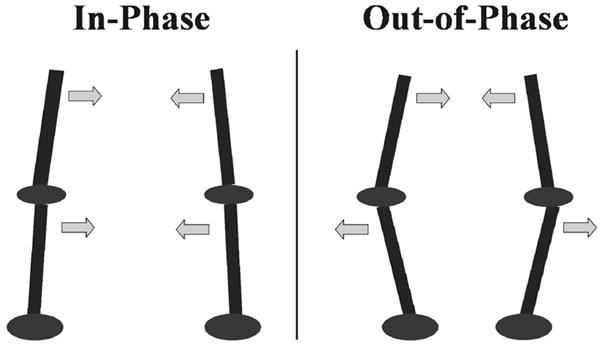
Schematic representation of the in-phase and the out-of-phase coordinative relationships between two connected segments.
The results of the present study could not be compared directly with other studies because there are no investigations examining coordination of thorax and pelvis in infants. Woollacott et al. (21) reported that infants as young as five months produce directionally postural responses as a result to perturbation in the trunk, while other infants did not. This result suggests that the organization of postural responses is not predetermined but arises from the synergistic interaction of the neuromuscular system as well as other constrains (21). Therefore, the coordination of the trunk and pelvis segments in infants acquiring the sitting skill should be governed by the same principles. An interesting observation of our data are that individual patterns have emerged regardless of the average picture of the statistical analysis, especially in the frontal plane of motion. Specifically, four out of the 10 infants presented decreasing values of MARP in the frontal plane, when comparing the onset with the last stage. Interestingly, these infants were the ones that appeared to have greater weight initially and at the last stage from almost all the other infants. Therefore, biomechanical constraints, such as weight, may have influenced the acquirement of the sitting skill in those infants and eventually regulated appropriate coordination of the thorax and pelvis mostly through the sagittal plane of motion. Variation between subjects, but also within subjects is one of the main characteristics of infant motor development and it has been observed in multiple studies (14,15).
A limitation of the present study is that data were analyzed on the basis of the infant’s motor behavior, i.e., the infant’s ability to sit. This means that the developmental changes in MARP reflect the developmental changes in what the child is doing, i.e., the data mainly reflect whether the child sits with support of the arms (first 2 stages) or without support of the arms. It is well known that even minimal support of the arms induces large changes in postural control (28). However, we decided to use this approach because this is the natural behavioral response by the infant while developing the ability to sit and thus we did not want to exclude it from the analysis.
In conclusion, the preferred behavioral state of infant sitting postural control was an out-of-phase relationship between the thorax and the pelvis for the sagittal and frontal planes. In addition, at the onset of sitting, we had a different behavioral state. We believe that the investigation of sitting postural control through the coordination of the thorax and the pelvis can assess the development of infant sitting posture and can quantify objectively, by means of a single variable, incremental change through the development of infant sitting postural control. Furthermore, there is lack of knowledge on which treatments are most efficacious for children that present developmental delays at an early age. Hence, the proposed method of evaluating sitting postural control could be a valuable tool for the study of therapeutic interventions directed at improving the postural control of infants with motor delays.
Acknowledgments
This work was supported by NIH (K25HD047194), NIDRR (H133G040118), the Nebraska Research Initiative and the Reichenbach fellowship from the Graduate Studies Office of University of Nebraska Medical Center.
Abbreviations
- DST
Dynamical Systems Theory
- MARP
Mean Absolute Relative Phase
References
- 1.Clark JE. On becoming skillful: patterns and constraints. Res Q Exerc Sport. 1995;66:173–183. doi: 10.1080/02701367.1995.10608831. [DOI] [PubMed] [Google Scholar]
- 2.Hirschfeld H, Forssberg H. Epigenetic development of postural responses for sitting during infancy. Exp Brain Res. 1994;97:528–540. doi: 10.1007/BF00241546. [DOI] [PubMed] [Google Scholar]
- 3.Thelen E, Smith LB. A dynamic systems approach to the development of cognition and action. MIT Press; Massachusetts: 1994. pp. 1–340. [Google Scholar]
- 4.Thelen E, Fisher DM. Newborn stepping: an explanation for a “disappearing reflex”. Dev Psychol. 1982;18:760–775. [Google Scholar]
- 5.Thelen E. Treadmill-elicited stepping in seven-month-old infants. Child Dev. 1986;57:1498–1505. [PubMed] [Google Scholar]
- 6.Thelen E, Ulrich BD. Hidden skills: a dynamic systems analysis of treadmill stepping during the first year. Monogr Soc Res Child Dev. 1991;56:1–98. discussion 99–104. [PubMed] [Google Scholar]
- 7.Marin L, Bardy BG, Baumberger B, Fluckiger M, Stoffregen TA. Interaction between task demands and surface properties in the control of goal-oriented stance. Hum Mov Sci. 1999;18:31–47. [Google Scholar]
- 8.Oullier O, Bardy BG, Stoffregen TA, Bootsma RJ. Task-specific stabilization of postural coordination during stance on a beam. Motor Control. 2004;8:174–187. doi: 10.1123/mcj.8.2.174. [DOI] [PubMed] [Google Scholar]
- 9.Bardy BG, Marin L, Stoffregen TA, Bootsma RJ. Postural coordination modes considered as emergent phenomena. J Exp Psychol Hum Percept Perform. 1999;25:1284–1301. doi: 10.1037//0096-1523.25.5.1284. [DOI] [PubMed] [Google Scholar]
- 10.Shumway-Cook A, Woollacott M. Motor Control: Theory and practical applications. Williams & Wilkins; Baltimore: 1995. pp. 143–166. [Google Scholar]
- 11.Van der Heide JC, Fock JM, Otten B, Stremmelaar E, Hadders-Algra M. Kinematic characteristics of postural control during reaching in preterm children with cerebral palsy. Pediatr Res. 2005;58:586–593. doi: 10.1203/01.pdr.0000176834.47305.26. [DOI] [PubMed] [Google Scholar]
- 12.Van der Heide JC, Otten B, van Eykern LA, Hadders-Algra M. Development of postural adjustments during reaching in sitting children. Exp Brain Res. 2003;151:32–45. doi: 10.1007/s00221-003-1451-3. [DOI] [PubMed] [Google Scholar]
- 13.Fallang B, Oien I, Hellem E, Saugstad O, Hadders-Algra M. Quality of reaching and postural control in young preterm infants is related to neuromotor outcome at 6 years. Pediatr Res. 2005;58:347–353. doi: 10.1203/01.PDR.0000170898.60160.09. [DOI] [PubMed] [Google Scholar]
- 14.Harbourne RT, Giuliani C, Neela JM. A kinematic and electromyographic analysis of the development of sitting posture in infants. Dev Psychobiol. 1993;26:51–64. doi: 10.1002/dev.420260105. [DOI] [PubMed] [Google Scholar]
- 15.Hadders-Algra M, Brogren E, Forssberg H. Ontogeny of postural adjustment during sitting in infancy: variation, selection and modulation. J Physiol. 1996a;493:273–288. doi: 10.1113/jphysiol.1996.sp021382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Harbourne RT, Stergiou N. Nonlinear analysis of the development of sitting postural control. Dev Psychobiol. 2003;42:368–377. doi: 10.1002/dev.10110. [DOI] [PubMed] [Google Scholar]
- 17.Folio MR, Fewell RR. Peabody Developmental Motor Scales. 2. Pro-ed Inc; Austin: 2000. pp. 1–125. [Google Scholar]
- 18.Kurz M, Stergiou N. Applied dynamical systems theory for the analysis of movement. In: Stergiou N, editor. Innovative Analyses of Human Movement. Human Kinetics; Champaign: 2003. pp. 93–120. [Google Scholar]
- 19.Clark JE, Phillips SJ. A longitudinal study of intralimb coordination in the first year of independent walking: A dynamical systems analysis. Child Dev. 1993;64:1143–1157. [PubMed] [Google Scholar]
- 20.Assaiante C, Mallau S, Viel S, Jover M, Schmitz C. Development of postural control in healthy children: a functional approach. Neural Plast. 2005;12:109–118. doi: 10.1155/NP.2005.109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Woollacott MH, Debu B, Shumway-Cook A. Children’s development of posture and balance control: changes in motor coordination and sensory integration. In: Gould D, Weiss M, editors. Advances in pediatric sport sciences: behavioral issues. Human Kinetics; Champaign: 1986. pp. 166–186. [Google Scholar]
- 22.Cordo PJ, Nashner LM. Properties of postural adjustments associated with rapid arm movements. J Neurophysiol. 1982;47:287–302. doi: 10.1152/jn.1982.47.2.287. [DOI] [PubMed] [Google Scholar]