

Abstract
Background
While knee osteoarthritis has been shown to affect a multitude of kinematic, kinetic and temporo-spatial gait parameters, few investigations have examined the effect of increasing levels of radiographic osteoarthritis severity on these gait parameters. Fewer still have investigated the effect of walking speed on gait variables in persons with knee osteoarthritis. The objective of this study was to investigate the influence of walking speed on biomechanical variables associated with joint loading in persons with varying severities of medial compartment knee osteoarthritis.
Methods
Twenty-one persons with moderate osteoarthritis (Kellgren-Lawrence score 2–3) and 13 persons with severe osteoarthritis (Kellgren-Lawrence score of 4) participated. Twenty-two persons without knee pain or radiographic evidence of arthritis comprised a healthy control group. Sagittal plane kinetics, knee adduction moment, sagittal plane knee excursion, ground reaction forces and knee joint reaction forces were calculated from 3-dimensional motion analysis at 1.0 m/s, self-selected and fastest tolerable walking speeds. Differences were analyzed using multivariate analysis of variance and multivariate analysis of covariance with speed as a covariate.
Findings
Persons with knee osteoarthritis showed significantly lower knee and ankle joint moments, ground reaction forces, knee reaction force and knee excursion when walking at freely chosen speeds. When differences walking in speed were accounted for in the analysis, the only difference found at all conditions was decreased knee joint excursion.
Interpretation
Compared to a healthy control group, persons with knee OA demonstrate differences in joint kinetics and kinematics. Except for knee excursion, these differences in gait parameters appear to be a result of slower freely chosen walking speeds rather than a result of disease progression.
Introduction
The use of three-dimensional gait analysis has allowed researchers and clinicians to better understand biomechanical alterations in the presence of lower extremity pathology. Measurement of joint kinematics and kinetics has allowed medical professionals, clinicians and biomechanists to quantitatively evaluate the functional success of innovative rehabilitation strategies (Agrawal et al., 2007, Yakimovich et al., 2005, Pollo et al., 2002) or surgical techniques (Mont et al., 2007). Gait analysis has also proved itself as an important tool in determining biomechanical factors that may influence the progression of pathologies, such as knee osteoarthritis (OA), that may be mechanically initiated (Chang et al., 2004, Miyazaki et al., 2002, Lynn et al., 2007).
While the presence of OA has been shown to affect a multitude of kinematic, kinetic and temporo-spatial gait parameters (Childs et al., 2004, Thorp et al., 2006, Al-Zahrani and Bakheit, 2002, Kaufman et al., 2001, Gok et al., 2002, Rudolph et al., 2007), few investigations have examined the effect of increasing levels of radiographic OA severity on these gait parameters (Astephen et al., 2008b, Thorp et al., 2006). Fewer still have investigated the effect of walking speed in persons with knee OA (Bejek et al., 2006, Landry et al., 2007). An evaluation of the effect of walking speed in persons with progressive grades of OA is currently lacking in the literature.
Gait speed is an important consideration when measuring gait parameters that are based on the magnitude of ground reaction forces and segmental accelerations (Andriacchi et al., 1977, Keller et al., 1996, Winter, 1983). Faster accelerations in the center of mass may result in higher ground reaction forces, and in turn, higher joint moments. In persons with and without arthritis of the hip and knee, increases in joint moments were seen when subjects were challenged to walk at faster speeds (Bejek et al., 2006, Lelas et al., 2003, Mockel et al., 2003). Larger joint moments have been shown to correlate to increased joint loads, which have been implicated in the disease progression (Zhao et al., 2007, Miyazaki et al., 2002). A reduction in walking speed has been suggested as a possible method used by persons with medial compartment knee OA to reduce the loads at the knee (Mundermann et al., 2004, Robon et al., 2000). However, these studies looked only at a cross-section of self-selected walking speeds and did not analyze differences at a control speed. In a population of healthy subjects, Lelas et al. (2003) showed that kinetic variables exhibited a significant linear or quadratic increase as walking speed was increased. Because changes in joint moment are associated with joint loading (Zhao et al., 2007), it is possible that subjects with severe OA will attempt to limit increases in these variables, or conversely, be unable to compensate for a change in speed and reveal a disproportionate increase in joint moments with increased walking speed.
Analysis at both a self-selected and control (1.0 m/s) walking speed will reveal which variables are associated with altered mechanics related to disease progression versus differences that exist as a result of decreased walking velocity. In addition, having the subjects walk at their fastest tolerable speed will establish how persons with varying degrees of knee OA compensate for challenges to the neuromuscular system. The purpose of this study is to investigate the influence of walking speed on biomechanical variables associated with joint loading in a population of persons with varying severities of medial compartment knee OA. We are hypothesizing that subjects with different severities of knee OA will demonstrate different walking patterns at freely chosen walking speeds. We also hypothesize that these differences will not exist when subjects walk at a constrained speed or when speed is accounted for in the statistical analysis.
Methods
Subjects
Subjects were recruited from a local orthopedic office, a local senior center, as well as through fliers placed throughout the community. Individuals were considered for inclusion in the OA group if they met the inclusion/exclusion criteria in Table 1. Subjects for the control group met all the same criteria, except radiographic evidence of OA, and all had no knee pain with daily activities. All subjects had a posterior to anterior, flexed knee radiograph read by a radiologist to confirm and classify the presence of OA based on the Kellgren-Lawrence (KL) severity levels (Kellgren and Lawrence, 1957). Subjects were grouped into three categories: asymptomatic controls (KL grade 0), moderate OA (KL grade 2 or 3), and severe OA (KL grade 4). Height, weight, body mass index (BMI) and Knee Outcome and Osteoarthritis Scores (KOOS) (Roos and Lohmander, 2003) were acquired from all of the subjects. An increase in KOOS score represents an increase in self-reported functional ability and quality of life. Each subject was made aware of the risks and benefits of the study and given the opportunity to withdraw from the study, without penalty, at any time. All subjects signed an informed consent form approved by the Human Subjects Review Board prior to participation in any portion of the study. Demographic data for the subject groups is presented in Table 2.
Table 1.
Inclusion/exclusion criteria for the OA subject groups
| Inclusion | Exclusion |
|---|---|
|
|
Table 2.
Demographic data for all subjects. Subjects with OA had significantly higher mean body mass, BMI and lower mean KOOS score when compared to the control group (*)(P≤0.05).
| Control (n=22) |
Moderate (n=21) |
Severe (n=13) |
|
|---|---|---|---|
| Mean (SD) | Mean (SD) | Mean (SD) | |
| Age (yrs) | 59 (11) | 63 (9.3) | 59 (9.8) |
| Height (m) | 1.65 (0.05) | 1.66 (0.08) | 1.7 (0.11) |
| Weight (kg) | 68.81 (9.5) | 81.19 (12.5) * | 94.69 (15.0) * |
| BMI | 25.1 (3.8) | 29.24 (4.1) * | 30.54 (5.2) * |
| KOOS | 477.1 (26.86) | 286.3 (80.8) * | 213.9 (99.3) * |
Data Acquisition
Gait analysis consisted of 3 separate walking trials on a split-belt treadmill (Bertec Corp, Columbus, OH, USA). This treadmill is capable of capturing three-dimensional forces, free moment and center of pressure (COP) data, which were collected at 1080 Hz. Individual belt velocity was controlled by the investigator at a computer terminal. As a safety precaution, subjects wore an overhead harness. Two emergency stop buttons, one located on the handrail and the other at located at the computer terminal, were utilized in the event an immediate stop was required. For determination of three-dimensional kinematics and kinetics, a Helen Hayes retro-reflective marker set was used. Walking data was obtained using a 6 camera infrared Motion Analysis system (Santa Rosa, CA, USA) and was collected at 60 Hz.
Subjects walked at 3 different speeds: 1.0 m/s (control speed), self-selected (determined by a 10m timed walk in the hallway), and fastest tolerable walking speed. Fastest speed was determined as the fastest speed at which the subject felt comfortable walking without the use of handrails while also maintaining a period of double limb support. Subjects were allowed to use the handrails during speed transitions, but walked without support during the collected trials. Subjects were given approximately 4 minutes to familiarize themselves with the experience of walking on a split-belt treadmill (Zeni Jr and Higginson, 2006). At each of the speeds, at least one 30 second trial was obtained. Data collection was performed using EvaRT 5.0.4 (Motion Analysis Corp., Santa Rosa, CA, USA).
Data Reduction
Coordinate marker data was filtered using a 4th order phase-corrected Butterworth filter with a cutoff frequency of 6 Hz. Calculation of joint angles, moments and forces were performed using OrthoTrak 6.3.5. Joint forces and joint moments were normalized to body mass. These data were divided into individual gait cycles from heel strike to ipsilateral heel strike. An ensemble averaged trial normalized to 101 points for each variable was created using custom written programs in LabView 8.2 (National Instruments, Austin, TX, USA). The averaged trial was calculated from a single 30 second walking trial at each of the speeds. While differences in cadence affected the actual number of strides used in the ensamble average, it averaged 26 consecutive gait cycles. Comparisons between individuals and groups were made based on the time normalized averaged trials. Peak sagittal plane hip, knee and ankle moments and peak frontal plane knee moments were compared. Peak vertical and anterior/posterior ground reaction forces (GRF), peak longitudinal knee joint reaction force (JRF), vertical loading rate and sagittal plane knee joint excursion during loading response were also included in the analysis. These variables were chosen based on their potential implications in joint loading or as compensatory strategies employed by persons with knee OA. Vertical loading rate was computed as the average slope of vertical GRF during loading response. It was computed over the first 10% of the gait cycle (Mundermann et al., 2005). Knee joint excursion was the range of sagittal plane knee flexion that occurred from heel strike to peak knee flexion during stance. These variables were determined at all three walking speeds, and the differences in these variables during fast and self-selected walking speeds were also examined.
Statistical Analysis
Differences between groups were evaluated using individual multivariate ANOVAs for each speed with post-hoc testing as needed. Internal Bonferroni adjustments in the level of significance were made to allow for the multiple comparisons and P values ≤0.05 represent significant differences. In the interest of further discerning differences that exist as a function of disease progression versus alterations in walking speed, the gait variables at the self-selected and fast speed were also analyzed between groups using individual MANCOVAs with the addition of the respective speed as a covariate. To assess the effect of speed on gait variables, repeated measures MANOVAs were used and evaluated for differences in main and interaction effect. A follow-up two-model hierarchal regression was used to support and validate the results from the ANOVA. The first model in the regression contained the walking speed and the second contained walking speed and OA grade. This does not provide us with the ability to determine differences between groups, but it does permit us to determine the relationship of OA grade to the gait variables, after accounting for the effect of walking speed. Significant changes in the F-score would suggest that OA grade is related to the gait parameter when accounting for walking speed. All statistical tests were performed using SPSS v.15 (Chicago, IL, USA).
Results
Walking Speed
There were significant differences in self-selected walking speed between the severe OA group, (1.03 SD 0.26 m/s; range 0.6–1.4), and the control group (1.22 SD 0.14 m/s; range 0.8–1.4)(p=0.008). The moderate group had a mean self-selected walking speed of 1.13 (SD 0.12; range 0.9–1.4) m/s, but was not statistically significantly different from either the severe or control group. At the fast speed, significant differences were found between all of the groups (p<0.004), although there were not significant differences in the percentage increase between groups (p>0.23). Mean fast walking speed was 1.75 (SD 0.23; range 1.2–2.2), 1.50 (SD 0.21; range 1.1–2.1), 1.37 (SD 0.28; range 0.8–1.8) m/s for the control, moderate OA and severe OA groups, respectively.
Between Group Differences
Significant differences in gait variables were found between groups for each of the walking speeds, although the variables that showed significant differences between groups were not the same at each speed. At 1.0 m/s, none of the gait variables were significantly different with the exception of loading rate (p=0.009) (Figure 1; Table 3). The moderate group showed a significantly lower vertical loading rate compared to the control or severe OA group (Table 3). When subjects walked at their self-selected speed, the number of significantly different gait variables increased. Peak knee flexion moment, peak ankle dorsiflexion moment, peak longitudinal knee JRF, peak vertical GRF, braking and pushoff GRF, loading rate and knee excursion all showed significant differences (Figure 2; Table 3). At the fast walking speed, differences were found between groups for all of the variables, except knee adduction moment, which showed no differences at any of the speeds (Figure 3; Table 3). For all of these variables, the severe OA group had the lowest values and the control group had the highest values.
Figure 1.
When speed was controlled and subjects walked at 1.0 m/s, there were no differences in sagittal plane hip, knee or ankle joint moments. No differences were seen for the knee adduction moment.
Table 3.
When compared to the control group, persons with knee OA demonstrate altered gait parameters (*). At the self-selected walking speed, differences in knee JRF, peak vertical GRF and loading rate remain significantly different when speed is accounted for in the analysis (β). When compared to the moderate group, persons with severe OA show significantly higher rate of joint loading (a).
| Variable | Group | 1.0 m/s | p-value | Self-Selected | p-value (NC) | p-value (CV) | Fast | p-value (NC) | p-value (CV) |
|---|---|---|---|---|---|---|---|---|---|
| Knee JRF (BW) | Control | 1.013 (0.06) | 1.084 (0.08) | 1.302 (0.15) | |||||
| Moderate | 0.971 (0.04) | 0.154 | 1.005 (0.05) *, β | 0.001 | 0.009 | 1.176 (0.11) * | 0.007 | 0.990 | |
| Severe | 0.977 (0.09) | 0.440 | 0.978 (0.06) *, β | 0.000 | 0.014 | 1.072 (0.11) * | 0.000 | 0.129 | |
|
| |||||||||
| Vertical GRF (BW) | Control | 1.076 (0.07) | 1.147 (0.09) | 1.374 (0.15) | |||||
| Moderate | 1.048 (0.05) | 0.654 | 1.075 (0.07) *, β | 0.006 | 0.036 | 1.356 (0.12) * | 0.015 | 0.990 | |
| Severe | 1.04 (0.10) | 0.566 | 1.045 (0.06) *, β | 0.001 | 0.026 | 1.145 (0.12) * | 0.000 | 0.188 | |
|
| |||||||||
| Braking GRF (BW) | Control | 0.144 (0.03) | 0.186 (0.05) | 0.281 (0.07) | |||||
| Moderate | 0.134 (0.03) | 0.990 | 0.157 (0.02) | 0.080 | 0.990 | 0.236 (0.05) * | 0.043 | 0.990 | |
| Severe | 0.153 (0.04) | 0.990 | 0.135 (0.05) * | 0.002 | 0.410 | 0.194 (0.05) * | 0.000 | 0.212 | |
|
| |||||||||
| Pushoff GRF (BW) | Control | 0.156 (0.02) | 0.201 (0.04) | 0.365 (0.05) | |||||
| Moderate | 0.15 (0.03) | 0.990 | 0.171 (0.04) * | 0.036 | 0.426 | 0.221 (0.04) * | 0.016 | 0.998 | |
| Severe | 0.152 (0.03) | 0.990 | 0.145 (0.05) * | 0.000 | 0.077 | 0.193 (0.05) * | 0.000 | 0.361 | |
|
| |||||||||
| Load Rate (BW/s) | Control | 9.236 (1.06) | 9.904 (0.96) | 11.353 (0.96) | |||||
| Moderate | 8.334 (1.14) * | 0.042 | 8.719 (0.98) *, β | 0.001 | 0.007 | 10.301 (1.27) * | 0.012 | 0.362 | |
| Severe | 9.562 (0.95)a | 0.017a | 9.22 (1.16)a | 0.001a | 0.039a | 10.23 (1.22) * | 0.021 | 0.990 | |
Figure 2.

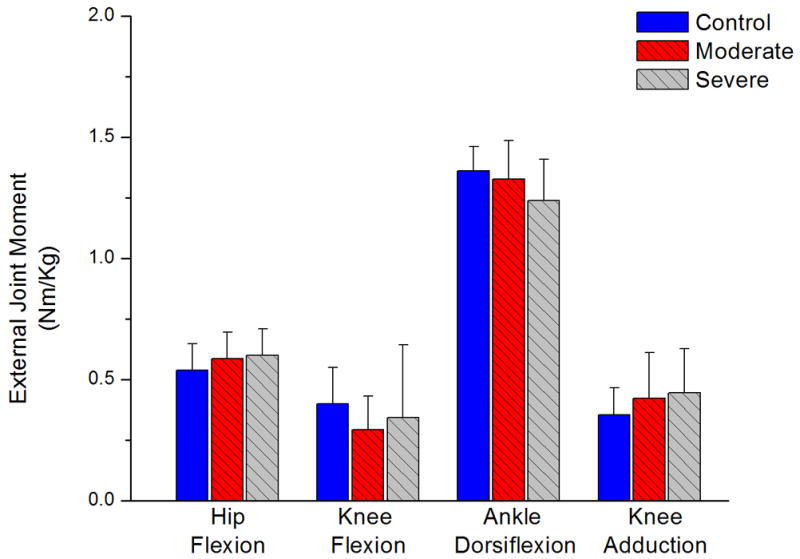
At self-selected walking speed subjects with moderate and severe OA showed a significant reduction in knee flexion moment (*) and subjects with severe OA showed a significant reduction in the ankle dorsiflexion moment (*). These differences were not significant when walking speed was included in the analysis. Although persons with OA had higher mean adduction moments, the difference was not significantly greater than the control group.
Figure 3.

At the fast walking speed, subjects with severe knee OA showed a significant reduction in sagittal plane hip, knee and ankle moments. These differences were not significant when speed was included as a covariate in the analysis.
Between Group Differences – Accounting for Speed
MANCOVA comparisons between groups using speed as a covariate revealed that the only variable that was still significant at both the self-selected and fast walking speed was knee excursion (Figure 4). The difference was significant between the severe and the control group (p<0.024). No other variables showed significant differences at the fast speed, however differences still existed at the self-selected speed. Longitudinal knee JRF and peak vertical GRF showed significant differences for both OA groups versus the control group and vertical loading rate and knee excursion showed differences between the severe and control group (Table 3).
Figure 4.
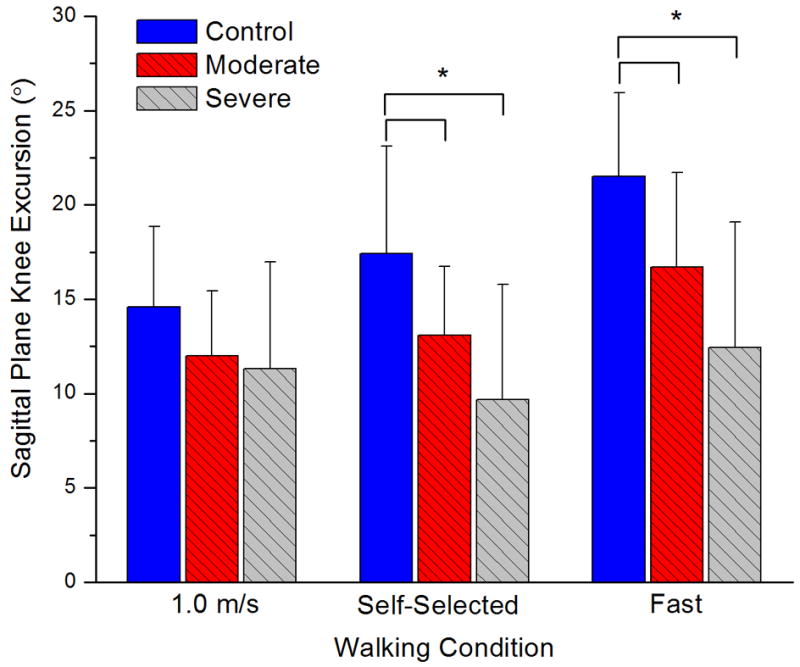
Knee joint excursion was significantly reduced in persons with knee OA at the self-selected and fast walking conditions (*). This difference was still significant for the severe group when speed was statistically controlled.
Between Speed Differences
Significant differences in gait variables were found between self-selected and fast walking speed (p<0.001) and the self-selected walking speed and 1.0 m/s (p<0.001). There was a significant speed*group interaction effect for the self-selected and fast speed comparison (p=0.036) and the self-selected and 1.0 m/s walking speed (p<0.001). Bonferroni corrected pair-wise comparisons between speeds for each group revealed that nearly all variables for all groups had significant increases between self-selected and fast walking speed. The only variable that did not have significant differences between speeds was the peak adduction moment for the severe OA group (p=0.51). Between the self-selected and 1.0 m/s walking speeds, all of the variables except adduction moment showed a significant reduction in the control (p<0.005) and moderate OA (p<0.040) groups. Contrarily, the severe group only showed a significant difference in the adduction moment between the self-selected and 1.0 m/s speeds (p=0.031). There was a reduction from 0.467 SD 0.17 Nm/kg at the self-selected speed to 0.439 SD 0.15 Nm/kg at 1.0 m/s. All other variables in this group showed no significant differences between self-selected and 1.0 m/s speeds.
Relational comparisons
Using the hierarchal regression, all of the variables were significantly related to self-selected walking speed (p≤0.045). The addition of the OA grade to the model did not significantly increase the R2 values for sagittal plane hip or knee moment, braking GRF or loading rate. When accounting for walking speed, the addition of OA grade did significantly increase the R2 value for sagittal plane ankle moment, knee adduction moment, vertical GRF, longitudinal knee JRF and push-off GRF. At the fast walking speed, all variables with the exception of braking GRF were also significantly related to walking speed (p<0.025; braking GRF p=0.10). The addition of OA grade to the model significantly increased the R2 value of only knee joint excursion (p=0.042; Adjusted R2 0.342). The addition of OA grade to the model approached significance levels for the adduction moment (p=0.06) and the push-off GRF (p=0.057).
Discussion
Subjects with varying degrees of knee OA demonstrate speed-dependent differences in a subset of gait parameters. At the controlled walking speed of 1.0 m/s, no differences were found for any of the variables, except loading rate, which was highest in the severe group. When speed was not controlled and subjects walked at freely chosen self-selected and fast speeds, differences were found in the majority of gait parameters studied. This is suggestive that speed is a factor responsible for differences between groups. This was further evidenced by the reduced differences between groups when speed was introduced as a covariate in the MANCOVA. These changes strongly suggest that modification of walking speed is responsible for the majority of differences noted between groups in this study.
Our results are similar to previous work that concluded that alterations in gait parameters associated with hip osteoarthritis may also arise mainly as a result of differences in freely chosen walking speeds (Mockel et al., 2003). This is an important consideration when making comparisons between groups with varying degrees of OA severity. Previous investigations which have found differences in similar gait parameters in an OA population have had subjects walk at freely chosen speeds (Ouellet and Moffet, 2002, Kaufman et al., 2001, Al-Zahrani and Bakheit, 2002, Maly et al., 2008, Landry et al., 2007, Astephen et al., 2008b, Astephen et al., 2008a). While these investigations provide important information on differences that exist in persons with knee OA, it may not be appropriate to suggest that changes in gait parameters arise as a result of mechanical changes that occur with the progression of knee osteoarthritis.
When different methodology is used, the effect of walking speed on gait parameters may make comparisons between studies difficult. The repeated measures MANOVA used to compare differences in gait variables between walking speeds showed significant differences between the 1.0 m/s and self-selected speed as well as between the self-selected and fast walking speed. While differences between self-selected and fast speed were expected (faster speeds result in higher joint moments and ground reaction forces for all groups), the differences between 1.0 m/s and self-selected speed are an important fact to consider when making comparison between studies. While the control group showed significant differences between 1.0 m/s and self-selected speeds for all variables, the severe group did not show any differences between the two speeds. This is likely due to the fact that the mean self-selected walking speed for the control group was 0.22 m/s faster than the control speed of 1.0 m/s, while the difference between the two speeds for the severe group was only 0.03 m/s. This is an important fact to consider when designing experimental methodologies or interpreting results from studies in which speed is controlled. It lends further support to the importance of including speed as a covariate in data analysis.
The validity of including speed as a covariate when exploring gait differences between persons of varying OA severity been questioned by previous authors (Astephen et al., 2008a). Particularly, they cite that using an ANCOVA in which the covariate (speed) is included in the model is inappropriate because it is affected by the main factor (OA severity) and is also inappropriate in cases in which large differences exist between the mean and range values of the covariate (speed). In our cohort of subjects, while differences did exist in freely chosen walking speed, the means were not vastly different and the total and interquartile range overlapped for all groups. Additionally, it was used as a supplementary analysis which supported the findings in the controlled walking speed trials. These results are complemented by the results from the regression analysis, although colinearity of speed and OA severity may be argued as a weakness of this technique as well.
While many previous investigations have found differences in adduction moment between OA and healthy subjects, the results from the ANOVA did not show significant differences between groups at any of the speeds. It should be noted, however, that for all of the conditions, the moderate and severe OA groups both had higher adduction moments, even though the difference was not significant. Also of note was the significant interaction effect between self-selected and fast walking speed. While the control and moderate OA groups showed significant increases in all the variables (including the adduction moment), no significant differences were seen in the severe group for the adduction moment between the self-selected and fast speeds. The severe group actually showed a decrease in the adduction moment as speed was increased (Figures 2 and 3). Since the adduction moment had been correlated with medial compartment joint loading (Zhao et al., 2007), tibial bone mineral content (Hurwitz et al., 1998), knee pain (Shrader et al., 2004), and disease progression (Miyazaki et al., 2002), the fact that persons with severe knee OA reduce the adduction moment when challenged to walk at faster speeds may be evidence of a compensatory mechanism to reduce the negative effects of medial joint loading. Increasing trunk sway, altering toe-out angle and changing frontal plane knee angles have been suggested as compensatory methods to reduce the knee adduction moment in persons with and without knee OA (Mundermann et al., 2008, Guo et al., 2007, Hunt et al., 2008). Further investigations into the mechanisms responsible for the reduction, or lack of increase, in the adduction moment during fast walking may be warranted.
While no differences in the adduction moment were seen between groups when using the ANOVA, we did see an important finding with the hierarchal regression. It showed that the severity of knee OA is related to the magnitude of the adduction moment, even when accounting for differences in freely chosen walking speed. These results support the findings of previous authors who have found an increase in the adduction moment in persons with OA when statistically controlling walking speed (Sharma et al., 1998, Baliunas et al., 2002).
Of particular interest in this study are the gait parameters that show significant differences between the control and OA group irrespective of walking speed. At 1.0 m/s and the self-selected walking speeds, when speed was included as a covariate, the severe group showed an increase in vertical loading rate when compared to the moderate OA group. Intuitively, this can be thought of as a variable that would be associated with increased rate of joint loading. At the self-selected speed, however, the subjects in both OA groups showed significant reductions in variables often associated with the magnitude of joint loading: longitudinal joint reaction force and peak vertical ground reaction force, when compared to the control group. It seems paradoxical that subjects with severe OA would have a higher rate of loading while potentially compensating to reduce the magnitude of the load. However, it is possible that the increased rate of loading may result from factors for which subjects with severe OA are not able to compensate for simply by decreasing walking speed. This supports previous findings that demonstrate an increase in the rate of joint loading (i.e. adduction moment) in persons with knee OA (Mundermann et al., 2005).
At the self-selected and fast walking speeds, subjects with more severe OA showed a reduction in knee excursion, even when accounting for differences in walking speed. During loading response, the rate of vertical loading may be affected by the vertical displacement of the center of mass. A reduction in the movement of the center of mass in the vertical direction has been proposed to result in higher “vertical stiffness” during walking (Butler et al., 2003). It is possible that a reduction in knee excursion during walking would result in smaller vertical displacement of the center of mass, and in turn a higher vertical stiffness. This higher vertical stiffness may be the underlying cause of increases in the rate of joint loading seen in subjects with severe knee OA. While further research is warranted to determine definitive reasons, intrinsic factors such as alterations in joint stability, changes in frictional values of the diseased knee joint or altered neuromuscular control strategies may reduce knee joint excursion, increase vertical stiffness of the body and, in turn, result in higher rates of vertical loading. This alteration may bode poorly for the integrity of cartilage in these subjects’ knees as higher joint loads have been shown to relate to disease initiation and progression (Griffin and Guilak, 2005). Decreased knee joint excursion in persons with knee OA has previously been established (Ramsey et al., 2007, Gok et al., 2002, Al-Zahrani and Bakheit, 2002, Weidow et al., 2006, Brinkmann and Perry, 1985). This alteration may be the defining kinematic characteristic of persons with knee OA, as differences between groups were found with the use of speed as a covariate. Additionally, knee excursion was related to OA grade, even when accounting for walking speed.
We have determined that altered gait parameters are found in persons with increasing severity of knee OA. The differences seen in this study were mainly a speed-dependent strategy. This supports previous work that has suggested alterations in gait variables may arise partially as a result of altered walking speed (Mundermann et al., 2004, Mockel et al., 2003). Although the majority of gait alterations may be the result of modified walking speeds, differences in certain gait variables persisted despite accounting for gait speed. These alterations may be the result of beneficial compensatory strategies employed by persons with knee OA (reduced vertical GRF and reduced longitudinal knee joint reaction force), or the end result of altered control strategies (increased rate of vertical load and decreased knee joint excursion) which may result in inefficient or detrimental gait patterns.
While this study provides pertinent information about kinematic and kinetic alterations between persons with varying degrees of OA, we are not able to ascertain whether some variables are related to the cause or the effect of the disease process. Future studies should incorporate a longitudinal design that would allow researchers to discern which variables contribute to disease progression and which are a result of advanced disease. This will lead to potential interventions that may decrease the rate of knee joint degeneration in certain individuals.
Acknowledgments
Funding support was received from NIH P20-RR16458
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- AGRAWAL SK, BANALA SK, FATTAH A, SANGWAN V, KRISHNAMOORTHY V, SCHOLZ JP, HSU WL. Assessment of motion of a swing leg and gait rehabilitation with a gravity balancing exoskeleton. IEEE Trans Neural Syst Rehabil Eng. 2007;15:410–20. doi: 10.1109/TNSRE.2007.903930. [DOI] [PubMed] [Google Scholar]
- AL-ZAHRANI KS, BAKHEIT AM. A study of the gait characteristics of patients with chronic osteoarthritis of the knee. Disabil Rehabil. 2002;24:275–80. doi: 10.1080/09638280110087098. [DOI] [PubMed] [Google Scholar]
- ANDRIACCHI TP, OGLE JA, GALANTE JO. Walking speed as a basis for normal and abnormal gait measurements. J Biomech. 1977;10:261–8. doi: 10.1016/0021-9290(77)90049-5. [DOI] [PubMed] [Google Scholar]
- ASTEPHEN JL, DELUZIO KJ, CALDWELL GE, DUNBAR MJ. Biomechanical changes at the hip, knee, and ankle joints during gait are associated with knee osteoarthritis severity. J Orthop Res. 2008a;26:332–41. doi: 10.1002/jor.20496. [DOI] [PubMed] [Google Scholar]
- ASTEPHEN JL, DELUZIO KJ, CALDWELL GE, DUNBAR MJ, HUBLEY-KOZEY CL. Gait and neuromuscular pattern changes are associated with differences in knee osteoarthritis severity levels. J Biomech. 2008b;41:868–76. doi: 10.1016/j.jbiomech.2007.10.016. [DOI] [PubMed] [Google Scholar]
- BALIUNAS AJ, HURWITZ DE, RYALS AB, KARRAR A, CASE JP, BLOCK JA, ANDRIACCHI TP. Increased knee joint loads during walking are present in subjects with knee osteoarthritis. Osteoarthritis Cartilage. 2002;10:573–9. doi: 10.1053/joca.2002.0797. [DOI] [PubMed] [Google Scholar]
- BEJEK Z, PAROCZAI R, ILLYES A, KISS RM. The influence of walking speed on gait parameters in healthy people and in patients with osteoarthritis. Knee Surg Sports Traumatol Arthrosc. 2006;14:612–22. doi: 10.1007/s00167-005-0005-6. [DOI] [PubMed] [Google Scholar]
- BRINKMANN JR, PERRY J. Rate and range of knee motion during ambulation in healthy and arthritic subjects. Phys Ther. 1985;65:1055–60. doi: 10.1093/ptj/65.7.1055. [DOI] [PubMed] [Google Scholar]
- BUTLER RJ, CROWELL HP, 3RD, DAVIS IM. Lower extremity stiffness: implications for performance and injury. Clin Biomech (Bristol, Avon) 2003;18:511–7. doi: 10.1016/s0268-0033(03)00071-8. [DOI] [PubMed] [Google Scholar]
- CHANG A, HAYES K, DUNLOP D, HURWITZ D, SONG J, CAHUE S, GENGE R, SHARMA L. Thrust during ambulation and the progression of knee osteoarthritis. Arthritis Rheum. 2004;50:3897–903. doi: 10.1002/art.20657. [DOI] [PubMed] [Google Scholar]
- CHILDS JD, SPARTO PJ, FITZGERALD GK, BIZZINI M, IRRGANG JJ. Alterations in lower extremity movement and muscle activation patterns in individuals with knee osteoarthritis. Clin Biomech (Bristol, Avon) 2004;19:44–9. doi: 10.1016/j.clinbiomech.2003.08.007. [DOI] [PubMed] [Google Scholar]
- GOK H, ERGIN S, YAVUZER G. Kinetic and kinematic characteristics of gait in patients with medial knee arthrosis. Acta Orthop Scand. 2002;73:647–52. doi: 10.1080/000164702321039606. [DOI] [PubMed] [Google Scholar]
- GRIFFIN TM, GUILAK F. The role of mechanical loading in the onset and progression of osteoarthritis. Exerc Sport Sci Rev. 2005;33:195–200. doi: 10.1097/00003677-200510000-00008. [DOI] [PubMed] [Google Scholar]
- GUO M, AXE MJ, MANAL K. The influence of foot progression angle on the knee adduction moment during walking and stair climbing in pain free individuals with knee osteoarthritis. Gait Posture. 2007;26:436–41. doi: 10.1016/j.gaitpost.2006.10.008. [DOI] [PubMed] [Google Scholar]
- HUNT MA, BIRMINGHAM TB, BRYANT D, JONES I, GIFFIN JR, JENKYN TR, VANDERVOORT AA. Lateral trunk lean explains variation in dynamic knee joint load in patients with medial compartment knee osteoarthritis. Osteoarthritis Cartilage. 2008;16:591–9. doi: 10.1016/j.joca.2007.10.017. [DOI] [PubMed] [Google Scholar]
- HURWITZ DE, SUMNER DR, ANDRIACCHI TP, SUGAR DA. Dynamic knee loads during gait predict proximal tibial bone distribution. J Biomech. 1998;31:423–30. doi: 10.1016/s0021-9290(98)00028-1. [DOI] [PubMed] [Google Scholar]
- KAUFMAN KR, HUGHES C, MORREY BF, MORREY M, AN KN. Gait characteristics of patients with knee osteoarthritis. J Biomech. 2001;34:907–15. doi: 10.1016/s0021-9290(01)00036-7. [DOI] [PubMed] [Google Scholar]
- KELLER TS, WEISBERGER AM, RAY JL, HASAN SS, SHIAVI RG, SPENGLER DM. Relationship between vertical ground reaction force and speed during walking, slow jogging, and running. Clin Biomech (Bristol, Avon) 1996;11:253–259. doi: 10.1016/0268-0033(95)00068-2. [DOI] [PubMed] [Google Scholar]
- KELLGREN JH, LAWRENCE JS. Radiological assessment of osteo-arthrosis. Ann Rheum Dis. 1957;16:494–502. doi: 10.1136/ard.16.4.494. [DOI] [PMC free article] [PubMed] [Google Scholar]
- LANDRY SC, MCKEAN KA, HUBLEY-KOZEY CL, STANISH WD, DELUZIO KJ. Knee biomechanics of moderate OA patients measured during gait at a self-selected and fast walking speed. J Biomech. 2007;40:1754–61. doi: 10.1016/j.jbiomech.2006.08.010. [DOI] [PubMed] [Google Scholar]
- LELAS JL, MERRIMAN GJ, RILEY PO, KERRIGAN DC. Predicting peak kinematic and kinetic parameters from gait speed. Gait Posture. 2003;17:106–12. doi: 10.1016/s0966-6362(02)00060-7. [DOI] [PubMed] [Google Scholar]
- LYNN SK, REID SM, COSTIGAN PA. The influence of gait pattern on signs of knee osteoarthritis in older adults over a 5–11 year follow-up period: a case study analysis. Knee. 2007;14:22–8. doi: 10.1016/j.knee.2006.09.002. [DOI] [PubMed] [Google Scholar]
- MALY MR, COSTIGAN PA, OLNEY SJ. Clin Biomech. Bristol: Avon; 2008. Mechanical factors relate to pain in knee osteoarthritis. [DOI] [PubMed] [Google Scholar]
- MIYAZAKI T, WADA M, KAWAHARA H, SATO M, BABA H, SHIMADA S. Dynamic load at baseline can predict radiographic disease progression in medial compartment knee osteoarthritis. Ann Rheum Dis. 2002;61:617–22. doi: 10.1136/ard.61.7.617. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MOCKEL G, PERKA C, LABS K, DUDA G. The influence of walking speed on kinetic and kinematic parameters in patients with osteoarthritis of the hip using a force-instrumented treadmill and standardised gait speeds. Arch Orthop Trauma Surg. 2003;123:278–82. doi: 10.1007/s00402-003-0513-0. [DOI] [PubMed] [Google Scholar]
- MONT MA, SEYLER TM, RAGLAND PS, STARR R, ERHART J, BHAVE A. Gait analysis of patients with resurfacing hip arthroplasty compared with hip osteoarthritis and standard total hip arthroplasty. J Arthroplasty. 2007;22:100–8. doi: 10.1016/j.arth.2006.03.010. [DOI] [PubMed] [Google Scholar]
- MUNDERMANN A, ASAY JL, MUNDERMANN L, ANDRIACCHI TP. Implications of increased medio-lateral trunk sway for ambulatory mechanics. J Biomech. 2008;41:165–70. doi: 10.1016/j.jbiomech.2007.07.001. [DOI] [PubMed] [Google Scholar]
- MUNDERMANN A, DYRBY CO, ANDRIACCHI TP. Secondary gait changes in patients with medial compartment knee osteoarthritis: increased load at the ankle, knee, and hip during walking. Arthritis Rheum. 2005;52:2835–44. doi: 10.1002/art.21262. [DOI] [PubMed] [Google Scholar]
- MUNDERMANN A, DYRBY CO, HURWITZ DE, SHARMA L, ANDRIACCHI TP. Potential strategies to reduce medial compartment loading in patients with knee osteoarthritis of varying severity: reduced walking speed. Arthritis Rheum. 2004;50:1172–8. doi: 10.1002/art.20132. [DOI] [PubMed] [Google Scholar]
- OUELLET D, MOFFET H. Locomotor deficits before and two months after knee arthroplasty. Arthritis Rheum. 2002;47:484–93. doi: 10.1002/art.10652. [DOI] [PubMed] [Google Scholar]
- POLLO FE, OTIS JC, BACKUS SI, WARREN RF, WICKIEWICZ TL. Reduction of medial compartment loads with valgus bracing of the osteoarthritic knee. Am J Sports Med. 2002;30:414–21. doi: 10.1177/03635465020300031801. [DOI] [PubMed] [Google Scholar]
- RAMSEY DK, SNYDER-MACKLER L, LEWEK M, NEWCOMB W, RUDOLPH KS. Effect of anatomic realignment on muscle function during gait in patients with medial compartment knee osteoarthritis. Arthritis Rheum. 2007;57:389–97. doi: 10.1002/art.22608. [DOI] [PMC free article] [PubMed] [Google Scholar]
- ROBON MJ, PERELL KL, FANG M, GUERERRO E. The relationship between ankle plantar flexor muscle moments and knee compressive forces in subjects with and without pain. Clin Biomech (Bristol, Avon) 2000;15:522–7. doi: 10.1016/s0268-0033(00)00007-3. [DOI] [PubMed] [Google Scholar]
- ROOS EM, LOHMANDER LS. The Knee injury and Osteoarthritis Outcome Score (KOOS): from joint injury to osteoarthritis. Health Qual Life Outcomes. 2003;1:64. doi: 10.1186/1477-7525-1-64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- RUDOLPH KS, SCHMITT LC, LEWEK MD. Age-related changes in strength, joint laxity, and walking patterns: are they related to knee osteoarthritis? Phys Ther. 2007;87:1422–32. doi: 10.2522/ptj.20060137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- SHARMA L, HURWITZ DE, THONAR EJ, SUM JA, LENZ ME, DUNLOP DD, SCHNITZER TJ, KIRWAN-MELLIS G, ANDRIACCHI TP. Knee adduction moment, serum hyaluronan level, and disease severity in medial tibiofemoral osteoarthritis. Arthritis Rheum. 1998;41:1233–40. doi: 10.1002/1529-0131(199807)41:7<1233::AID-ART14>3.0.CO;2-L. [DOI] [PubMed] [Google Scholar]
- SHRADER MW, DRAGANICH LF, POTTENGER LA, PIOTROWSKI GA. Effects of knee pain relief in osteoarthritis on gait and stair-stepping. Clin Orthop Relat Res. 2004:188–93. doi: 10.1097/01.blo.0000119248.70353.a5. [DOI] [PubMed] [Google Scholar]
- THORP LE, SUMNER DR, BLOCK JA, MOISIO KC, SHOTT S, WIMMER MA. Knee joint loading differs in individuals with mild compared with moderate medial knee osteoarthritis. Arthritis Rheum. 2006;54:3842–9. doi: 10.1002/art.22247. [DOI] [PubMed] [Google Scholar]
- WEIDOW J, TRANBERG R, SAARI T, KARRHOLM J. Hip and knee joint rotations differ between patients with medial and lateral knee osteoarthritis: gait analysis of 30 patients and 15 controls. J Orthop Res. 2006;24:1890–9. doi: 10.1002/jor.20194. [DOI] [PubMed] [Google Scholar]
- WINTER D. Biomechanical motor patterns in normal walking. J Mot Behav. 1983;15:302–30. doi: 10.1080/00222895.1983.10735302. [DOI] [PubMed] [Google Scholar]
- YAKIMOVICH T, KOFMAN J, LEMAIRE E. Design, construction and evaluation of an electromechanical stance-control knee-ankle-foot orthosis. Conf Proc IEEE Eng Med Biol Soc. 2005;3:2333–40. doi: 10.1109/IEMBS.2005.1616934. [DOI] [PubMed] [Google Scholar]
- ZENI JRJ, HIGGINSON J. Familiarization to walking on a split belt treadmill. American Society of Biomechanics; Blacksburg, VA: 2006. [Google Scholar]
- ZHAO D, BANKS SA, MITCHELL KH, D’LIMA DD, COLWELL CW, JR, FREGLY BJ. Correlation between the knee adduction torque and medial contact force for a variety of gait patterns. J Orthop Res. 2007;25:789–97. doi: 10.1002/jor.20379. [DOI] [PubMed] [Google Scholar]