

Abstract
Background
Impulsive behavior is a prominent characteristic of antisocial personality disorder. Impulsivity is a complex construct, however, representing distinct domains of cognition and action. Leading models refer to impulsivity as an inability to evaluate a stimulus fully before responding to it (rapid-response impulsivity), and as an inability to delay responding despite a larger reward (reward-delay impulsivity). We investigated these models in terms of the diagnosis and severity of antisocial personality disorder.
Methods
Thirty-four male subjects on probation/parole who met DSM-IV criteria for ASPD, and 30 male healthy comparison subjects, matched by ethnicity, were recruited from the community. The Barratt Impulsiveness Scale (BIS-11) provided an integrated measure of trait impulsivity. Rapid-response impulsivity was assessed using the Immediate Memory Task (IMT), a continuous performance test. Reward delay impulsivity was assessed using the Two-choice Impulsivity Paradigm (TCIP), where subjects had the choice of smaller-sooner or larger-delayed rewards, and the Single Key Impulsivity Paradigm (SKIP), a free operant responding task.
Results
Compared to controls, subjects with ASPD had higher BIS-11 scores (Effect Size (E.S.) = 0.95). They had slower reaction times to IMT commission errors (E.S. = 0.45). Correct detections, a measure of attention, were identical to controls. On the SKIP, they had a shorter maximum delay for reward (E.S. = 0.76), but this was not significant after correction for age and education. The groups did not differ on impulsive choices on the TCIP (E.S. < 0.1). On probit analysis with age and education as additional independent variables, BIS-11 score, IMT reaction time to a commission error, and IMT positive response bias contributed significantly to diagnosis of ASPD; SKIP delay for reward did not. Severity of ASPD, assessed by the number of ASPD symptoms endorsed on the SCID-II, correlated significantly with commission errors (impulsive responses) on the IMT, and with liberal IMT response bias. This relationship persisted with correction for age and education.
Discussion
These results suggest that ASPD is characterized by increased rapid-response impulsivity. Aspects of impulsivity related to reward-delay or attention appear relatively intact.
Keywords: Antisocial personality disorder, impulsive behavior, impulse control disorders, attention, reward
Introduction
Impulsivity, defined as a propensity to act without the apparent capacity to adapt behavior to contextual demands, is prominent in many psychiatric disorders (Moeller et al., 2001). Impulsivity is complex, comprising neural mechanisms that could relate to distinct aspects of cognition. Two mechanisms involved in impulsivity, which may differ in mechanisms and treatments, are the inability to evaluate a stimulus adequately before responding to it (rapid-response impulsivity), and the inability to delay responding to an immediate small reward for a delayed larger one (reward-delay or delay-discounting impulsivity) (Swann et al., 2002;Evenden, 1999).
Impulsivity plays a central role in the so-called cluster B personality disorders, including antisocial personality disorder (ASPD) (American Psychiatric Association, 1995;First et al., 1997). ASPD is a common and potentially dangerous disorder, characterized by poor impulse control and destructive behavior that begins in childhood and persists into adulthood (American Psychiatric Association, 1995). In contrast with positive effects of treatment in individuals with impulsive aggression (Sheard et al., 1976;Barratt et al., 1997;Stanford et al., 2005), there is no systematic or reliably effective treatment specifically for ASPD.
ASPD and impulsivity
There is relatively little information on quantitative measures of impulsivity in ASPD. An integrated questionnaire measure of impulsivity, the Barratt Impulsiveness Scale (BIS-11) (Barratt & Patton, 1983) is increased in adults with histories of conduct disorder (Dougherty et al., 2000a), adults with ASPD or with adult antisocial behavior (Lijffijt et al., 2008), and in adolescents with disruptive behavior disorders (Dougherty et al., 2003) and their parents (Swann et al., 2002). BIS-11 Motor impulsiveness, related to acting without thinking, was increased in subjects with ASPD who were identified in a nonclinical sample (Fossati et al., 2004) and correlated with symptoms of ASPD and borderline personality disorder (Fossati et al., 2004;Fossati et al., 2007).
In subjects with ASPD and substance-use disorders, there appears to be an additive increase in reward-delay impulsivity, though the task used fictitious rewards and there was no group with ASPD only (Petry, 2002). A study of ASPD and alcohol use disorder found reward-delay impulsivity to be increased as a marker for alcohol-use disorder, but rapid-response impulsivity (measured using a CPT) to be increased largely in the subgroup of subjects with both alcohol-use disorder and a cluster B personality disorder (ASPD or borderline personality disorder) (Rubio et al., 2007). Similarly, another study found that subjects with ASPD performed normally on the Iowa Gambling Task but had impaired performance in a Stroop test designed to measure impulsivity (Vassileva et al., 2007).
Impulsivity, therefore, appears to be a core characteristic of ASPD that may link it to other Cluster B personality disorders, and may relate more to an inability to withhold responding until stimuli are fully processed (rapid-response) than to an inability to delay responding for a larger reward. However, the evidence is limited. Other characteristics commonly found in subjects with ASPD may confound assessment of the specific role of impulsivity. For example, impulsivity has complex potential relationships with education, since impulsivity can interfere with completion of education and education can provide tools to compensate for impulsivity (Nusslock et al., 2008). We have reported that impulsivity in either clinical or nonclinical samples is potentially influenced by age and education (Swann et al., 2008a;Swann et al., 2008b). Ethnicity also may alter the relationship between impulsivity and antisocial traits (Jackson et al., 2007).
Aims and Hypotheses
We have compared impulsivity in subjects with ASPD to that in controls. We used 1) an integrated measure of impulsivity, the BIS-11, 2) the Immediate Memory Task (IMT), a measure of rapid-response impulsivity based on the Continuous Performance Test, and 3) the Single Key Impulsivity Paradigm (SKIP) and Two-Choice Impulsivity Paradigm (TCIP), measures of ability to delay response for a larger reward. Our hypotheses were that subjects with ASPD would have 1) higher BIS-11 scores than controls, 2) abnormal performance on the IMT consistent with greater rapid-response impulsivity, and 3) relatively intact performance on the TCIP or SKIP, tests of ability to delay reward. In terms of these hypotheses, we investigated characteristics of impulsivity in subjects with ASPD and healthy controls, evaluating potential roles of age, education, and ethnicity, and relationships to severity of ASPD symptoms.
Methods
This study was reviewed and approved by the Committee for the Protection of Human Subjects (CPHS), the IRB for The University of Texas Health Science Center at Houston. Before any research-related procedures were carried out, the study was explained thoroughly to subjects and they were given ample opportunity to answer any questions. Subjects then signed informed consent documents approved by the CPHS. All advertisements, flyers, and other study-related material had prior CPHS approval.
Subjects
Subjects were recruited through advertisements in the local press for healthy subjects or for subjects who were on probation/parole. The ASPD group included 34 men and only 5 women; the analyses in this report were limited to men. Healthy controls (not meeting DSMIV criteria for any Axis I or II disorder including substance-related disorders) included 36 men but 6 were Asians, while no ASPD subjects were Asian, so the Asian controls were excluded from the current analysis, leaving 30 healthy comparison subjects. ASPD subjects could have histories of substance or alcohol abuse or dependence, and could have current substance or alcohol use, but were excluded if they currently met DSM-IV criteria for alcohol or other substance abuse or dependence. All subjects with ASPD and histories of a substance-use disorder met criteria for ASPD at an earlier age than that at which they met criteria for a substance—use disorder. At the time that they were studied, subjects were required to have negative screens for drugs of abuse (urine) and alcohol (breath).
Measures
Diagnostic
Diagnoses were rendered using the SCID-II (First et al., 1997); the SCID-I was also administered in order to identify comorbidities and to assure that subjects did not have schizophrenia or bipolar disorder, exclusion criteria (First et al., 1996). Raters were trained in these instruments, using standard training tapes and manuals. Diagnoses from structured clinical interviews were verified in consensus meetings that included co-authors ACS, JLS, and FGM.
Barratt Impulsiveness Scale (BIS-11)
This BIS-11 is a well-validated 30-item self-rated measure of impulsivity as a stable trait (Barratt & Patton, 1983). It has three oblique factors: attentional impulsivity, measuring cognitive instability; motor impulsivity, measuring impetuousness and acting on the spur of the moment; and nonplanning impulsivity, measuring lack of a sense of the future (Patton et al., 1995).
Rapid-response impulsivity: Immediate Memory Task (IMT)
The IMT is a continuous Performance Test developed to assess impulsivity and attention (Dougherty et al., 2000b). 5-digit numbers are displayed on a computer screen for 0.5 seconds, with 0.5 seconds between stimuli. Subjects are instructed to respond as quickly as possible when they see a number that matches the previous one. There are three types of responses: correct detections (CD), where the stimulus exactly matches the one before it; commission errors (CE), where 4 of 5 digits match (the position in the 5-digit sequence of the nonmatching digit is varied randomly); and filler errors, where the number has no relationship to the one before it. Reaction times to CD or CE are also measured, and there are two parameters derived from signal detection theory: discriminability, ranging from 0.5 – 1, where a higher value reflects ability to distinguish target from off-target stimuli (A′), and response bias (beta), ranging from -1 to 1, where a higher value reflects a conservative response bias with low rates of commission errors but also of correct detections (Donaldson, 1992;Green & Swets, 1966).
Reward-delay impulsivity: Single key Impulsivity Paradigm (SKIP)
The SKIP is a free operant responding test designed to measure ability to delay response for a larger reward (Dougherty et al., 2005;Dougherty et al., 2003). Unlike two-choice tests, the duration of the task does not depend on responses by the subject. Subjects are instructed that they can press a button to obtain money, and that the longer they wait, the more money they will get. The amount obtained (cumulative and for each response) is displayed on the computer screen. The total number of responses, average delay, shortest delay, and longest delay are recorded.
Reward-delay impulsivity: Two-Choice Impulsivity Paradigm (TCIP)
This procedure gives the subject a choice between receiving a small reward after a 5 sec delay or a larger reward after a 15-sec delay (Dougherty et al., 2003). Subjects are told they will receive 5c after 5 sec or 15c after 15 sec. A counter displays results on the computer screen. Short-delay responses are taken as impulsive responses (Cherek et al., 1997;Cherek & Lane, 1999;Dougherty et al., 2003). This procedure has been widely used by our and other groups in studies of potentially impulsive populations (Cherek et al., 1997;Cherek & Lane, 1999;Dougherty et al., 2003).
Statistical analysis
Before analysis, data were checked for normality of distribution. Data with non-normal distribution were either log-transformed or analyzed using appropriate nonparametric methods. Two-way comparisons used independent-samples t tests. Effect sizes were calculated using the difference divided by the pooled standard deviation, weighted by sample size (Lipsey & Wilson, 2001). Prediction of continuous dependent variables by combinations of categorical and continuous independent variables used general linear models (GLM) analysis. For basic comparisons, we used GLM with experimental group as a dichotomous independent variable and age and education as dependent variables, because both age (Stevenson et al., 2003;Keilp et al., 2005) and education (Keilp et al., 2005;Nusslock et al., 2008) can potentially influence impulsivity and differed between groups (see Results). Prediction of binomial variables (ie, presence or absence of ASPD) by combinations of categorical and continuous variables used probit analysis (Gibbons & Hedeker, 1994). Means are presented with standard deviations (SD). Effects were considered statistically significant if two-tailed p < 0.05.
Results
Characteristics of subjects
The 34 subjects with ASPD differed from 30 healthy comparison subjects in age (ASPD 38.7 ± 10.3 vs controls 31.5 ± 9.5, t = 3.02, p = 0.004) and education (ASPD 12.7 ± 2.1 vs controls 15 ± 2.4, t = 4.1, p = 0.0001). Because of these differences, we controlled for effects of age and education in the analyses in this report. Ethnic/racial composition of the two groups was similar (African-American 14 controls and 14 ASPD, Hispanic 5 controls and 7 ASPD, Caucasian 11 controls and 13 ASPD; X2 (df=2) = 0.25, p = 0.88).
BIS-11 Scores
GLM analysis, with diagnosis as categorical independent variable and age and education as continuous independent variables, is summarized in Table 1. There were significant effects of group on total BIS-11 scores and on each factor score, without significant effects of age or education.
Table 1. BIS-11 Scores in Subjects with ASPD and Controls.
| Score | Controls (n=30) |
ASPD (n=32) |
t | p | Effect size |
|---|---|---|---|---|---|
| Total | 55.6 ± 7.9 | 66.2 ± 11.3 | 4.5 | 0.00003 | 0.97 |
| Nonplanning | 20.8 ± 4.5 | 25.8 ± 4.9 | 4.4 | 0.00004 | 0.95 |
| Motor | 20.9 ± 3.2 | 24.4 ± 4.5 | 3.7 | 0.0004 | 0.83 |
| Attentional | 13.9 ± 3.8 | 16.1 ± 3.8 | 2.4 | 0.02 | 0.56 |
Scores are given with SD.
IMT performance
Table 2 summarizes GLM analysis of IMT performance in subjects with ASPD and controls. Subjects with ASPD had significantly slower reaction times to a commission error than controls, with a trend toward slower reaction times to a correct detection. In addition, there were significant effects of education on commission errors and on reaction time to a commission error.
Table 2. IMT Performance in Subjects with ASPD and Controls.
| Measure | Controls (n=30) |
ASPD (n=32) |
t | P | Effect size |
|---|---|---|---|---|---|
| Correct detections (CD) | 83.5 ± 10.5 | 85.9 ± 10.8 | 0.9 | 0.4 | 0.23 |
| Commission errors (CE) | 24.6 ± 15.3 | 28.8 ± 14.2 | 1.1 | 0.3 | 0.28 |
| CE/CD | 0.239 ± 0.125 | 0.265 ± 0.209 | 0.5 | 0.6 | 0.13 |
| CD reaction time | 456 ± 73 | 491 ± 68 | 1.9 | 0.055 | 0.48 |
| CE reaction time | 453 ± 78 | 498 ± 76 | 2.3 | 0.028 | 0.56 |
| Discriminability | 0.873 ± 0.058 | 0.865 ± 0.065 | 0.5 | 0.6 | 0.09 |
| Response bias | -0.181 ± 0.525 | -0.419 ± 0.390 | 2 | 0.049 | 0.50 |
Correct detections (CD) and commission errors (CE) are in percent; reaction times are in msec; discriminability and response bias do not have units.
There were consistent negative correlations between commission errors and education (for all subjects, r = -0.28, p < 0.01) and positive correlations between education and discriminability (r = 0.24 for all subjects, r = 0.31 in ASPD). There were significant effects of education on commission errors (F=6.3, p = 0.015) and reaction time to a commission error (F=5.1, p = 0.03). There were no significant effects of age.
SKIP performance
Scores on the SKIP are summarized in Table 3. Subjects with ASPD had shorter maximal delay to a response (ES = 0.76) and more responses (ES = 0.46) but these differences were not significant after accounting for age and education on GLM analysis. This is consistent with the significant correlation between education and maximum delay (r = 0.287, p = 0.034).
Table 3. SKIP Performance in Subjects with ASPD and Controls.
| Measure | Controls (n=30) |
ASPD (n=32) |
t | P | Effect size |
|---|---|---|---|---|---|
| Responses | 3.952 ± 2.265 | 4.46 ± 1.836 | 0.9 | 0.36 | 0.25 |
| Shortest delay | 0.648 ± 2.386 | -0.137 ± 0.126 | 1.1 | 0.3 | 0.32 |
| Longest delay | 5.152 ± 1.275 | 4.477 ± 1.698 | 2.2 | 0.03 | 0.57 |
All SKIP variables were log-transformed.
TCIP performance
Table 4 summarizes TCIP performance. There were no significant group differences for any measure. Further, neither age nor education made significant contributions (though their effects appeared larger than those of diagnostic group).
Table 4. TCIP Performance in Subjects with ASPD and Controls.
| Measure | Percent immediate responses | Maximum consecutive delayed responses |
|---|---|---|
| Controls (n=23) | 26.9 ± 27.6 | 26.7 ± 19.4 |
| ASPD (n=24) | 33.0 ± 29.1 | 24.3 ± 16.7 |
| Effect Size | 0.22 | 0.18 |
| F (df 1,45) Group | 0.05 (0.8) | 0.40 (0.6) |
| F (df 1,45) Age | 0.73 (0.4) | 1.35 (0.3) |
| F (df 1,45) Education | 0.60 (0.5) | 1.59 (0.3) |
Relative contributions of different impulsivity-related measures to ASPD diagnosis
In order to estimate the relative contributions of the impulsivity-related measures to the difference between comparison subjects and subjects with ASPD, we conducted a probit analysis that included the measures that showed significant or near-significant group differences, including age and education, as independent variables; experimental group (control or ASPD) was included as dependent variable. As shown in Table 5, BIS-11 total score, IMT reaction time to a commission error, and IMT response bias all contributed significantly to the model, while age, education, and SKIP maximal response delay did not.
Table 5. Probit analysis of impulsivity-related measures and ASPD.
| Independent Variable | Wald statistic | P |
|---|---|---|
| Age | 2.69 | 0.10 |
| Education | 2.24 | 0.13 |
| BIS-11 Total | 6.73 | 0.01 |
| IMT reaction time to CE | 6.44 | 0.01 |
| IMT response bias (beta) | 4.67 | 0.03 |
| SKIP maximal delay | 2.92 | 0.11 |
Presence/absence of ASPD was the dependent variable
Relationships to severity and clinical features
In order to determine relationships between impulsivity-related measures and severity of ASPD, we investigated relationships between the number of SCID-II ASPD symptoms endorsed and measures of impulsivity. The number of symptoms had a normal-appearing distribution (median = 6, Kolmogorov-Smirnov p > 0.1) but because of the discrete nature of the variable, in addition to the Pearson r we required that the nonparametric Kendall tau statistic also be statistically significant. The number of endorsed ASPD symptoms correlated significantly with IMT commission errors (r = 0.62, n=25, p = 0.001), and IMT discriminability (r = -0.42, n = 25, p = 0.037). Figure 1 shows the relationship between symptoms and commission errors. The number of symptoms did not correlate significantly with BIS-11 scores (r < 0.11) or IMT reaction times or correct detection rates (all P > 0.5), showing that the variables that correlated with severity within subjects with ASPD were different from the variables that distinguished subjects with ASPD from controls. Finally, we entered the variables having significant or near-significant (p < 0.1) correlations with ASPD symptoms, and potential confounding variables of age and education, into a GLM analysis, with ASPD symptoms as dependent variable. In the resulting model, only IMT commission errors contributed significantly to number of ASPD symptoms (F(1,18)=5.3, p = 0.035).
Figure 1.
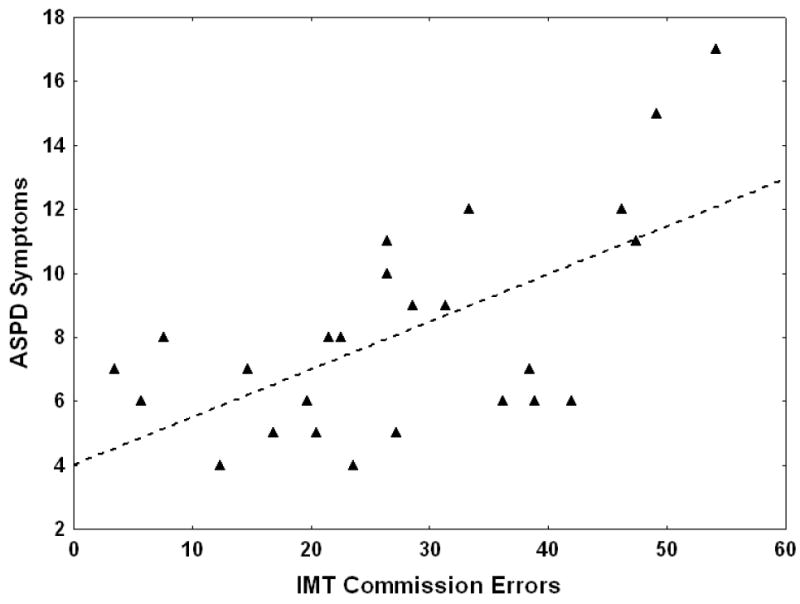
ASPD symptoms and IMT commission errors (r = 0.62, n = 25, p = 0.001). The horizontal axis shows the rate of IMT commission errors as a percentage of stimuli with 4 of 5 digits correct. The vertical axis shows the number of ASPD symptoms endorsed (SCID-II).
Of the 34 subjects with ASPD, 21 had a substance use disorder (dependence or abuse) by SCID-DSMIV and 13 did not; 20 had an alcohol-use disorder while 14 did not. Subjects with an alcohol-use disorder, a substance-use disorder, or either an alcohol- or a substance use disorder did not differ significantly from remaining subjects with respect to BIS-11 scores (t < 1, p > 0.4), IMT measures (t < 1.5, P > 0.2), TCP measures (t < 1, p > 0.4), or SKIP parameters (t < 1.5, P > 0.2). While the number of subjects was limited, none of the comparisons even approached statistical significance.
Definite smoking histories were available for 27 subjects with ASPD, of whom 14 were smokers. Smokers had higher BIS-11 nonplanning scores than nonsmokers (28.3 ± 4.9 vs 23.9 ± 3.7, t = 2.6, p = 0.016), with a trend toward higher BIS-11 total scores (70.9 ± 12.1 vs 63.6 ± 9.2, t = 1.7, p = 0.09). No other measures (education, age, IMT, TCP, SKIP) had t > 1.5. Neither substance-related disorder nor smoking history was related to total ASPD symptoms (Mann-Whitney or Student t-test, p > 0.8).
Discussion
Integrated impulsivity, assessed by the BIS-11, was increased in subjects with ASPD. This increase was not accounted for by age, ethnicity, or education. Subjects with ASPD also had slower reaction times, especially to a commission error, than healthy controls, but did not differ in correct detection rates. ASPD subjects appeared to have reduced ability to delay response for a larger reward, but this was accounted for by demographic characteristics. BIS-11 scores and delayed reaction time to commission errors were the features that most strongly predicted diagnosis of ASPD. Interestingly, severity of ASPD did not correlate with these measures, but correlated most strongly with commission error rates. These results suggest that more severe ASPD behavior is related most strongly to impaired response inhibition. Severity of ASPD or the diagnosis of ASPD per se appeared unrelated to attention. Interpretation requires consideration of the nature of the group of subjects studied, and characteristics of the measures used.
BIS-11 scores
The BIS-11 was developed to measure multiple facets of impulsivity and to differentiate it from other action-oriented traits and from characteristics like anxiety and aggression. Its three factors are attentional (lack of ability to maintain cognitive focus or persistence), motor (acting on the spur of the moment) and nonplanning (lack of a future sense) (Patton et al., 1995). Subjects with ASPD differed most strongly from controls in nonplanning and motor impulsivity and less strongly in attentional impulsivity. This resembles our results with parents of children with disruptive behavior disorders (Swann et al., 2002) and adolescents with conduct disorder (Dougherty et al., 2003), consistent with the finding that attention, at least as reflected by IMT correct detection rates and discriminability, was intact in subjects with ASPD. By contrast, we have found attentional impulsivity to be associated with Axis I diagnosis (Swann et al., 2002) and subjects with bipolar disorder to have impaired attention, manifested by reduced IMT correct detection rates (Swann et al., 2008b). However, BIS-11 attentional impulsivity is not specifically a measure of attention, but reflects aspects of impulsivity that are related to cognitive instability and lack of tolerance for complexity (Patton et al., 1995). Therefore it measures a domain that is affected by many Axis I disorders and that differs from, but may overlap with, attention.
Rapid-response impulsivity: IMT performance
IMT performance measures aspects of cognition related to rapid-response impulsivity. Subjects with ASPD had significantly slower reaction times to a commission error than controls, suggesting that the ability to withhold the response was more difficult to organize in that group than in controls, resembling another report of delayed reaction times on a Stroop test (Vassileva et al., 2007).
ASPD subjects had a more liberal response bias (Table 4), which seems inconsistent with the slower reaction times. Slower reaction times are generally associated with a more conservative response bias, potentially resulting in fewer commission errors at the expense of fewer correct detections. Instead, subjects with ASPD had slower reaction time with a more liberal response bias, potentially biasing toward correct detections at the expense of more commission errors. As the two groups did not differ on rates of correct detections or commission errors, these results suggest that slower reaction times in ASPD represent a partial compensation for disrupted information processing prior to generating the response. This compensation resulted in correct detection and commission error rates resembling controls. The finding that the groups did not differ on discriminability supports the conclusion that the abnormal process in ASPD is not primarily related to attention.
On the other hand, severity of ASPD correlated with increased commission error rates but not with reaction times. This suggests that severity in ASPD is related to diminished response inhibition. As severity did not correlate significantly with correct detections or response times, the relationship with commission errors did not appear related to deficient attention or to changes in speed of generating responses. Instead, our findings suggest that, with increasing severity, the compensatory mechanism reflected by slower reaction times fails, with uncompensated deficient response inhibition leading to increased commission error rates. Deficient response inhibition in subjects with ASPD, partially compensated by slower response times, breaks through in subjects with more severe ASPD. The data, therefore, are consistent with impaired response inhibition, correlating with severity, in ASPD.
These findings are similar to our previous report in parents of adolescents with disruptive behavior disorders (Swann et al., 2002). Furthermore, among subjects with alcohol-use disorders, those with cluster B personality disorders had impairment in response inhibition tasks that led the authors to conclude that presence of cluster B personality disorder was associated with behavioral disinhibition (Rubio et al., 2007). Subjects with ASPD also had impaired performance on tasks that required suppression of a prepotent response (Newman et al., 1985;Howland et al., 1993).
Reward-delay impulsivity: SKIP
Impulsivity could also be related to an inability to delay responding for a larger reward. This, in turn, is related to what might be considered the afferent arm of impulsivity, inability to consider the consequences of behavior, and subsequently plan future behavior. We assessed this aspect of impulsivity using the SKIP, essentially a free-operant task where a subject presses a key for money, instructed that the amount of money increases as the delay increases (Dougherty et al., 2003). Compared with traditional two-choice tasks, this procedure has the advantages that response choices do not influence the duration of the task, and that the subject is not responding to discrete stimuli. A disadvantage is that it is not possible to construct a delay discounting curve; the task is designed to measure inability to withhold a response regardless of mechanism.
SKIP responses are increased in adolescents with disruptive behavior disorders (Dougherty et al., 2003), and in adults with bipolar disorder (Swann et al, in press b) and with histories of suicide attempts (Dougherty et al., 2004); the maximal SKIP delay is decreased in bipolar disorder (Swann et al, in press b). While SKIP delays were shorter in ASPD in the current study, this difference did not persist with GLM or probit analysis accounting for demographic characteristics, so the impairment in response inhibition described above appears not to be related to inability to delay a reward. One study in which ASPD was apparently associated with inability to delay reward used prolonged delay times and manifestly fictitious rewards; furthermore, all subjects had a substance use disorder, so the results may not have been specifically relevant to this aspect of impulsivity or to ASPD (Petry, 2002). In summary, ASPD appears not to be primarily related to inability to delay reward.
Reward-delay impulsivity:TCIP
Subjects with ASPD did not differ from controls in TCIP measures, and TCIP scores were also not related to comorbidities or number of ASPD symptoms. This is consistent with the data in Tables 2 and 3 suggesting that increased impulsivity in ASPD is largely related to rapid-response impulsivity. Some studies of aggressive subjects, mostly with ASPD, have reported increased impulsive responding on the TCIP (Cherek & Lane, 1999;Dougherty et al., 2003;Cherek et al., 1997). However, when performance on different impulsivity tests were compared, differences in TCIP were smaller than differences in SKIP, and differences in SKIP were smaller than differences in IMT performance (Dougherty et al., 2003).
Limitations
In interpreting these data, one must consider several factors involving the sample and methods: 1) The sample size was relatively small, yielding limited statistical power to evaluate complex interactions among multiple impulsivity and demographic measures. 2) The sample consisted entirely of men. There were too few women in our study group for meaningful analysis of gender effects, consistent with the epidemiology of ASPD. It has been suggested that ASPD and borderline personality disorder are parallel disorders across gender (Paris, 1997). 3) The SKIP is less established than 2-choice methods in measuring reward-delay impulsivity. Its advantage is its simplicity, and its relative isolation of ability to delay a reward from other aspects of attention or disinhibition. 4) Number of symptoms endorsed may not be an ideal measure of ASPD severity, due to variable recall and to variable relationships between specific symptoms and overall severity. Number of Cluster B symptoms has been previously shown to be related to laboratory-measured impulsivity (Swann et al., 2002), however, and can be considered a more continuous and generalizable measure of personality disturbance than histories of specific severe acts.
Conclusion
Compared with healthy comparison subjects, subjects with ASPD had greater impulsivity as reflected by increased BIS-11 scores (especially nonplanning and motor), and increased IMT commission error reaction times, which may reflect a partial compensation mechanism related to impaired response inhibition, which becomes more apparent with more severe ASPD, when the number of ASPD symptoms correlates negatively with commission error reaction times. These differences were not due to ethnicity, age, or education. The data support a relationship between ASPD and impaired response inhibition, in which attention and the ability to delay reward are relatively intact.
Acknowledgments
This study was supported in part by the Pat R Rutherford, Jr Chair in Psychiatry (ACS) and by NIH grants RO1-MH69944 (ACS), RO1-DA08425 (FGM), KO2-DA00403 (FGM), and UL1-RR024148 (CTSA; General Clinical Research Center UT Houston). We thank Blake Cox, Stacy Maier, Leslie Paith, Irshad Prasla, Tammy Souter, R.N., and Anthony Zamudio, R.N., for their skilled assistance.
Role of funding source: This project was funded by NIH RO1 grants MH69944 and DA 08425, NIH K award K02 DA00403, and a CCTS award, UL-RR-24148, which supported the Clinical Research Unit on which some studies were conducted. In addition there was funding support from an endowment, the Rutherford Chair in Psychiatry. None of the funding sources was involved in the design or conduct of the studies, the analysis or interpretation of the data, the decision to publish, or the content or preparation of the manuscript.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Contributors: Aan C. Swann MD was primarily responsible for the design and conduct of the study, the analysis of the data, writing the first draft of the manuscript, and coordinating editing and revisions.
Marijn Lijffijt PhD prepared the database, conducted statistical analyses, supervised work with subjects, and participated in revising and editing the manuscript.
Scott Lane PhD participated in design of the studies, design and interpretation of human laboratory studies, and revising and editing the manuscript.
Joel Steinberg MD participated in design of the studies, developing statistical strategies, and revising and editing the manuscript.
Frederick Moeller MD participated in design of the studies, supervision of the research group, and revising and editing the manuscript.
Reference List
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th. Washington, D.C.: APA; 1995. [Google Scholar]
- Barratt ES, Patton JH. Impulsivity: Cognitive, behavioral, and psychophysiological correlates. In: Zuckerman M, editor. Biological Basis of Sensation-seeking, Impulsivity, and Anxiety. Hillsdale, New Jersey: Lawrence Erlbaum Associates; 1983. pp. 77–116. [Google Scholar]
- Barratt ES, Stanford MS, Felthous AR, Kent TA. The effects of phenytoin on impulsive and premeditated aggression: a controlled study. J Clin Psychopharmacol. 1997;17:341–349. doi: 10.1097/00004714-199710000-00002. [DOI] [PubMed] [Google Scholar]
- Cherek DR, Lane SD. Laboratory and psychometric measurements of impulsivity among violent and nonviolent female parolees. Biological Psychiatry. 1999;46:273–280. doi: 10.1016/s0006-3223(98)00309-6. [DOI] [PubMed] [Google Scholar]
- Cherek DR, Moeller FG, Dougherty DM, Rhoades H. Studies of violent and nonviolent male parolees: II. Laboratory and psychometric measurements of impulsivity. Biological Psychiatry. 1997;41:523–529. doi: 10.1016/s0006-3223(96)00426-x. [DOI] [PubMed] [Google Scholar]
- Donaldson W. Measuring recognition memory. J Exp Psychol Gen. 1992;121:275–277. doi: 10.1037//0096-3445.121.3.275. [DOI] [PubMed] [Google Scholar]
- Dougherty DM, Bjork JM, Harper RA, Marsh DM, Moeller FG, Mathias CW, Swann AC. Behavioral impulsivity paradigms: A comparison in hospitalized adolescents with disruptive behavior disorders. J Child Psychol Psychiatry. 2003;44:1145–1157. doi: 10.1111/1469-7610.00197. [DOI] [PubMed] [Google Scholar]
- Dougherty DM, Bjork JM, Marsh DM, Moeller FG. A comparison between adults with conduct disorder and normal controls on a continuous performance test: Differences in impulsive response characteristics. Psychological Record. 2000a;50:203–219. [Google Scholar]
- Dougherty DM, Bjork JM, Marsh DM, Moeller FG. A comparison between adults with conduct disorder and normal controls on a Continuous Performance Test: Differences in impulsive response characteristics. Psychological Record. 2000b;50:203–219. [Google Scholar]
- Dougherty DM, Mathias CW, Marsh DM, Jagar AA. Laboratory behavioral measures of impulsivity. Behav Res Methods. 2005;37:82–90. doi: 10.3758/bf03206401. [DOI] [PubMed] [Google Scholar]
- Dougherty DM, Mathias CW, Marsh DM, Papageorgiou TD, Swann AC, Moeller FG. Laboratory-measured behavioral impulsivity relates to suicide attempt history. Suicide and Life-Threatening Behavior. 2004 doi: 10.1521/suli.34.4.374.53738. In press. [DOI] [PubMed] [Google Scholar]
- Evenden JL. Varieties of impulsivity. Psychopharmacology (Berl) 1999;146:348–361. doi: 10.1007/pl00005481. [DOI] [PubMed] [Google Scholar]
- First MB, Gibbon M, Spitzer RL, Williams JB, Benjamin L. Structured Clinical Interview for DSM-IV Axis II Personality Disorders (SCID-II) New York: Biometrics Research Institute; New York State Psychiatric Institute; 1997. [Google Scholar]
- First MB, Spitzer RL, Gibbon M, Williams JB. Structured Clinical Interview for DSM-IV Axis I Disorders Patient Edition. New York: Biometrics Research Institute; New York State Psychiatric Institute; 1996. [Google Scholar]
- Fossati A, Barratt ES, Borroni S, Villa D, Grazioli F, Maffei C. Impulsivity, aggressiveness, and DSM-IV personality disorders. Psychiatry Research. 2007;149:157–167. doi: 10.1016/j.psychres.2006.03.011. [DOI] [PubMed] [Google Scholar]
- Fossati A, Barratt ES, Carretta I, Leonardi B, Grazioli F, Maffei C. Predicting borderline and antisocial personality disorder features in nonclinical subjects using measures of impulsivity and aggressiveness. Psychiatry Res. 2004;125:161–170. doi: 10.1016/j.psychres.2003.12.001. [DOI] [PubMed] [Google Scholar]
- Gibbons RD, Hedeker D. Application of random-effects probit regression models. J Consult Clin Psychol. 1994;62:285–296. doi: 10.1037//0022-006x.62.2.285. [DOI] [PubMed] [Google Scholar]
- Green DM, Swets JA. Signal Detection Theory and Psychophysics. New York: Wiley; 1966. [Google Scholar]
- Howland EW, Kosson DS, Patterson CM, Newman JP. Altering a dominant response: performance of psychopaths and low-socialization college students on a cued reaction time task. J Abnorm Psychol. 1993;102:379–387. doi: 10.1037//0021-843x.102.3.379. [DOI] [PubMed] [Google Scholar]
- Jackson RL, Neumann CS, Vitacco MJ. Impulsivity, anger, and psychopathy: the moderating effect of ethnicity. J Personal Disord. 2007;21:289–304. doi: 10.1521/pedi.2007.21.3.289. [DOI] [PubMed] [Google Scholar]
- Keilp JG, Sackeim HA, Mann JJ. Correlates of trait impulsiveness in performance measures and neuropsychological tests. Psychiatry Res. 2005;135:191–201. doi: 10.1016/j.psychres.2005.03.006. [DOI] [PubMed] [Google Scholar]
- Lijffijt M, Moeller FG, Boutros NN, Burroughs S, Steinberg JL, Lane SD, Swann AC. A pilot study revealing impaired P50 gating in childhood-onset but not adult-onset antisocial behavior. J Neuropsychiatry Clin Neurosci. doi: 10.1176/appi.neuropsych.21.3.328. In press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lipsey MW, Wilson DB. Practical Meta-Analysis. Thousand Oaks, CA: Sage Publications; 2001. [Google Scholar]
- Moeller FG, Barratt ES, Dougherty DM, Schmitz JM, Swann AC. Psychiatric aspects of impulsivity. American Journal of Psychiatry. 2001;158:1783–1793. doi: 10.1176/appi.ajp.158.11.1783. [DOI] [PubMed] [Google Scholar]
- Newman JP, Widom CS, Nathan S. Passive avoidance in syndromes of disinhibition: psychopathy and extraversion. J Pers Soc Psychol. 1985;48:1316–1327. doi: 10.1037//0022-3514.48.5.1316. [DOI] [PubMed] [Google Scholar]
- Nusslock R, Alloy LB, Abramson LY, Harmon-Jones E, Hogan ME. Impairment in the achievement domain in bipolar spectrum disorders: role of behavioral approach system hypersensitivity and impulsivity. Minerva Pediatr. 2008;60:41–50. [PubMed] [Google Scholar]
- Paris J. Antisocial and borderline personality disorders: two separate diagnoses or two aspects of the same psychopathology? Comprehensive Psychiatry. 1997;38:237–242. doi: 10.1016/s0010-440x(97)90032-8. [DOI] [PubMed] [Google Scholar]
- Patton JH, Stanford MS, Barratt ES. Factor structure of the Barratt impulsiveness scale. J Clin Psychol. 1995;51:768–774. doi: 10.1002/1097-4679(199511)51:6<768::aid-jclp2270510607>3.0.co;2-1. [DOI] [PubMed] [Google Scholar]
- Petry NM. Discounting of delayed rewards in substance abusers: relationship to antisocial personality disorder. Psychopharmacology (Berl) 2002;162:425–432. doi: 10.1007/s00213-002-1115-1. [DOI] [PubMed] [Google Scholar]
- Rubio G, Jimenez M, Rodriguez-Jimenez R, Martinez I, Iribarren MM, Jimenez-Arriero MA, Ponce G, AVila C. Varieties of impulsivity in males with alcohol dependence: the role of Cluster-B personality disorder. Alcohol Clin Exp Res. 2007;31:1826–1832. doi: 10.1111/j.1530-0277.2007.00506.x. [DOI] [PubMed] [Google Scholar]
- Sheard MH, Marini JL, Bridges CI, Wagner E. The effect of lithium on impulsive aggressive behavior in man. American Journal of Psychiatry. 1976;133:1409–1413. doi: 10.1176/ajp.133.12.1409. [DOI] [PubMed] [Google Scholar]
- Stanford MS, Helfritz LE, Conklin SM, Villemarette-Pittman NR, Greve KW, Adams D, Houston RJ. A comparison of anticonvulsants in the treatment of impulsive aggression. Exp Clin Psychopharmacol. 2005;13:72–77. doi: 10.1037/1064-1297.13.1.72. [DOI] [PubMed] [Google Scholar]
- Stevenson J, Meares R, Comerford A. Diminished impulsivity in older patients with borderline personality disorder. Am J Psychiatry. 2003;160:165–166. doi: 10.1176/appi.ajp.160.1.165. [DOI] [PubMed] [Google Scholar]
- Swann AC, Bjork JM, Moeller FG, Dougherty DM. Two models of impulsivity: Relationship to personality traits and psychopathology. Biological Psychiatry. 2002;51:988–994. doi: 10.1016/s0006-3223(01)01357-9. [DOI] [PubMed] [Google Scholar]
- Swann AC, Lijffijt M, Lane SD, Steinberg JL, Moeller FG. Increased trait-like impulsivity and course of illness in bipolar disorder. Bipolar Disorders. doi: 10.1111/j.1399-5618.2009.00678.x. In press a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Swann AC, Lijffijt M, Lane SD, Steinberg JL, Moeller FG. Severity of bipolar disorder is associated with impairment of response inhibition. J Affective Disord. doi: 10.1016/j.jad.2008.10.022. In press b. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vassileva J, Gonzalez R, Bechara A, Martin EM. Are all drug addicts impulsive? Effects of antisociality and extent of multidrug use on cognitive and motor impulsivity. Addict Behav. 2007;32:3071–3076. doi: 10.1016/j.addbeh.2007.04.017. [DOI] [PMC free article] [PubMed] [Google Scholar]