

Abstract
We performed respiratory-gated magnetic resonance imaging to evaluate airway dynamics during tidal breathing in 10 children with obstructive sleep apnea syndrome (OSAS; age, 4.3 ± 2.3 years) and 10 matched control subjects (age, 5.0 ± 2.0 years). We hypothesized that respiratory cycle fluctuations in upper airway cross-sectional area would be larger in children with OSAS. Methods: Studies were performed under sedation. Respiratory gating was performed automatically at 10, 30, 50, 70, and 90% of inspiratory and expiratory volume. Airway cross-sectional area was measured at four ascending oropharyngeal levels at each increment of the respiratory cycle. Results: We noted the following in subjects with OSAS compared with control subjects: (1) a smaller upper airway cross-sectional area, particularly during inspiration; (2) airway narrowing occurred during inspiration without evidence of complete airway collapse; (3) airway dilatation occurred during expiration, particularly early in the phase; and (4) magnitude of cross-sectional areas fluctuations during tidal breathing noted in OSAS at levels 1 through 4 were 317, 422, 785, and 922%, compared with 19, 15 17, and 24% in control subjects (p < 0.001, p < 0.005, p < 0.001, and p < 0.001, respectively). Conclusions: Fluctuations in airway area during tidal breathing are significantly greater in subjects with OSAS compared with control subjects. Resistive pressure loading is a probable explanation, although increased airway compliance may be a contributing factor.
Keywords: magnetic resonance imaging (MRI), respiratory-gated MRI, upper airway
Obstructive sleep apnea syndrome (OSAS) in children is a common disorder and may affect as many as 2% of children (1, 2). Frequently, OSAS is associated with adenoid and/or tonsillar hypertrophy. However, other anatomic and physiologic factors affecting upper airway size, shape, and function may play a role in the causation of OSAS in children (3).
Studies suggest that the upper airway in children with OSAS is more collapsible compared with control subjects during wakefulness and sleep, and under general anesthesia (4–6). Several mechanisms may lead to more airway collapse in these subjects, including the following: decreased motor tone, increased airway compliance, and excessive inspiratory driving pressures caused by proximal airway narrowing. This increased propensity of the airway to collapse should be reflected by increased motion of airway boundary during respiration as negative upper airway intraluminal pressure is increased. Hence, the quantification of such changes during respiration is important in understanding the pathogenesis of OSAS in children.
Various techniques have been used in recent years to detect dynamic changes in the upper airway including the following: fluoroscopy, cine computed tomography, and fast magnetic resonance imaging (MRI) (7–12). However, newer methodologies capable of gating image acquisition to the respiratory cycle are now becoming available and may further enhance our knowledge about the temporal sequence leading to OSAS.
To this end, we used respiratory-gated MRI to quantify changes in shape and airway cross-section area during tidal breathing in children with OSAS as compared with control subjects. We hypothesized that changes in upper airway cross-sectional area during tidal breathing will be larger in children with OSAS and that maximal narrowing will occur during inspiration when more negative intraluminal pressures are present.
METHODS
The study was approved by the Institutional Review Board of the Children's Hospital of Philadelphia. Informed consent was obtained from each subject's parent, and assent was obtained from children older than 6 years.
Subjects
Children with OSAS were recruited from the pool of patients evaluated for sleep-disordered breathing and adenotonsillar hypertrophy at the Children's Hospital of Philadelphia. After OSAS was confirmed by polysomnography, these subjects underwent an upper airway MRI under sedation.
Control children with normal growth and development and intact tonsils and adenoids were matched to subjects with OSAS. Adenoid and/or tonsillar hypertrophy per se did not exclude them from the study if they did not have symptoms suggestive of OSAS (13). Control subjects were selected from patients who underwent head MRI for other medical indications. Parents gave consent for an upper airway MRI that followed head MRI, with no additional sedation.
Exclusion criteria for control subjects included the following: (1) likelihood of OSAS assessed by standard questionnaire (13); (2) evidence of a brain tumor or a seizure disorder requiring therapy; (3) genetic disorders associated with any craniofacial anomaly; or (4) chronic respiratory disease, such as asthma.
Overnight Polysomnography
For subjects with OSAS, polysomnography was performed 0 to 4 weeks before MRI. Subjects were studied in the Sleep Disorders Center at the Children's Hospital of Philadelphia. The scoring of respiratory variables was performed based on standards set by the American Thoracic Society and previously published data in children (14, 15). Flow was measured using an oral/nasal thermistor and a nasal end-tidal Pco2 catheter. We used the definition of obstructive apnea as the absence of oral/nasal thermistor signal for at least two respiratory cycles associated with out-of-phase movement of the rib cage and abdomen. Hypopnea was defined as a decrease of 50% or more in oral/nasal thermistor signal and a concurrent fall in 4% or more of basal oxygen saturation. Sleep stages were determined by the criteria of Rechtschaffen and Kales (16). Control subjects did not undergo polysomnography; sleep-disordered breathing in these subjects was excluded by a validated questionnaire (13).
Sleep Questionnaire
Symptoms of sleep-disordered breathing were assessed according to a questionnaire developed by Brouillette and coworkers (13). Subjects with scores below –1 are not expected to have OSAS; a score between –1 and 3.5 is considered intermediate, and a score greater than 3.5 is considered highly suggestive of OSAS.
MRI
MRI studies were performed in the Department of Radiology at the Children's Hospital of Philadelphia. All studies were performed under sedation. Sedation was administered as intravenous pentobarbital of 2-mg/kg increments until patients were sedated well enough to render their eyes closed and not move or arouse unless by a verbal or physical stimuli. A maximum of three doses or 200 mg was administered. All subjects were monitored continuously by pulse oximetry and were observed by an intensive care unit physician until recovery (∼ 1 hour).
Images were acquired using a standard, circular, polarized head coil. The patient's head was positioned supine in the soft tissue Frankfort plane (tragus of the ear to orbital fissure) perpendicular to the table. Axial images were obtained on a 1.5-T Siemens Sonata system (Malvern, PA), using a two-dimensional trueFISP sequence with the following parameters: repetition time/echo time (TR/TE)/α = 4.6/2.3/50°; field of view (FOV) = 20 0 × 1 50; matrix (MA) = 25 6 × 1 92; half-Fourier acquisition, acquisition time = 300 milliseconds/slice.
Respiratory gating was performed using the Siemens Sonata gating system. A single respiratory bellows was placed around the lower chest/upper abdomen to obtain an expansion and contraction synchronous with tidal breath inspiratory and expiratory volumes. The bellows-based Vt waveform signal triggered the scanner at preset volume percentage increments. Data for a 40-mm-thick axial slab from the level of the epiglottis to the upper nasopharynx (Figure 1) were obtained by acquiring 10 4-mm-thick slices (0 gap) during 10 successive breaths, each slice gated to the same increment in Vt. Ten slabs were acquired at the following increments: 10, 30, 50, 70, and 90% of inspiration, and 90, 70, 50, 30, and 10% of expiration.
Figure 1.

Midsagittal magnetic resonance image demonstrating the four ascending levels for analysis (thick dotted lines). Level 1 is 4 mm above tip of epiglottis.
Upper airway cross-sectional areas from four consecutive cross-sectional levels 4 mm apart from above the tip of the epiglottis (Figure 1) during 10 phases of tidal breathing were measured using Volumetric Image Display and Analysis (Department of Radiology, University of Iowa, Ames, IA) (VIDA) (17, 18). The following analyses were performed:
Cross-sectional area during each phase of inspiration/expiration.
Minimal cross-sectional area during inspiration.
Maximal cross-sectional area during expiration.
Group mean of the greatest percentage changes in cross-sectional area during a tidal breath ([area maxexpiration − area mininspiration]/area mininspiration) × 100.
Upper airway shape change during inspiration/expiration: to quantify and compare anteroposterior (A-P) and lateral dimension changes in the airway cross-sections, we measured the maximum width along these axes for each image slice. Results for all subjects were averaged for each gated volume phase and oropharyngeal level. The measured A-P and lateral dimensions were used to create a simple geometric model of the airway cross-sections, based on an ellipse.
Validation of Gating System
We assessed the accuracy of the Siemens bellows triggering system in a normal, awake, adult volunteer by measuring the timing of the gating signal of the Siemens Sonata bellows volume trigger signal concurrently with the gating signal produced by a mask/pneumotach-based system at each volume level (10, 30, 50, 70, and 90% of inspiration, and 90, 70, 50, 30, and 10% of expiration). This measurement was repeated 10 times at each phase of tidal breathing. We later determined the percentage differences between each system's triggering times.
Sample Size and Data Analysis
A sample size of 10 subjects in each group was required to obtain 88% power to detect an effect size of 1.5 SD using a two-group t test with a 0.05 two-sided significance level. This effect size assumption was calculated on the basis of a previous study of ours assessing mean airway cross-sectional area in subjects with OSAS and control subjects (18).
Mean and SD were used to summarize continuous variables. For comparisons between the groups for MRI data, demographics, and questionnaire data, we used a two-tailed unpaired t test, Wilcoxon rank test, or χ2 test, as appropriate. A p value of 0.05 or less was considered to indicate statistical significance.
RESULTS
We studied 10 sequential children with adenotonsillar hypertrophy and OSAS; their mean age was 4.3 ± 2.3 years (range, 2.0–7.2 years). The recruitment rate for subjects with OSAS was 30%. In addition, 10 control subjects were studied; their mean age was 5.0 ± 2.0 years (range, 2.6–8.0 years). Control subjects were not significantly different from subjects with OSAS with respect to age, sex, ethnicity, height, or weight (Table 1). All subjects had normal development and cognitive function, intact tonsils and adenoids, and no respiratory disorders or craniofacial anomalies. The primary indications for head MRI in control subjects were as follows: migraine/headache (six subjects), single seizure/febrile convulsion (three subjects), and external ear mass (one subject). Thus, none of these clinical indications would be expected to affect upper airway anatomy.
TABLE 1.
Demographic data
| Subjects with OSAS (n = 10) |
Control Subjects (n = 10) |
|
|---|---|---|
| Age, yr | 4.3 ± 2.3 | 5.0 ± 2.0 |
| Sex, male/female | 8/2 | 7/3 |
| Ethnicity, AA/white | 4/6 | 4/6 |
| Height, cm | 104 ± 18 | 108 ± 16 |
| Weight, kg | 21.2 ± 10.1 | 21.1 ± 7.3 |
| BMI | 18.7 ± 3.9 | 17.8 ± 2.3 |
Definition of abbreviations: AA = African American; BMI = body mass index; OSAS = obstructive sleep apnea syndrome.
Values represent means ± SD; p = not significant.
Polysomnography
For subjects with OSAS the mean total sleep time during polysomnography was 8.1 ± 0.7 hours (Table 2). The mean respiratory variables values during this period were as follows: apnea index, 1.5 ± 1.9; apnea–hypopnea index, 5.7 ± 4.7; SpO2 nadir, 85 ± 5%; peak end-tidal CO2, 50 ± 6 mm Hg; and arousal/awakening index, 16.8 ± 3.6. Thus, these data suggest mild–moderate OSAS in this group.
TABLE 2.
Polysomnography
| OSAS (n = 10) | |
|---|---|
| TST, h | 8.1 ± 0.7 |
| Apnea index | 1.5 ± 1.9 |
| Apnea–hypopnea index | 5.7 ± 4.7 |
| Arousal/awakening index | 16.8 ± 3.6 |
| SpO2 nadir, % | 85 ± 5 |
| End-tidal CO2, mm Hg | 50 ± 6 |
Definition of abbreviations: OSAS = obstructive sleep apnea syndrome; TST = total sleep time.
Values represent means ± SD.
Sleep Questionnaire
All control subjects had an apnea score of less than –1, indicating the unlikelihood of OSA (10), and as a group, had a mean apnea score of –3.83 ± 0.0. This score was significantly lower than the apnea score noted in the OSAS group of 2.06 ± 1.33 (p < 0.0001).
MRI
Mean changes in cross-sectional areas at four ascending oropharyngeal levels during 10 phases of tidal breathing (five inspiratory phases and five expiratory phases) of subjects with OSAS and control subjects are presented in Figure 2. Areas at 0 and 100% of Vt are estimated as the midpoint between measured values (dashed lines). A representative comparison of changes in cross-sectional area at midtonsillar level (level 2) during tidal breathing of a subject with OSAS and a control subject is presented in Figure 3. Movies showing gated dynamic images during tidal breathing in a subject with OSAS and control subject are available in the online supplement (Figure E1).
Figure 2.

Mean upper airway cross-sectional area at 5-vol increments of inspiration and 5-vol increments of expiration as percentage of VT. Subjects with obstructive sleep apnea syndrome (OSAS) are shown in red, control subjects in blue. Inspiration: open triangles/squares; expiration: closed triangles/squares. Dashed segments represent estimated changes. *p < 0.05; **p < 0.001; ***p < 0.0001.
Figure 3.
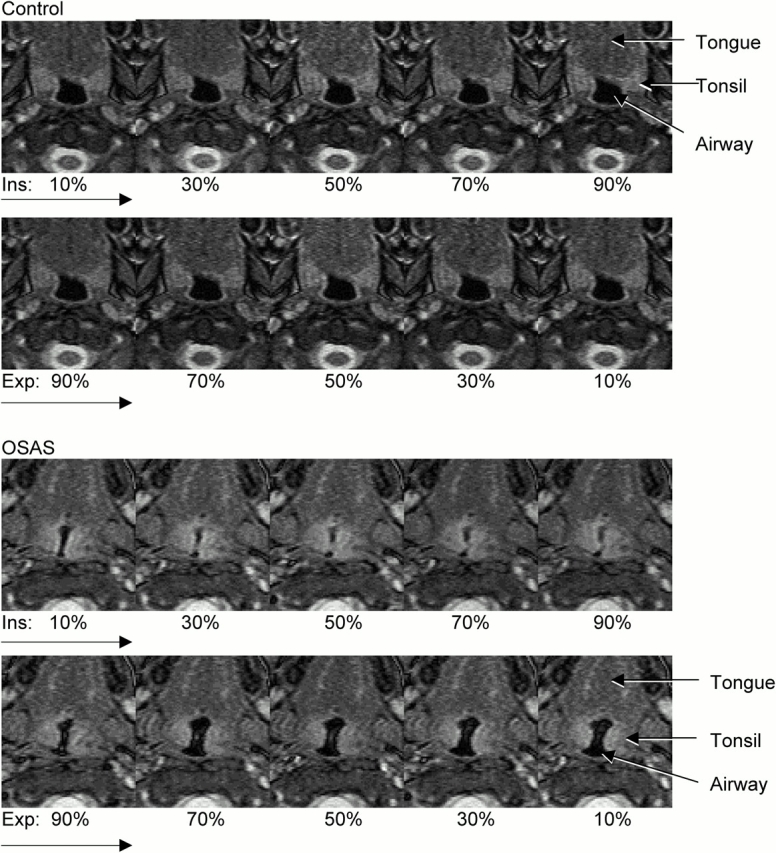
Dynamic changes in cross-sectional area at midtonsillar level (level 2) during tidal breathing (5-vol increments of inspiration [Ins], 5-vol increments of expiration [Exp]) of control subjects (top panels) and subjects with OSAS (bottom panels). Note differences in anteroposterior (A-P) and lateral airway dimension.
Changes in cross-sectional area during inspiration/expiration.
There is a significantly smaller upper airway cross-sectional area during tidal breathing at most volume increments in subjects with OSAS compared with control subjects, particularly during inspiration (Figure 2). There is also a much larger dynamic change in cross-sectional area in subjects with OSAS throughout the respiratory cycle, compared with the relatively constant cross-sectional area throughout tidal breathing in the control subjects. We now provide quantitative data on these dynamic changes.
Minimal cross-sectional area measurements during inspiration.
Children with OSAS exhibited significantly smaller cross-sectional area at oropharyngeal levels 1, 2, 3, and 4 compared with control subjects (p < 0.0001, for all). A trend for a narrower airway at the higher oropharyngeal levels was noted (Figure 4).
Figure 4.

Mean and SD of minimal upper airway cross-sectional area at four oropharyngeal levels (detailed in Figure 1) during inspiration. There are highly significant differences between subjects with OSAS and control subjects at all levels (p < 0.0001).
Maximal cross-sectional area measurements during expiration.
Maximal cross-sectional area measurements at each oropharyngeal level were similar in subjects with OSAS and control subjects during expiration (p = not significant; Figure 5).
Figure 5.

Mean and SD of maximal upper airway cross-sectional area at four oropharyngeal levels (detailed in Figure 1) during expiration. There is no significant difference between subjects with OSAS and control subjects.
Percentage of change in upper airway cross-sectional area during expiration/inspiration.
Changes in cross-sectional areas from inspiration minimum to expiration maximum with respiration were much larger at all oropharyngeal levels in subjects with OSAS as compared with control subjects (Figure 6). Changes noted in OSAS at levels 1 to 4 were as follows: 317, 422, 785, and 922%, compared with 19, 15, 17, and 24% noted in control subjects (p < 0.001, p < 0.005, p < 0.001, and p < 0.001, respectively).
Figure 6.

Maximal percentage of change in upper airway cross-sectional area at the four oropharyngeal levels (detailed in Figure 1) during tidal breathing. *p < 0.005; **p < 0.001.
Shape analysis.
Airway configuration in OSAS differed significantly from control subjects in both inspiration and expiration. Results for all subjects were averaged for each gated volume phase and oropharyngeal level and are shown in Figure 7. Consecutive volume phases along each inspiration and expiration are connected by lines. It can be seen that control dimensions through the breathing cycle change very little as compared with the OSAS in both A-P and lateral dimensions. The mean percentage of change in control subjects ranged in the A-P dimension between −0.9 and −2.1%, and in the lateral dimension between 2.3 and 2.9%, compared with 49 to 82% in the A-P and 32 to 91% in the lateral dimensions in OSAS, respectively. The elliptically modeled OSAS cross-sections illustrate a narrowing in the lateral dimension as compared with the A-P, which is more pronounced at higher levels above the epiglottis (Figure 7). They also exhibit a large change from inspiration to expiration, primarily occurring on the lateral axis. In contrast, the control airway cross-sections are narrower along the A-P axis as compared with the lateral, are similarly sized at all levels, and exhibit only slight narrowing during inspiration. (19).
Figure 7.
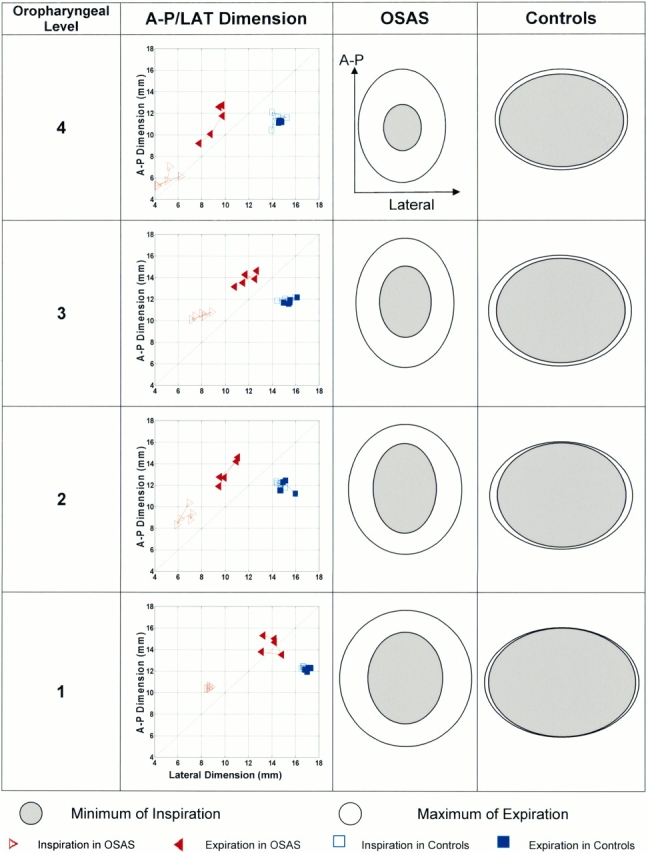
Shape analysis: average A-P and lateral (LAT) dimension for all percentages of VT levels for both groups. Lines link segmental volume levels. Subjects with OSAS are shown in red; control subjects in blue. Open triangles: inspiratory A-P and lateral dimension in OSAS; closed triangles: expiratory A-P and lateral dimension in OSAS; open squares: inspiratory A-P and lateral dimension in control subjects; closed squares: expiratory A-P and lateral dimension in control subjects. Ellipses illustrate relative differences in A-P and lateral dimensions in OSAS and control subjects. Ellipses are shown for minimum during inspiration (filled ellipses) and maximum during expiration (open ellipses).
Validation of Gating System
Differences in timing of triggering between the Siemens bellow system and the pneumotach-based system did not exceed 5% for any volume levels.
DISCUSSION
This study describes changes in upper airway area and shape during tidal breathing in mildly sedated children with OSAS. We found that the upper airway in these children is significantly narrower compared with control subjects, particularly during inspiration, whereas dilatation occurs during expiration. In contrast, the upper airway area changed little during tidal respiration in normal children. As compared with control subjects, the magnitude of area change in OSAS was more prominent in the upper oropharyngeal levels, ranging from 317 to 922% in children with OSAS as compared with 15 to 24% in control subjects. Regarding shape, we found, in general, control subjects had airway cross-sections wider along the lateral axis, whereas subjects with OSAS exhibited airway shape wider along the A-P axis.
Several methodologic issues deserve an initial comment. First, MRI can provide both accurate and reliable measurements of the upper airway (18, 20). However, a disadvantage of MRI is its sensitivity to motion artifact. Although we used a fast image sequence of 300 milliseconds/image, acquisition of data required approximately 15 minutes to collect all breath phases for all slices. To minimize movement, light sedation is given routinely for MRI studies to all children younger than 8 years in our institution. Sedation might have differentially affected upper airway dilator muscle responses in subjects with OSAS compared with control subjects because in children with OSAS there is increased activity of the upper airway dilator muscles during wakefulness (21). Conceivably, this had an impact on the magnitude of differences we found between groups.
Second, respiratory gating for obtaining MRI images of the upper airway has not been used previously. We used the Siemens commercial system, which is based on a single respiratory bellows to follow the changes in volume and trigger the imaging at desired inspiratory or expiratory volumes. An optimal system would be one gated by an integrated flow measurement; however, such a system is not yet available for clinical use. The purpose of our validation study was to assess the accuracy of the commercial bellows' abdominal signal to track lung volume changes as measured by an integrated pneumotach flow signal at the mouth. We demonstrated that, in a normal, awake, adult volunteer, when no obstruction is apparent, the bellows track volume change within ± 5% of the optimal measurement. We are therefore confident that our images were accurately gated in control subjects.
Regarding the subjects with OSAS, these subjects had mild to moderate OSAS during polysomnography. However, during data acquisition, none had evidence of obstruction based on direct inspection and respiratory and pulse oximetry monitoring, although snoring in some subjects was noted. Our MRI data obtained from these patients do not demonstrate complete airway occlusion at any point during data acquisition.
Bellows placement was made on the abdomen or abdominal–chest border where tidal excursion was visibly greatest. The Siemens gating algorithm is designed to avoid triggering an image if the abdominal waveform does not conform to a standard template created by averaging previous regular breaths. In this way, transient and malformed abdominal waveform shapes were definitely excluded.
It is possible, however, that partial obstructive events inducing some degree of paradoxic motion in the chest during inspiration did occur and could have shifted the inspiratory data points of our curves shown in Figure 2, by delaying thoracic filling with respect to abdominal expansion. In addition, an opposite displacement of the curve points could occur during expiration, when emptying would be delayed with respect to abdominal relaxation. However, for each subject, at each phase of respiration, each image slice was collected by gating a single and different breath, and the calculated airway area values represent averages from all subjects. Therefore, errors caused by sporadic asynchrony would tend to be reduced. In more severe cases of OSAS where obstructions occur, chest and abdominal asynchrony could be expected and a gating system based on measurements of chest wall or abdominal motion alone would be inappropriate.
Changes in the upper airway size during tidal breathing using gated cine computed tomography have been described by Schwab and colleagues (10) in normal, awake adults. They noted mean tidal change in upper airway cross-sectional area to be 17% and that during expiration the upper airway expanded to maximal cross-sectional area. In another study, the same authors compared dynamic changes in airway size during wakefulness in adults with OSAS and control subjects. They noted a smaller airway in subjects with OSAS, particularly in the low retropalatal and retroglossal levels, and that airway narrowing occurred mostly during inspiration, whereas dilatation of the airway occurred in expiration, leading to significant change in cross-sectional area in all oropharyngeal regions in subjects with OSAS. Furthermore, upper airway shape analysis in the regions of maximal dynamic changes showed a lengthened A-P configuration in subjects with OSAS, unlike the normal airway, which had a lengthened lateral configuration (9). The previously described findings in adults with OSAS are very similar to the present study in children. Our findings suggest that, despite a different pathophysiology for OSAS in adults and children, namely adenotonsillar hypertrophy (3), similar mechanical forces influence upper airway dynamics and shape in both age groups. It should also be emphasized that, by using MRI, our subjects were not exposed to ionizing radiation and therefore our methodology may be considered as an advantage over computed tomography when studying airway dynamics.
Children presenting with adenotonsillar hypertrophy and OSAS do not usually undergo dynamic imaging of the upper airway. However, when OSAS is associated with more complex medical conditions, such as craniofacial anomalies or after upper airway surgery, fluoroscopy is commonly used to detect the level of airway obstruction (22, 23). The limitations of fluoroscopy are both radiation exposure and that one obtains only a plane lateral image. More recently, Donnelly and coworkers (24, 25) applied ungated cine MRI to children with OSAS with complex medical conditions. They demonstrated significant fluctuations in airway size during respiration in subjects with OSAS along the entire upper airway compared with control subjects, a finding that is compatible with our results.
In the present study, we performed respiratory-gated MRI of the upper airway during tidal breathing using respiratory gating to quantify the temporal changes during respiration in children with adenotonsillar hypertrophy who otherwise had no additional risk factors, such as craniofacial anomalies or neurologic disorders. Several observations can be made from our data. The first is further confirmation of previous studies demonstrating a smaller airway size in children with OSAS (18, 26, 27). A second finding is the significant fluctuation in airway area in subjects with OSAS during inspiration and expiration. Because of their increased upper airway resistance caused by adenotonsillar hypertrophy, inspiratory pressure load on the airway was probably more negative than in control subjects on inspiration, thus reducing area, and more positive than control subjects on expiration, thus increasing area. It is possible that a more compliant airway is involved in this effect, but this is impossible to determine without having measured airway pressures. A third finding is the absence of progressive narrowing of the upper airway during inspiration in both control and OSAS subjects. It was expected that at peak inspiratory flow rate (midinspiration), the airway would progressively narrow with the increasing negative intraluminal pressure. The latter finding indirectly supports evidence for inspiratory activation of upper dilator muscles described in normal adults (28–31), and also noted in children with OSAS (32, 33). This mechanism is assumed to protect the airway from collapse during the negative pressures generated in the upper airway during inspiration (34). Previous studies in adults have demonstrated marked attenuation of this reflex, even in the lighter stages of sleep (35). Our conjecture is that this mechanism still seems to be operative in children, even during light sedation given that our subjects with OSAS did not fully obstruct, even under increased negative loads.
Shape analysis demonstrated different configuration of the airway of children with OSAS in both inspiration and expiration as compared with control subjects. Subjects with OSAS exhibited airway shape narrowed across the A-P axis. This could be caused by anatomic features influencing the width of the lateral pharyngeal wall and/or by neuromotor factors affecting upper airway dilator muscle activity along this axis (i.e., genioglossus activation). These differences together with the magnitude of area changes during tidal breathing may contribute to a more collapsible airway in children with OSAS during sleep as suggested by functional studies (4–6).
In summary, we describe changes in upper airway area and shape during tidal breathing in children with OSAS and contrast these to changes in control subjects. We noted significantly more fluctuation in airway size, with narrowing during inspiration that was more prominent in higher oropharyngeal levels.
Supplementary Material
Supported by grants HL-62408 and MO1-RR00240 from the National Institutes of Health.
This article has an online supplement, which is accessible from this issue's table of contents at www.atsjournals.org
Conflict of Interest Statement: R.A. does not have a financial relationship with a commercial entity that has an interest in the subject of this manuscript; S.S. does not have a financial relationship with a commercial entity that has an interest in the subject of this manuscript; J.M.M. does not have a financial relationship with a commercial entity that has an interest in the subject of this manuscript; J.M.P. does not have a financial relationship with a commercial entity that has an interest in the subject of this manuscript; T.D. does not have a financial relationship with a commercial entity that has an interest in the subject of this manuscript; H.M. does not have a financial relationship with a commercial entity that has an interest in the subject of this manuscript; D.M.W. does not have a financial relationship with a commercial entity that has an interest in the subject of this manuscript; A.I.P. has a grant from ResMed, Inc., to study the relative role of ambulatory recording of sleep-disordered breathing as it compares to full-sleep study. He also receives royalties from Marcel Dekker Publishers for a book he edited entitled, “Sleep Apnea: Pathogenesis, Diagnosis, and Treatment.” He has a patent pending related to the use of serotonin agonists to treat sleep apnea in mammals.
References
- 1.Ali NJ, Pitson DJ, Stradling JR. Snoring, sleep disturbance, and behaviour in 4–5 year olds. Arch Dis Child 1993;68:360–366. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Redline S, Tishler PV, Schluchter M, Aylor J, Clark K, Graham G. Risk factors for sleep-disordered breathing in children: associations with obesity, race, and respiratory problems. Am J Respir Crit Care Med 1999;159:1527–1532. [DOI] [PubMed] [Google Scholar]
- 3.Arens R, Marcus CL. Pathophysiology of upper airway obstruction: a developmental perspective. Sleep 2004;27:997–1019. [DOI] [PubMed] [Google Scholar]
- 4.Marcus CL, McColley SA, Carroll JL, Loughlin GM, Smith PL, Schwartz AR. Upper airway collapsibility in children with obstructive sleep apnea syndrome. J Appl Physiol 1994;77:918–924. [DOI] [PubMed] [Google Scholar]
- 5.Gozal D, Burnside MM. Increased upper airway collapsibility in children with obstructive sleep apnea during wakefulness. Am J Respir Crit Care Med 2004;169:163–167. [DOI] [PubMed] [Google Scholar]
- 6.Isono S, Shimada A, Utsugi M, Konno A, Nishino T. Comparison of static mechanical properties of the passive pharynx between normal children and children with sleep-disordered breathing. Am J Respir Crit Care Med 1998;157:1204–1212. [DOI] [PubMed] [Google Scholar]
- 7.Suratt PM, Dee P, Atkinson RL, Armstrong P, Wilhoit SC. Fluoroscopic and computed tomographic features of the pharyngeal airway in obstructive sleep apnea. Am Rev Respir Dis 1983;127:487–492. [DOI] [PubMed] [Google Scholar]
- 8.Shellock FG, Schatz CJ, Julien P, Steinberg F, Foo TK, Hopp M, Westbrook PR. Occlusion and narrowing of the pharyngeal airway in obstructive sleep apnea: evaluation by ultrafast spoiled GRASS MR imaging. AJR Am J Roentgenol 1992;158:1019–1024. [DOI] [PubMed] [Google Scholar]
- 9.Schwab RJ, Gefter WB, Hoffman EA, Gupta KB, Pack AI. Dynamic upper airway imaging during awake respiration in normal subjects and patients with sleep disordered breathing. Am Rev Respir Dis 1993;148:1385–1400. [DOI] [PubMed] [Google Scholar]
- 10.Schwab RJ, Gefter WB, Pack AI, Hoffman EA. Dynamic imaging of the upper airway during respiration in normal subjects. J Appl Physiol 1993;74:1504–1514. [DOI] [PubMed] [Google Scholar]
- 11.Ciscar MA, Juan G, Martinez V, Ramon M, Lloret T, Minguez J, Armengot M, Marin J, Basterra J. Magnetic resonance imaging of the pharynx in OSA patients and healthy subjects. Eur Respir J 2001;17:79–86. [DOI] [PubMed] [Google Scholar]
- 12.Ikeda K, Ogura M, Oshima T, et al. Quantitative assessment of the pharyngeal airway by dynamic magnetic resonance imaging in obstructive sleep apnea syndrome. Ann Otol Rhinol Laryngol 2001;110:183–189. [DOI] [PubMed] [Google Scholar]
- 13.Brouilette R, Hanson D, David R, Klemka L, Szatkowski A, Fernbach S, Hunt C. A diagnostic approach to suspected obstructive sleep apnea in children. J Pediatr 1984;105:10–14. [DOI] [PubMed] [Google Scholar]
- 14.American Thoracic Society. Standards and indications for cardiopulmonary sleep studies in children. Am J Respir Crit Care Med 1996;153:866–878. [DOI] [PubMed] [Google Scholar]
- 15.Marcus CL, Omlin KJ, Basinki DJ, Bailey SL, Rachal AB, Von Pechmann WS, Keens TG, Ward SL. Normal polysomnographic values for children and adolescents. Am Rev Respir Dis 1992;146:1235–1239. [DOI] [PubMed] [Google Scholar]
- 16.Rechtschaffen A, Kales A. A manual of standardized terminology, techniques and scoring systems for sleep stages on human subjects. Washington DC: National Institutes of Health; 1968. Publication No. 204.
- 17.Schwab RJ, Gupta KB, Gefter WB, Metzger LJ, Hoffman EA, Pack AI. Upper airway and soft tissue anatomy in normal subjects and patients with sleep-disordered breathing: significance of the lateral pharyngeal walls. Am J Respir Crit Care Med 1995;152:1673–1689. [DOI] [PubMed] [Google Scholar]
- 18.Arens R, McDonough JM, Costarino AT, Mahboubi S, Tayag-Kier CE, Maislin G, Schwab RJ, Pack AI. Magnetic resonance imaging of the upper airway structure of children with obstructive sleep apnea syndrome. Am J Respir Crit Care Med 2001;164:698–703. [DOI] [PubMed] [Google Scholar]
- 19.Leiter JC. Upper airway shape: is it important in the pathogenesis of obstructive sleep apnea? Am J Respir Crit Care Med 1996;153:894–898. [DOI] [PubMed] [Google Scholar]
- 20.Welch KC, Foster GD, Ritter CT, Wadden TA, Arens R, Maislin G, Schwab RJ. A novel volumetric magnetic resonance imaging paradigm to study upper airway anatomy. Sleep 2002;25:532–542. [PubMed] [Google Scholar]
- 21.Katz ES, White DP. Genioglossus activity in children with obstructive sleep apnea during wakefulness and sleep onset. Am J Respir Crit Care Med 2003;168:664–670. [DOI] [PubMed] [Google Scholar]
- 22.Felman AH, Loughlin GM, Leftridge CA Jr, Cassisi NJ. Upper airway obstruction during sleep in children. AJR Am J Roentgenol 1979;133:213–216. [DOI] [PubMed] [Google Scholar]
- 23.Gibson SE, Myer CM III, Strife JL, O'Connor DM. Sleep fluoroscopy for localization of upper airway obstruction in children. Ann Otol Rhinol Laryngol 1996;105:678–683. [DOI] [PubMed] [Google Scholar]
- 24.Donnelly LF, Casper KA, Chen B. Correlation on cine MR imaging of size of adenoid and palatine tonsils with degree of upper airway motion in asymptomatic sedated children. AJR Am J Roentgenol 2002;179:503–508. [DOI] [PubMed] [Google Scholar]
- 25.Donnelly LF, Surdulescu V, Chini BA, Casper KA, Poe SA, Amin RS. Upper airway motion depicted at cine MR imaging performed during sleep: comparison between young patients with and those without obstructive sleep apnea. Radiology 2003;227:239–245. [DOI] [PubMed] [Google Scholar]
- 26.Fregosi RF, Quan SF, Kaemingk KL, Morgan WJ, Goodwin JL, Cabrera R, Gmitro A. Sleep-disordered breathing, pharyngeal size and soft tissue anatomy in children. J Appl Physiol 2003;95:2030–2038. [DOI] [PubMed] [Google Scholar]
- 27.Arens R, McDonough JM, Corbin AM, et al. Upper airway size analysis by magnetic resonance imaging of children with obstructive sleep apnea syndrome. Am J Respir Crit Care Med 2003;167:65–70. [DOI] [PubMed] [Google Scholar]
- 28.Tangel DJ, Mezzanotte WS, White DP. Respiratory-related control of palatoglossus and levator palatini muscle activity. J Appl Physiol 1995;78:680–688. [DOI] [PubMed] [Google Scholar]
- 29.Wiegand L, Zwillich CW, White DP. Collapsibility of the human upper airway during normal sleep. J Appl Physiol 1989;66:1800–1808. [DOI] [PubMed] [Google Scholar]
- 30.Leiter JC, Knuth SL, Bartlett D Jr. Dependence of pharyngeal resistance on genioglossal EMG activity, nasal resistance, and airflow. J Appl Physiol 1992;73:584–590. [DOI] [PubMed] [Google Scholar]
- 31.Horner RL, Innes JA, Murphy K, Guz A. Evidence for reflex upper airway dilator muscle activation by sudden negative airway pressure in man. J Physiol 1991;436:15–29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Thach BT, Menon AP, Schefft GL. Effects of negative upper airway pressure on pattern of breathing in sleeping infants. J Appl Physiol 1989;66:1599–1605. [DOI] [PubMed] [Google Scholar]
- 33.Katz ES, White DP. Genioglossus activity during sleep in normal control subjects and children with obstructive sleep apnea. Am J Respir Crit Care Med 2004;170:553–560. [DOI] [PubMed] [Google Scholar]
- 34.Horner RL. Motor control of the pharyngeal musculature and implications for the pathogenesis of obstructive sleep apnea. Sleep 1996;19:827–853. [DOI] [PubMed] [Google Scholar]
- 35.Horner RL, Innes JA, Morrell MJ, Shea SA, Guz A. The effect of sleep on reflex genioglossus muscle activation by stimuli of negative airway pressure in humans. J Physiol 1994;476:141–151. [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.