

Abstract
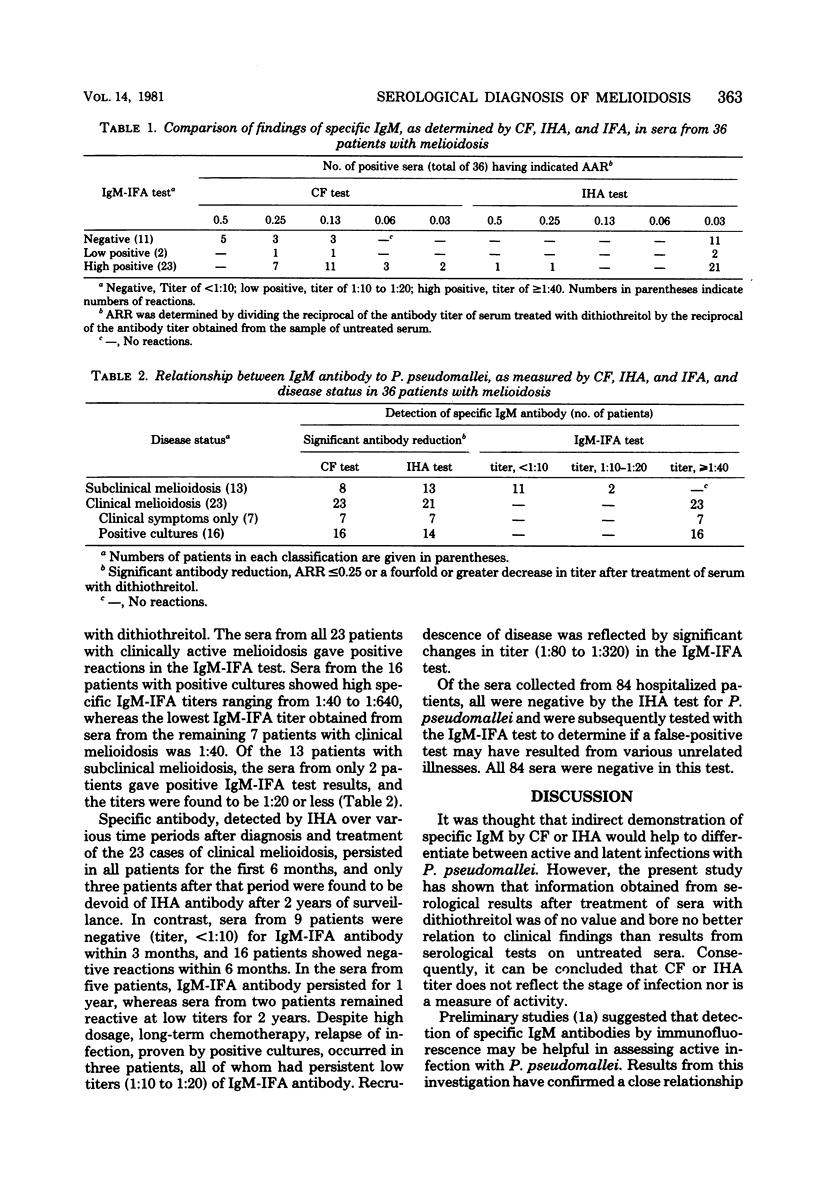
Thirty-six hospitalized patients with circulating antibody to pseudomonas pseudomallei were classified as having either clinical or subclinical melioidosis after full clinical examinations and supplementary radiological and culture investigations. Qualitative estimations of immunoglobulin M (IgM) antibody response were determined by complement fixation, indirect hemagglutination, and immunofluorescence, and the estimations were correlated with the clinical findings in each patient. An attempt was made to appraise the importance of IgM antibody, as determined by each test, in establishing the diagnosis of clinical melioidosis. Results obtained from serological tests were of no value in differentiating between active and latent infections. However, the IgM-immunofluorescent test appeared to be relevant to the diagnosis of clinical melioidosis, since the presence and absence of IgM-immunofluorescent antibody bore a close relation to clinical and subclinical disease, respectively. Surveillance studies indicated that the IgM-immunofluorescent test may be of value in monitoring the activity and treatment of the infection, since the results of the test were generally negative 3 to 6 months after administration of chemotherapy appropriate for melioidosis.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Alexander A. D., Huxsoll D. L., Warner A. R., Jr, Shepler V., Dorsey A. Serological diagnosis of human melioidosis with indirect hemagglutination and complement fixation tests. Appl Microbiol. 1970 Nov;20(5):825–833. doi: 10.1128/am.20.5.825-833.1970. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ashdown L. R. Demonstration of human antibodies to Pseudomonas pseudomallei by indirect fluorescent antibody staining. Pathology. 1981 Jul;13(3):597–601. doi: 10.3109/00313028109059078. [DOI] [PubMed] [Google Scholar]
- Ashdown L. R., Duffy V. A., Douglas R. A. Meliodosis. Med J Aust. 1980 Apr 5;1(7):314–316. [PubMed] [Google Scholar]
- Everett E. D., Nelson R. A. Pulmonary melioidosis. Observations in thirty-nine cases. Am Rev Respir Dis. 1975 Sep;112(3):331–340. doi: 10.1164/arrd.1975.112.3.331. [DOI] [PubMed] [Google Scholar]
- ILERI S. Z. THE INDIRECT HAEMAGGLUTINATION TEST IN THE DIAGNOSIS OF MELIOIDOSIS IN GOATS. Br Vet J. 1965 Apr;121:164–170. doi: 10.1016/s0007-1935(17)41254-1. [DOI] [PubMed] [Google Scholar]
- KHAIRA B. S., YOUNG W. B., DE HART P V. Melioidosis. Br Med J. 1959 Apr 11;1(5127):949–952. doi: 10.1136/bmj.1.5127.949. [DOI] [PMC free article] [PubMed] [Google Scholar]
- NIGG C., JOHNSTON M. M. Complement fixation test in experimental clinical and subclinical melioidosis. J Bacteriol. 1961 Aug;82:159–168. doi: 10.1128/jb.82.2.159-168.1961. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pirofsky B., Rosner E. R. DTT test: a new method to differentiate IgM and IgG erythrocyte antibodies. Vox Sang. 1974;27(5):480–488. doi: 10.1111/j.1423-0410.1974.tb02446.x. [DOI] [PubMed] [Google Scholar]
- Spotnitz M., Rudnitzky J., Rambaud J. J. Melioidosis pneumonitis. Analysis of nine cases of a benign form of melioidosis. JAMA. 1967 Dec 4;202(10):950–954. doi: 10.1001/jama.202.10.950. [DOI] [PubMed] [Google Scholar]