

Abstract
In order to overcome the significant mortality associated with ovarian cancer, a highly sensitive and specific screening test is urgently needed. CA125 is used to monitor response to chemotherapy, detect recurrence and detect late stage ovarian cancer. However, CA-125 alone or in combination with ultrasonography has not been adequate for early detection of ovarian cancer. Here we discuss our recent report of a novel multiplex assay that uses a panel of six serum biomarkers:Leptin, Prolactin, Osteopontin, Insulin-Like Growth Factor II, Macrophage Inhibitory Factor and CA-125. The combination of these six proteins yielded 95.3 % sensitivity and 99.4% specificity. The application of this test in the clinical context and the most appropriate population which could benefit of the test is discussed.
Keywords: ovarian cancer, early detection, leptin, prolactin, osteopontin, MIF, IGF-II multiplex
Introduction
Epithelial ovarian cancer (EOC) is a complex disease that arises due to genetic alterations related to proliferation, apoptosis, and senescence. Majority of EOC arise because of sporadic accumulation of genetic damage 1 but 10% arise in women with a known germ line mutation in BRCA1 or BRCA22.
The high mortality rate of EOC is due to the lack of a screening strategy for early detection. Such test would aid in the identification of patients with early stage disease, which usually presents with vague and nonspecific symptoms. Indeed, 80% of patients are diagnosed with advanced stagedisease, and usually when acute symptoms related to metastasis and bowel obstruction are present 3, 4. A large study in the year 2000 showed that in 1,725 women evaluated for EOC, 95% exhibited symptoms only 3 months prior to seeing their physician. The women presented with: abdominal (77%) and gastrointestinal (70%) symptoms, pain (58%), urinary (34%), and pelvic symptoms (26%). Gynecologic symptoms were the least common 5.
Early detection can significantly improve patient survival. In patients who are diagnosed with early disease (stage I or II), the five-year survival ranges from 60 to 90%, depending on the degree of tumor differentiation6 7. However, in patients with advanced disease, although 80%-90% will initially respond to chemotherapy, less than 10 – 15% will remain in permanent remission 8. While advances in treatment have led to an improved five-year survival rate approaching 45%, overall survival has not been enhanced. Therefore the discovery of a method for early detection of EOC cancer is crucial.
Although ovarian cancer has a high mortality rate, it is still a relatively uncommon disease. The incidence is no more than 40 per 100,000 per year even in the postmenopausal population 9. There is therefore a concern that the morbidity (and potentially mortality) associated with complications of surgery for false-positive screening results will outweigh the benefits of early detection in women with true-positive results. To be acceptable for this population, a screening strategy must achieve a minimum positive predictive value (PPV) of 10% (i.e. no more than nine false positives for each true positive). To achieve this 10% PPV target on screening the general population of postmenopausal women with an incidence of 40/100,000/year, a screening test for ovarian cancer will need to achieve a minimum of 99.6% specificity.
The lack of specific markers for ovarian cancer makes it difficult to achieve the clinical objective of early detection using noninvasive screening methods. Until now, screening consisted of physical examination, ultrasound, and/or cancer antigen 125 (CA-125). However, when taken together, these parameters only detect 30-45% of early disease. Thus, the identification of other cancer-specific markers for early detection of EOC is essential to improve our ability to accurately detect premalignant changes or early stage EOC in asymptomatic women 10.
Because currently available strategies for the prevention of ovarian cancer have not proven as effective as interventions targeted against other cancers in women, there has been tremendous interest in using genomics and proteomics to identify potential new markers which can be used in early detection of this disease 11. Technological developments i have led to rapidly expanding knowledge about gene expression and protein patterns in ovarian cancer. ///Genomic tests have been used for the presence or quantity of the product of a single gene, tests for inherited or acquired mutations in genes which convey an increased risk of developing ovarian cancer, or which predict differential responses to therapy (polymorphisms of breast cancer genes 1 and 2 (BRCA1/2), tests for quantitative expression of either single genes or multiple genes (antibody micro-arrays) and tests for protein expression, particularly in serum, which identify differential patterns between normal patients and patients with ovarian cancer. Analysis of the presence/absence/abundance of known proteins/peptides in the serum using, ELISA or cytokine/antibody multiplex has yielded a number of biomarker combinations with increased specificity and sensitivity for ovarian cancer relative to CA-125 alone 12 13. The main objective of these biomarkers is to improve our ability to accurately detect pre-malignant changes or early stage EOC in asymptomatic women. Once the markers are established a major challenge is to define the right population which will benefit from the test and how to apply it in a clinical framework./// Below we will discuss the strategies used for the development of a novel panel for the early detection of ovarian cancer and the pros and cons of its clinical application
Proteomics for the detection of ovarian cancer
Proteomics involve the measurement of serum proteins to identify potential biomarkers 14 15 16 17. Enzyme-Linked ImmunoSorbent Assay (ELISA) and multiplex bead array are two main proteomic assays that have been used for the development of blood tests for early detection of ovarian cancer. These assays have yielded a number of biomarker combinations with increased specificity and sensitivity for ovarian cancer relative to CA-125 alone 18, 19 20. Because of the complexity and heterogeneity of ovarian cancer, no single biomarker will be able to discriminate between healthy women and ovarian cancer patients. Similarly, no single biomarker will be able to detect all subtypes and stages of the disease with a high enough specificity and sensitivity. The use of a combination of biomarker candidates would provide greater potential for early detection of ovarian cancer 19, 20. Moreover, the selection of an appropriate combination of biomarker candidates, which can be multiplexed may provide a great potential for ovarian cancer biomarker discovery and pre-validation.
ELISA
ELISA is a biochemical technique used in immunology to detect specific proteins in a sample. It has been widely used as a diagnostic tool in medicine and involves the capture of an unknown amount of antigen onto a polystyrene microtiter plate. After antigen immobilization, it is detected using a conjugated secondary antibody, which forms a complex (“sandwich”) with the antigen. The enzyme conjugated to the secondary antibody then catalyzes a reaction that yields a detectable signal. Signals are either chromogenic or fluorometric.
Multiplex bead array
Multiplex bead arrays permit the simultaneous quantitation of multiple proteins in solution using spectrally distinct beads coated with different antibodies. This technology allows the analysis of up to 100 different proteins in a single microplate well. Essentially,it is an ELISA on a bead. The constituents of each well are drawn up into the flow-based Luminex array reader, which identifies each specific protein/antigen based on the bead color of its corresponding antibody. This system can simultaneously quantify up to 100 protein targets in culture media, sera, or other matrices and can automatically analyze up to 96 samples in under 35 minutes. The system generates a standard curve and therefore provides specific measurements of protein concentration 21.
Development of biomarker panels: a “roadmap” for success
A great deal of effort has been invested by multiple groups into identifying combinations of markers that could improve the sensitivity and specificity for the diagnosis of early-stage ovarian cancer. At least 30 blood and urine markers have so far been combined with CA125 for this purpose. These studies, however, compared only two or three markers at a time and showed an increased sensitivity but an associated decreased in specificity.
As mentioned above, for the early detection of EOC, It is crucial to develop panels of biomarkers that can increase both the sensitivity and the specificity. An ideal test should be able able to distinguish between a healthy woman and a patient with early stage disease, with a high degree of specificity and sensitivity. It must be reproducible, quantitative, non-invasive, and inexpensive.
Our approach in the development of an early detection test has followed the suggested “roadmap” proposed by Anderson and by Gagnon and Ye 12 22, which is comprised of three phases: discovery, verification/validation, and clinical implementation. The process used in developing the final panel of protein markers involved several different screening steps, used samples obtained from different patient populations, and validated with different techniques.
Discovery Phase
In the first step of the Discovery Phase, novel biomarkers are identified by comparing factors in serum or urine samples collected from healthy controls and ovarian cancer patients. This approach seems to lead to more clinically relevant candidates, as the ultimate goal of a diagnostic test is one that is non-invasive, can be easily performed on serum or urine, and is relatively painless. In this phase, we used the Rolling Circle amplification (RCA) assay, which like Mass spectrometry, is a powerful technology for discovery but not for diagnostics. We first analyzed the expression levels of 169 proteins in serum samples collected from 18 untreated EOC patients and 28 healthy, age-matched controls. We limited the output to proteins associated with the control of cell growth and therefore avoided covering the whole proteome. In this initial screen, 35 proteins were differentially expressed between healthy women and newly diagnosed EOC patients based on ANOVA tests, with P values of 0.05.
In the second step of the Discovery Phase, we evaluated the specificity of the 35 potential markers by changing the patient cohort. Still using the RCA technology, we evaluated a different patient population while maintaining the same clinical characteristics as the previous group. After further validation with an additional 40 patients, the number of potential biomarkers was reduced from 35 to ten, based on analysis of variance tests (ANOVA), with P-values of less than 0.05. This second screening step has the advantage of removing potential “stress proteins” which could lead to non-specific biomarkers. Furthermore, these results emphasize the importance of using multiple patient groups for discovery and as we will discuss below, for validation.
The third step in the Discovery phase involves the evaluation of each individual marker using a different technology and preferentially one that could be used in the clinic. In our case, we proceeded to evaluate the markers obtained from the Discovery phase using commercially available ELISA kits for each of the identified proteins.
Our ELISA results showed that four proteins, out of the 10 could accurately discriminate between healthy individuals and cancer patients. These proteins were Leptin, Prolactin, Osteopontin (OPN) and Insulin Growth Factor II (IGF-II). These four biomarkes showed perfect correlation between the RCA immunoassays and ELISA. In addition, the expression pattern between the control (healthy) and case (ovarian cancer) sets was different for each protein. Both prolactin and OPN were significantly elevated in EOC serum, whereas leptin and IGF-II levels were reduced.
We then evaluated the capacity of each protein to discriminate between the case and the control cohorts. Although each protein had an AUC significantly above 0.5, none of the markers individually had enough sensitivity and specificity. Only when used together were the panel of biomarkers able to discriminate between control and cancer group samples.
To differentiate between healthy subjects and ovarian cancer patients, and healthy subjects after sample decoding, we evaluated several statistical approaches and used statistical cluster analysis for the final model. First we established split points for each biomarker. The split point divides the sample space into two intervals: one for normal and another for cancer. The best split point for each marker was chosen to minimize the number of misclassified individuals. Using split point analysis with four markers, cancer is predicted by having two or more markers in the abnormal range and normal is defined by one or zero markers in the abnormal range.
Validation phase
The first step in the validation process is the evaluation of the model in a blind study. Thus, we used a cohort consisting of 206 serum samples, which included samples from 106 healthy subjects and 100 ovarian cancer patients (24 Stage I/II and 76 Stage III/IV). The model was able to identify 96 out of 100 EOC patients (96%) (including 23 of 24 patients with Stage I/II EOC). In the healthy group, 6 out of 106 individual were incorrectly diagnosed (5.6%).
The final results of the test have shown a sensitivity of 95%, a specificity of 95%, (Figure 1). Therefore, not only did ELISA provide a platform for the quantitative measurement of proteins and assay reproducibility, there was also verification in pattern of response of biomarkers between RCA and ELISA 19, 20.
Figure 1.
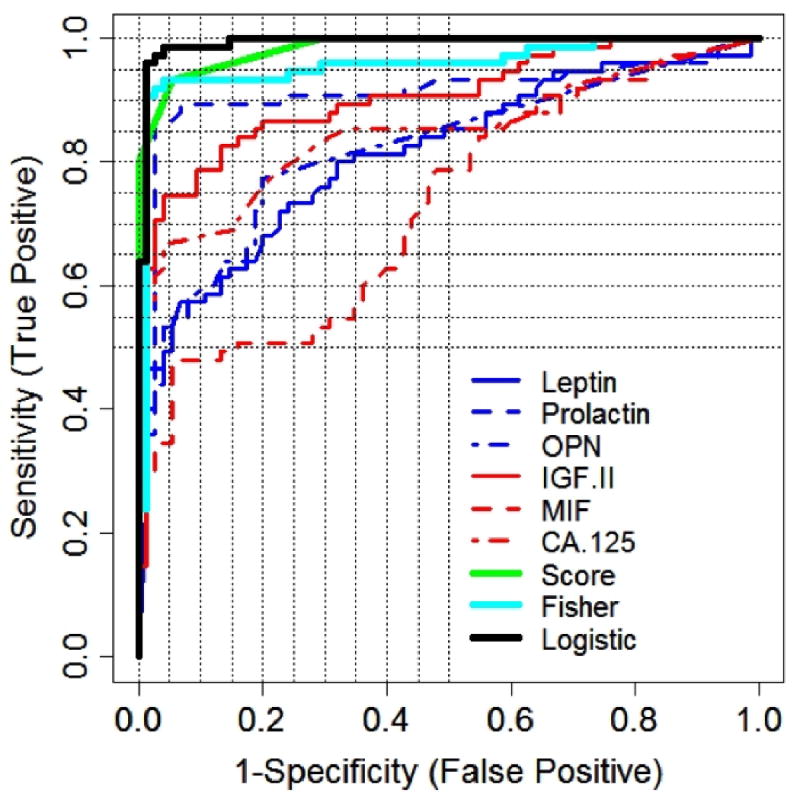
ROC curves for composite predictors corresponding to final model using four markers and the six markers with the different cohorts. Note the improvement with the six markers and the similarity of the results independent on the cohort analyzed.
Clinical Implementation
Although ELISA could discriminate between healthy and early stage disease with a high degree of specificity and sensitivity, there are limitations with the use of this technology for a multiple biomarker test. First is the potential variability in overall results between the different ELISA kits, and second is the high cost of performing multiple ELISAs. Therefore, the use of Multiplex bead array could represent a better approach for this type of tests.
Multiplex bead array provides numerous advantages as a platform for the diagnostic implementation 19. With Multiplex bead array, one has the ability to measure multiple markers in a small sample volume. Thus, this platform could simplify the development of a diagnostic test and could decrease the potential inter-assay variability. This makes the Multiplex bead array suitable for large validation studies.
Our first objective was to determine whether a multiplex bead array could adequately replicate the results previously obtained with ELISA. Therefore, we compared concentrations obtained for Prolactin, Leptin, OPN and IGF-II from by ELISA and a multiplex bead array using 50 serum samples from newly diagnosed ovarian cancer patients and 50 serum samples from age-matched healthy individuals. Results showed that both ELISA and multiplex assay exhibited the same pattern for the four markers. Statistical analysis of the values obtained from the Multiplex assay showed similar results to that previously reported using ELISA (95% sensitivity and 94% specificity).
Thus, we selected this platform as a potential replacement for the combination ELISA; in addition, we added two markers to the panel: Macrophage Inhibitory Factor (MIF), which we found to be highly expressed in the serum of ovarian cancer patients 23, and CA-125. The combination of these six biomarkers is more than adequate to provide the sensitivity and specificity required but not sizable enough to impede and complicate evaluation. The characterization of this new panel was done following the same guidelines as described for the biomarkers using ELISA. That is, a test group was used for creating the model and a different test group was used to create the model. In both steps, evaluation was done in a blind manner. The statistical results for the final model indicates a sensitivity of 95.3% and specificity of 99.4% 24.
The multiplex bead array for the detection of ovarian cancer was developed in collaboration with Millipore. The kit, known as the Beadlyte® Cancer Biomarker Panel Kit, includes two panels: one for Leptin, Prolactin, Macrophage Inhibitory Factor (MIF), Osteopontin, and CA-125 (Beadlyte 5-plex Cancer Panel); and a separate panel for Insulin Growth Factor-II (IGF-II) (Beadlyte Anti-Human IGF-II Bead Set).
The panel is manufactured under strict regulatory conditions ensuring the reproducibility of each batch and a low coefficient of variation (Intra and Inter CV%) - two important requirements for its application in clinical trials and potential clinical use.
Biological Relevance of the markers
The biological significance of the described biomarkers provides for a better understanding of the test. The proteins identified in this study, with the exception of CA-125 and MIF, are all related to the normal physiology of the ovaries. These proteins are produced either by the surrounding supportive cells or as a response to signals originating from the ovary. IGF-II is the primary IGF in the human ovary, acting as mediator of gonadotropin action 25, 26. Prolactin on the other hand, has been shown to participate in the regulation of steroidogenesis in ovarian follicles, particularly the inhibition of progesterone secretion in the early stages of the follicular growth and its enhancement in the luteal phase 27, 28. There is strong evidence that links leptin and the hypothalamic gonadotropin releasing hormone secretion, which affects the hypothalamic pituitary-ovarian axis 29. Osteopontin is overexpressed in a cancers including lung cancer, breast cancer, colorectal cancer, stomach cancer, ovarian cancer, melanoma and mesothelioma 30 31. Cancer antigen (CA-125) is a mucinous glycoprotein and product of the MUC16 gene, and a protein antigen found in abnormally high levels in the serum of women with ovarian cancer. However, as already stated, CA-125 is not specific enough to be used for population-based screening due to its poor specificity 13. Macrophage migration inhibiting factor (MIF) is an inflammatory mediator involved in cell-mediated immunity, immunoregulation and inflammation 32, 33.
The level of expression of these proteins are maintained by a delicate balance between each of the cellular components of the ovary. We hypothesize that the presence of abnormal cells may alter this intercellular communication and disrupt the axis, resulting in the abnormal expression levels observed in cancer samples. The proteins identified in this study may not represent factors produced by the tumor but instead represent the organ/body's response to the presence of neoplastic cells. We propose that significant levels of products secreted by the tumor could only be detected in peripheral blood at later stages of tumor development; however, the body is able to recognize and respond to early stages of the tumorigenicity, and this is reflected in peripheral blood proteins. Based on this premise, the protein panel identified in this study is able to detect early stages of the disease.
Clinical Application: Who and When
A major concern associated with the clinical use of biomarkers is the potential “false positives”. The positive predictive value (PPV) is used as the standard for the determination of potential benefit/risk of the test. As indicated above, ovarian cancer is a “rare” but lethal disease. Any test, even with a specificity of 99.9%, will have a PPV not larger than 10% if it is calculated based on the general population. It means that only 1 out of 10 women who were positive for the test would in fact have ovarian cancer. If that approach is adopted, there is no value in developing a test. This is true for all forms of cancers which have a low incidence such as ovarian and pancreatic cancer.
Based on this knowledge, there is a general consensus in the biomarkers community that screening the general population has no value. It is therefore, necessary to focus on specific groups where the risk of developing the cancer is higher. This population might be the group that can benefit from the test 10.
The value of a test exists when it is applied to what is considered a high-risk population, which may further differ in incidences due to different genetic background and family history. For these cases, we need to calculate PPV for each subgroup. Research on previous screening technologies suggests that cancers detected by screening may be more likely to have clinicopathologic features and better prognosis than cancers diagnosed clinically. Therefore, to obtain valid estimates of sensitivity, specificity, and predictive values for screening women at high-risk, research may need to be conducted within the specified high risk populations, not among women in the general population.
Furthermore, no blood test, in any clinical context, even with a high PPV, is meant to be used as a final diagnosis. A blood test is usually inexpensive, and it can be performed repeatedly. In the context of ovarian cancer, a blood test would provide an excellent alternative to less sensitive, more invasive, and more expensive tests such as imaging. A blood test will limit the use of CT scan or MRI unless clearly indicated.
Another major concern is that the use of these types of test will lead to unnecessary surgeries. Interestingly, the recommended approach for the prevention of ovarian cancer for patients in the high-risk group is preventive surgery (salpingo-oophorectomy)34. However, from 100 preventive oophorectomies, only 1 or 2 cancers are identified 35. Therefore, 98 women undergo unnecessary surgeries. The use of this test may help to postpone or completely avoid the surgical procedure if the results of the test are negative.
Conclusion
In summary, we have discussed the steps in the development and characterization of a test for detection of ovarian cancer using three different platforms, four types of statistical analysis, and two different sample cohorts. The use of this or other panels with similar sensitivity and specificity provides a potential viable alternative to screening for CA125 alone for the diagnosis of ovarian cancer. The implementation of this test for a high-risk population may postpone or completely avoid unnecessary surgical procedures and may providean additional tool for the management of this deadly disease.
Acknowledgments
These studies were supported in part by Nicolas Brady, the Adler Foundation and the Discovery to Cure Translational Research Program
Footnotes
Financial Disclosure : LabCorp has a license agreement with Yale University for the Multiplex biomarker test. GM is a consultant for Teva pharmaceutical.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Bibliography
- 1.Permuth-Wey J, Sellers TA. Epidemiology of ovarian cancer. Methods Mol Biol. 2009;472:413–437. doi: 10.1007/978-1-60327-492-0_20. [DOI] [PubMed] [Google Scholar]
- 2.Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2006. CA Cancer J Clin. 2006 Mar-Apr;56(2):106–130. doi: 10.3322/canjclin.56.2.106. [DOI] [PubMed] [Google Scholar]
- 3.Schwartz PE. Current diagnosis and treatment modalities for ovarian cancer. Cancer Treat Res. 2002;107:99–118. doi: 10.1007/978-1-4757-3587-1_4. [DOI] [PubMed] [Google Scholar]
- 4.Berchuck A, Elbendary A, Havrilesky L, Rodriguez GC, Bast RC., Jr Pathogenesis of ovarian cancers. J Soc Gynecol Investig. 1994;1(3):181–190. doi: 10.1177/107155769400100302. [DOI] [PubMed] [Google Scholar]
- 5.Goff BA, Muntz HG. Screening and early diagnosis of ovarian cancer. Women's Health in Primary Care. 2005;8(6):262–268. [Google Scholar]
- 6.Miller BA, Chu KC, Hankey BF, Ries LA. Cancer incidence and mortality patterns among specific Asian and Pacific Islander populations in the U.S. Cancer Causes Control. 2008 Apr;19(3):227–256. doi: 10.1007/s10552-007-9088-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Espey DK, Wu XC, Swan J, et al. Annual report to the nation on the status of cancer, 1975-2004, featuring cancer in American Indians and Alaska Natives. Cancer. 2007 Nov 15;110(10):2119–2152. doi: 10.1002/cncr.23044. [DOI] [PubMed] [Google Scholar]
- 8.Mutch D. Surgical manegement of ovarian cancer. Semin Oncol. 2002;29:3–8. doi: 10.1053/sonc.2002.31589. [DOI] [PubMed] [Google Scholar]
- 9.Permuth-Wey J, Boulware D, Valkov N, et al. Sampling strategies for tissue microarrays to evaluate biomarkers in ovarian cancer. Cancer Epidemiol Biomarkers Prev. 2009 Jan;18(1):28–34. doi: 10.1158/1055-9965.EPI-08-0713. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Nick AM, Sood AK. The ROC ‘n’ role of the multiplex assay for early detection of ovarian cancer. Nat Clin Pract Oncol. 2008 Oct;5(10):568–569. doi: 10.1038/ncponc1214. [DOI] [PubMed] [Google Scholar]
- 11.Berger RP, Ta'asan S, Rand A, Lokshin A, Kochanek P. Multiplex assessment of serum biomarker concentrations in well-appearing children with inflicted traumatic brain injury. Pediatr Res. 2008 sep 10; doi: 10.1203/PDR.0b013e31818c7e27. [DOI] [PubMed] [Google Scholar]
- 12.Gagnon A, Ye B. Discovery and application of protein biomarkers for ovarian cancer. Curr Opin Obstet Gynecol. 2008 Feb;20(1):9–13. doi: 10.1097/GCO.0b013e3282f226a5. [DOI] [PubMed] [Google Scholar]
- 13.Bast RC, Jr, Badgwell D, Lu Z, et al. New tumor markers: CA125 and beyond. Int J Gynecol Cancer. 2005 Nov-Dec;15 3:274–281. doi: 10.1111/j.1525-1438.2005.00441.x. [DOI] [PubMed] [Google Scholar]
- 14.Wu B, Abbott T, Fishman D, et al. Comparison of statistical methods for classification of ovarian cancer using mass spectrometry data. Bioinformatics. 2003 Sep 1;19(13):1636–1643. doi: 10.1093/bioinformatics/btg210. [DOI] [PubMed] [Google Scholar]
- 15.Bast RC, Jr, Brewer M, Zou C, et al. Prevention and early detection of ovarian cancer: mission impossible? Recent Results Cancer Res. 2007;174:91–100. doi: 10.1007/978-3-540-37696-5_9. [DOI] [PubMed] [Google Scholar]
- 16.Petricoin EF, Ardekani AM, Hitt BA, et al. Use of proteomic patterns in serum to identify ovarian cancer. Lancet. 2002 Feb 16;359(9306):572–577. doi: 10.1016/S0140-6736(02)07746-2. [DOI] [PubMed] [Google Scholar]
- 17.Chang J, Powles TJ, Allred DC, et al. Biologic Markers as Predictors of Clinical Outcome From Systemic Therapy for Primary Operable Breast Cancer. J Clin Oncol. 1999;17(10):3058–3063. doi: 10.1200/JCO.1999.17.10.3058. Record as supplied by publisher. [DOI] [PubMed] [Google Scholar]
- 18.Woolas RP, Xu FJ, Jacobs IJ, et al. Elevation of multiple serum markers in patients with stage I ovarian cancer. J Natl Cancer Inst. 1993 Nov;Mar;85(21):1748–1751. doi: 10.1093/jnci/85.21.1748. [DOI] [PubMed] [Google Scholar]
- 19.Gorelik E, Landsittel DP, Marrangoni AM, et al. Multiplexed immunobead-based cytokine profiling for early detection of ovarian cancer. Cancer Epidemiol Biomarkers Prev. 2005 Apr;14(4):981–987. doi: 10.1158/1055-9965.EPI-04-0404. [DOI] [PubMed] [Google Scholar]
- 20.Mor G, Visintin I, Lai Y, et al. Serum protein markers for early detection of ovarian cancer. Proc Natl Acad Sci U S A. 2005 May 24;102(21):7677–7682. doi: 10.1073/pnas.0502178102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Vignali DA. Multiplexed particle-based flow cytometric assays. J Immunol Methods. 2000 Sep 21;243(12):243–255. doi: 10.1016/s0022-1759(00)00238-6. [DOI] [PubMed] [Google Scholar]
- 22.Anderson NL. The roles of multiple proteomic platforms in a pipeline for new diagnostics. Mol Cell Proteomics. 2005 Oct;4(10):1441–1444. doi: 10.1074/mcp.I500001-MCP200. [DOI] [PubMed] [Google Scholar]
- 23.Agarwal R, Alvero A, Visintin I, et al. Macrophage Migration Inhibitory Factor expression in ovarian cancer. American Journal of Obstetrics and Gynecology. 2007;196(4):348.e341–345. doi: 10.1016/j.ajog.2006.12.030. [DOI] [PubMed] [Google Scholar]
- 24.Visintin I, Feng Z, Longton G, et al. Diagnostic markers for early detection of ovarian cancer. Clin Cancer Res. 2008 Feb 15;14(4):1065–1072. doi: 10.1158/1078-0432.CCR-07-1569. [DOI] [PubMed] [Google Scholar]
- 25.Giudice LC. Insulin-like growth factor family in Graafian follicle development and function. J Soc Gynecol Investig. 2001 Jan-Feb;8(1 Suppl Proceedings):S26–29. doi: 10.1016/s1071-5576(00)00102-7. [DOI] [PubMed] [Google Scholar]
- 26.Kaipia A, Hsueh AJ. Regulation of ovarian follicle atresia. Annu Rev Physiol. 1997;59:349–363. doi: 10.1146/annurev.physiol.59.1.349. [DOI] [PubMed] [Google Scholar]
- 27.Grosdemouge I, Bachelot A, Lucas A, Baran N, Kelly PA, Binart N. Effects of deletion of the prolactin receptor on ovarian gene expression. Reprod Biol Endocrinol. 2003 Feb 6;1:12. doi: 10.1186/1477-7827-1-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Bachelot A, Binart N. Corpus luteum development: lessons from genetic models in mice. Curr Top Dev Biol. 2005;68:49–84. doi: 10.1016/S0070-2153(05)68003-9. [DOI] [PubMed] [Google Scholar]
- 29.Popovic V, Casanueva FF. Leptin, nutrition and reproduction: new insights. Hormones (Athens) 2002 Oct-Dec;1(4):204–217. doi: 10.14310/horm.2002.1169. [DOI] [PubMed] [Google Scholar]
- 30.Brakora KA, Lee H, Yusuf R, et al. Utility of osteopontin as a biomarker in recurrent epithelial ovarian cancer. Gynecol Oncol. 2004 May;93(2):361–365. doi: 10.1016/j.ygyno.2004.01.050. [DOI] [PubMed] [Google Scholar]
- 31.Chambers AF, Vanderhyden BC. Ovarian cancer biomarkers in urine. Clin Cancer Res. 2006 Jan 15;12(2):323–327. doi: 10.1158/1078-0432.CCR-05-2563. [DOI] [PubMed] [Google Scholar]
- 32.Morand EF, Leech M, Weedon H, Metz C, Bucala R, Smith MD. Macrophage migration inhibitory factor in rheumatoid arthritis: clinical correlations. Rheumatology (Oxford) 2002 May;41(5):558–562. doi: 10.1093/rheumatology/41.5.558. [DOI] [PubMed] [Google Scholar]
- 33.Mitchell RA, Liao H, Chesney J, et al. Macrophage migration inhibitory factor (MIF) sustains macrophage proinflammatory function by inhibiting p53: regulatory role in the innate immune response. Proc Natl Acad Sci U S A. 2002 Jan 8;99(1):345–350. doi: 10.1073/pnas.012511599. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Piver MS, Jishi MF, Tsukada Y, Nava G. Primary peritoneal carcinoma after prophylactic oophorectomy in women with a family history of ovarian cancer. A report of the Gilda Radner Familial Ovarian Cancer Registry. Cancer. 1993 May 1;71(9):2751–2755. doi: 10.1002/1097-0142(19930501)71:9<2751::aid-cncr2820710911>3.0.co;2-j. [DOI] [PubMed] [Google Scholar]
- 35.Finch A, Beiner M, Lubinski J, et al. Salpingo-oophorectomy and the risk of ovarian, fallopian tube, and peritoneal cancers in women with a BRCA1 or BRCA2 Mutation. Jama. 2006 Jul 12;296(2):185–192. doi: 10.1001/jama.296.2.185. [DOI] [PubMed] [Google Scholar]