

Abstract
Objective Recent increases in adolescent pregnancies have sparked a renewed impetus to identify risk factors, such as childhood sexual abuse (CSA), associated with adolescent pregnancy. Given mixed evidence regarding the strength of the relationship between CSA and adolescent pregnancy (Blinn-Pike, Berger, Dixon, Kuschel, & Kaplan, 2002), our objective was to provide an estimate of the effect size of this relationship using updated literature and meta-analytic techniques. Methods Meta-analyses of 21 studies were conducted using a random effects model of binary outcomes to determine aggregate effect-size estimates controlling for study heterogeneity. Results CSA significantly increased the odds of experiencing an adolescent pregnancy by 2.21-fold (95% CI: 1.94–2.51). A supplemental analysis suggested that 4.5 out of 10 pregnant adolescents may have a prior history of CSA. Conclusions CSA places females at increased risk for subsequent adolescent pregnancy. Addressing conditions associated with CSA might impact the overall adolescent pregnancy rate.
Keywords: child abuse and neglect, high-risk behaviors, meta-analysis
Introduction
Rates of adolescent pregnancy and motherhood, for all age groups and ethnicities within the United States, are at their lowest levels in recent history. Pregnancy and motherhood rates for adolescents 15–19 years of age have declined 36 and 34%, respectively, since 1991 (Martin et al., 2007; The Alan Guttmacher Institute, 2006). Yet, even with this substantial decline, rates of adolescent pregnancy and motherhood in the United States are still among the highest in industrialized nations, with 7.5% of adolescents becoming pregnant each year and over 4% becoming mothers (Hoffman, 2006; Martin et al., 2007). These numbers are considered in view of recent data showing a 3% overall increase in the number of adolescent births during 2006, the first time an increase has occurred in 15 years (Hamilton, Martin, & Ventura, 2007). Although the reasons for this increase in adolescent births are unknown, this result is especially troublesome because adolescent motherhood is known to be associated with poverty (Furstenberg, Brooks-Gunn, & Morgan, 1987; Moore et al., 1993), fewer years of maternal education (Hofferth, Reid, & Mott, 2001; Nord, Moore, Morrison, Brown, & Myers, 1992), and rapid-repeat pregnancies (Boardman, Allsworth, Phipps, & Lapane, 2006). In addition, children of adolescent mothers are more likely to face cognitive and academic impairment, increased behavior problems, and a greater likelihood of becoming an adolescent parent themselves (Brooks-Gunn & Furstenberg, 1986; Corcoran, 1998; Furstenberg et al., 1987). At its current level, adolescent motherhood is estimated to cost 9.1 billion dollars annually (Hoffman, 2006). Given this inordinate public health impact, there is continued impetus to understand comprehensively the various pathways to adolescent pregnancy and motherhood in order for intervention and prevention programs to be at maximum efficacy.
A comprehensive picture of adolescent pregnancy risk factors includes (a) cognitive or attitudinal vulnerabilities such as positive or ambivalent attitudes toward sex and childbearing, perceived invulnerability to pregnancy, a lack of contraception knowledge, perceived parental approval of birth control use, and low educational and occupational expectations (Anda et al., 2001; Jaccard & Dittus, 2000; Miller, 2002; Polacsek, Celentano, O’Campo, & Santelli, 1999; Quinlivan, Tan, Steele, & Black, 2004; Stevens-Simon, Kelly, Singer, & Cox, 1996); (b) romantic partner characteristics such as being in a relationship with a violent romantic partner, dating older boyfriends, having early and high levels of seriousness with boyfriends, and difficulty negotiating the use of birth control with a partner (Berry, Shillington, Peak, & Hohman, 2000; Brazzell & Acock, 1988; Marin, Coyle, Gomez, Carvajal, & Kirby, 2000; Polacsek et al., 1999; Salazar et al., 2004; Santelli et al., 2004; Silverman, Raj, Mucci, & Hathaway, 2001; Whitbeck, Yoder, Hoyt, & Conger, 1999); and (c) familial and contextual factors such as socioeconomic status, single-parent families, family violence, having an older, sexually active sibling or pregnant/parenting adolescent sister, low maternal education, lack of parental warmth and supervision, parental approval of sex, contraception, early dating, and low perceived support from parents and peers (Berry et al., 2000; Chandy, Blum, & Resnick, 1996; Connolly, Furman, & Konarski, 2000; East & Jacobson, 2001; Jaccard & Dittus, 2000; Meschke, Zweig, Barber, & Eccles, 2000; Mezzich et al., 1999; Miller, Benson, & Galbraith, 2001; Miller, McCoy, & Olson, 1986; Quinlivan et al., 2004; Santelli, Lowry, Brener, & Robin, 2000; Scaramella, Conger, Simons, & Whitbeck, 1998; Sieving et al., 2001). Despite intervention efforts addressing these identified risk factors, adolescent pregnancy continues at a high rate and remains a significant social concern.
There are several plausible explanations for the persisting high rates of adolescent pregnancy and motherhood, such as additional, unidentified risk factors explaining a large proportion of adolescents who become pregnant. One area that has received considerable attention is whether individuals who experienced childhood maltreatment (sexual, physical, and emotional abuse) show higher rates of adolescent pregnancy and motherhood in comparison to their non-maltreated counterparts. Childhood sexual abuse (CSA), in particular, has received much of the focus, perhaps due to the sexual nature of the act and the considerable literature regarding sexual disturbances and distortions, greater pregnancy desire or intent, earlier age of intercourse, multiple sexual partners, and concerns about infertility that have been studied as developmental sequelae of CSA (Boyer & Fine, 1992; Butler & Burton, 1990; Noll, Trickett, & Putnam, 2003; Rainey, Stevens-Simon, & Kaplan, 1995; Raj, Silverman, & Amaro, 2000; Stevens-Simons & Reichert, 1994). While there have been several studies linking child maltreatment and adolescent pregnancy (Fiscella, Kitzman, Cole, Sidora, & Olds, 1998; Kellogg, Hoffman, & Taylor, 1999; Smith, 1996), there remains considerable controversy in this literature because studies report inconsistent findings or a lack of relationship between abuse and adolescent pregnancy or motherhood (Adams & East, 1999; Widom & Kuhns, 1996).
In a comprehensive literature review, Blinn-Pike et al. (2002) examined previous studies to determine the connection between childhood maltreatment and adolescent pregnancy. The authors used explicit inclusion criteria that included a clear definition of maltreatment involving physical, sexual, or emotional abuse, or all, and limited their search criteria to empirical studies published between 1980 and 2000. The search yielded 15 published articles and, based on their review, Blinn-Pike et al. (2002) concluded that a causal link between child maltreatment and adolescent pregnancy could not be determined because of conflicting results in the literature and methodological limitations such as cross-sectional designs and retrospective methods of data collection.
The current article sought to build on issues raised in the review of Blinn-Pike et al.. First, we focused explicitly on CSA in order to provide homogeneity with regard to the group of “maltreated children.” Second, we used meta-analysis to empirically derive estimates about the relationship between CSA and adolescent pregnancy instead of relying solely on an impressionistic review of the literature. Our primary meta-analysis relied on well-designed studies that included adequate comparison groups in order to evaluate stringently the relationship between CSA and rates of adolescent pregnancy in direct comparison to non-abused adolescent peers. We supplemented this primary analysis by executing a secondary analysis that included studies without relevant control conditions in order to provide a comprehensive analysis of the largest number of extant studies examining the topic. Finally, we included studies that have been published subsequent to the original review of Blinn-Pike et al. (2002) to ensure the most up-to-date findings. It should be noted that, by and large, the adolescent pregnancy literature [including the review of Blinn-Pike et al. (2002)] makes little distinction between adolescent pregnancy and adolescent motherhood and the two terms often are used interchangeably. Although these two outcomes are highly distinctive and each is associated with differing long-term sequelae for women, we found it very difficult to focus exclusively on one or the other, given that many of the study designs and operational definitions made it difficult to disaggregate the two outcomes. In order to be consistent with the literature and to avoid arbitrarily excluding relevant studies based solely on the operational definitions (or lack thereof) of outcomes, we combined studies that examined adolescent pregnancy, studies of adolescent motherhood, and studies that did not make a distinction between the two, in the present meta-analyses. Henceforth, the term adolescent pregnancy is used to describe the outcome of interest with full acknowledgement that this term is inclusive of both adolescent pregnancy and adolescent motherhood.
Method
To be included in the analyses, each study was required to meet specific inclusion criteria. Inclusion criteria consisted of: (a) studies focused on female participants, (b) self-reported or documented experiences of some form of CSA, exclusively or in combination with other forms of childhood maltreatment, (c) reported or derived (e.g., via offspring birth dates) experiences of adolescent pregnancy as operationally defined by the respective authors, (d) studies published in English, and (e) original empirical contributions published in peer-reviewed journals. Attempts to contact the corresponding authors were made when sample characteristics needed to determine a study's inclusion were not reported or easily identifiable in the respective study. Studies using both prospective and retrospective methods of data collection were included in the analysis. Adolescent pregnancy was defined as pregnancy or motherhood prior to age 20 years for the majority of studies (n = 18) with two studies reporting an upper age limit of 20 years and one study reporting an upper age limit of 21 years (these studies are denoted in Table II, as is the fact that the percentage of enrollees older than 20 years is minute). CSA was defined per respective study operational definition criteria and thus is broadly defined to include unwanted sexual experiences ranging from overt verbal advances, exposure to sexual media, unwanted touching, or penetration. This range of sexual abuse constitutes a wide spectrum of relatively mild to more severe forms; however, most studies included cases at varying points along this continuum and there were no studies that focused solely on the mild or severe ends. Hence, this broad definition of CSA was essentially unavoidable and was utilized because it reflects the nature of the majority of definitions that currently comprise the CSA literature facilitating the inclusion of as many relevant studies as possible.
Table II.
Summary of Studies Included in the Secondary Meta-analysisa
| Citation | Sexually abused/ pregnant n (%) | Total N |
|---|---|---|
| Boyer and Fine (1992b) | 295 (62) | 476c |
| Butler and Burton (1990) | 22 (54) | 41 |
| Esperat and Esparza (1997)b | 51 (46) | 111 |
| Fiscella et al (1998) | 126 (13) | 957d |
| Herman-Giddens et al. (1998) | 231 (31) | 734 |
| Kellogg et al. (1999)b | 75 (49) | 153e |
| Steven-Simon and McAnarney (1994) | 42 (33) | 127 |
aAll studies reported in this table examined samples where all subjects were currently pregnant or mothering.
bThis study reported a total sample size of 535, however 59 subjects provided insufficient or conflicting data and were excluded from this analysis. This resulted in a reduced total sample size of 476.
cAlthough the total sample size for this study was reported as 1,026 we analyzed only those who were sexually abused (N = 126) in comparison to the total number of non-abused (N = 831) resulting in total N = 957 for purposes of the present meta-analysis.
dTotal sample size reported in this study was 166. However, the authors indicated 13 subjects (8% of sample) were unsure whether they experienced sexual abuse and were therefore excluded in our analysis.
eOperational definitions of adolescent pregnancy included pregnancies over the age of 20 for these studies: 11% were aged 20–21 in the Boyer and Fine (1992) study; 6% were aged 19–20 in the Esperat and Esparza (1997) study; we were unable to obtain the distribution of 20–21 year-olds from the Kellogg et. al., (1999) study. To assess potential bias in the estimated odds attributable to these three studies, a nested likelihood ratio test was performed for the full (N = 21) versus nested (N = 18) models. Results indicated that there was not a significant difference in model fit between the full (Odds = 0.81; −2 log-likelihood = 49.10) and nested (Odds = 0.77; −2 log-likelihood = 44.10) models, χ 2(3) = 5.00, p =.17. Hence, these three studies did not significantly influence the overall odds derived in the secondary meta-analysis.
Literature Search
Literature searches of peer-reviewed journals were conducted on the PubMed, Medline, CINAHL, PsycArticles, and PsychInfo databases between the years 1980 and 2007 to identify studies meeting our inclusion criteria. Each search crossed the term “sexual abuse” with terms associated with adolescent pregnancy. The reference sections of identified studies and literature reviews (Becker-Lausen & Rickel, 1995; Blinn-Pike et al., 2002; Tyler, 2002) examining child sexual abuse were also reviewed to retrieve studies not included in the results of our electronic searches.
The searches yielded a total of 407 articles, all of which were returned from electronic searches and article reviews, screened, and cross-referenced to remove duplicates. Of this pool, a total of 40 articles met our criteria, warranting further examination. A closer examination of these 40 articles resulted in 20 being excluded based on the following grounds: (a) the outcome variable did not include pregnancy per se but instead focused on high-risk sexual behaviors (Abma, Driscoll, & Moore, 1998; Hillis, Anda, Felitti, & Marchbanks, 2001; Rainey et al., 1995; Senn, Carey, Vanable, Coury-Doniger, & Urban, 2006; Upchurch & Kusunoki, 2004), (b) the study's focus was on childhood maltreatment combined into a single category precluding the disaggregating of child sexual abuse from other forms of maltreatment (Smith, 1996; Thornberry, Ireland, & Smith, 2001), (c) the study's author(s) did not respond to requests for additional data so as to facilitate the primary or secondary analyses (Buzi et al., 2003; Mason, Zimmerman, & Evans, 1998; Nagy, DiClemente, & Adcock, 1995; Roberts, O’Connor, Dunn, & Golding, 2004), (d) all the participants were sexually abused (i.e., a non-abused comparison group was not included) (Cinq-Mars, Wright, Cyr, & McDuff, 2003; Raj et al., 2000), (e) analyses focused on male paternity (Anda et al., 2001, 2002; Pierre, Shrier, Emans, & DuRant, 1998), and (f) the article reported a review of the literature and no original data were presented (Becker-Lausen & Rickel, 1995; Blinn-Pike et al., 2002; Resnick & Acierno, 1997; Stevens-Simons & Reichert, 1994). As a result, we were able to include a comprehensive array of extant data including 12 of the 15 articles referenced in the review of Blinn-Pike et al. (2002) [3 were excluded in our initial set of 20 articles (Nagy et al., 1995; Rainey et al., 1995; Smith, 1996)] plus 8 additional articles published between 1980 to 2007, totaling 20 articles.
Thirteen of the remaining 20 articles met all inclusion criteria, yielding 14 distinct studies; the article by Saewyc, Magee, and Pettingell (2004) reported on two samples (designated in this paper as Saewyc, 2004); therefore, we gleaned 14 studies from the 13 articles. These 14 studies constitute our primary meta-analysis: the aggregate between-group effect size estimate of an odds ratio (OR) test among four distinct cells of individuals including sexually abused/pregnant, sexually abused/non-pregnant, non-abused/pregnant, and non-abused/non-pregnant cells (Table I). There were seven remaining articles meeting full inclusion criteria but whose study design did not include a non-pregnant comparison group (Table II). Although not optimally designed for inclusion in our primary meta-analysis, these studies contain valuable information about the rate of abused females within samples of pregnant adolescents and therefore were considered supplementary in nature. As such, our secondary meta-analysis included these seven supplementary studies in addition to the pregnant arms (sexually abused/pregnant vs. non-abused/pregnant) of the 14 studies used in the primary meta-analysis. Hence, all 21 studies constituted the basis for our secondary meta-analysis: the probability of having a history of CSA among pregnant adolescents.
Table I.
Summary of Studies Included in the Primary Meta-analysis
| Citation | Sexually abused/ pregnant n (%) | Sexually abused/ Non-pregnant n (%) | Non-abused/ Pregnant n (%) | Non-abused/ non-pregnant n (%) | Total Na | Study design | Country |
|---|---|---|---|---|---|---|---|
| Adams and East (1999) | 16 (55) | 13 (45) | 34 (49) | 36 (51) | 99 | I; R | US |
| Chandy et al. (1996) | 98 (10) | 913 (90) | 50 (5) | 961 (95) | 2,022 | S; R | US |
| Fergusson et al. (1997) | 14 (16) | 76 (84) | 29 (7) | 401 (93) | 520 | I; R | NZ |
| Haley et al. (2004) | 67 (48) | 74 (52) | 27 (32) | 57 (68) | 225 | S; R | CAN |
| Herrenkohl et al. (1998) | 33 (48) | 36 (52) | 20 (28) | 51 (72) | 140 | I; R | US |
| Hillis et al. (2004) | 728 (32) | 1534 (68) | 1,410 (21) | 5,416 (79) | 9,088 | S; R | US |
| Kenney et al. (1997) | 250 (37) | 432 (63) | 253 (21) | 975 (79) | 1,910 | S; R | US |
| Noll et al. (2003) | 22 (33) | 44 (67) | 7 (10) | 65 (90) | 138 | Ib; P | US |
| Romans et al. (1997) | 40 (16) | 207 (84) | 15 (7) | 206 (93) | 468 | I; R | NZ |
| Roosa et al. (1997) | 254 (36) | 451 (64) | 273 (21) | 1,025 (79) | 2,003 | S; R | US |
| Saewyc et al. (2004) | 979 (26) | 2,786 (74) | 1097 (11) | 8,879 (89) | 13,741 | S; R | US |
| Saewyc et al. (2004) | 580 (22) | 2,058 (78) | 952 (10) | 8,569 (90) | 12,159 | S; R | US |
| Stock et al. (1997) | 21 (7) | 286 (93) | 65 (3) | 2,032 (97) | 2,404 | S; R | US |
| Widom & Kuhns (1996) | 12 (16) | 64 (84) | 51 (21) | 193 (79) | 320 | Ib; P | US |
aThe total N reflects the total number of subjects across each of the four cells analyzed and may not necessarily reflect the total N reported in studies where these four cells represents only a portion of the total N.
bInterview method in these cases indicates a substantiated CPS investigation occurred.
I, Interview; S, Survey; P, Prospective; R, Retrospective; US, United States; CAN, Canada; NZ, New Zealand.
Data Coding
All information was collected from tables, figures, or text of the respective study and coded accordingly. Based on the study descriptions and reported methodologies of the eligible studies, coding was accomplished to determine sample characteristics such as sexual abuse status, pregnancy status, study design, study method, and country where the study was conducted. Sexual abuse status was coded as sexually abused (1) versus non-abused (0) and adolescent pregnancy status was coded as pregnant (1) versus non-pregnant (0). Study design was categorized as either using a retrospective (retrospective recall of prior sexual abuse or adolescent pregnancy, or both) or prospective (longitudinal follow-up of victims with substantiated, confirmed sexual abuse into adolescence and early adulthood in order to ascertain adolescent pregnancy rates) means of data collection. Study method was classified based on whether the researchers used interview (face-to-face interview), survey (checklist or medical record search), or documentation [via Child Protective Services (CPS) reports] to capture sexual abuse. Since there were only two studies relying on CPS reports (Noll et al., 2003; Widom & Kuhns, 1996), this method was combined with other interview studies for purposes of method evaluation because it most closely resembles interview methodology (i.e., interviews with social workers and other individuals comprise the case reports) and so that we could enhance power to detect differences between studies interview versus survey methods. Study country of origin was coded simply by identifying and listing where the study was conducted and categorized as US or Outside US. Study design, method, country, and sample and subsample sizes in Table I were rated to determine coding reliability by two independent coders. Kappa coefficients for these variables ranged from. 69 to 1.00, indicating substantial to perfect agreement. Discrepancies in coding were reconciled and a consensus was achieved. Table I summarizes data retrieved and coded from each of the 14 studies in the primary meta-analysis and contrasts four distinct groups of females, as depicted in columns 1 through 4: sexually abused/pregnant, sexually abused/non-pregnant, non-abused/pregnant, and non-abused/non-pregnant. Table II summarizes data coded from each of the seven studies that were included in the secondary meta-analysis and did not have non-pregnant comparison groups.
Results
Analytic Strategy
The goal of meta-analysis is to derive a single best estimate of a population effect size, utilizing individual parameter estimates reported across several studies. Our primary meta-analysis concerned the odds (as expressed in terms of ORs) of an adolescent pregnancy occurring in individuals with and without a history of CSA. We derived estimates of effect size using OR of the binary outcome (pregnant vs. not pregnant), via SAS PROC MIXED, and their associated log variances based on individual study point estimates. A mean OR was then calculated from all individual study point estimates to reflect the overall estimable effect size (Sutton, Abrams, Jones, Sheldon, & Song, 2000). Our secondary meta-analysis focused only on studies of adolescents who were already pregnant and the probability of prior CSA histories present in these studies. Hence, we consider this secondary analysis to be supplemental and not definitive in nature because only non-comparative binary outcomes could be examined, simply reflecting the probability of these particular samples of pregnant adolescents having a prior history of CSA.
Primary Meta-analysis
Cochran's Q Homogeneity statistic indicated significant heterogeneity (p <.01) between studies. A significant Q-statistic suggests that the error observed in a group of studies is significantly different than what would be expected from sampling error alone and is likely the result of additional variation and indicates the necessity to apply a random effects model in order to estimate a common effect size while controlling this heterogeneity (Knapp & Hartung, 2003; Petitti, 2001). A random effects model was then examined to calculate a reliable estimate of the effect size while incorporating between study variance. Random effects models incorporate heterogeneity by assuming that the study effects are randomly distributed within a sample taken from a population of all studies. Results of the random effects model produced an effect size estimate of OR = 2.21 (95% CI: 1.94–2.51), indicating that victims of CSA are 2.21 times more likely to experience an adolescent pregnancy than are women without such histories. As is depicted in the forest plot of Fig. 1, 12 of the 14 studies reported significantly higher rates of adolescent pregnancy among girls who had a previous history of CSA.
Figure 1.

Forest plot of studies included in the primary meta-analysis depicting the likelihood (via odds ratio effect size calculations) of childhood sexual abuse victims experiencing an adolescent pregnancy. Note: *Significant OR (p <.05).
Although by definition the random effects estimate is unbiased with respect to study heterogeneity, a set of post hoc analyses attempted to identify the potential sources of heterogeneity across studies, given the significant Q-statistic at the fixed effects level. Covariates defining study design, method, and country were univariately (one at a time) added to the primary meta-analysis. F-values associated with covariates were then evaluated for significance. Statistical tests of heterogeneity and covariate analyses typically have lower power than other meta-analytic tests. Hence, as suggested by others (Petitti, 2001), we adopted a significance level of p <.10 instead of traditional levels of p <.05 to avoid Type II errors. Each covariate had a non-significant F-value: study design, F = 2.26, p = 0.13; method, F = 0.60, p = 0.44; and country, F = 0.06, p = 0.81. Non-significant F-values suggested that covariates did not significantly alter the overall OR derived from the primary meta-analysis.
Sensitivity analyses were conducted in order to evaluate whether any single study was overly influential, thereby biasing the effect size estimate. Serial sensitivity analyses involving each of the 14 studies consisted of comparisons between the mean effect size generated in the full random effects model and the effect sizes generated in reduced models that omitted one study at a time. If any single study was extremely influential in the overall mean effect size estimate, then omitting that study would produce a significantly different mean OR. Results indicate that the OR's did not significantly differ across the 13 nested models (range OR: 2.12–2.53), suggesting that there was not a single study biasing the overall mean estimate.
Secondary Meta-analysis
The secondary meta-analysis focused on the non-comparative binary outcome of the probability of pregnant adolescents having had a prior history of CSA. For this meta-analysis, the pregnant arms from each of the 14 studies used in the primary analysis were combined with the additional 7 pregnant-only studies described in Table II resulting in a total of 21 studies from which to calculate the probability of having a history of CSA in samples of pregnant adolescents. The effect sizes reported in Fig. 2 were calculated by evaluating the number of events (sexually abused/pregnant) divided by the number of non-events (non-abused/pregnant) using the same analytic procedures as described above for the primary meta-analysis. As was the case in the primary meta-analysis, the Q-statistic was significant, suggesting significant heterogeneity between studies and necessitating the use of a random effects model to control for this heterogeneity. Results from the random effects model yielded an overall effect size estimate (as expressed in terms of “odds” yielded from the SAS PROC MIXED output) equal to 0.81 (range 0.15–3.14), which was significantly different from zero, as illustrated in the forest plot of Fig. 2. This resulting statistic reflects that, on average across 21 studies, the probability that a pregnant adolescent had a prior history of CSA was roughly 4.5 out of 10 (i.e., 0.81/(1 + 0.81) = 0.45). As can be seen in Table II, three of the studies included on the secondary analysis included some women over the age of 20 years. Secondary analyses were performed with and with and without these three studies, with no significant differences in the overall odds for this nested comparison.
Figure 2.
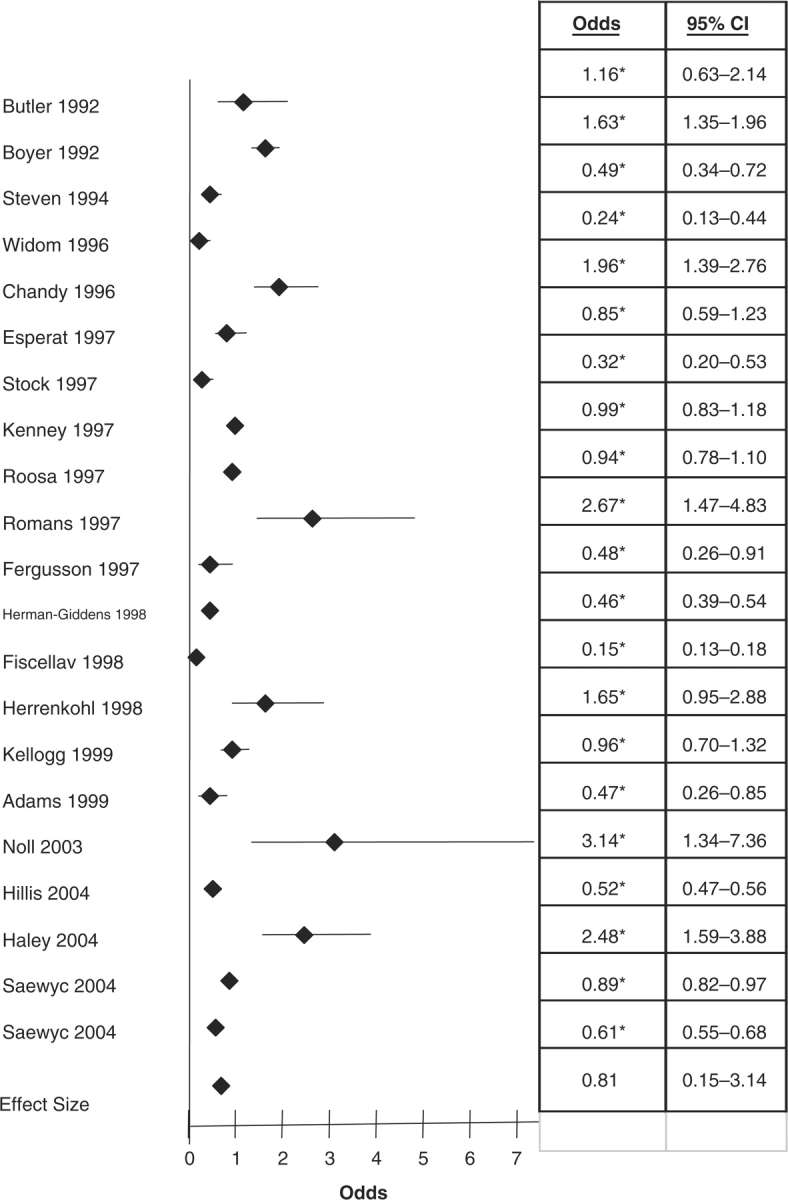
Forest plot of studies included in the secondary analysis depicting the odds of a pregnant adolescent having a history of childhood sexual abuse. Note: *Significant OR (p <.05).
Discussion
Overall, results from this study lend further empirical support to the conclusion that CSA increases the risk of becoming pregnant during adolescence. Based on our primary analysis of 14 distinct samples using appropriate comparison groups, women who had a history of CSA were more than two times more likely to have experienced a pregnancy in adolescence than women who did not experience abuse. This result, based on an aggregate estimated effect size from 14 studies, was upheld when stringent evaluative procedures were employed including differential methodological covariates and serial study specificity evaluations. To our knowledge, this is the first systematic meta-analysis to empirically test the extent of the relationship between CSA and adolescent pregnancy, which is a considerable advancement relative to extant generalized conclusions that have been based on subjective reviews of the literature (Blinn-Pike et al., 2002). A secondary, supplemental meta-analysis of the pregnant-only arms of 21 studies suggested that, on average, 4.5 in 10 pregnant adolescents likely have a prior history of CSA. It should be noted that the studies used in this secondary analysis may not necessarily be representative of the larger population of pregnant adolescents because several were regionally (Boyer & Fine, 1992) or racially (Fiscella et al., 1998) focused. However, none of these studies included samples at particularly high risk (i.e., samples selected solely on low socioeconomic status) such that generalizability would be systematically compromised. Albeit not based on controlled methodologies and not necessarily representative of all pregnant adolescents, this secondary meta-analysis provides supplemental evidence for an empirical association between CSA and adolescent pregnancy. Considered in light of US adolescent pregnancy rates that are on the rise for the first time in almost two decades, these results imply that victims of CSA may be a particularly important group of adolescents to target for intervention.
Possible Mechanisms Leading Sexually Abused Children to Adolescent Pregnancy
There are several plausible, theoretical reasons why CSA in particular might be associated with higher rates of adolescent pregnancy. First, many of the identified pregnancy risk factors for adolescents in general have also been studied as correlates or outcomes attributable, at least in part, to the experience of sexual abuse (Cicchetti & Lynch, 1995; Feiring, Taska, & Lewis, 2002; Kendler et al., 2000; Thornberry et al., 2001; Trickett & McBride-Chang, 1995). Ergo, it is quite plausible that the experience of CSA serves to amplify these risks. Second, due to the explicit sexual nature of this form of abuse, there are likely unique risk mechanisms operating for victims that may not necessarily be salient for non-victims or victims of other forms of childhood adversity.
For example, models for the development of psychopathology (Cicchetti & Carlson, 1989) posit that child abuse likely requires a child to make adaptations that may alter the child's developmental trajectory and disrupt the consolidation of emotional or social-cognitive skills, or both. Several conceptual models have been proposed describing how forms of maltreatment might affect social cognitions including the alteration of cognitive appraisals (i.e., cognitive distortions) of themselves, others, and the world (Briere, 1992). Such distortions may include confused sexual boundaries, ambiguities regarding sexual appropriateness, compulsive or overly negative attitudes toward sex, or both, and the pairing of sexuality with violence or exploitation, or both. Distortions that directly impact sexual decision-making and sexual activities could be thought of as “pregnancy-vulnerable cognitions” and likely constitute one plausible pathway to inordinate early pregnancy. Indeed, in one of the few longitudinal, prospective studies of the sexual development of abused females (Noll et al., 2003), sexually abused females reported significantly greater sexual distortions (i.e., were more preoccupied with sex by reporting more sexual thoughts and feelings, displayed more ambivalent sexual attitudes, and expressed a heightened desire to become pregnant) than their non-abused adolescent counterparts. These variables were, in turn, related to early and risky sexual behaviors and teenage motherhood.
Post-traumatic stress disorder is highly common in victims of CSA (Kendall-Tackett, Williams, & Finkelhor, 1993; Paolucci, Genuis, & Violato, 2001) and, due in part to its associated dissociative features and high comorbidity with substance and alcohol use disorders, can contribute to impairments in judgment (Bugental, 1993; Jones & Barlow, 1990) and interfere with accurate appraisal of threat and consequences thereby precluding appropriate action in sexual risk situations. Furthermore, there is emerging evidence that children exposed to chronic and traumatic forms of stress, such as sexual abuse, experience a global dysregulation in the hypothalamus–pituitary–adrenal (HPA) axis (Carrion et al., 2002; DeBellis, Lefter, Trickett, & Putnam, 1994; Gunnar & Vazquez, 2001; Hart, Gunnar, & Cicchetti, 1996), which may in turn affect certain regions of the brain implicated in neurocognitive impairments and high-risk social and emotional functioning that are thought to predispose high-risk behaviors in adolescents (Dahl, 2001; Giancola, Mezzich, & Tarter, 1998; Kirisci, Tarter, Vanyukov, Reynolds, & Habeych, 2004).
Limitations and Recommendations for Future Study
The results presented in this meta-analytic study should be considered in light of several limitations. First, the generalizability of these analyses is limited to the effects of CSA. We focused on CSA because (a) there is theoretical parsimony in examining risk and outcome variables that are both sexual in nature, (b) much of the previous literature has focused on sexual abuse as opposed to other forms of abuse providing a substantial pool of articles from which to power our analysis, and (c) we hoped to clarify some of the mixed conclusions about whether any relationship exists between sexual abuse and adolescent pregnancy. While this deliberate focus on sexual abuse adds precision to our aims and strengthens our primary conclusions, we are unable to comment on the risk posed by other forms of childhood abuse or adversity. Moreover, as highlighted in the Methods section, operational definitions of CSA varied widely across studies and adolescent pregnancy rates were not always reported for subtypes of sexual abuse. This made it difficult to discern if adolescent pregnancy might be more strongly related to one form of sexual abuse versus another.
We were also limited in our ability to conduct moderator analyses that would add important insight into factors that alter the risk posed by CSA. For instance, we were unable to examine the effects of race, socioeconomic status, or abuse severity (e.g., genital fondling vs. penetration) in moderator analyses because the power to do so was limited. More importantly, most studies, with notable exception (Stock et al. 1997), lacked sufficient detail regarding differential rates of adolescent pregnancy associated with these types of variables. The limited reporting of such detail also rendered us unable to differentiate between those who only experienced sexual abuse versus those who experienced sexual abuse in conjunction with other forms of child maltreatment. Although we were careful to maximize homogeneity by focusing on studies of victims of CSA, we did so in full acknowledgment that sexual abuse quite often occurs within the context of other forms of abuse and that it would be almost impossible to have conducted this investigation utilizing studies of sexual abuse alone or as isolated from other forms of overlapping, co-occurring, or past maltreatment (cf. Smith, 1996; Thornberry et al., 2001). Although we cannot definitively conclude that CSA in and of itself increases risk for adolescent pregnancy, the presence of this variable (albeit overlapping with other forms of abuse in some studies) was strongly related to adolescent pregnancy in almost all of the studies included in this review.
There was considerable methodological heterogeneity in the studies included in the present analysis, which could potentially limit generalizability. Studies varied in terms of retrospective recall versus protective service reports of childhood abuse, country of origin, longitudinal versus cross-sectional study, and interview versus survey data collection. Despite this heterogeneity, use of the random effects model provided a reliable estimate of the relationship between CSA and adolescent pregnancy while controlling for this heterogeneity. Moreover, sources of methodological variation did not significantly alter the average effect size estimation nor did any one study significantly bias the overall effect size estimate. Use of the random effects model, assessing for the effects of specified covariates, and the conducting of the sensitivity analysis adds support to the conclusions drawn from the main finding of this article—that CSA is a significant risk factor for adolescent pregnancy.
In light of these limitations, we make the following recommendations for future studies aimed at examining how childhood abuse might be related to adolescent pregnancy. First, we recommend the assessment and reporting of the specific details regarding abuse characteristics and the types and subtypes of abuse. Such reporting would facilitate continuity in operational definitions of abuse across studies, and more comprehensive statistical models elucidating the moderating effects of distinct abuse types, the co-occurrence of multiple forms of abuse, and abuse severity. Second, we recommend the inclusion of assessment methods with the greatest potential for reliable and detailed reporting of CSA such as interview methods confirmed by protective service records. Finally, the employment of controlled prospective, longitudinal designs, that include large sets of potential confounding and mediating variables, is greatly needed in order to (a) determine whether CSA, in and of itself, sets females at risk and (b) more fully understand the processes that place victims on a trajectory that increases their chances of becoming pregnant during adolescence—a line of research that is sorely needed before causal assertions can be drawn and before systematic study of protective factors can commence.
Conclusions
Findings gleaned from this meta-analysis indicate that the experience of CSA significantly increased the risk of becoming pregnant during adolescence. We join other researchers and practitioners (Adams & East, 1999; Kellogg et al., 1999) in recommending that the assessment and monitoring of abuse survivors should extend into adolescence and specifically address issues related to sexual development, sexual decision-making, and other factors associated with sexual risk-taking and early pregnancy. These results may be particularly important for pediatric psychologists and other practitioners who have knowledge of patient victimization histories. In such cases, careful monitoring of abuse-related risk factors (such as persisting PTSD symptoms, distortions in self-concept or sexual attitudes, and physiological dysregulation) may improve overall care and health outcomes for victims. In pediatric settings, psychologists who encounter young mothers should be aware of the possibility of abuse histories in order to provide optimal care and appropriate pre- and post-natal services for both the mother and her infant. Given that there are approximately 140,000 new substantiated cases of CSA each year in the US (National Child Abuse and Neglect Data System, 2007), addressing the risk factors associated with being sexually abused may have a considerable impact on the overall national rate of adolescent pregnancy.
Acknowledgments
This paper was supported in part by NIH grants R01HD052533 and T32DK063929. Authors would like to acknowledge the collegial support of Jeffrey D. Long, Julie London, Christine Hampton, and Ann Daltrey Madden.
Conflict of interest: None declared.
References
- Abma J, Driscoll A, Moore K. Young women's degree of control over first intercourse: An exploratory analysis. Family Plannning Perspectives. 1998;30(1):12–18. [PubMed] [Google Scholar]
- Adams JA, East PL. Past physical abuse is significantly correlated with pregnancy as an adolescent. Journal of Pediatric and Adolescenct Gynecology. 1999;12(3):133–138. doi: 10.1016/s1038-3188(99)00005-4. [DOI] [PubMed] [Google Scholar]
- Anda RF, Chapman DP, Felitti VJ, Edwards V, Williamson DF, Croft JB, et al. Adverse childhood experiences and risk of paternity in teen pregnancy. Obstetrics and Gynecology. 2002;100(1):37–45. doi: 10.1016/s0029-7844(02)02063-x. [DOI] [PubMed] [Google Scholar]
- Anda RF, Felitti VJ, Chapman DP, Croft JB, Williamson DF, Santelli J, et al. Abused boys, battered mothers, and male involvement in teen pregnancy. Pediatrics. 2001;107(2):E19. doi: 10.1542/peds.107.2.e19. [DOI] [PubMed] [Google Scholar]
- Becker-Lausen E, Rickel AU. Integration of teen pregnancy and child abuse research: Identifying mediator variables for pregnancy outcome. Journal of Primary Prevention. 1995;16:39–53. doi: 10.1007/BF02407232. [DOI] [PubMed] [Google Scholar]
- Berry EH, Shillington AM, Peak T, Hohman MM. Multi-ethnic comparison of risk and protective factors for adolescent pregnancy. Child and Adolescent Social Work Journal. 2000;17(2):79–96. [Google Scholar]
- Blinn-Pike L, Berger T, Dixon D, Kuschel D, Kaplan M. Is there a causal link between maltreatment and adolescent pregnancy? A literature review. Perspectives on Sexual and Reproductive Health. 2002;34(2):68–75. [PubMed] [Google Scholar]
- Boardman LA, Allsworth J, Phipps MG, Lapane KL. Risk factors for unintended versus intended rapid repeat pregnancies among adolescents. Journal of Adolescent Health. 2006;39(4):e1–e8. doi: 10.1016/j.jadohealth.2006.03.017. [DOI] [PubMed] [Google Scholar]
- Boyer D, Fine D. Sexual abuse as a factor in adolescent pregnancy and child maltreatment. Family Planning Perspectives. 1992;24(1):4–11. , 19. [PubMed] [Google Scholar]
- Brazzell JF, Acock AC. Influence of attitudes, significant others, and aspirations on how adolescents intend to resolve a premarital pregnancy. Journal of Marriage & the Family. 1988;50(2):413–425. [Google Scholar]
- Briere J. Methodological issues in the study of sexual abuse effects. Journal of Consulting & Clinical Psychology. 1992;60:196–203. doi: 10.1037//0022-006x.60.2.196. [DOI] [PubMed] [Google Scholar]
- Brooks-Gunn J, Furstenberg FF. The children of adolescent mothers: Physical, academic, and psychological outcomes. Developmental Review. 1986;6(3):224–251. [Google Scholar]
- Bugental DB. Communication in abusive relationships: Cognitive constructions of interpersonal power. American Behavioral Scientist. 1993;36:288–308. [Google Scholar]
- Butler J, Burton L. Rethinking teenage childbearing: Is sexual abuse a missing link? Family Relations: Journal of Applied Family & Child Studies. 1990;39(1):73–80. [Google Scholar]
- Buzi RS, Tortolero SR, Roberts RE, Ross MW, Addy RC, Markham CM. The impact of a history of sexual abuse on high-risk sexual behaviors among females attending alternative schools. Adolescence. 2003;38(152):595–605. [PubMed] [Google Scholar]
- Carrion V, Weems C, Ray R, Glaser B, Hessl D, Reiss A. Diurnal salivary cortisol in pediatric posttraumatic stress disorder. Biological Psychiatry. 2002;51(7):575–582. doi: 10.1016/s0006-3223(01)01310-5. [DOI] [PubMed] [Google Scholar]
- Chandy JM, Blum RW, Resnick MD. Female adolescents with a history of sexual abuse: Risk outcome and protective factors. Journal of Interpersonal Violence. 1996;11:503–518. [Google Scholar]
- Cicchetti D, Carlson V. Child maltreatment: Theory and research on the causes and consequences of child abuse and neglect. New York: Cambridge University Press; 1989. [Google Scholar]
- Cicchetti D, Lynch M. Failures in the expectable environment and their impact on individual development: The case of child maltreatment. In: Cicchetti D, Cohen DJ, editors. Developmental psychopathology, Vol. 2: Risk, disorder, and adaptation. Wiley series on personality processes. New York: John Wiley & Sons; 1995. pp. 32–71. [Google Scholar]
- Cinq-Mars C, Wright J, Cyr M, McDuff P. Sexual at-risk behaviors of sexually abused adolescent girls. Journal of Child Sexual Abuse. 2003;12:2–18. doi: 10.1300/J070v12n02_01. [DOI] [PubMed] [Google Scholar]
- Connolly J, Furman W, Konarski R. The role of peers in the emergence of heterosexual romantic relationships in adolescence. Child Development. 2000;71(5):1395–1408. doi: 10.1111/1467-8624.00235. [DOI] [PubMed] [Google Scholar]
- Corcoran J. Consequences of adolescent pregnancy/parenting: A review of the literature. Social Work in Health Care. 1998;27(2):49–67. doi: 10.1300/J010v27n02_03. [DOI] [PubMed] [Google Scholar]
- Dahl RE. Affect regulation, brain development, and behavioral/emotional health in adolescence. CNS Spectrums. 2001;6(1):60–72. doi: 10.1017/s1092852900022884. [DOI] [PubMed] [Google Scholar]
- DeBellis MD, Lefter L, Trickett PK, Putnam FW. Urinary catecholamine excretion in sexually abused girls. Journal of the American Academy of Child Adolescent Psychiatry. 1994;33:320–327. doi: 10.1097/00004583-199403000-00004. [DOI] [PubMed] [Google Scholar]
- East PL, Jacobson LJ. The younger siblings of teenage mothers: A follow-up of their pregnancy risk. Developmental Psychology. 2001;37(2):254–264. doi: 10.1037/0012-1649.37.2.254. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Feiring C, Taska L, Lewis M. Adjustment following sexual abuse discovery: The role of shame and attributional style. Developmental Psychology. 2002;38(1):79–92. doi: 10.1037//0012-1649.38.1.79. [DOI] [PubMed] [Google Scholar]
- Fergusson DM, Horwood LJ, Lynskey MT. Childhood sexual abuse, adolescent sexual behaviors and sexual revictimization. Child Abuse & Neglect. 1997;21(8):789–803. doi: 10.1016/s0145-2134(97)00039-2. [DOI] [PubMed] [Google Scholar]
- Fiscella K, Kitzman HJ, Cole RE, Sidora KJ, Olds D. Does child abuse predict adolescent pregnancy? Pediatrics. 1998;101(4 Pt. 1):620–624. doi: 10.1542/peds.101.4.620. [DOI] [PubMed] [Google Scholar]
- Furstenberg FF, Jr, Brooks-Gunn J, Morgan SP. Adolescent mothers and their children in later life. Family Planning Perspectives. 1987;19(4):142–151. [PubMed] [Google Scholar]
- Giancola PR, Mezzich AC, Tarter RE. Disruptive, delinquent and aggressive behavior in female adolescents with a psychoactive substance use disorder: Relation to executive cognitive functioning. Journal of Studies on Alcohol. 1998;59(5):560–567. doi: 10.15288/jsa.1998.59.560. [DOI] [PubMed] [Google Scholar]
- Gunnar MP, Vazquez DM. Low cortisol and a flattening of expected daytime rhythm: Potential indices of risk in human development. Development & Psychopathology. 2001;13:515–538. doi: 10.1017/s0954579401003066. [DOI] [PubMed] [Google Scholar]
- Haley N, Roy E, Leclerc P, Boudreau JF, Boivin JF. Characteristics of adolescent street youth with a history of pregnancy. Journal of Pediatric & Adolescence Gynecology. 2004;17(5):313–320. doi: 10.1016/j.jpag.2004.06.006. [DOI] [PubMed] [Google Scholar]
- Hamilton BE, Martin JA, Ventura SJ. Births: Preliminary data for 2006. National Vital Statistics Report. 2007;56(7):1–18. [PubMed] [Google Scholar]
- Hart J, Gunnar M, Cicchetti D. Altered neuroendocrine activity in maltreated children related to symptoms of depression. Development & Psychopathology. 1996;8(1):201–214. [Google Scholar]
- Herman-Giddens ME, Kotch JB, Browne DC, Ruina E, Winsor JR, Jung J.-W, et al. Childbearing patterns in a cohort of women sexually abused as children. Journal of Interpersonal Violence. 1998;13(4):504–513. [Google Scholar]
- Herrenkohl EC, Herrenkohl RC, Egolf BP, Russo MJ. The relationship between early maltreatment and teenage parenthood. Journal of Adolescence. 1998;21(3):291–303. doi: 10.1006/jado.1998.0154. [DOI] [PubMed] [Google Scholar]
- Hillis SD, Anda RF, Dube SR, Felitti VJ, Marchbanks PA, Marks JS. The association between adverse childhood experiences and adolescent pregnancy, long-term psychosocial consequences, and fetal death. Pediatrics. 2004;113(2):320–327. doi: 10.1542/peds.113.2.320. [DOI] [PubMed] [Google Scholar]
- Hillis SD, Anda RF, Felitti VJ, Marchbanks PA. Adverse childhood experiences and sexual risk behaviors in women: A retrospective cohort study. Family Planning Perspectives. 2001;33(5):206–211. [PubMed] [Google Scholar]
- Hofferth SL, Reid L, Mott FL. The effects of early childbearing on schooling over time. Family Planning Perspectives. 2001;33(6):259–267. [PubMed] [Google Scholar]
- Hoffman S. By the numbers: the public cost of teen childbearing. Washington, DC: The National Campaign To Prevent Teen Pregnancy; 2006. [Google Scholar]
- Jaccard J, Dittus PJ. Adolescent perceptions of maternal approval of birth control and sexual risk behavior. American Journal of Public Health. 2000;90(9):1426–1430. doi: 10.2105/ajph.90.9.1426. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jones JC, Barlow DH. The etiology of post-traumatic stress disorder. Clinical Psychology Review. 1990;10:299–328. [Google Scholar]
- Kellogg ND, Hoffman TJ, Taylor ER. Early sexual experiences among pregnant and parenting adolescents. Adolescence. 1999;34:293–303. [PubMed] [Google Scholar]
- Kendall-Tackett KA, Williams LM, Finkelhor D. Impact of sexual abuse on children: A review and synthesis of recent empirical studies. Psychological Bulletin. 1993;113(1):164–180. doi: 10.1037/0033-2909.113.1.164. [DOI] [PubMed] [Google Scholar]
- Kendler KS, Bulik CM, Silberg J, Hettema JM, Myers J, Prescott CA. Childhood sexual abuse and adult psychiatric and substance use disorders in women: An epidemiological and cotwin control analysis. Archives of General Psychiatry. 2000;57(10):953–959. doi: 10.1001/archpsyc.57.10.953. [DOI] [PubMed] [Google Scholar]
- Kenney JW, Reinholtz C, Angelini PJ. Ethnic differences in childhood and adolescent sexual abuse and teenage pregnancy. Journal of Adolescent Health. 1997;21(1):3–10. doi: 10.1016/s1054-139x(97)00035-9. [DOI] [PubMed] [Google Scholar]
- Kirisci L, Tarter RE, Vanyukov M, Reynolds M, Habeych M. Relation between cognitive distortions and neurobehavior disinhibition on the development of substance use during adolescence and substance use disorder by young adulthood: A prospective study. Drug and Alcohol Dependence. 2004;76(2):125–133. doi: 10.1016/j.drugalcdep.2004.04.015. [DOI] [PubMed] [Google Scholar]
- Knapp G, Hartung J. Improved tests for a random effects meta-regression with a single covariate. Statistics in Medicine. 2003;22(17):2693–2710. doi: 10.1002/sim.1482. [DOI] [PubMed] [Google Scholar]
- Marin BV, Coyle KK, Gomez CA, Carvajal SC, Kirby DB. Older boyfriends and girlfriends increase risk of sexual initiation in young adolescents. Journal of Adolescent Health. 2000;27(6):409–418. doi: 10.1016/s1054-139x(00)00097-5. [DOI] [PubMed] [Google Scholar]
- Martin JA, Hamilton BE, Sutton PD, Ventura SJ, Menacker F, Kirmeyer S, et al. United States Department of Health and Human Services. National Vital Statistics Report. Vol. 56. Atlanta: Centers for Disease Control; 2007. Births: Final Data for 2005; pp. 1–104. [PubMed] [Google Scholar]
- Mason WA, Zimmerman L, Evans W. Sexual and physical abuse among incarcerated youth: Implications for sexual behavior, contraceptive use, and teenage pregnancy. Child Abuse & Neglect. 1998;22(10):987–995. doi: 10.1016/s0145-2134(98)00080-5. [DOI] [PubMed] [Google Scholar]
- Meschke LL, Zweig JM, Barber BL, Eccles JS. Demographic, biological, psychological, and social predictors of the timing of first intercourse. Journal of Research and Adolescence. 2000;10(3):315–338. [Google Scholar]
- Mezzich AC, Giancola PR, Lu SY, Parks SM, Ratica GM, Dunn M. Adolescent females with a substance use disorder: Affiliations with adult male sexual partners. American Journal on Addictions. 1999;8(3):190–200. doi: 10.1080/105504999305802. [DOI] [PubMed] [Google Scholar]
- Miller BC. Family influences on adolescent sexual and contraceptive behavior. Special Issue: Promoting sexual health and responsible sexual behavior. 2002;39(1):22–26. doi: 10.1080/00224490209552115. [DOI] [PubMed] [Google Scholar]
- Miller BC, Benson B, Galbraith KA. Family relationships and adolescent pregnancy risk: A research synthesis. Developmental Review. 2001;21(1):1–38. [Google Scholar]
- Miller BC, McCoy JK, Olson TD. Dating age and stage as correlates of adolescent sexual attitudes and behavior. Journal of Adolescent Research. 1986;1(3):361–371. doi: 10.1177/074355488613009. [DOI] [PubMed] [Google Scholar]
- Moore KA, Myers DE, Morrison DR, Nord CW, Brown B, Edmonston B. Age at first childbirth and later poverty. Journal of Research on Adolescence. 1993;3(4):393–422. doi: 10.1207/s15327795jra0304_5. [DOI] [PubMed] [Google Scholar]
- Nagy S, DiClemente R, Adcock AG. Adverse factors associated with forced sex among southern adolescent girls. Pediatrics. 1995;96(5 Pt. 1):944–946. [PubMed] [Google Scholar]
- National Child Abuse and Neglect Data System. Child maltreatment 2005. Washington, DC: US Government Printing Office; 2007. [Google Scholar]
- Noll JG, Trickett PK, Putnam FW. A prospective investigation of the impact of childhood sexual abuse on the development of sexuality. Journal of Consulting and Clinical Psychology. 2003;71(3):575–586. doi: 10.1037/0022-006x.71.3.575. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nord CW, Moore KA, Morrison DR, Brown B, Myers DE. Consequences of teen-age parenting. Journal of School Health. 1992;62(7):310–318. doi: 10.1111/j.1746-1561.1992.tb01249.x. [DOI] [PubMed] [Google Scholar]
- Paolucci EO, Genuis ML, Violato C. A meta-analysis of the published research on the effects of child sexual abuse. Journal of Psychology. 2001;135(1):17. doi: 10.1080/00223980109603677. [DOI] [PubMed] [Google Scholar]
- Petitti DB. Approaches to heterogeneity in meta-analysis. Statistics in Medicine. 2001;20(23):3625–3633. doi: 10.1002/sim.1091. [DOI] [PubMed] [Google Scholar]
- Pierre N, Shrier LA, Emans SJ, DuRant RH. Adolescent males involved in pregnancy: Associations of forced sexual contact and risk behaviors. Journal of Adolescent Health. 1998;23:364–369. doi: 10.1016/s1054-139x(98)00035-4. [DOI] [PubMed] [Google Scholar]
- Polacsek M, Celentano DD, O’Campo P, Santelli J. Correlates of condom use stage of change: Implications for intervention. AIDS Education and Prevention. 1999;11(1):38–52. [PubMed] [Google Scholar]
- Quinlivan JA, Tan LH, Steele A, Black K. Impact of demographic factors, early family relationships and depressive symptomatology in teenage pregnancy. The Australian and New Zealand Journal of Psychiatry. 2004;38(4):197–203. doi: 10.1080/j.1440-1614.2004.01336.x. [DOI] [PubMed] [Google Scholar]
- Rainey DY, Stevens-Simon C, Kaplan DW. Are adolescents who report prior sexual abuse at higher risk for pregnancy? Child Abuse and Neglect. 1995;19(10):1283–1288. doi: 10.1016/0145-2134(95)00088-p. [DOI] [PubMed] [Google Scholar]
- Raj A, Silverman JG, Amaro H. The relationship between sexual abuse and sexual risk among high school students: Findings from the 1997 Massachusetts Youth Risk Behavior Survey. Maternal and Child Health Journal. 2000;4(2):125–134. doi: 10.1023/a:1009526422148. [DOI] [PubMed] [Google Scholar]
- Resnick HS, Acierno R. Health impact of interpersonal violence 2: Medical and mental health outcomes. Behavioral Medicine. 1997;23(2):65. doi: 10.1080/08964289709596730. [DOI] [PubMed] [Google Scholar]
- Roberts R, O’Connor T, Dunn J, Golding J. The effects of child sexual abuse in later family life; mental health, parenting and adjustment of offspring. Child Abuse & Neglect. 2004;28:525–545. doi: 10.1016/j.chiabu.2003.07.006. [DOI] [PubMed] [Google Scholar]
- Romans SE, Martin JL, Morris EM. Risk factors for adolescent pregnancy: How important is child sexual abuse? Otago Women's Health Study. N Z Med J. 1997;110(1037):30–33. [PubMed] [Google Scholar]
- Roosa MW, Tein J.-Y, Reinholtz C, Angelini PJ. The relationship of childhood sexual abuse to teenage pregnancy. Journal of Marriage & the Family. 1997;59(1):119–130. [Google Scholar]
- Saewyc EM, Magee LL, Pettingell SE. Teenage pregnancy and associated risk behaviors among sexually abused adolescents. Perspectives on Sexual and Reproductive Health. 2004;36(3):98–105. doi: 10.1363/psrh.36.98.04. [DOI] [PubMed] [Google Scholar]
- Salazar LF, DiClemente RJ, Wingood GM, Crosby RA, Harrington K, Davies S, et al. Self-concept and adolescents’ refusal of unprotected sex: A test of mediating mechanisms among African American girls. Prevention Science. 2004;5(3):137–149. doi: 10.1023/b:prev.0000037638.20810.01. [DOI] [PubMed] [Google Scholar]
- Santelli J, Kaiser J, Hirsch L, Radosh A, Simkin L, Middlestadt S. Initiation of sexual intercourse among middle school adolescents: The influence of psychosocial factors. Journal of Adolescent Health. 2004;34(3):200–208. doi: 10.1016/j.jadohealth.2003.06.004. [DOI] [PubMed] [Google Scholar]
- Santelli J, Lowry R, Brener N, Robin L. The association of sexual behaviors with socioeconomic status, family structure, and race/ethnicity among US adolescents. American Journal of Public Health. 2000;90(10):1582–1588. doi: 10.2105/ajph.90.10.1582. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Scaramella LV, Conger RD, Simons RL, Whitbeck LB. Predicting risk for pregnancy by late adolescence: A social contextual perspective. Developmental Psychology. 1998;34(6):1233–1245. doi: 10.1037//0012-1649.34.6.1233. [DOI] [PubMed] [Google Scholar]
- Senn TE, Carey MP, Vanable PA, Coury-Doniger P, Urban MA. Childhood sexual abuse and sexual risk behavior among men and women attending a sexually transmitted disease clinic. Journal of Consulting & Clinical Psychology. 2006;74(4):720–731. doi: 10.1037/0022-006X.74.4.720. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sieving RE, Beuhring T, Resnick MD, Bearinger LH, Shew M, Ireland M, et al. Development of adolescent self-report measures from the National Longitudinal Study of Adolescent Health. Journal of Adolescent Health. 2001;28(1):73–81. doi: 10.1016/s1054-139x(00)00155-5. [DOI] [PubMed] [Google Scholar]
- Silverman JG, Raj A, Mucci LA, Hathaway JE. Dating violence against adolescent girls and associated substance use, unhealthy weight control, sexual risk behavior, pregnancy, and suicidality. JAMA. 2001;286(5):572–579. doi: 10.1001/jama.286.5.572. [DOI] [PubMed] [Google Scholar]
- Smith C. The link between childhood maltreatment and teenage pregnancy. Social Work Research. 1996;20(3):131–141. [Google Scholar]
- Stevens-Simon C, Kelly L, Singer D, Cox A. Why pregnant adolescents say they did not use contraceptives prior to conception. Journal of Adolescent Health. 1996;19(1):48–55. doi: 10.1016/1054-139X(95)00281-V. [DOI] [PubMed] [Google Scholar]
- Stevens-Simon C, McAnarney ER. Childhood victimization: Relationship to adolescent pregnancy outcome. Child Abuse & Neglect. 1994;18(7):569–575. doi: 10.1016/0145-2134(94)90083-3. [DOI] [PubMed] [Google Scholar]
- Stevens-Simons C, Reichert S. Sexual abuse, adolescent pregnancy, and child abuse. Archives of Pediatrics & Adolescent Medicine. 1994;148(1):23–27. doi: 10.1001/archpedi.1994.02170010025005. [DOI] [PubMed] [Google Scholar]
- Stock JL, Bell MA, Boyer DK, Connell FA. Adolescent pregnancy and sexual risk-taking among sexually abused girls. Family Planning Perspectives. 1997;29(5):200–203, 227. [PubMed] [Google Scholar]
- Sutton AJ, Abrams KR, Jones DR, Sheldon TA, Song F. Methods for meta-analysis in medical research. West Sussex, England, UK: John Wiley & Sons; 2000. [Google Scholar]
- The Alan Guttmacher Institute. U.S. teenage pregnancy statistics: National and state trends and trends by race and ethnicity. New York: The Alan Guttmacher Institute; 2006. [Google Scholar]
- Thornberry T, Ireland T, Smith C. The importance of timing: The varying impact of childhood and adolescent maltreatment on multiple problem outcomes. Development and Psychopathology. 2001;13(4):957–979. [PubMed] [Google Scholar]
- Trickett PK, McBride-Chang C. The developmental impact of different forms of child abuse and neglect. Developmental Review. 1995;15(3):311–337. [Google Scholar]
- Tyler KA. Social and emotional outcomes of childhood sexual abuse: A review of recent research. Aggression and Violent Behavior. 2002;7(6):567–589. [Google Scholar]
- Upchurch DM, Kusunoki Y. Associations between forced sex, sexual and protective practices, and sexually transmitted diseases among a national sample of adolescent girls. Women's Health Issues. 2004;14(3):75–84. doi: 10.1016/j.whi.2004.03.006. [DOI] [PubMed] [Google Scholar]
- Whitbeck LB, Yoder KA, Hoyt DR, Conger RD. Early adolescent sexual activity: A developmental study. Journal of Marriage & the Family. 1999;61(4):934–946. [Google Scholar]
- Widom CS, Kuhns JB. Childhood victimization and subsequent risk for promiscuity, prostitution, and teenage pregnancy: A prospective study. American Journal of Public Health. 1996;86:1607–1612. doi: 10.2105/ajph.86.11.1607. [DOI] [PMC free article] [PubMed] [Google Scholar]