

Abstract
Objective This article describes website use and behavioral outcomes in a multi-component lifestyle intervention promoting healthy diet and exercise. Methods A 2-year randomized clinical trial to improve bone density in 228 adolescent girls, the intervention included a website designed to enhance intervention adherence, retention of participants, and behavioral outcomes. Measures included diet and exercise recalls, surveys, and web-usage data. Results Website use was associated with increases in calcium intake (ß = 69.72, p =.01, ES = 0.15) and high-impact activity (ß = 10.93, p =.04, ES =.13). Use of web pages related to behavioral feedback and communications was not significantly associated with behavioral outcomes. The most visited website pages had content related to incentive points, caption contests, and fun facts. Conclusions Web elements of a multi-component intervention may promote retention and engagement in target behaviors. Such websites may be most acceptable to adolescent participants if they blend fun and behavioral elements, rather than exclusively focusing on behavioral changes.
Introduction
E-health, the use of interactive technologies (e.g., Internet, CD-ROMs, and voice response systems), is emerging as a promising tool to address the limited capacity of the health care system to provide health behavior change and chronic disease management interventions (Ahern, Kreslake, & Phalen, 2006). The Internet is one of the most powerful tools e-health has to offer, both for health care recipients to gather information and for health care providers to deliver a variety of behavioral/educational interventions. Almost 80% of Internet users report seeking health information online (Fox, 2006). Furthermore, 44% of Internet users report searching for exercise or fitness information with an equal percentage reporting that information accessed on the Internet changed the way they think about diet, exercise, or stress management (Fox, 2006).
Over the past few years, numerous studies have used online technologies to deliver a variety of health interventions including those targeting mental health issues such as panic disorder (e.g., Carlbring, Ekselius, & Andersson, 2003) and depression (e.g., Clarke et al., 2005). Other on-line programs promote weight management and physical activity through Internet interventions (e.g., Napolitano et al., 2003; Papadaki & Scott, 2005). The use of e-health modalities in the delivery and/or support of health care interventions has advantages over traditional in-person health services including: reduced cost and increased convenience for users and health care providers alike, overcoming user isolation and stigma, and enabling options for more individual-tailoring (Griffiths, Lindenmeyer, Powell, Lowe, & Thorogood, 2006). Furthermore, web-based interventions that incorporate peer support have been well-received by participants and found to reduce levels of functional impairment (e.g., Barrera, Glasgow, McKay, Boles, & Feil, 2002).
Teens are perhaps the ideal targets for Internet intervention. Nearly three-quarters (73%) of adults in the United States use the Internet; in adolescents that number jumps to 93% (Lenhart, Madden, Macgill, & Smith, 2007). In addition, the developmental importance of peer support among adolescents (Brown, Eicher, & Petrie, 1986) makes the use of Internet sites incorporating peer interaction a natural fit for this age group. Finally, it has been widely reported that adolescents are more comfortable with technologies like the Internet and perceive them as more helpful than do adults (Macgill, 2007). Thus, by adding a website component to a conventional intervention aimed at adolescents, our intervention was structured to take advantage of the fact that the Internet is both highly attractive to teens and widely used by them.
The Youth, Osteoporosis, and Understanding Total Health Project (YOUTH) was a randomized controlled trial testing the efficacy of a health plan-based, 2-year lifestyle intervention to increase bone mineral density (BMD) and prevent bone loss in female adolescents (DeBar et al., 2004; DeBar et al., 2006). Both dietary (increased consumption of calcium and fruits and vegetables) and physical activity (high-impact exercise and strength training) behaviors were targeted as a means of increasing BMD among participants. The main intervention components included both group and individual in-person visits as well as coaching telephone calls and the completion of weekly self-monitoring postcards; these study components are described in detail in other publications (DeBar et al., 2004; 2006). The YOUTH intervention was offered to adolescent HMO members who otherwise had no pre-existing connections with one another. We believed it was important to create a virtual, and real, community-support network in the absence of the shared environment typical of many conventional school-based health promotion programs. All youth randomized to the experimental condition were granted access to a study website designed to foster communication and interaction among participants and project staff, as well as to provide feedback about intervention-related behavioral changes.
In this article, we describe how intervention participants used the study website as one element of a multi-component lifestyle intervention. We describe the components of the website and its development, address issues of site access, and discuss how website use related to general adherence to the overall YOUTH intervention. Finally, we analyze whether website usage improved health behavior (dietary and physical activity) outcomes in this study. These analyses are exploratory, as the overall YOUTH study was powered only to examine principle dietary, bone density, and activity outcomes affected by the overall multi-component intervention. Our study included a randomized control condition of participants who used a parallel site with the same design, look, and feel as the intervention site but that did not include any section emphasizing study-specific lifestyle targets or personalized feedback about behavioral goal attainment. This paper focuses on results from the intervention arm only.
Methods
Study Population
We selected girls with age- and gender-adjusted body mass index (BMI)- values below the national median (Blum et al., 2001) as targets for the YOUTH intervention, because of their heightened risk of not achieving maximal bone mass density and therefore being at risk for later development of osteoporosis. We calculated BMIs based on a review of health records, after which the girls received mailed study invitations followed by telephone calls from research staff. An informational meeting for interested families was held to review the study and complete informed consent procedures prior to randomization. The HMO Human Subjects Protection Committee monitored and approved all study procedures.
Because the YOUTH study design, intervention, and primary outcomes have been fully described elsewhere (DeBar et al., 2004, 2006), here we include only a brief description of our study sample. The main YOUTH cohort consisted of 228 healthy 14–16 year-old girls enrolled from a HMO in the Pacific Northwest. Of the original cohort, 209 completed follow-up assessments and were the focus of our main study outcome analyses (DeBar et al., 2006). We report here on the subsample of 82 girls receiving the intervention (Table I) which excludes the 86 participants randomized to the comparison condition and the 41 participants enrolled before the website was fully operational.
Table I.
Intervention Study Participant Characteristics and Baseline Behaviors (N = 82)
| Characteristics | Mean (SD; range) or percentages |
|---|---|
| General demographics | |
| Age (years at randomization) | 15.6 (.6; 14.6–16.9) |
| White (%)a | 80.5% |
| BMI | 20.5 (1.9; 16.1–24.6) |
| Mother's education (percentage reporting post- secondary education)a | 78.9% |
| Family socioeconomic status (annual household income) | $68,656 ($31,395; $10,000–125,000) |
| Nutrition | |
| Calcium intake (mg/day) | 996.7 (474.1; 193.3–2,739.3) |
| Fruit/vegetable intake (servings/day) | 3.7 (2.5;.2–17.0) |
| Physical activity | |
| Total physical activity (min/week) | 477.0 (506.4; 0–2,590) |
| High impact activity (min/week) | 94.6 (140.3; 0–756) |
| Strength/weight training (min/week) | 35.4 (121.0; 0–910) |
| Screen time (hours/day) | 2.4 (1.6; 0–7) |
aTo preserve anonymity, we did not further disaggregate race/ethnicity or education categorization of participant demographics.
Intervention
The intervention aimed to increase consumption of calcium and fruits and vegetables (diet) and increase physical activity involving high-impact and weight-bearing activities (exercise). Specifically, participants were urged to consume 1350 mg/day of calcium (four glasses of milk a day or the equivalent) and eight servings of fruits and vegetables, as well as to participate in both 20 min of high impact exercise and 10 min of strength training twice a week. The rationale for these behavioral targets is described elsewhere (DeBar et al., 2004). Attention was given to avoid iaotrogenic effects of concern when working with female adolescents (e.g., eating disorders) by ensuring that intervention content emphasized increasing healthy behaviors (e.g., increasing fruit and vegetable intake) rather than dietary restriction and including content in both in-person and web components aimed at helping participants develop a healthy body image.
In addition to the in-person components of the intervention (overnight retreat, monthly events) and quarterly coaching calls, participants were encouraged to use the study website at least once a week for the duration of the 2-year study. The website was password protected and housed on a secure server. During the orientation retreat, participants received their username and password and went through the log on process with study staff. They had time to explore the website and ask questions. The majority of the study participants (95%) indicated no barriers to Internet access when queried upon enrollment in the study.
Website Development and Content
Focus Groups
Before starting recruitment for the randomized control trial (RCT), we conducted six preliminary focus groups with freshman and sophomore girls from three regional high schools (N = 59) to guide development of website content and design. Participants were recruited through counselors and health teachers at the schools. All focus group data were transcribed, and common themes were identified using ATLAS software. Data analysis suggested that teens were less interested in on-line components of the intervention, such as web-based monitoring tools, than we had anticipated.
Participants were asked in an open-ended manner about features of program websites they would be most inclined to use. Based on their responses, our goal was to develop a “fun” website that would enhance study retention and adherence rather than serve primarily as a means for delivering the bulk of the intervention targets. We determined that self-monitoring should be conducted by postcards sent via regular U.S. mail instead of the website, and we limited this planned portion of the website to providing feedback on participants’ behavioral progress in comparison to the average of other girls in the intervention (My Progress described more fully below).
Content Development
The primary objectives of the website were to keep participants informed of project activities, offer communication with staff and other participants, and provide feedback about intervention participants’ progress toward intervention dietary and physical activity goals. We tried to develop an engaging and easy-to-use site that offered health information and was interactive. Ultimately, our goal was to produce a website that enhanced the sense of community among participants [through their ability to communicate remotely with one another (see YOUTH Talk below) and view one another's “Scrapbook” (see below)] and offered fun and interactive pages to aid study retention and adherence.
The website for the intervention arm provided information specific to the lifestyle-change goals of the study, including calcium intake, fruit and vegetable consumption, and increased physical activity (specifically high-impact activity).
Special Features Within the Website
Three website elements centered on communication: YOUTH Talk, a bulletin board for participants to communicate with one another and with staff; I Need, a form participants could fill out to ask questions to staff and receive a direct confidential reply through the website; and Ask a Health Question, a separate forum in which participant questions and staff answers were anonymously posted for everyone to view. A Resources section provided handouts and other materials from study events as well as links to health information relevant for teens. Hot Tips had summaries on exercise, nutrition, wellness/stress management, beauty (e.g., skin and hair care), and fashion.
To promote community-building, the Scrapbook provided a page where participants could view photos and biographies of staff and other YOUTH participants. Finally, the Fun Stuff menu had a picture caption contest where participants could win monthly prizes, take pop-up quizzes, and “count up” and “cash in” incentive points (redeemable with local merchants) they earned for project participation.
In addition, the experimental condition website included a My Progress page where participants could view graphs of monthly exercise, food intake, and weight training data. These data were collected from the self-monitoring postcards that participants were asked to fill out and return to us by mail. On this page, participants could view their individual information compared to the cohort average.
Measures
Phone Calls
Prior to baseline, we conducted three unannounced 24-h diet and 72-h exercise phone recalls. Additional follow-up phone recalls were conducted every 2 months throughout the study by certified dietary interviewers (for more detail on these methods see DeBar et al., 2004, 2006). These recalls were averaged across every two time points to maximize reliability (e.g., months 2 and 4; months 6 and 8; etc.), for a total of six 4-month time periods over the 2 years; 93% of the participants had data for at least five of the six study periods included.
Tracking Website Usage Through Automation and Self-Reporting
To measure website usage, we relied on two methods: an automated tracking system, which stored each participant's website use, and self-reporting. The automated tracking system collected information on all pages and areas of the site viewed, as well as time spent on the site. In addition, at the 12-month follow-up visit, we asked participants to report on their patterns using the YOUTH website, computers, and the Internet in general.
We chose to analyze the number of times the study website was visited as our overall measure of use. We also captured the number of page-specific hits to analyze content-specific use. Both were examined as time varying covariates to take into account whether visits were spread out over the course of the 2-year intervention or occurred within a narrower window of time after joining the study, as is often seen with web-based interventions (Christensen, Griffiths, Groves, & Korten, 2006; Eysenbach, 2005).
Categorizing Usage
We recorded website use within each of six 4-month segments. Those youth logging on in not more than one of the 4-month segments were categorized as “infrequent” users; “intermittent” users if they logged on in two to three segments, and “consistent” users if they logged on during at least four of the six study segments. In each case, we only counted the logons in which participants visited one of the behavioral feedback or communications web pages.
We report the total accumulated time participants spent on the study website in our descriptive analyses (Tables II and III). However, we do not include time on the overall website or specific page views in our inferential analyses (Table IV) because of concerns about their appropriateness and accuracy. For example, number of pages viewed may misrepresent overall usage because of the different levels of interactivity on different web pages (e.g., some web pages are more time-intensive than others, both by design and due to content). Similarly, total website time may be an overestimate of usage because of difficulties determining the end of a session (i.e., participants leaving the website through a hyperlink or leaving a window dormant do not trigger the end of a session, so metered time continues to accrue until the session ends or the computer is turned off).
Table II.
Characteristics of Internet Use (Intervention Participants Only, N = 82)
| Characteristics | Mean (SD; range) or percentages |
|---|---|
| Number of website visits (from automated tracking)a | 23.2 (38.6; 0–233) |
| Minutes of website use (from automated tracking)a | 112.1 (138.6; 0–623) |
| Minutes per week on study website (self-report)a | 4.4 (4.9; 0–22.5) |
| Reasons for visiting study websiteb | |
| To learn new information | 50.0% |
| To communicate with other participants in the study | 7.3% |
| To communicate with YOUTH staff | 11.0% |
| Because it is fun | 22.0% |
| Because of the Caption Contest | 18.3% |
| To check my number of points earned | 52.4% |
| I like to see my feedback | 28.1% |
| Like best about study websiteb | |
| The design | 18.3% |
| Learn new information | 36.6% |
| Communicating with other participants in the study | 9.8% |
| Communicating with YOUTH staff | 11.0% |
| It is fun | 23.17% |
| The Caption Contest | 19.3% |
| The points system | 50.0% |
| Seeing my feedback | 26.8% |
| Like least about study websiteb | |
| The design | 9.8% |
| The information doesn't change quick enough | 30.5% |
| No one else uses the website | 8.5% |
| The points system | 0.0% |
| Communicating with other participants in the project | 1.2% |
| Communicating with staff on the project | 0.0% |
| Seeing my feedback | 1.2% |
| Barriers to useb | |
| Too busy | 69.5% |
| The information doesn't change often enough | 9.8% |
| The website is boring | 9.8% |
| Additional feedback | |
| Percent of girls who would recommend a website for future studies | 70.7% |
aAll website use variables represent the entire 2-year intervention period.
bAnswers not mutually exclusive.
Table III.
Participant Characteristics by Consistency of Study Website Use
| Infrequent Internet Use (n = 26) | Intermittent Internet Use (n = 31) | Consistent Internet Use (n = 25) | F or χ2 | Sig. | |
|---|---|---|---|---|---|
| Internet Use Patterns | |||||
| Number of overall visits | 3.6 (7.3) | 8.2 (9.8) | 62.0 (50.8) | NA | NA |
| Percentage of study periods web use | 21.8 (20.4) | 49.5 (18.0) | 90.0 (11.8) | NA | NA |
| Overall minutes of use | 18.6 (26.2) | 59.7 (44.4) | 274.4 (145.5) | NA | NA |
| Number of days between first and last sign-on | 216.2 (297.7) | 472.4 (191.5) | 630.6 (54.5) | NA | NA |
| Self-reported weekly use | 4.0A (2.7) | 4.60 A (4.6) | 7.9 B (5.2) | 4.42 | .02 |
| Demographics | |||||
| Age (years at randomization) | 15.5 (0.5) | 15.7 (0.6) | 15.7 (0.7) | 1.42 | .25 |
| Percentage white | 84.6% | 80.6% | 76.0% | .60 | .74 |
| Mother's education (percentage post-secondary education) | 73.9% | 82.8% | 79.2% | .60 | .74 |
| Distance between home and study meeting site | 12.6A (5.4) | 18.0B (10.1) | 13.6A (6.8) | 3.86 | .03 |
| Study adherence | |||||
| Team meeting attendance | 1.8A (1.9) | 2.1A (1.9) | 3.6B (2.2) | 6.59 | 0.00 |
| Number of self-monitoring postcards returneda | 19.6A (25.8) | 25.7A (29.8) | 46.7B (31.9) | 6.06 | 0.00 |
| Baseline behavioral characteristics | |||||
| Calcium intake (mg/day) | 915.1 (444.3) | 1080.8 (482.4) | 977.4 (495.2) | .89 | .41 |
| Fruit/vegetable servings/day | 3.3 (1.6) | 3.7 (2.2) | 4.2 (3.5) | .99 | .37 |
| Total physical activity (min/week) | 610.7 (718.5) | 445.2 (401.8) | 377.4 (308.4) | 1.47 | .24 |
| High impact activity (min/week) | 48.7 (122.4) | 115.8 (157.2) | 116.0 (128.8) | 2.09 | .13 |
| Strength/weight training (min/week) | 54.4 (186.8) | 27.3 (63.4) | 25.7 (86.4) | .46 | .63 |
| Screen time hours/day | 2.3 (1.4) | 2.3 (1.5) | 2.8 (2.1) | .73 | .49 |
Note. A, B superscripts denote groups that are significantly different. NA, not applicable.
aIt was possible for participants to complete and return 100 weekly self-monitoring postcards over the 2 years of the project; thus the numbers can be roughly interpreted as 20%, 26%, and 47% of the postcards returned among the infrequent, intermittent, and consistent internet users, respectively.
Table IV.
Summary of Web Use Coefficient or Odds Ratio by Dependent Variablesa
| Independent variables |
||||||
|---|---|---|---|---|---|---|
| Total number of website visits |
Total number of intervention-related website hits |
|||||
| Original DV measureb | Met DV study target (1 = Yes) | Percentage of DV study target met | Original DV measureb | Met DV study target (1 = Yes) | Percentage of DV study target met | |
| Dependent variables (“DV”) | βcoef. | OR | βcoef. | βcoef. | OR | βcoef. |
| Dietary | ||||||
| Calcium intake (mg/day) | 69.72** | 1.21& | .01 | 15.58 | 1.05 | 0.00 |
| Fruits and vegetables intake (servings/day) | −.13 | 1.13 | .00 | −.11 | 1.13 | −.01 |
| Soda intake (ounces/day) | .09 | NA | NA | −.14 | NA | NA |
| Cola intake (ounces/day) | .09 | NA | NA | .02 | NA | NA |
| Physical activity | ||||||
| High-impact activity (min/week) | 10.93* | 1.22 | .04& | 1.13 | .98 | .00 |
| Strength/weight training (min/week) | 2.59 | 1.11 | .03 | 3.15 | .94 | −.01 |
| Combined activity targetc | NA | 1.33& | NA | NA | .97 | NA |
Note. NA, not applicable.
aAll models include distance, baseline computer use, mother's education, and household income as covariates in addition to website use, which is transformed as log(x + 1).
bModel also includes baseline values.
cCombination of high impact and strength/weight training targets.
*p ≤.05, **p ≤.01; &p ≤.10
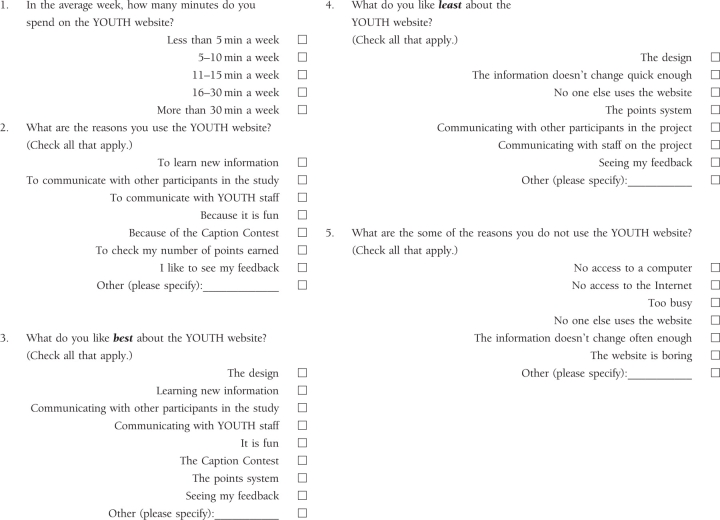
Survey on Self-Reported Website Usage
Five questions pertaining to participants’ use of the study website were developed by the study investigators; these were included on the self-report survey administered after the first year of the study. The questions asked participants about the number of self-reported minutes they spent per week on the study website, the reasons that they used the study website, and what they liked best and least about the website. Specific study questions are included in the appendix. While the principal analyses were based on participants’ tracked logons to the study website, including these questions allowed us to more fully describe participants’ use of the study website.
Unit of Measure for Adherence
To measure overall participant adherence, we decided to use the metric of in-person intervention sessions rather than include the proportion of returned self-monitoring postcards. We chose this unit of measurement because we believed that in-person sessions provided a more independent and therefore conservative metric than did the return of self-monitoring postcards (we were concerned that the return of self-monitoring postcards was more closely related to page-specific website use rather than overall adherence because participants could view these data on the My Progress web pages as a gauge of their progress toward behavioral study goals).
Determining Distance to Research Center
We expected that distance might be an important determinant of website use, anticipating that longer travel times (associated with higher opportunity costs and expense) would motivate participants to substitute web-based intervention components for in-person sessions. Therefore, as a variable in these analyses, we included distance between a participant's residence and the research center where in-person intervention sessions were held. Geocoding software (MapMarker Plus) provided latitude and longitude of the main intervention site and the participant's address to calculate distance. If a participant's address was missing or the street address did not resolve to a detailed value, we substituted median latitude and longitude measures by zip code in our calculations (13.4% of the girls had missing address values).
Other measures not reported here included bone mass density, urinary and blood markers of bone turn-over, strength measurements, and general health questionnaires (see DeBar et al., 2004, for more detail on these outcomes).
Analysis Plan
This report is limited to analyses conducted on the following: bi-monthly 24 h diet and 72 h exercise phone recalls; responses to baseline questionnaires on participant characteristics and behaviors; and the responses to the 12-month follow-up questionnaire specific to use patterns of the YOUTH website. Most reported findings are descriptive in nature. Descriptive and inferential statistical analyses were conducted using SAS Release 9.1 (SAS Institute Inc, Cary, NC) and STATA version 9.2 (StataCorp, College Station, Tex). Comparisons of Internet use patterns, demographics, study adherence to the larger RCT, and baseline behavioral characteristics between the three levels of web use (infrequent, intermittent, and consistent website users) were conducted using ANOVAs for continuous variables and chi-square analyses for categorical variables.
We analyzed the relation between dietary and physical activity outcomes and tracked website use by fitting random effects models to the data with random effects taking the form of random intercepts for different girls. We used logit models with dichotomous outcomes and linear models with continuous dependent variables. Each outcome measure was analyzed separately as an unadjusted continuous measure, a binary value indicating whether or not the intervention target level was reached (1 = met 100% or more of target), and a percentage of the target reached, limited to 100%. Analyzing dietary and physical activity data as a percentage of target attained provided a straightforward way to remove extreme values often encountered in these types of data. All available recall data from baseline through month 24 were included in the analyses.
The test of the coefficient on website use provided us with a basis to infer the relation between intervention target outcomes and website use. We constructed website use as a time-varying covariate, which counted the number of unique website logons or webpage hits between each assessment and utilized a natural log (log of value plus one) transformation to approximate a normal distribution of the data. We ran separate models for total number of website visits and total number of webpage hits of content related more directly to behavioral feedback and communications. The latter represented the use of the following website pages: YOUTH Talk, I Need, Ask a Health Question, or My Progress.
Other covariates included baseline measures of mother's education, household income, the teen's self-reported hours of computer usage per week, total number of in-person intervention sessions attended, and distance from the main intervention location. With the exception of the analyses of combined activity target (high-impact and strength training), all models included baseline values of the dependent variable. Total number of in-person intervention sessions was included in these analyses to control for the effect of adherence to other elements of the intervention.
Results
Characteristics of Participants
Intervention participant characteristics at baseline are shown in Table I. The sample was mostly Caucasian, with a large proportion reporting that mothers had a high level of educational attainment (78.9% reporting post-secondary education) and reflected a fairly high socioeconomic status (average annual family income $68,656). Participants reported fairly high levels of calcium (996.7 mg) and fruit and vegetable intake at study onset and reported being generally physically active (more than an hour of total activity on average per day) with only modest levels of reported daily screen time (2.4 h; operationalized as a combination of “time on computer” and “time watching TV”).
Characteristics of Internet Use
Table II shows characteristics of Internet use for those participating in the study intervention. Automated tracking records indicated that participants logged on to the study website 23 times (SD = 38.6) on average over the 2 years of intervention participation, for a total overall accumulated time of 112 min (SD = 138.6). Participants self-reported spending a little more than 4 min per week on average on the study website.
Participant Motivations, Preferences, and Opinions
The most frequently reported reason for visiting the study website was to check the number of incentive points earned (52%) and learn new information (50%), although more than a quarter of the sample (28%) reported visiting the study website to view feedback on their progress towards dietary and physical activity study targets (totals exceed 100% because youth could give more than one reason).
When asked what they liked best about the study website, participants cited the incentive point system (50%), although several cited learning new information (37%) and receiving feedback on study-related lifestyle changes (26%) as appealing study website features. When asked what they liked least about the website, 30% of participants noted that the information on the website did not change frequently enough. Despite this complaint, only 10% identified this as a barrier to using the study website. The largest single barrier cited was that participants were “too busy” to use the website more frequently (70%). Overall, 71% of the intervention participants said they recommended including a website for similar studies in the future. Figure 1 shows the overall pattern of website use underscoring the draw of the “fun” elements of the website (caption contests, fun facts, pop-up quizzes, and count-up and cash-in points) as compared to the behavioral feedback and communications portions of the website (My Progress, Youth Talk, I Need, and Ask a Health Question).
Figure 1.

Pattern of YOUTH website use by Enhanced Fitness Participants (proportion of content page “hits” to total page “hits”).
Patterns of Website Usage
We were interested in the participants’ consistency, or persistent use, of the website across the 2-year intervention; these results are presented in Table III. Categorizing website use as “infrequent”, “intermittent”, and “consistent”, we only counted the logons in which participants visited one of the behavioral feedback or communications web pages. As expected, the pattern of use showed a higher overall number of study website visits and minutes of use for the more consistent users; although, interestingly, there were no significant differences among the infrequent, intermittent, and consistent groups in the self-reported weekly use of the study website as reported in the 1-year follow-up survey.
The distance between home and study meeting site was significantly farther for intermittent users than for infrequent users; however, this relation did not hold for more consistent users. More consistent use of the study website was associated with higher rates of in-person meeting attendance and number of self-monitoring postcards returned. Interestingly, the total number of in-person sessions was only modestly correlated with total website visits (r =.20, p =.08). There were no significant differences found in baseline dietary intake and physical activity reported by those with differing levels of web use. Finally, overall reported screen time at the study onset was not associated with the consistency of study website use.
Patterns of Behavioral Change
Our last set of analyses, summarized in Table IV, examined whether changes in primary behavioral outcomes (dietary and physical activity) were associated with (1) the overall use of the website and (2) use of subset of study web pages composed of behavioral feedback and communications. Overall website use was associated with increases in calcium intake (for untransformed DV: ß = 69.72, p =.01, effect size [ES] =.15), and higher levels of high-impact activity (for untransformed DV: ß = 10.93, p =.04, ES =.13; for % of study target: ß =.04, p =.06, ES =.11). Interestingly, the specific use of study web pages related to behavioral feedback and communications did not show significant associations with these behavioral outcomes, although they were generally in the same direction as the overall web use effects.
Discussion
Primary Findings
Our results suggest a significant but modest association between overall study website use and improvements in key study behavioral targets (calcium consumption, high-impact activity). The modest effect sizes (ESs) are not surprising given that this represents variance in calcium and exercise outcomes accounted for by website usage just within the experimental participants. Typical RCTs often report the ES for the between-condition comparison of experimental and control participants, whereas this report examines effects accounted for by within-condition variation in website usage. Furthermore, this website was only a single element of a multi-component intervention that included several in-person visits. Therefore it is less surprising or concerning that this Internet element accounted for just a modest proportion of the overall change in primary outcomes. It is of note, however, that the findings held up when controlling for adherence to in-person intervention sessions, suggesting that the study website had an intervention effect above and beyond that of overall adherence to intervention elements of the study.
Interestingly, specific use of the behavioral feedback and communications elements of the study website did not show a significant association with these targets, even though we hypothesized these would be the elements most strongly associated with improvements in dietary and physical activity study targets. Furthermore, that more than one-third of webpage hits were on the Fun Stuff web pages suggests that some of the ancillary features of websites developed primarily to attract younger visitors (e.g., viewing incentive points, fun facts, caption contests) may be important elements to keep teens linked to the study and adherent to behavioral targets. Consistent with this, responses from teens during early formative research on this study suggested that they were most focused on whether intervention activities would be fun in the moment and were far less concerned about achieving behavioral changes to improve short- or longer-term health outcomes.
Secondary Findings
Secondary findings of note include the general overall acceptance and use of the website by study participants. The majority of intervention participants (56.1%) used the website in at least half of the six 4-month intervention study increments measured, with a per-participant average of nearly two dozen log-ins. Most of the teens recommended the inclusion of a similar website for future studies.
Also, the association of distance between home and study meeting site and frequency of website use was less straightforward than anticipated. Although we anticipated that those living at farther distances might use the website more frequently, we found that those who had “intermittent” study website use lived farther from the in-person intervention meetings site than did either those who were “consistent” or “infrequent” study website users. This suggests that while distance may encourage some website use, there are clearly other important factors.
Finally, those who were the most consistent Internet users returned significantly more of the weekly self-monitoring postcards. This is not surprising, as one of the study web pages allowed participants to monitor their progress toward behavioral goals and compare those to the overall average of their group; therefore, those participants completing the postcards likely had additional incentive to log on to the study website.
Study Limitations
Despite these positive findings, the study has some limitations. This study was not powered to obtain significant findings for these web elements. As such, the analytic results described here must be viewed as hypothesis-generating rather than hypothesis-testing. In addition, as is common when comparing self-reported and objectively tracked outcomes, participants appeared to over-reported the number of minutes-per-week of website use1. However, because objectively tracked outcomes were used for the main study analyses, this discrepancy should not affect the overall pattern of the outcomes.
Finally, the demographics of our sample may limit the extent to which these findings may be generalized. Study participants generally came from well-resourced households with high levels of parental post-secondary education and total household incomes; these families are also more likely than families of lower socio-economic status to have computers in their homes. Such factors may lower barriers to providing environmental support for the kinds of lifestyle changes targeted in this study. In addition, web usage patterns might have been different in an intervention which targeted a broader cross section of adolescents. Recent studies suggest that although the gap is narrowing between Internet usage rates among male and female adolescents, males remain more likely to access gaming and other entertainment applications while females are more likely to use the Internet for interpersonal communications (Jackson et al., 2008; Odell, Korgen, Schumacher, & Delucchi, 2000; Shaw & Gant, 2002). Accordingly, we likely would have seen a different pattern of usage of program components and effects on behavioral outcomes had males been included in our sample. Our sample was also comprised of healthy adolescents; recent reviews of use of web-based behavior change programs suggest healthier individuals are among those least benefiting from, yet most likely to use, such programs (Verheijden, et al., 2007). Despite such findings, others are showing the promise of Internet interventions targeted towards adolescents with chronic illnesses for whom such interventions may provide the broadest public health impact (Kyngas, 2004; Van der Meer et al., 2007).
In summary, although there have been other reports suggesting modest improvements in healthy dietary intake and physical activity among adults (Hurling et al., 2007; Park et al., 2008) and youth (Thompson et al., 2008) associated with participant web use in exclusively Internet-delivered interventions, we are aware of no other studies that have demonstrated such an effect when a website is a secondary element in a multi-component behavioral intervention in which the majority of the intervention was delivered in person such as the one reported here. As such, the current study's findings are of significance. Furthermore, our findings suggest that it may be preferable to offer an online element as just one part of a multicomponent program rather than relying solely on Internet programs in a stand alone fashion a format in which retention and adherence are frequently a problem (Baranowski et al., 2003).
Funding
National Institute of Child Health and Human Development (R01-HD037744-01 to L.L.D).
Conflicts of interest: None declared.
Acknowledgments
We thank Jen Coury for her helpful comments on previous versions of this article. In addition, without the assistance of Colleen Flattum, Gina Keppel, Chris Catlin, Patty LeGarda, Megan Porter, and Cynthia Roh, this study could not have been conducted.
Appendix
 |
Footnotes
1If participants consistently logged on close to the rate they self-reported (4 min per week on average), their overall use of the study website would result in more than 400 min of time logged onto the study website rather than the 112 min on average actually recorded.
References
- Ahern DK, Kreslake JM, Phalen JM. What is eHealth (6): Perspectives on the evolution of eHealth research. Journal of Medical Internet Research. 2006;8:e4. doi: 10.2196/jmir.8.1.e4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baranowski T, Baranowski JC, Cullen KW, Thompson DI, Nicklas T, Zakeri IE, et al. The Fun, Food, and Fitness Project (FFFP): the Baylor GEMS pilot study. Ethnicity & Disease. 2003;13:S30–S39. [PubMed] [Google Scholar]
- Barrera M, Jr, Glasgow RE, McKay HG, Boles SM, Feil EG. Do Internet-based support interventions change perceptions of social support?: An experimental trial of approaches for supporting diabetes self-management. American Journal of Community Psychology. 2002;30:637–654. doi: 10.1023/A:1016369114780. [DOI] [PubMed] [Google Scholar]
- Blum M, Harris SS, Must A, Phillips SM, Rand WM, Dawson-Hughes B. Weight and body mass index at menarche are associated with premenopausal bone mass. Osteoporosis International. 2001;12:588–594. doi: 10.1007/s001980170082. [DOI] [PubMed] [Google Scholar]
- Brown BB, Eicher SA, Petrie S. The importance of peer group (“crowd”) affiliation in adolescence. Journal of Adolescence. 1986;9:73–96. doi: 10.1016/s0140-1971(86)80029-x. [DOI] [PubMed] [Google Scholar]
- Carlbring P, Ekselius L, Andersson G. Treatment of panic disorder via the Internet: A randomized trial of CBT vs. applied relaxation. Journal of Behavioral Therapy and Experimental Psychiatry. 2003;34:129–140. doi: 10.1016/s0005-7916(03)00026-0. [DOI] [PubMed] [Google Scholar]
- Christensen H, Griffiths K, Groves C, Korten A. Free range users and one hit wonders: Community users of an Internet-based cognitive behaviour therapy program. Australian and New Zealand Journal of Psychiatry. 2006;40:59–62. doi: 10.1080/j.1440-1614.2006.01743.x. [DOI] [PubMed] [Google Scholar]
- Clarke G, Eubanks D, Reid E, Kelleher C, O’Connor E, DeBar LL, Lynch F, Nunley S, Gullion C. Overcoming Depression on the Internet (ODIN): A randomized trial of a self-help depression skills program with reminders. Journal of Medical Internet Research. 2005;7:e16. doi: 10.2196/jmir.7.2.e16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- DeBar LL, Ritenbaugh C, Vuckovic N, Stevens VJ, Aickin M, Ernst D, Elliot D, Moe E, Orwoll E, Irving LM. YOUTH: Decisions and challenges in designingan osteoporosis prevention intervention for teen girls. Preventive Medicine. 2004;39:1047–1055. doi: 10.1016/j.ypmed.2004.04.010. [DOI] [PubMed] [Google Scholar]
- DeBar L, Ritenbaugh C, Aickin M, Orwoll E, Elliot D, Dickerson J, et al. YOUTH: A health-plan based lifestyle intervention increases bone mineral density among teen girls. Archives of Pediatrics and Adolescent Medicine. 2006;160:1269–1276. doi: 10.1001/archpedi.160.12.1269. [DOI] [PubMed] [Google Scholar]
- Eysenbach G. The law of attrition. Journal of Medical Internet Research. 2005;7:e11. doi: 10.2196/jmir.7.1.e11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fox S. Online Health Search 2006. 2006 Oct 29; Washington, DC: Pew Internet & American Life Project, http://www.pewinternet.org/pdfs/PIP_Online_Health_2006.pdf.
- Griffiths F, Lindenmeyer A, Powell J, Lowe P, Thorogood M. Why are health care interventions delivered over the internet? A systematic review of the published literature. Journal of Medical internet Research. 2006;8:e12. doi: 10.2196/jmir.8.2.e10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hurling R, Catt M, DeBoni M, Fairley BW, Hurst T, Murray P, Richardson A, Sodhi JS. Using Internet and mobile phone technology to deliver an automated physical activity program: Randomized controlled trial. Journal of Medical Internet Research. 2007;9:e7. doi: 10.2196/jmir.9.2.e7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jackson LA, Zhao Y, Kolenic, A, Figerald HE, Harold R, Von Eye A. Race, gender, and information technology use: the new digital divide. Cyberpsychology & Behavior. 2008;11:437–442. doi: 10.1089/cpb.2007.0157. [DOI] [PubMed] [Google Scholar]
- Kyngas H. Support network of adolescents with chronic disease: Adolescents’ perspective. Nurs Health Sci. 2004;6:287–293. doi: 10.1111/j.1442-2018.2004.00207.x. [DOI] [PubMed] [Google Scholar]
- Lenhart A, Madden M, Macgill AR, Smith A. Teens and Social Media. Pew Internet & American Life Project. 2007 Retrieved October 15, 2008, from http://www.pewinternet.org/pdfs/PIP_Teens_Social_media_Final.pdf.
- Macgill AR. Parents, teens and technology. Pew Internet and American Life Project. 2007 Retrieved October 24, 2007, from http://pewresearch.org/pubs/621/parents-teens-and-technology.
- Napolitano MA, Fotheringham M, Tate D, Sciamanna C, Leslie E, Owen N, et al. Evaluation of an internet-based physical activity intervention: a preliminary investigation. Annals of Behavioral Medicine. 2003;25:92–99. doi: 10.1207/S15324796ABM2502_04. [DOI] [PubMed] [Google Scholar]
- Odell PM, Korgen KO, Schumacher P, Delucchi M. Internet use among female and male college students. CyberPsychology & Behavior. 2000;3:855. [Google Scholar]
- Papadaki A, Scott JA. The Mediterranean eating in Scotland experience project: Evaluation of an Internet-based intervention promoting the Mediterranean diet. British Journal of Nutrition. 2005;94:290–298. doi: 10.1079/bjn20051476. [DOI] [PubMed] [Google Scholar]
- Park A, Nitzke S, Kritsch K, Kattelmann K, White A, Boeckner L, et al. Internet-based interventions have potential to affect short-term mediators and indicators of dietary behavior of young adults. J Nutr Educ Behav. 2008;40:288–297. doi: 10.1016/j.jneb.2008.02.001. [DOI] [PubMed] [Google Scholar]
- Shaw LH, Gant LM. Users divided? Exploring the gender gap in Internet use. Cyberpsychology & Behavior. 2002;5:517. doi: 10.1089/109493102321018150. [DOI] [PubMed] [Google Scholar]
- Thompson D, Baranowski T, Cullen K, Watson K, Liu Y, Canada A. Preventive Medicine. 2008. Food, fun, and fitness internet programs for girls: Pilot evaluation of an e-Health youth obesity prevention program examining predictors of obesity. Epub ahead of print doi;10,1016/j.ypmed.2008.07.014. [DOI] [PubMed] [Google Scholar]
- Van der Meer V, van Stel HF, Detmar SB, Otten W, Sterk PJ, Sont JK. Internet-based self-management offers an opportunity to achieve better asthma control in adolescents. Chest. 2007;132:112–119. doi: 10.1378/chest.06-2787. [DOI] [PubMed] [Google Scholar]
- Verheijden MW, Jans MP, Hildebrandt VH, Hopman-Rock M. Rates and determinants of repeated participation in a web-based behavior change program for healthy body weight and healthy lifestyle. Journal of Medical Internet Research. 2007;9:1–7. doi: 10.2196/jmir.9.1.e1. [DOI] [PMC free article] [PubMed] [Google Scholar]