

Abstract
Background
Sudden cardiac arrest (SCA) is a significant public health problem and better understanding of triggers could enhance prevention. Vigorous physical activity has been suggested as a prominent trigger but has not been welcvaluated in the general population. We performed a community-based study to analyze the role of physical activity as a potential trigger of SCA.
Methods
Medical records of 1180 subjects who sustained SCA during the ongoing Oregon Sudden Unexpected Death Study (Multnomah County, Oregon, USA; 2002–05) were reviewed. Analysis was limited to first responder and hospital records of patients who experienced witnessed SCA, with information available regarding physical activity immediately prior to SCA. An estimated metabolic equivalent (MET) score was used to classify levels of physical activity.
Results
A total of 304 adults met criteria for analysis (mean age 69 years, 67% male). The majority (n=193, 63%) were performing light activities, 51 (17%) subjects were sleeping, 39 (13%) were performing moderate activities, 14 (5%) were performing heavy activities, and 7 (2%) were engaged in sexual activity. Light activities were associated with older age (72 years) and heavy activities with the youngest (51 years, p<0.001). Males were more likely to be involved in heavy activity (93% male) and the sexual activity group was exclusively male ( p=0.04).
Conclusion
Vigorous physical activity was a potential trigger of SCA in a minority (5%). The vast majority (80%) of subjects were asleep or were performing light activities. The traditional view of SCA triggers may have to be re-visited, with renewed focus on factors such as emotional stress and sleep-related disorders.
Keywords: Sudden cardiac arrest, Sudden cardiac death, Trigger, Exercise, Population, Community
1. Introduction
Sudden cardiac arrest is a significant public health problem at the global level with at least 200,000 events per year in the US. In spite of advancements in methods of resuscitation, the rate of survival following SCA continues to remain low [1,2]. In large part, the lack of advancement in prevention of SCA is due to a poor understanding of causative mechanisms. There are associations with multiple conditions such as coronary artery disease (CAD), but methods for identification of the high risk patient remain quite inadequate.
Since the majority of sudden cardiac arrests occur due to onset of a fatal ventricular arrhythmia, the substrate–trigger hypothesis is often evoked. This is a traditional concept for genesis of arrhythmia that requires the existence of both a substrate (e.g. coronary artery disease) and a trigger (an external physical or emotional factor believed to incite acute cardiovascular instability in a subject), thereby resulting in SCA. Many have postulated that physical activity and emotional stress are triggers of SCA [3–7]. However, these have not been evaluated in a community-based setting. A better understanding of potential triggers of SCA, particularly among those that suffer SCA in the general population would assist in developing measures to treat and prevent SCA. In this ongoing community-wide Oregon Sudden Unexpected Death Study, we evaluated the role of physical activity as a potential trigger of SCA.
2. Methods
2.1. Study population
The Study population consisted of all residents of Multnomah County, Oregon, who sustained SCA, from February 1, 2002 to January 31, 2005. Multnomah County, located in northwestern Oregon, covers an area of 435 square miles with an estimated population of 677,813 [8]. All cases of presumed sudden cardiac arrest in Multnomah County were reported to researchers conducting the Sudden Unexpected Death Study (SUDS) at Oregon Health & Science University, Portland, Oregon, by one of three sources: First Responders (Emergency Medical Services, EMS), Medical Examiner (ME) and the 16 hospitals in Multnomah County.
Each of these cases was then independently evaluated by a team of three cardiologists. This process of evaluation used the World Health Organization (WHO) definition for SCA and pre-determined inclusion and exclusion criteria described later in this section. In the event of a conflict of opinion, the majority opinion was considered.
2.2. Inclusion and exclusion criteria
Subjects of all ages and both genders who experienced SCA were included. SCA secondary to trauma, hemorrhage, drug overdose, suicide, pulmonary embolism and malignancy were excluded. Sudden cardiac arrests in terminally ill patients with non-cardiac disease were excluded.
2.3. Data collection
First responder and hospital records of all study subjects were reviewed for demographics and subjects’ activities prior to sustaining SCA. Hospital records, autopsy and medical examiner reports were used for information relating to CAD status.
2.4. Definitions
Witnessed SCA [1]: Sudden unexpected death that occurred within an hour of developing symptoms.
Un-witnessed SCA [1]: Sudden unexpected death in a subject within 24 h of being seen alive and symptom free.
Physical activity was defined as any form of physical activity that a subject was performing immediately prior to sustaining SCA. An estimated metabolic equivalent (MET) score was assigned to each type of physical activity based on the criteria described by Ainsworth et al. [9] and the criteria used by MIOS [10]. One MET [9,10] is the amount of energy spent by a person sitting quietly. Physical activity was classified into five groups: Sleep, Light activity, Moderate activity, Heavy activity and Sexual activity.
Sleep (MET 0.9): subjects who were sleeping when they sustained SCA.
Light activity (MET 1.0–3.4): included bathing, dressing, cooking, cleaning, feeding, household walking and driving.
Moderate activity (MET 3.5–5.9): included walking for exercise, mowing lawn, gardening, working in the yard, dancing.
Heavy activity (MET score ≥6): included sports such as tennis, running, jogging, treadmill, skiing, biking.
Sexual activity (MET score 1.3): included acts of sexual intercourse. We chose to keep sexual activity as a separate category as this activity involves both physical and emotional components.
Coronary artery disease (CAD) [1]: coronary artery obstruction of >50% diagnosed on angiogram or at autopsy or documentation of myocardial infarction, coronary artery bypass graft, or coronary angioplasty in subjects’ medical records.
2.5. Statistical analysis
SPSS 15.0 for Windows (SPSS Inc., Chicago, Illinois) was used for data analysis. Means with standard deviations were used to represent continuous variables. Proportions were used for categorical variables. Oneway ANOVA and Pearson Chi-Square tests were used to detect differences among activity groups for continuous and categorical variables, respectively. Where required, Bonferroni tests were used for post-hoc analysis. P-values <0.05 were considered statistically significant.
3. Results
The study sample consisted of 1180 subjects, of whom 516 (44%) suffered witnessed SCA and 664 (56%) sustained un-witnessed SCA. Of the 516 subjects, 512 (99%) were adults and 4 (1%) were children.
In adults with witnessed SCA, physical activity information immediately prior to arrest was available in 304 (59%) subjects and analysis was limited to this group of subjects. Of these, 51 (17%) subjects were sleeping, 193 (63%) were performing light activities, 39 (13%) were performing moderate activities, 14 (5%) were performing heavy activities, and 7 (2%) were engaged in sexual activity prior to sustaining sudden cardiac arrest (Fig. 1).
Fig. 1.

Prevalence of the five physical activity groups.
3.1. Age
The mean age of the 304 adult subjects was 69 years. Overall, men with a mean age of 67 years were younger compared to women whose mean age was 71 years ( p-value 0.037). The mean ages of the subjects in the five physical activity groups were: 65 years in those who were sleeping, 72 in the light activity group, 67 in the moderate activity group, 51 in the heavy activity group, and 65 in the sexual activity group. There was a statistically significant difference in the mean ages across these groups (Oneway Anova p-value < 0.001) Table 1. Further analysis using Bonferroni post-hoc tests revealed a statistically significant difference in the mean ages of the subjects engaged in heavy physical activities compared to those who were sleeping and those who were performing light and moderate physical activities ( p 0.02, <0.001 and 0.006, respectively) (Fig. 2).
Table 1.
Distribution of mean age, gender and CAD in 304 adults with witnessed sudden cardiac arrest
| Patient characteristics | Sleep (N=51) | Light activity (N=193) | Moderate activity (N=39) | Heavy activity (N =14) | Sexual activity (N=7) | P-value |
|---|---|---|---|---|---|---|
| Mean age years (SD) | 65 (16) | 72 (14) | 67 (15) | 51 (21) | 65 (10) | <0.001* |
| Gender | 0.036** | |||||
| Men (%) | 34 (67) | 121 (63) | 29 (74) | 13 (93) | 7 (100) | |
| Women (%) | 17 (33) | 72 (37) | 10 (26) | 1 (7) | 0 (0) | |
| Known CAD (%) | 25 (49) | 69 (36) | 11 (28) | 4 (29) | 4 (57) | 0.184** |
Sources for p-value:
Oneway Anova,
Pearson Chi-Square Test.
CAD = Coronary Artery Disease; N = number of study subjects; SD = Standard Deviation.
Fig. 2.

Distribution of age across the five physical activity groups.
3.2. Gender
204 (67%) were men and 100 (33%) were women. There was a statistically significant difference in the distribution of men and women across the five physical activity groups (p=0.04) (Table 1 and Fig. 3).
Fig. 3.
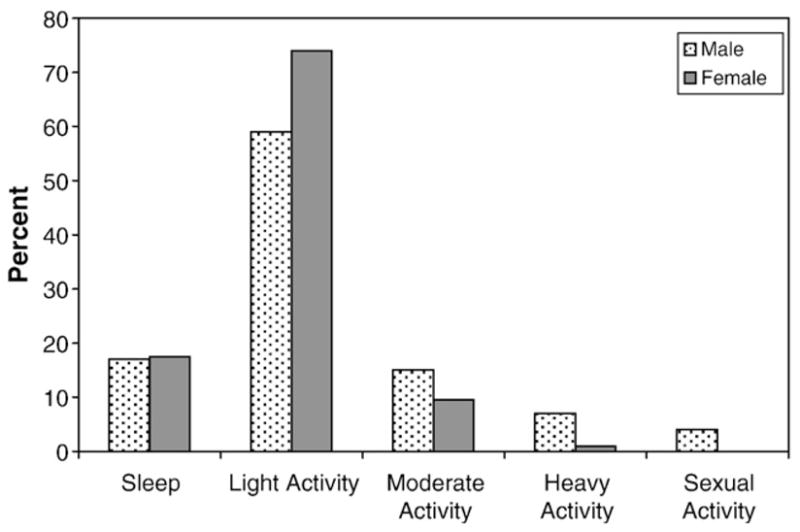
Distribution of physical activity groups by gender.
3.3. CAD
113 (37%) had known CAD. There was no statistically significant difference in the distribution of known CAD across the five physical activity groups (p=0.18), though the individuals in the moderate and heavy activity groups (who were younger) tended to have a lower proportion of known CAD (Table 1).
3.4. Children
Among the four children who sustained witnessed SCA, three were boys aged 1, 11 and 12 years and one was a female infant. The 11 year old boy was running laps at a gym, while the 12 year old boy was learning to ski when he sustained a sudden cardiac arrest.
In the remaining 208 adults who sustained witnessed SCA, physical activity information was not available in their medical records. Nine of these 208 subjects were exposed to a wide range of emotional and behavioral stressors prior to the onset of sudden cardiac arrest. These included: argument; verbal dispute; loss of spouse, child or family member; social isolation secondary to depression; depression secondary to loss of spouse; frequent crying spells; and anxiety attacks. Exposure to emotional and behavioral stressors occurred either immediately prior to the occurrence of SCA or, in some cases, for a prolonged period of time prior to sustaining SCA. Their mean age was 57 years. Of the 9 subjects, 4 were men and 5 were women. Three subjects had known CAD.
4. Discussion
Our community-wide prospective study described the prevalence of different types of physical activity in adults who sustained witnessed sudden cardiac arrest over a 3 year period. Light physical activity (63%) was the most prevalent, followed by sleep (17%), moderate physical activity (13%), heavy physical activity (5%) and sexual activity (2%).
Previous studies [4–6] have examined the relationship of physical activity and sudden cardiac arrest. Thompson et al. [4] reported that Rhode Island men aged 30 to 64 years engaged in jogging had 7 times the risk of having sudden cardiac death relative to those performing non-vigorous activities (95% CI, 4 to 26). Albert et al. [5] found that the male physicians engaged in vigorous physical activity had 16.9 times the risk of having sudden cardiac death, during or up to 30 min following vigorous activity, relative to periods following lighter activity or no activity (95% CI, 10.5 to 27.0; p-value<0.001). Siscovick et al. [6] observed that in men with low levels of habitual activity, the risk of sustaining cardiac arrest during high intensity activity was 56 times the risk of sustaining cardiac arrest at other times (95% CI 23 to 131). This relative risk dropped to 5, among men with the highest levels of habitual activity (95% CI 2 to 14).
However, there has been a lack of community-based analyses regarding physical activity during sudden cardiac arrest. The results of our study are not directly comparable to the findings of Thompson et al. [4], Albert et al. [5] and Siscovick et al. [6] for several reasons. Firstly, ours was a community-based study, which included adult men and women of all ages, whereas Thompson et al., Albert et al. and Siscovick et al. were limited to men of specific age groups (30–64 years, 40–84 years, 25–75 years) only. Secondly, these three studies [4–6] examined the relationship of one particular type of heavy physical activity to sudden cardiac death, whereas our study examined the relationship of a range of physical activities (sleep; light, moderate and heavy activities and sexual activity) to the occurrence of sudden cardiac arrest. Thirdly, the study designs were different. Thompson et al. was a longitudinal study, while Albert et al. was a case-crossover study nested within a large prospective study, and Siscovick et al. was a case-control study. Ours on the other hand was a prospective study which used a cross-sectional analysis.
Other studies [10–14] have also evaluated the relationship of physical activities and acute myocardial infarction. In the MILIS Study [11], about 23% of the study subjects were performing moderate or heavy physical activities prior to experiencing acute myocardial infarction. In the TIMI II Study [14] 19% of the subjects were engaged in moderate or heavy physical activities, while 81% of the subjects were either asleep, resting or were engaged in mild physical activities prior to the occurrence of acute myocardial infarction. The MIOS [10] reported an increased risk for myocardial infarction in the hour following physical activity. This was 5.9 times higher when subjects were engaged in heavy physical activities relative to less vigorous physical activities or no activity (95% CI 4.6–7.7).
Of all the myocardial infarction studies, our results were most consistent with those of TIMI II. Like in the TIMI II Study [14], about 20% of our subjects were engaged in moderate to heavy activities, while 80% were either asleep or were performing light activities at the time of the event. The prevalence of moderate to heavy physical activity in our study (18%) was slightly lower compared to that in the MILIS (23%) [12] study. The proportion of subjects engaged in heavy physical activity prior to sustaining SCA in our study (5%) was similar to the proportion of subjects engaged in heavy activity prior to sustaining acute myocardial infarction in MIOS (4.4%) [10].
Our study has several strengths. To our knowledge this is the first population based community study that analyzed the prevalence of different types of physical activity in subjects who sustained SCA, using a cross-sectional analysis. SCA cases were identified from a large source population of Multnomah County (677,813) that accounts for about one fifth [8] of the population of the state of Oregon, USA.
Also, methods of case ascertainment used an extensive network of available resources in Multnomah County and this minimized the likelihood of otherwise unidentified cases of SCA. The data collection process involved a comprehensive review of subjects’ medical records, autopsy and medical examiner records. This helped reduce misclassification of cases. Having clear definitions for SCA, well defined eligibility criteria and a team of three cardiologists to screen cases also helped reduce misclassification. Lastly, our analysis was appropriately limited to subjects with witnessed SCA and known physical activity information. This enabled us to perform a more scientific evaluation of the physical activities prior to the occurrence of SCA.
Potential limitations of this study include a lack of adequate description of physical activities immediately prior to the event in 41% of adults who experienced witnessed SCA. However, this is consistent with the dynamic and catastrophic nature of the event. As a result, obtaining precise physical activity information prior to SCA is a challenge. There were no statistically significant differences in the distribution of mean age and CAD in adult subjects with and without physical activity information as shown in Table 2, but gender proportions were different. We believe that information may have been missing at random and therefore, is unlikely to have resulted in a significant bias.
Table 2.
Distribution of mean age, gender and CAD in 512 adults with witnessed sudden cardiac arrest
| Patient characteristics | Subjects with known physical activity information N = 304 | Subjects without known physical activity information N = 208 | P-value |
|---|---|---|---|
| Mean age years (SD) | 69 (15) | 68 (15) | 0.82* |
| Gender | 0.01** | ||
| Men (%) | 204 (67) | 116 (56) | |
| Women (%) | 100 (33) | 92 (44) | |
| Known CAD (%) | 113 (37) | 75 (36) | 0.80** |
Sources for p-value:
t-test,
Pearson Chi-Square Test.
CAD = Coronary Artery Disease; N = number of study subjects; SD = Standard Deviation.
5. Conclusions
In this community-based study, only 5% of SCA victims were performing vigorous physical activity immediately prior to the fatal event. The vast majority (80%) of the adult subjects that suffered sudden cardiac arrest were performing light physical activity or was asleep at the time of the event. The potential role of emotional or behavioral stressors as well as sleep-related disorders, which this study was not designed to evaluate, warrants further assessment.
Acknowledgments
The authors are grateful to the first responders (American Medical Response, Portland and Gresham fire departments) and health care providers of the Portland, Oregon metropolitan area, without whom this study would not have been possible.
Footnotes
Funded, in part, by R01HL088416 (SSC) and The Donald W. Reynolds Clinical Cardiovascular Research Center Grant to Johns Hopkins University (SSC).
References
- 1.Chugh SS, Jui J, Gunson K, Stecker EC, John BT. Current burden of sudden cardiac death: multiple source surveillance versus retrospective death certificate-based review in a large U.S. Community J Am Coll Cardiol. 2004;44:1268–75. doi: 10.1016/j.jacc.2004.06.029. [DOI] [PubMed] [Google Scholar]
- 2.Muller D, Agarwal R, Arntz HR. How sudden is sudden cardiac death? Circulation. 2006;114:1146–50. doi: 10.1161/CIRCULATIONAHA.106.616318. [DOI] [PubMed] [Google Scholar]
- 3.Willich SN, Maclure M, Mittleman M, Arntz HR, Muller JE. Sudden cardiac death: support for a role of triggering in causation. Circulation. 1993;87:1442–50. doi: 10.1161/01.cir.87.5.1442. [DOI] [PubMed] [Google Scholar]
- 4.Thompson PD, Funk EJ, Carleton RA, Sturner WQ. Incidence of death during jogging in Rhode Island from 1975 through 1980. JAMA. 1982;247:2535–8. [PubMed] [Google Scholar]
- 5.Albert CM, Mittleman M, Chae CU, Lee IM, Hennekens CH. Triggering of sudden death from cardiac causes by vigorous exertion. N Engl J Med. 2000;343:1355–61. doi: 10.1056/NEJM200011093431902. [DOI] [PubMed] [Google Scholar]
- 6.Siscovick DS, Weiss NS, Fletcher RH, Lasky T. The incidence of primary cardiac arrest during vigorous exercise. N Engl J Med. 1984;311:874–7. doi: 10.1056/NEJM198410043111402. [DOI] [PubMed] [Google Scholar]
- 7.Eliot RS, Buell JC. Role of emotions and stress in the genesis of sudden death. J Am Coll Cardiol. 1985;5:95B–8B. doi: 10.1016/s0735-1097(85)80535-0. [DOI] [PubMed] [Google Scholar]
- 8.http://www.placenames.com/us/41051/facts/.
- 9.Ainsworth BE, Haskell WL, Whitt MC. Compendium of physical activities: an update of activity codes and MET intensities. Med Sci Sports Exerc. 2000;32(Suppl):S498–516. doi: 10.1097/00005768-200009001-00009. [DOI] [PubMed] [Google Scholar]
- 10.Mittleman M, Maclure M, Tofler GF. Triggering of acute myocardial infarction by heavy physical exertion (MIOS) N Engl J Med. 1993;329:1677–83. doi: 10.1056/NEJM199312023292301. [DOI] [PubMed] [Google Scholar]
- 11.Culic Viktor, Eterovic D, Miric Dinko. Meta-analysis of possible external triggers of acute myocardial infarction. Int J Cardiol. 2005;99:1–8. doi: 10.1016/j.ijcard.2004.01.008. [DOI] [PubMed] [Google Scholar]
- 12.Tofler GF, Stone PH, Maclure M. Analysis of possible triggers of acute myocardial infarction (The MILIS Study) Am J Cardiol. 1990;66:22–7. doi: 10.1016/0002-9149(90)90729-k. [DOI] [PubMed] [Google Scholar]
- 13.Servoss SJ, Januzzi JL, Muller JE. Triggers of acute coronary syndromes. Prog Cardiovasc Dis. 2002;44:369–80. doi: 10.1053/pcad.2002.123470. [DOI] [PubMed] [Google Scholar]
- 14.Tofler GH, Muller JE, Stone PH. Modifiers of timing and possible triggers of acute myocardial infarction in the Thrombolysis in Myocardial Infarction phase II (TIMI II) Study Group. Am Coll Cardiol. 1992;20:1049–55. doi: 10.1016/0735-1097(92)90356-r. [DOI] [PubMed] [Google Scholar]