

Abstract
We report an unusual case of strangulated diaphragmatic (Morgagni) hernia resulting in ischaemia of the small and large bowel, which was initially diagnosed as a pneumonia. This case highlights the importance of being aware of this rare, but potentially fatal condition when assessing patients with respiratory symptoms and abdominal pain.
Keywords: Morgagni hernia, Diaphragmatic hernia, Strangulation
A 40-year-old man was admitted with a 1-day history of sudden onset of left-sided chest pain radiating down to his left abdomen. The pain was constant in nature and he denied any previous episodes. He described one episode of vomiting but his bowel habit was normal and, in particular, he denied any episodes of rectal bleeding or diarrhoea. On functional enquiry, he described episodes of exertional dyspnoea which was new in onset. There was no past medical history of note, nor had he had recent trauma or surgery.
On examination, he looked unwell and dyspnoeic. He was apyrexial and haemodynamically stable. Examination of the respiratory system revealed decreased air entry in the left lung base. He was noted to have a soft abdomen with some tenderness in the epigastrium. An ECG was normal. Initial laboratory investigations revealed a white cell count of 13.9. Arterial blood gases on air revealed a pO2 of 9.01 and mildly raised lactate of 2.73. Initial chest radiography confirmed left lower lobe consolidation. Pleural tap and septic screen were sent.
Eight hours after admission, the patient became progressively more tachycardic and complained of increasing abdominal pain. A surgical review was requested and this revealed tenderness in the LUQ. It was still felt that his abdominal signs were secondary to a primary chest infection. However, as his pain was disproportionate to his abdominal signs, a CT scan was arranged to exclude further pathology. This revealed evidence of herniation of small bowel loops through a left-sided anterior diaphragmatic hernia. A fluid collection was seen at the superior aspect of the hernia with collapse of the underlying lung and shift of the mediastinum to the right (Fig. 1).
Figure 1.
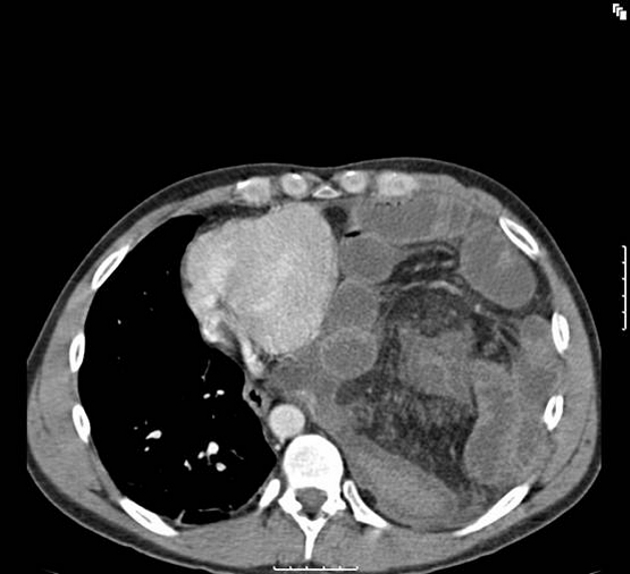
CT scan showing anterior left diaphragmatic hernia with small and large bowel contents in the left hemithorax.
Twelve hours after admission, the patient was taken to theatre. Initial laparoscopy revealed a strangulated 3-cm left diaphragmatic hernia containing small bowel and transverse colon. The contents of the hernia were difficult to reduce laparoscopically; therefore, an emergency laparotomy was performed. Resection of 40 cm of small bowel was undertaken with a side-to-side stapled anastomosis. The transverse colon and splenic flexure were also ischaemic. This was resected and a double-barrel stoma fashioned in the LIF consisting of transverse and sigmoid colon. There was a degree of mid-gut malrotation with a mobile caecum situated in the left iliac fossa. Therefore, a routine appendicectomy was also performed. Copious peritoneal and left hemithorax lavage was undertaken using 6 l of saline. The diaphragmatic defect was closed using 1/0 Prolene with interrupted vertical mattress sutures. Prior to closure, a 32-F chest drain was inserted in the left intercostal space, in the axillary line.
The patient was transferred to the intensive care unit for further management. He made an uneventful recovery.
Discussion
Diaphragmatic hernias of Morgagni were first described in 1769 as anatomical defects in the anterior diaphragm that allow herniation of abdominal viscera into the thorax. They are the rarest of congenital diaphragmatic hernias, making up 2–3% of cases.1 They usually present in childhood with respiratory symptomatology.2 Incidental findings of this condition in adults are less common with only 81 asymptomatic cases reported in a recent review.2 Symptomatic adult cases of Morgagni hernias are even rarer with only 12 cases described.2 Very few present with chest symptoms, the majority describing abdominal pain due to strangulation of the viscera. Of the symptomatic adult cases, the herniated viscera involve omentum, small bowel or stomach.2 To our knowledge, this is the first described adult case presenting with initial respiratory symptoms that has such extensive small and large bowel necrosis.
The pathophysiology of diaphragmatic hernias is not clear. Patients reported to have previous normal radiographs suggest that these hernias may be acquired through a congenital defect in the diaphragm.3 The sequence of events is probably herniation of abdominal viscera through a pre-existing diaphragmatic defect. It can occur on either side of the sternum through a muscle-free triangular space of Larrey, although it is more common on the right.2 Our case is unusual as the defect was on the left side.
Most hernias of Morgagni are diagnosed late because patients can be asymptomatic or present with vague gastrointestinal and respiratory symptoms and signs.4 The clinical presentation of this patient was clearly misleading with his pulmonary symptoms delaying a diagnosis. It is important to bear in mind that patients who do have features of pneumonia on assessment should always have a thorough abdominal examination and, if necessary, radiological evaluation to exclude this potentially life-threatening condition. Ultrasonography has been shown to be useful in assessing diaphragmatic hernias but CT is the most sensitive as it gives excellent anatomical detail on the contents of the hernia and its complications such as strangulation.4
Once diagnosed, the requirement for surgery is largely dependent upon the presentation.2 Repair avoids further complications but it is the timing which is important. Emergency intervention is not always necessary unless there is evidence of strangulation.2,3 In these circumstances, it is often better to delineate the anatomy with radiology before proceeding to surgery.
Recently, there has been a trend towards laparoscopy which is useful particularly when the diagnosis is unclear. It provides the benefit of an excellent view, minimal tissue trauma with subsequently faster recovery and superior cosmesis.5 Laparotomy, however, is still the most common approach for repair.2,3 Although laparoscopy was initially used in our case, early conversion to a laparotomy was undertaken as there was evidence of necrotic small and large bowel which was difficult to reduce.
Conclusions
This case represents the first report in the English literature of left-sided adult Morgagni hernia with an unusual presentation and significant bowel necrosis. It highlights the difficulties in diagnosis, prompting a need for a high index of suspicion when assessing patients with respiratory distress and with symptoms suggestive of gastrointestinal obstruction. A missed diagnosis can lead to life-threatening complications such as obstruction or strangulation which warrants early surgical intervention. Although laparoscopy is suitable for certain cases, signs of respiratory distress and bowel obstruction constitute a surgical emergency and an indication for laparotomy.
References
- 1.Comer TP, Clagett OT. Surgical treatment of hernia of the foramen of Morgagni. J Thorac Cardiovasc Surg. 1966;52:461–8. [PubMed] [Google Scholar]
- 2.Loong TP, Kocher HM. Clinical presentation and operative repair of hernia of Morgagni. Postgrad Med J. 2005;81:41–4. doi: 10.1136/pgmj.2004.022996. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Eren S, Ciri F. Diaphragmatic hernia: diagnostic approaches with review of the literature. Eur J Radiol. 2005;54:448–59. doi: 10.1016/j.ejrad.2004.09.008. [DOI] [PubMed] [Google Scholar]
- 4.Lin ST, Moss DM, Henderson SO. A case of Morgagni hernia presenting as pneumonia. J Emerg Med. 1997;15:297–301. doi: 10.1016/s0736-4679(97)00011-5. [DOI] [PubMed] [Google Scholar]
- 5.Contini S, Dalla Valle R, Bonati L, Zinicola R. Laparoscopic repair of a Morgagni hernia: report of a case and review of the literature. J Laparoendosc Adv Surg Tech. 1999;9:93–9. doi: 10.1089/lap.1999.9.93. [DOI] [PubMed] [Google Scholar]