

Abstract
Youth who initiate sexual intercourse in early adolescence (age 11–14) experience multiple risks, including concurrent adjustment problems and unsafe sexual practices, The current study tested two models describing the links between childhood precursors, early adolescent risk factors, and adolescent sexual activity: a cumulative model and a meditational model, A longitudinal sample of 694 boys and girls from four geographical locations was utilized, with data collected from kindergarten through high school. Structural equation models revealed that, irrespective of gender or race, high rates of aggressive disruptive behaviors and attention problems at school entry increased risk for a constellation of problem behaviors in middle school (school maladjustment, antisocial activity, and substance use) which, in turn, promoted the early initiation of sexual activity. Implications are discussed for developmental models of early sexual activity and for prevention programming.
Keywords: Risky sexual activity, Externalizing behaviors, Early adolescent problems
The initiation of sexual activity is a major milestone for many adolescents on the road to adulthood. Whereas only 13–15% of American teens report having sexual intercourse before turning 15, the rate climbs steeply after that. Forty-five percent report having sex before turning 17, and approximately 70% have had sex by the time they reach age 19 (Guttmacher Institute 2006; Leitenberg and Saltzman 2000). Early initiation of sexual intercourse (i.e., occurring during preadolescence or very early in adolescence) is associated with a variety of concurrent risk factors for both boys and girls, including school maladjustment and substance use (Kotchick et al. 2001; Martin et al, 2005). In addition, girls who initiate intercourse early are at higher risk for unintended pregnancy and sexually transmitted diseases compared with girls who delay intercourse until late adolescence (Crockett et al, 1996; Leitenberg and Saltzman 2000).
These statistics point towards a clinical and societal need to explore the predictors of early sexual activity, in order to better inform preventive interventions. Although a significant body of research has documented the concurrent risky behaviors that characterize sexually active teenagers in cross-sectional samples, very few studies have examined childhood precursors of early sexual activity. The present study utilized a sample of 694 boys and girls from four geographical locations, with an oversampling of youth with high rates of externalizing behavior problems at school entry. Youth were followed from kindergarten through high school. A central aim of the current study was to compare two competing theoretical models of developmental processes implicated in early sexual activity: (1) a cumulative model of risk over time, and (2) a mediational model based on problem behavior theory (Jessor 1991) which suggests that high rates of externalizing problems in early childhood increase risk for a constellation of problem behaviors in early adolescence (school maladjustment, antisocial activity, and substance use) which, in turn, promote the early initiation of sexual activity.
Externalizing Behavior Problems in Childhood
A basic, though not well-tested, tenet of problem behavior theory is that some children enter adolescence with a history of socialization difficulties that predispose them to take an alienated stance toward adult authority and conventions (Udry et al. 1995; Willoughby et al. 2004). Based upon this general undersocialized and rebellious orientation, these at-risk youth initiate a range of rule-breaking behaviors as they achieve greater autonomy in early adolescence, including substance use, antisocial behaviors, and sexual activity {Boles et al. 2006; Willoughby et al. 2004; Zweig et al. 2001). There is substantial longitudinal evidence that childhood aggressive–disruptive behaviors exhibited at school entry predict elevated risk for antisocial behavior later in adolescence (Fergusson et al. 2005). Longitudinal studies have also demonstrated that a childhood history of aggressive–disruptive behaviors is associated with early initiation of intercourse and elevated rates of adolescent sexual activity among boys (Barkley et al. 2006; Moffitt 1993; Ramrakha et al. 2007), and early initiation of intercourse, multiple sex partners, and increased rate of teen pregnancies among girls (Ramrakha et al. 2007; Woodward and Ferguson 1999). One prospective study found that girls who were described as “domineering” when they were 9 years old were likely to initiate intercourse at a younger age (Udry et al. 1995), suggesting that aggressive and domineering behavior may directly predict early sexual activity.
Childhood conduct problems may also increase risk for early sexual activity due to co-occurring impulsivity and attention problems, which are frequently associated with aggression and reflect deficits in inhibitory control, planning, and decision-making skills. Prior research has linked childhood inattention with adolescent risk behaviors, including smoking (Nadeau et al. 1999) and substance use (Biederman et al. 1999). In one prospective study, impulsivity assessed at age 3 predicted age of first romantic relationship and alcohol use at age 16, which in turn led to a greater accumulation of sexual partners by age 19 (Zimmer-Gembeck et al. 2004). Similarly, Crockett et al. (2006) found that low levels of self-regulation at age 8–9 predicted risky sexual activity at age 16–17, including early sexual debut, multiple partners, and sex without condoms. Overall, research suggests that early inattention and impulsivity may increase involvement in rule-breaking behaviors directly, as well as through their association with childhood conduct problems.
Three longitudinal studies have examined the relative roles of early inattention/hyperactivity and conduct problems in predicting risky sexual activity. In one (Ramrakha et al. 2007) childhood conduct problems were the primary predictor of early sexual debut, and hyperactivity ratings did not contribute to this prediction after conduct problems were controlled. Similarly, in another longitudinal study, youth diagnosed as hyperactive in childhood engaged in more risky sexual activity (e.g., earlier initiation of sexual activity, significantly higher rates of sexually transmitted disease) than non-hyperactive youth, but co-occurring conduct disorder emerged as the primary predictor of early sexual debut (Barkley et al. 2006). In contrast to these two studies, Flory et al. (2006) found that childhood attention problems and conduct problems made independent predictions, each increasing the likelihood that boys would participate in risky sexual behaviors and experience early parenthood.
It is well established that early aggressive–disruptive behaviors and attention problems often occur concurrently, and that children with these combined problems are at particular risk for academic and social difficulties in elementary school. This may set them up for school maladjustment and deviant peer involvement during adolescence, thus increasing the likelihood of peer-facilitated rule-breaking activities during that time period (Moffitt 1993). It is less certain from existing research whether these two early behavioral risks function jointly to increase risk or whether they make independent contributions towards predicting early sexual activity.
Early Adolescent Risk Behaviors
Many children who show high rates of externalizing behavior problems and attention problems at school entry continue to experience conflict with parents, teachers, and peers throughout their elementary years (Moffitt 1993), As these youth make the transition into middle or junior high school, they typically experience a reduced level of monitoring by teachers and parents, along with increased mobility and unsupervised free time (Dishion et al. 1997). Early adolescents who are bonded to school—that is, academically engaged, connected to peers and teachers, and engaged in extracurricular activities—are at reduced risk for early sexual activity (Kotchick et al. 2001; Resnick et al. 1997). In contrast, youth who are alienated from school are at heightened risk, perhaps due to the reduced social control of adult authorities or mainstream peers. As alienated youth gather with other similarly disaffected youth in unstructured and unsupervised settings, they experience increased opportunity (and often peer encouragement) for rule-breaking and norm-breaking behaviors, including substance use, antisocial behavior, and early sexual activity (Bearman and Bruckner 2001).
Extensive research suggests that early sexual activity typically occurs in the context of other risky adolescent behaviors (Elliot and Morse 1987), For example, cross-sectional studies of early adolescents reveal strong associations between sexual activity and delinquent behavior among boys (Bingham and Crockett 1996; Farrell et al. 1992) and status offences among girls, such as school truancy and running away from home (Lanctot and Smith 2001), In addition, smoking and the early use of alcohol and other substances often accompany sexual activity in early adolescence (Lanctot and Smith 2001; Whitbeck et al. 1999).
Possible Developmental Pathways: Cumulative or Mediated
Despite the valuable contributions of a number of longitudinal studies, the developmental pathways linking childhood problems (aggression, inattention) and early adolescent risk (school maladjustment, antisocial activity, substance use) to early adolescent sexual activity are not well understood. These developmental effects may be cumulative. That is, childhood inattention and impulsivity may impair decision-making skills while aggressive–disruptive behaviors fuel oppositional and domineering behaviors that contribute directly to early sexual activity. Early adolescent behaviors may make additional contributions to risk, by providing the opportunity and peer support for early sexual activity. Alternatively, the developmental pathway may be mediated, in that early aggressive–disruptive behaviors and attention problems may contribute to early sexual activity primarily by undermining positive socialization experiences and increasing risk for an adolescent lifestyle that fosters and supports a range of risky behaviors (Broidy et al. 2003; Miller-Johnson et al. 2004; Moffitt 1993). In this latter model, the link between childhood problems and early sexual activity is mediated by early adolescent school maladjustment, antisocial activity, and substance use.
Gender and Race Effects
The base rates of some of the risk factors associated with early sexual activity vary as a function of gender and race, but the extent to which developmental processes vary as a function of gender and race is largely unknown (Zweig et al. 2001). With regard to gender, girls are less likely than boys to show high rates of overt aggression in early childhood (Silverthom and Frick 1999). However, gender differences are much less pronounced on other types of early-starting behavior problems, such as oppositional-defiant behavior and attention problems (Bierman et al. 2004). With regard to race, prior studies have documented earlier ages of initiation of sexual activity among African American girls compared with European-American girls (Doljanac and Zimmerman 1998; Miller et al. 1997). Some have argued that adjustment problems are more indicative of risk when they are relatively rare in a population (Silverthom and Frick 1999), suggesting that early aggression and the early initiation of sexual activity may be more problematic for European American girls than for African American girls or European American boys. Certainly, the exploration of possible gender and race differences in the predictability of early sexual activity is warranted.
The Present Study
The present study examined childhood and early adolescent precursors of early sexual activity in a multisite, longitudinal sample of 694 boys and girls. Aggressive behaviors and attention problems were assessed when children were in kindergarten and first grade (age 5–7). School maladjustment, antisocial activity, smoking, alcohol and drug use were assessed when youth were in middle school (age 12–13). Outcomes included age of initiation of sexual intercourse, and the number of years of sexual activity reported during adolescence (through grade 11, age 17). This study offered a unique opportunity to examine both early childhood and early adolescent predictors of adolescent sexual activity, and to explore potential moderation of developmental processes by gender and race. It also enabled the comparison of a cumulative model of prediction with a mediational model informed by problem behavior theory (Jessor 1991), in which the impact of childhood problems on early adolescent sexual activity is mediated by early adolescent risky behaviors.
Materials and Methods
Participants
Participants were drawn from the Fast Track multisite investigation of the development and prevention of conduct problems (CPPRG 1992). This study included youth from the high-risk control and normative subsamples to obtain an over-sampling of children with disruptive behavior problems at school entry, thus enabling the study of gender and race differences in the pattern and predictability of those problems. Youth who received preventive intervention services as part of Fast Track were not included.
High-risk youth were identified using a multiple-gating screening procedure that combined teacher and parent ratings of aggressive–disruptive behavior. Initially, 55 schools serving poor neighborhoods at four sites were identified (Durham, NC; Nashville, TN; Seattle, WA; and rural central Pennsylvania). Over three successive years, teachers at these schools completed the Teacher Observation of Child Adaptation—Revised (TOCA-R) Authority Acceptance scale (Werthamer-Larsson et al. 1991) on all 9,594 children attending kindergarten. Those children scoring in the top 40% within cohort and site were then solicited for the next stage of screening of home behavior problems. Ninety-one percent (N=3,274) of parents participated in this screening, which utilized 24 items from the Child Behavior Checklist (CBCL; Achenbach 1991a) and similar scales. The teacher and parent screening scores were summed to yield a total severity-of-risk screen score. Children were selected for inclusion into the high-risk sample based on this screen score, moving from the highest score downward until desired sample sizes were reached within sites, cohorts, and conditions. Average child t scores on the externalizing scales of the kindergarten Teacher’s Report Form (TRF; Achenbach 1991b) and the parent-reported CBCL (Achenbach 1991a) were 66.31 and 61.34, respectively. The normative sample was randomly selected to represent the range of problem behaviors in each school in the control condition on the kindergarten TOCA-R.
The final sample for this study included 694 youth (42% female; 47% African American; 53% European American), including 281 youth from the normative sample (40%) and 413 from the high-risk sample (60%). Youth who were of other races (e.g., not African American or European American) were excluded from analyses, due to the very small number in the sample (n=30). Youth who reported that their first experience of intercourse was coerced or forced were also excluded from this study (n=30). The mean age of children at the start of the study (end of their kindergarten year) was 6.40 years (SD=0.47). On average, children were 13.42 in the summer when their early adolescent interviews were conducted. The early adolescent interviews always occurred in year 8 of the study, which followed the completion of 7th grade for students progressing on time, and the completion of 6th grade for students who experienced grade retention between the kindergarten and early adolescent interviews. Approximately 36% of the participating youth were from families in the lowest category of socioeconomic status (SES) according to the Hollingshead index (Hollingshead, 1975), and 28% were from families in the next to lowest category.
Procedures
All procedures followed APA guidelines for the ethical conduct of research and were approved by the institutional review boards at each of the four sites. Youth self-report and parent ratings were obtained during face-to-face home interviews that occurred annually each summer; informed consent and assent were obtained at the time of each assessment. Two interviewers visited the home; one interviewed the primary caregiver (usually the mother) and the other one interviewed the youth. The interviewer read through all questionnaires, and recorded the caregiver’s response. Computer-assisted interviews were conducted with the youth, to increase their sense of privacy and confidentiality. Youth wore headphones and listened to items being read to them on a laptop computer, and answered directly to the computer. To collect teacher ratings, an interviewer visited the school to explain the measures to teachers, and teachers then completed the measures and returned them to the project. Parents, youth, and teachers were all compensated financially for their participation.
Measures
Childhood aggressive–disruptive behaviors and attention problems at school entry were assessed with kindergarten and first-grade teacher ratings. Early adolescent adjustment was assessed when youth were in 7th grade, using self-reports (for antisocial behavior and substance use), teacher ratings (for school maladjustment and antisocial behavior) and parent reports (for school maladjustment). Youth reported on their sexual activity during annual interviews (from 7th through 11th grades).
Childhood aggressive–disruptive behavior
Kindergarten teachers completed the TRF (Achenbach 1991b) and first-grade teachers completed the TOCA-R (Werthamer-Larsson et al. 1991). The TRF Aggressive Behavior scale, used in kindergarten, included 19 aggressive, disruptive, and antisocial behavior problems (e.g., argues, fights, stubborn, disobedient), each rated on a three-point scale (from 0 = “Not true” to 2 = “Very true or often true”; α=0.97 in this sample). The Authority Acceptance scale of the TOCA-R, used in first grade, included 10 items describing disobedient and aggressive behavior problems (e.g., yells at others, fights, breaks rules), each rated on a six-point scale (from 0 = almost never to 5=almost always, α =0.94 in this sample). Higher scores on the TRF and TOCA-R indicated higher levels of problem behavior. Kindergarten and first-grade teacher ratings were significantly correlated, r=0.48, p< 0.001, and represented the latent construct of early aggressive–disruptive behaviors.
Childhood attention problems
Attention problems were assessed with the Attention Problems scale of the TRF in kindergarten, which included 9 items (e.g., cannot concentrate, hyperactive, confused, impulsive), each rated on a three-point scale (α=0.96 in this sample). Attention problems also were assessed with the Cognitive Concentration scale of the TOCA-R in first grade, which included 12 items (e.g., works hard, easily distracted, concentrates, pays attention), each rated on a six-point scale (α=0.97 in this sample). These kindergarten and first-grade teacher ratings were significantly correlated, r=0.45, p<0.001, and were used to represent the latent construct of early attention problems.
Early adolescent school maladjustment
Teachers and parents provided ratings reflecting youth school maladjustment. Guidance counselors were asked to distribute the Teacher Rating of Student Adjustment (CPPRG 1995) to at least three teachers who knew each youth well. This measure asked teachers to rate the student’s skills in the six domains of academic performance, academic motivation, social skills, adult relationships, conduct, and personal maturity, using a five-point scale (from 1=poor, unsatisfactory skills to 5=excellent skills), and a total score was computed (α=0.91 in this sample). Items were reverse coded when necessary, such that higher scores on this measure indicated higher levels of school maladjustment and poorer functioning. Two or more ratings were available for most youth (86%) and were averaged; a single teacher rating was used for the remaining youth. The intraclass correlations for individual items across teachers rating the same youth ranged from 0.60 (conduct) to 0.39 (relationships with adults); highly significant differences between high-risk and normative sample youth on all items provided evidence of discriminant validity.
Parents also reported on their child’s school adjustment, using the School Adjustment—Parent Report (CPPRG 1997), a 16-item measure created for the Fast Track Project. Items were rated on a five-point scale (1=strongly disagree to 5=strongly agree) and included parent perceptions of student academic performance, social adjustment, and general school adjustment (e.g., “My child had a good year at school,” “My child stayed out of trouble with teachers and the staff at school,” “My child got along well with other kids at school this year”). A total score was used to represent school maladjustment (α=0.91 in this sample). As with the teacher reports, some items were reverse coded, and higher scores indicated higher levels of school maladjustment. Teacher and parent reports were significantly correlated, r=0.60, p<0.001, and were used to represent the latent construct of early adolescent school maladjustment.
Early adolescent antisocial behavior
Teacher ratings and youth self-reports were used to assess antisocial behavior when youth were in 7th grade (12–13 years old). Guidance counselors identified a core teacher who knew each youth well enough to complete the TRF (Achenbach 1991b). The Delinquent Behavior scale was used to represent antisocial behavior, and included 9 items (e.g., lying or cheating, steals, swearing or obscene language, truancy), each rated on a three-point scale (α=0.83 in this sample). Higher scores indicated higher levels of antisocial behavior.
Youth completed the 13-item Self-Report of Delinquency (drawn from the National Youth Survey, Huizinga and Elliot 1986). This instrument yields a sum score, reflecting the number of serious index offenses committed in the past year, including 13 items (e.g., “stolen an item greater than $100 in value,” “sold heroin or LSD,” and “attacked someone with intent to hurt”). Higher scores indicated higher levels of antisocial behavior. Although scores ranged from 0 to 13, they tended to be skewed, as many youth reported low levels of these relatively severe antisocial behaviors (α=0.75 in this sample). Teacher ratings and youth self-reports were significantly, but only moderately, correlated, r=0.29, p<0.001, and were used to represent the latent construct of early adolescent antisocial behavior.
Early adolescent substance use
Youth self-reports of tobacco use and alcohol/drug use were collected, using questions from the National Longitudinal Study of Adolescent Health (Add Health, Resnick et al. 1997). For tobacco use, youth received a score of 1 if they indicated they had used any tobacco product (cigarettes, chewing tobacco, snuff) in the past year, and a 0 if they had not. For alcohol and drug use, youth received a score of 1 if they reported drinking alcohol (beer, wine, wine coolers or liquor) or using any illegal drug (marijuana, cocaine, crack, inhalants, heroin, LSD, PCP, ecstasy, mushrooms, speed, or pills not prescribed by a physician) during the past year. Youth self-reports of tobacco and alcohol/drug use were significantly correlated, tetrachoric r=0.73, p<0.001. These two measures were used to represent the latent construct of early adolescent substance use.
Adolescent sexual activity
Information regarding sexual activity was gathered using a 41-item self-report questionnaire drawn from Add Health (Bearman et al. 1997), which was administered every year between 7th and 11th grades. To create the first indicator of early sexual activity, youth were stratified into three groups according to their reported age at first vaginal intercourse: very early initiation (age 14 and under for girls, age 13 and under for boys; score=3, n= 204, 35.79%), early initiation (ages 15–16 for girls, 14–16 for boys; score=2, n=173, 30.35%), and normative initiation (age 17 or older for girls and boys; score=1, n= 193, 33.86%.). This type of stratification is standard in this area of research, because it reduces the impact of outliers at either end of the distribution, and anchors age of sexual initiation around established national norms (Crockett et al. 1996; Phinney and Jensen 1990). For the second indicator, we calculated the percentage of interviews, held across five years in adolescence, in which a youth reported being sexually active (i.e., had engaged in vaginal intercourse). Age at first intercourse and the percentage of years in which a youth reported being sexually active were significantly correlated, r=0.72, p< 0.001, and were used to represent the latent construct of adolescent sexual activity.
Results
Data analyses for this study proceeded in three stages. First, correlations were computed to examine associations between individual measures of behavior problems at school entry, early adolescent adjustment, and adolescent sexual activity. Second, a measurement model was estimated to determine whether observed measures served as satisfactory indicators of latent constructs, to examine bivariate relations among latent constructs, and to test measurement invariance across gender and race. Third, a series of structural equations models were estimated to determine whether empirical evidence was more consistent with developmental models of cumulative effects or mediation.
Most analyses in this study were performed using the AMOS program of SPSS. This software allowed maximum likelihood estimation of individual parameters and model fit statistics based on every youth in the sample, even if the youth was missing data on some of the follow-up measures. All together, we had data for 88% of the original sample (n=610) at the early adolescent assessment, when most youth were in 7th grade, and we had data for 86% of the original sample (n=599), for our assessment of adolescent sexual activity, when most youth were between 7th and 11th grades. Attrition was not significantly related to youth gender, race, initial behavior problems, or SES.
Descriptive Analyses
Descriptive statistics for all measures included in this study are presented in Table 1. Pearson correlations were computed to determine the degree to which the kindergarten and first-grade teacher ratings of aggressive–disruptive behaviors and attention problems predicted early adolescent adjustment problems (e.g., school maladjustment, antisocial behavior, and substance use). As shown in Table 2, early aggressive–disruptive behavior and attention problems were significantly predictive of teacher- and parent-rated school maladjustment and teacher-rated antisocial behavior, and moderate in value according to Cohen’s (1988) criteria. Statistically significant correlations also emerged with self-reported antisocial behavior, but were small in magnitude. Childhood behavior problems showed relatively small correlations with self-reported substance use.
Table 1.
Descriptive Statistics for All Variables
| Measures | Number | Mean | Standard deviation | Minimum | Maximum |
|---|---|---|---|---|---|
| Childhood problems | |||||
| Aggression—K teacher | 599 | 15.19 | 13.06 | 0 | 49 |
| Aggression—Gr. I teacher | 671 | 1.27 | 1.15 | 0 | 5 |
| Inattention—K teacher | 599 | 13.70 | 10.47 | 0 | 38 |
| Inattention—Gr. I teacher | 671 | 2.11 | 1.23 | 0 | 5 |
| Early adolescent risks | |||||
| School maladjustment—teacher | 577 | 2.10 | 0.89 | 0 | 4 |
| School maladjustment—parent | 565 | 1.63 | 0.75 | 0 | 3.63 |
| Antisocial behavior—self | 564 | 0.02 | 0.07 | 0 | 0.77 |
| Antisocial behavior—teacher | 549 | 15.71 | 15.27 | 0 | 66 |
| Tobacco use—self | 566 | 42% | NA | 0 | 1 |
| Alcohol/drug use—self | 566 | 30% | NA | 0 | 1 |
| Early sexual activity | |||||
| Very early initiation—self | 204 | 36% | NA | ||
| Early initiation—self | 173 | 30% | NA | ||
| Normative initiation—self | 193 | 34% | NA | ||
| % Years sexually active—self | 598 | 31% | 0.33 | 0 | 1 |
The percentage scores represent the portion of the sample reporting substance use, the proportion of the sample reporting very early, early, or normative initiation of sexual activity, and the % of years each youth reported sexual activity from 7th to 11th grade. K Kindergarten, Gr. 1 grade 1
Table 2.
Correlations among Childhood Problems and Early Adolescent Adjustment
| Early adolescent adjustment | Aggressive–disruptive |
Attention problems |
||
|---|---|---|---|---|
| Kindergarten | Grade 1 | Kindergarten | Grade 1 | |
| School maladjustment | ||||
| Teacher ratings | 0.39*** | 0.39*** | 0.42*** | 0.46** |
| Parent ratings | 0.36*** | 0.32*** | 0.32*** | 0.34*** |
| Antisocial behavior | ||||
| Self-report | 0.12** | 0.14** | 0.09* | 0.06 |
| Teacher ratings | 0.42*** | 0.45*** | 0.30*** | 0.35*** |
| Substance use | ||||
| Self-report of tobacco | 0.12** | 0.07 | 0.10* | 0.09* |
| Self-report of alcohol/drugs | 0.12** | 0.09* | 0.10* | 0.07 |
p<0.05,
p<0.01,
p<0.001.
Next, correlations were computed to determine the degree to which childhood aggressive–disruptive behaviors and attention problems and early adolescent risky behaviors predicted early sexual activity (e.g., age of first intercourse and the percent of years of adolescent sexual activity). As shown in Table 3, all individual childhood and early adolescent measures were significantly correlated with early sexual activity.
Table 3.
Correlations between Childhood Problems, Early Adolescent Adjustment, and Early Sexual Activity
| Childhood and early adolescent adjustment | Early sexual activity |
|
|---|---|---|
| Age of first intercourse | Years of adolescent sexual activity | |
| Childhood behavior problems | ||
| Aggression—Kindergarten | 0.30* | 0.22* |
| Aggression—Grade 1 | 0.17* | 0.16* |
| Attention problems—Kindergarten | 0.31* | 0.21* |
| Attention problems—Grade 1 | 0.17* | 0.13* |
| Early adolescent school maladjustment | ||
| Teacher ratings | 0.39* | 0.33* |
| Parent ratings | 0.36* | 0.33* |
| Early adolescent antisocial behavior | ||
| Self-report | 0.25* | 0.35* |
| Teacher ratings | 0.30* | 0.32* |
| Early adolescent substance use | ||
| Self-report of tobacco | 0.29* | 0.34* |
| Self-report of alcohol/drugs | 0.29* | 0.33* |
Age of first intercourse is reverse-scored, such that higher scores indicate an earlier and more risky age of initiation.
p <0.001
Measurement Model
In the second stage of data analyses, a measurement model was estimated to assess relations among observed measures and latent constructs. This measurement model is presented in Fig. 1. Once two sets of errors were allowed to correlate between the observed measures of early aggressive–disruptive behaviors and early attention problems (measures that shared common informants and were based on scales from the same instruments), the fit indices of this measurement model suggested that the hypothesized relations among observed measures and latent constructs did a satisfactory job of representing patterns in the actual data, χ2 (df=37, N=694)= 126.52, p<0.001. Although a nonsignificant χ2 is preferable, that is rare in large samples, and the other fit indices were good. The Comparative Fit Index (CFI; Bentler 1990), which ideally should be above 0.90, was 0.96. The Tucker–Lewis Index (TLI, also known as the Bentler–Bonett Non-normed Fit Index; Bentler and Bonett 1980), which should be above 0.90, was 0.92. The Root Mean Square Error of Approximation (RMSEA, Browne and Cudeck 1993) was 0.06, placing it between a good fit (RMSEA less than 0.05) and a reasonable fit (RMSEA less than 0.10).
Fig. 1.
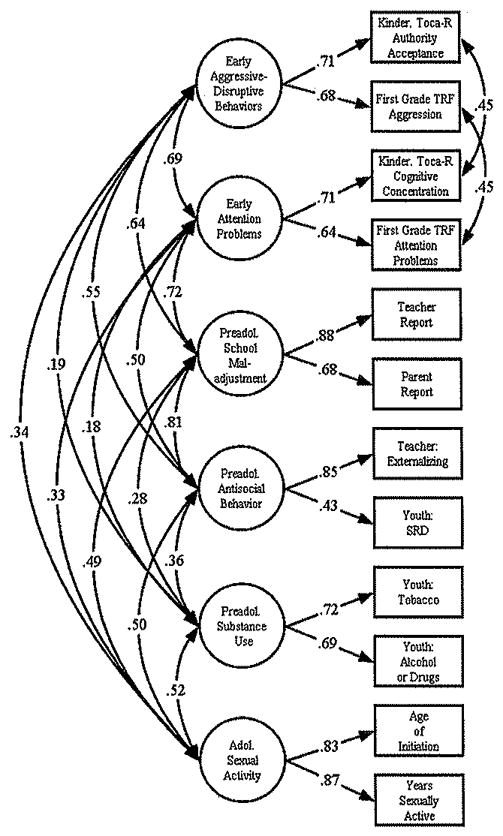
Measurement model
The measurement model revealed that observed measures served as acceptable indicators of their respective latent constructs. All relations between observed measures and latent constructs were statistically significant at the 0.001 probability level. Although one factor loading was small (.43), all of the other factor loadings were between 0.64 and 0.88. Relations between all pairs of latent constructs were small (ϕ=0.18) to large (ϕ=0.81) in magnitude and were statistically significant at the 0.01 or 0.001 probability level.1
Measurement invariance among subsamples
Although the measurement model appeared satisfactory for the entire sample, it was important to know whether it applied equally well to distinct subsamples. Thus, tests of measurement invariance were conducted for gender and race. These tests compared a measurement model in which all relations between observed measures and their respective latent constructs and between all pairs of latent constructs were allowed to vary across subsamples with a measurement model in which all of those relations were constrained to be equal. If the relations that are allowed to vary are so comparable to one another that the goodness of fit of the measurement model is not compromised by forcing them to be equal, then the measurement model is considered invariant across subsamples. For this purpose, a difference in the CFI of −0.01 or less is considered to be one of the most accurate and reliable assessments of invariance, according to an extensive evaluation of 20 different goodness-of-fit indices, including the traditional χ2 difference test (Cheung and Rensvold 2002).
When all relations between observed measures and their respective latent constructs and between all pairs of latent constructs were allowed to vary for boys and girls, the CFI of the measurement model was 0.957. When all relations were constrained to be equal, the CFI was 0.954. This difference of −0.003 suggests that our measurement model applied equally well to both boys and girls.
When all relations were allowed to vary for African American and European American adolescents, the CFI of the measurement model was 0.961; when all relations were constrained to be equal, the CFI was 0.943. This difference of −0.018 suggests the existence of some differences across subsamples. When each equality constraint was tested individually, no statistically significant differences were found in the measurement of latent constructs (i.e, the relations between latent constructs and their observed measures), but four differences were found in relations among latent constructs. The relation between early aggressive–disruptive behaviors and early adolescent school maladjustment was smaller for African American youth (ϕ=0.49, p<0.001) than European American youth (ϕ=0.70, p<0.001); the relation between early attention problems and school maladjustment was smaller for African American youth (ϕ=0.57, p<0.001) than European American youth (ϕ=0.80, p<0.001); the relation between antisocial behavior and school maladjustment was larger for African American youth (ϕ=0.87, p<0.001) than European American youth (ϕ=0.77, p<0.001); and the relation between antisocial behavior and adolescent sexual activity was larger for African American youth (ϕ=0.46, p<0.001) than European American youth (ϕ=0.45, p<0.001). Although these relations were statistically significantly different from one another, they were all moderate to large in magnitude and quite similar in terms of substantive meaning.2
Structural Equations Models
In the third stage of data analyses, a series of structural equations models were estimated. The purpose of these analyses was to examine whether patterns of relations among the distal predictors of childhood problems (early aggressive behaviors and attention problems), the proximal predictors/hypothesized mediators (early adolescent school maladjustment, antisocial behavior, and substance use), and the outcome (adolescent sexual activity) were more consistent with developmental hypotheses of cumulative effects or meditation.
The first step in these analyses was to establish that our data met the necessary prerequisites to assess cumulative effects and mediation (Baron and Kenny 1986; Holmbeck 1997, 2002). For developmental hypotheses of both cumulative effects and mediation, each distal predictor needs to be related to the outcome, controlling for the effect of the other distal predictor.3 In a structural equations model in which only these relations were estimated—and all other relations were constrained to be zero—we found that early aggressive–disruptive behavior and early attention problems each uniquely predicted adolescent sexual activity with standardized path coefficients of 0.21 (p<0.01) and 0.25 (p<0.01), respectively.
For developmental hypotheses of mediation, but not cumulative effects, each distal predictor also needs to be related to the more proximal predictors/hypothesized mediators, controlling for the effect of the other distal predictor. In a structural equation in which only these relations were estimated—and all relations to the outcome were constrained to be zero—we found that the standardized path estimates between early aggressive–disruptive behaviors and early adolescent school maladjustment, antisocial behavior, and substance use were 0.49 (p<0.001), 0.78 (p<0.001), and 0.21 (p<0.05), respectively, and the standardized path estimates between early attention problems and early adolescent school maladjustment, antisocial behavior, and substance use were 0.57 (p< 0.001), 0.21 (p<0.05), and 0.13 (p=ns), respectively.
Finally, for developmental hypotheses of both cumulative effects and mediation, the proximal predictors/hypothesized mediators must predict the outcome, controlling for the effect of the distal predictors. In a structural equations model in which only these relations were estimated, the effects of early adolescent school maladjustment, antisocial behavior, and substance use on adolescent sexual activity were 0.35 (p< 0.001), 0.25 (p<0.001), and 0.38 (p<0.001), respectively.
Having established that our data met the necessary prerequisites for developmental hypotheses of both cumulative effects and mediation, we then estimated all relations among distal predictors, proximal predictors/hypothesized mediators, and the outcome simultaneously. Evidence for cumulative effects would consist of direct relations between the distal predictors (aggressive–disruptive behaviors and attention problems) and the outcome (adolescent sexual activity) that were still statistically significant and not reduced much in magnitude, in the context of simultaneous pathways of influence linking childhood problems to early adolescent problems and early adolescent problems to adolescent sexual activity. The most compelling evidence for mediation would consist of direct relations between the distal predictors and outcome that were much smaller in magnitude and ideally zero. For this saturated structural equations model, χ2 (df=40, N=694)= 173.56, p<0.001; the CFI was 0.95; the TLI was 0.90; and the RMSEA was 0.07. In this model, the relation between early aggressive–disruptive behaviors and adolescent sexual activity was reduced from its previous value of 0.21 (p<0.01) to 0.00 (p=ns). The relation between early attention problems and adolescent sexual activity was reduced from its previous value of 0.25 (p<0.01) to −0.12 (p=ns). The change in these relations was not consistent with developmental hypotheses of cumulative effects, but rather reflected support for mediation.
Hence, in the final structural equations model, which is presented in Fig. 2, we eliminated the nonsignificant direct paths between our distal predictors and outcome. Results from this model suggested a satisfactory fit, χ2 (df=42, N=694)=174.14, p<0.001; the CFI was 0.95; the TLI was 0.90; and the RMSEA was 0.07. The difference in χ2 between this more parsimonious structural equations model and the saturated structural equations model was 0.57 (174.14–173.56) with 2 degrees of freedom (42–40), which was nonsignificant, as we would expect with the elimination of two nonsignificant paths; the CFI increased by 0.001. Because there was no meaningful difference in the fit of the two structural equations models, this more parsimonious structural equations model was preferred.
Fig. 2.
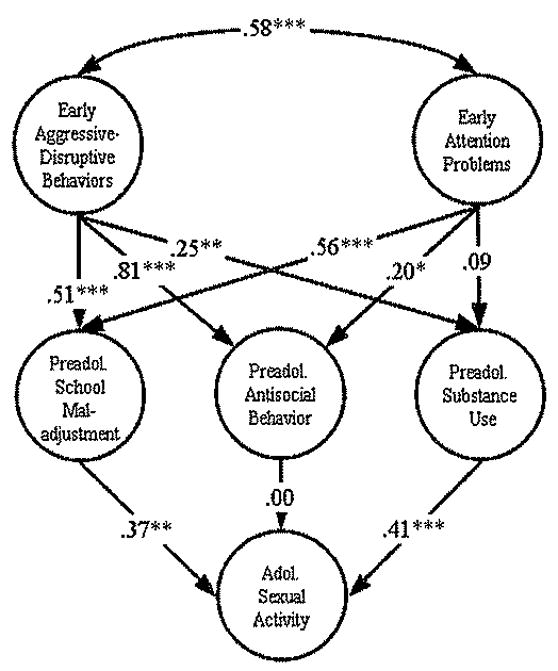
Final structural equations model
Interestingly, in this structural equations model, the relation between early attention problems and early adolescent substance use was nonsignificant, and the relation between early adolescent antisocial behavior and adolescent sexual activity was nonsignificant. This suggests that: (1) the relation between early aggressive–disruptive behaviors and adolescent sexual activity was mediated by early adolescent school maladjustment and early adolescent substance use (Sobel test statistic=2.87, p<0.01, and 2.62, p<0.01, respectively; Sobel, 1986); (2) the relation between early attention problems and adolescent sexual activity was mediated by early adolescent school maladjustment only (Sobel test statistic=2.83, p<0.01); and (3) after accounting for the effects of early adolescent school maladjustment and early adolescent substance use, there was no unique effect of early adolescent antisocial behavior on adolescent sexual activity.
Discussion
Our findings support the meditational model, based on problem behavior theory (Jessor 1991), that high rates of childhood aggressive–disruptive behavior and attention problems increase risk for a set of problem behaviors in early adolescence (school maladjustment, antisocial behavior, and substance use), which in turn, promote early sexual activity.
A major strength of the longitudinal design of this study was the availability of multiple sources of information about youth adjustment prior to the years of sexual activity, which enabled multi-informant assessments of each of the distal and proximal predictors. Kindergarten and first-grade teacher ratings were available to assess child aggressive–disruptive behaviors and attention problems at entry into elementary school (ages 5–7). Teacher, parent, and youth reports assessed early adolescent school maladjustment, antisocial behavior, and substance use, all collected when youth were in seventh grade (ages 12–14), prior to the initiation of sexual activity for most of them. Annual interviews with youth (7th through 11th grade) provided information about age at first intercourse and the number of years of adolescent sexual activity. With the exception of the youth who reported initiating sexual activity prior to or during 7th grade (20% of this sample), information on predictors was collected prior to the initiation of sexual activity, providing clarity in interpreting directionality of developmental influences. The extent and nature of the prospective longitudinal data enabled us to test the mediational model predicted by problem behavior theory, thereby contributing in a unique way to the growing empirical literature on this topic.
Kindergarten Behavior Problems as Risk Factors for Early Sexual Activity
A premise of problem behavior theory is that some children make the transition into adolescence with a history of socialization difficulties that predisposes them to resist adult authority, defy conventions, and engage in a range of rule-breaking activities (Udry et al. 1995; Willoughby et al. 2004). In support of this model, the results of this study document significant predictions from kindergarten and first-grade aggressive–disruptive behaviors to a set of rule-breaking behaviors in adolescence. Prior investigators have suggested that early rebelliousness subverts social controls and undermines the socialization efforts of parents and teachers, contributing to acting out in adolescence, including precocious sexual activity (Udry et al. 1995). In support of this conjecture, both boys and girls who engaged in high rates of externalizing behavior problems, which included an oppositional and aggressive orientation toward others, were at elevated risk for early adolescent school maladjustment, antisocial behavior, and substance use, as well as early sexual activity.
In this study, we also found evidence for the unique contributions of childhood attention problems to early adolescent difficulties, particularly school maladjustment and antisocial behavior, and to early sexual activity. These findings are consistent with other studies in which early deficits in self-regulation, inhibitory control, and poor decision-making skills have emerged as risk factors for early sexual activity (Crockett et al. 2006; Zimmer-Gembeck et al. 2004). Relatively few longitudinal studies have examined the predictive consequences associated with childhood aggression and inattention concurrently. In one of those studies, childhood hyperactivity did not predict early sexual debut or risky sexual activity, once concurrent childhood aggression was controlled (Ramrakha et al. 2007). However, in another such study, boys with childhood diagnoses of ADHD displayed elevated sexual risk in young adulthood (e.g., earlier age of sexual debut, multiple partners, infrequent condom use), whether or not they also exhibited concurrent aggressive–oppositional disorders, reflecting an independent contribution of early ADHD to later sexual risk (Flory et al. 2006). The findings of the present study highlight the independent predictive contributions of both aggressive–disruptive behaviors and attention problems to adolescent sexual activity.
Whereas childhood aggressive–disruptive behaviors and attention problems each predicted early adolescent sexual activity in this study, the link was not direct. Rather, the link was mediated by a set of risky early adolescent behaviors. Further research regarding the developmental influences of childhood aggression and inattention on later sexual risk is warranted, to better clarify the mechanisms by which these two types of childhood problems, alone and in combination, affect adolescent functioning and sexual behavior.
Early Adolescent Behaviors Associated with Early Sexual Activity
When simple correlations were computed, measures representing each of the early adolescent behavior problems studied (school maladjustment, antisocial behavior, substance use) significantly predicted age at first intercourse and years of adolescent sexual activity. When considered together in the structural equation model, school maladjustment and substance use played primary roles in mediating the impact of childhood problems on risky adolescent sexual activity. In contrast, early adolescent antisocial behavior did not make a unique contribution to adolescent sexual activity, when the other problems were considered concurrently.
In this study, school maladjustment reflected difficulties reported by teachers and parents in domains of academic engagement, social skills and peer relations, behavioral conduct at school, and student–teacher conflicts. Youth who showed this broad pattern of academic disengagement and interpersonal alienation were also likely to exhibit antisocial behavior and to engage in early sexual activity. These findings are consistent with a social control theory, which suggests that adolescents who feel closely connected to parents, peers, and teachers are more likely to delay sexual activity. Most likely, they are responding to the social control that these individuals exert which reduces interest and constrains opportunity to engage in behavior that is not permitted (Bearman and Bruckner 2001), In general, youth who show strong academic performance are involved in more extracurricular activities and have fewer unstructured, unsupervised opportunities for unsanctioned activities than peers who are disengaged from school (Resnick et al, 1997). Conversely, youth who are disengaged from school and alienated from mainstream peers are not deterred by these conventional social controls, and instead are attracted to the perceived pleasures of unrestrained activities, including substance use and sexual activity (Bearman and Bruckner 2001). As deviant peer groups coalesce, they may provide each other with both opportunity and reinforcement for rule-breaking behavior, including antisocial activity, substance use, and sexual activity (Dishion et al. 1997; Pedersen et al. 2003).
In this study, the failure of antisocial behavior to make an independent contribution to early sexual activity likely reflects the high level of association between these antisocial behavior and school maladjustment. Bivariate correlations reveal that levels of predictive association between early adolescent antisocial behavior and early sexual activity were similar to those between school maladjustment and early sexual activity. However, youth appear unlikely to engage in the extreme antisocial behaviors measured (e.g., stealing, truancy, drug selling, physically attacking others) without also showing school maladjustment. Evidence that a youth is disengaged academically and alienated interpersonally at school appears sufficient to predict risk for early sexual activity, whether or not that school maladjustment is accompanied by more severe antisocial behaviors.
Early adolescent substance use also figured prominently as a predictor of early sexual activity, consistent with studies that demonstrate the frequent co-occurrence of substance use and risky sexual activity among older adolescents (Lanctot and Smith 2001; Leitenberg and Saltzman 2000; Whitbeck et al. 1999). This finding is especially important given the longitudinal nature of the data. Early adolescent substance use emerged as an independent predictor of the early initiation of sexual activity, and a mediator of the influence of early aggressive–disruptive behavior on early sexual activity.
Interestingly, differences in the mediational pathways linking childhood aggressive–disruptive behavior and attention problems to early sexual activity suggest processes of equifinality, in which different risky pathways lead to the same outcome. Whereas the link between childhood aggressive–disruptive behavior and early sexual activity was mediated by school maladjustment and substance use, the link between childhood attention problems and early sexual activity was mediated only by school maladjustment. Consistent with problem behavior theory and perhaps reflecting a high level of self-interest and short-term reward-seeking orientation, childhood aggressive–disruptive behavior strongly predicted the range of early adolescent undercontrolled behaviors studied here (school maladjustment, antisocial behavior, and substance use), which fueled interest in and provided opportunity for early sexual activity. In contrast, the self-regulatory deficits and learning problems associated with childhood inattention may have impaired functioning and disrupted adjustment in both academic and interpersonal school contexts, contributing to early adolescent school disengagement and social alienation, thereby fostering interest in and opportunity for early sexual activity.
Race and Gender Effects
Prior research has documented gender differences in the variables studied here, with boys showing higher rates of childhood aggression and inattention than girls. Similarly, in this study, a higher proportion of the high-risk sample (selected on the basis of elevated rates of childhood externalizing problems) was male than female. However, the developmental model was comparable across gender. In general, the “gender gap” that is caused by significantly higher rates of externalizing problem behaviors for boys than girls during middle childhood begins to diminish in adolescence, when girls show rates of non-violent delinquent and antisocial behaviors that are often equivalent to boys (Silverthorn and Frick 1999). The results of this study suggest that the indices of childhood risk for early adolescent maladjustment and early sexual initiation are similar for boys and girls, despite higher base rates among boys.
Likewise, prior research has documented earlier ages of initiation of sexual activity among African American girls compared with European American girls (Furstenberg et al. 1987; Brooks-Gunn and Furstenberg 1989; Miller et al. 1997; Doljanac and Zimmerman 1998), leading us to examine whether the developmental model tested here was invariant across race. In this study, race affected the strength of several predictive and concurrent associations with school maladjustment. Specifically, childhood externalizing problems (aggressive–disruptive behaviors and attention problems) were more strongly predictive of early adolescent school maladjustment for European American youth than African American youth, whereas antisocial behavior was more strongly associated with school maladjustment and adolescent sexual activity for African American youth than for European American youth. However, these variations were small in magnitude and the same key pathways remained statistically significant and clinically meaningful for both African American and European American youth. Hence, despite these variations, the basic developmental pathways contributing to risk for early sexual activity appear similar across race.
Limitations and Future Directions
Although this data set allowed us to examine the timing of early sexual activity, we did not have information regarding characteristics of the sexual activity that might elucidate the emergence of risk patterns within the sexually active group. Future research might take a closer look at the emergence of risky sexual practices during the course of middle school for the early-starting group, including number of same-sex and opposite-sex partners, relationships with partners, substance use during sexual activity, use of protective birth control, and safe-sex practices. More detailed information regarding the motives and beliefs of these youth might also be helpful in understanding their decision-making processes. In addition, given that our information about sexual activity was limited to self-reports given in annual interviews, we know little about the contexts in which sexual activity occurred, and the impact on the individuals. Prior investigators have suggested that adolescent girls typically feel worse after becoming sexually active, increasing the likelihood that early adolescent sexual activity will contribute to depression and substance use (Bearman and Bruckner 2001). Studies of high-risk youth that provided more information about the events (feelings, behaviors, social interactions) leading up to, surrounding, and following sexual activity might provide additional insight regarding the impact of this activity on adjustment.
In terms of informing prevention programming to reduce early sexual activity, this study suggests that programs targeting childhood risk factors (early aggression and inattention) might be important. It also suggests that the transition into middle school represents a critical period. Vulnerable youth showed behavior problems and self-regulation deficits beginning in elementary school, which progressed to a broad spectrum of school maladjustment and risk-taking behaviors as they entered middle school, including sexual activity. The growth in problem behaviors at middle school entry may be due to several developmental factors. First, monitoring and supervision by teachers and parents decreases, and youth have greater autonomy and mobility. Second, pubertal development continues (typically between ages 11 and 14), which motivates and facilitates sexual activity. Third, when children transition into larger middle schools with academic tracking (as the majority of youth in the USA do), large groups of disengaged peers are brought together, increasing the opportunities for finding social partners who support deviant attitudes and rule-breaking behaviors. Youth who are showing elevated aggressive behavior and attention problems in elementary school appear in particular need of support programs over the transition to middle school to reduce the likelihood of school maladjustment, unsupervised time, and deviant peer affiliation which foster the pattern of alienated behavior and substance use that serves as the springboard for early sexual activity. These findings suggest that this broad pattern of vulnerabilities and risky behaviors should be targeted by prevention programs to prevent early sexual activity.
Sexual activity becomes normative later in high school, and at that point, prevention programs may be effective with a more specific focus on promoting safe sex practices. For the youth who are early-starting, in contrast, prevention programs may be most helpful when they target a range of important competencies, promoting stronger connections to family and teachers, social inclusion with mainstream peers, and extracurricular and vocational interests that provide structured opportunities for adaptive skill development.
Acknowledgments
This work was supported by National institute of Mental Health (NIMH) grants R18 MH48043, R18 MH50951, R18 MH50952, and R18 MH50953. The Center for Substance Abuse Prevention and the National Institute on Drug Abuse also provided support for Fast Track through a memorandum of agreement with the NIMH. This work was also supported in part by Department of Education grant S184U30002 and NIMH grants K05MH00797 and K05MH01027. We are grateful for the close collaboration of the Durham Public Schools, the Metropolitan Nashville Public Schools, the Bellefonte Area Schools, the Tyrone Area Schools, the Mifflin County Schools, the Highline Public Schools, and the Seattle Public Schools, We appreciate the dedication of hundreds of staff members who implemented the project, collected the evaluation data, and assisted with data management. For additional information concerning Fast Track, see http://www.fasttrackproject.org.
Footnotes
Members of the CPPRG in alphabetical order include Karen L. Bierman (Pennsylvania State University), John D. Coie (Duke University), Kenneth A. Dodge (Duke University), Mark T. Greenberg (Pennsylvania State University), John E. Lochman (University of Alabama), Robert J. McMahon (University of Washington), and Ellen E. Pinderhughes (Tufts University).
Maximum likelihood assumes multivariate normality; estimates involving substance use may be less reliable because both observed indicators were dichotomous.
Although not as relevant to the hypotheses of this study, measurement invariance also was assessed for subsamples of youth with and without severe aggressive-disruptive behaviors at school entry (i.e., in the high-risk or normative control groups, based on our screening procedure), and for subsamples of youth above and below the sample median in family SES. In both cases, the change in CFI was less than −.01, suggesting the existence of measurement invariance.
These traditional criteria can be quite restrictive and are not necessary for all conceptualizations of mediation (Dearing and Hamilton 2006).
References
- Achenbach TM. Manual for the Child Behavior Checklist: 4–18 and 1991 profile. Burlington, VT: University of Vermont Department of Psychiatry; 1991a. [Google Scholar]
- Achenbach TM. Manual for the Teacher’s Report Form and 1991 profile. Burlington, VT: University of Vermont Department of Psychiatry; 1991b. [Google Scholar]
- Barkley RA, Fischer M, Smallish L, Fletcher K. Young adult outcome of hyperactive children(:) Adaptive functioning in major life activities. Journal of the American Academy of Child and Adolescent Psychiatry. 2006;45:192–202. doi: 10.1097/01.chi.0000189134.97436.e2. [DOI] [PubMed] [Google Scholar]
- Baron RM, Kenny DA. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology. 1986;51:1173–1182. doi: 10.1037/0022-3514.51.6.1173. [DOI] [PubMed] [Google Scholar]
- Bearman PS, Bruckner H. Promising the future: Virginity pledges and first intercourse. American Journal of Sociology. 2001;106:859–912. doi: 10.1086/320295. [DOI] [Google Scholar]
- Bearman PS, Jones J, Udry RJ. The National Longitudinal Study of Adolescent Health: Research Design. Chapel Hill, NC: Carolina Population Center, University of North Carolina at Chapel Hill; 1997. [Google Scholar]
- Bentler P. Comparative fit indexes in structural models. Psychological Bulletin. 1990;107:238–246. doi: 10.1037/0033-2909.107.2.238. [DOI] [PubMed] [Google Scholar]
- Bentler P, Bonett DG. Significance tests and goodness of fit in the analysis of covariance structures. Psychological Bulletin. 1980;88:588–606. doi: 10.1037/0033-2909.88.3.588. [DOI] [Google Scholar]
- Biederman JB, Faraone SV, Mick E. Clinical correlates of ADHD in females: Findings from a large group of girls ascertained from pediatric and psychiatric referral services. Journal of the American Academy of Child and Adolescent Psychiatry. 1999;38:966–975. doi: 10.1097/00004583-199908000-00012. [DOI] [PubMed] [Google Scholar]
- Bierman KL, Bruschi C, Domitrovich C, Fang GY, Miller-Johnson S. Early disruptive behaviors associated with emerging antisocial behavior among girls. In: Putallaz M, Bierman K, editors. CPPRG Aggression, antisocial behavior, and violence among girls: A developmental perspective. New York: Guilford; 2004. pp. 137–161. [Google Scholar]
- Bingham CR, Crockett LJ. Longitudinal adjustment patterns of boys and girls experiencing early, middle, and late sexual intercourse. Developmental Psychology. 1996;32:647–658. doi: 10.1037/0012-1649.32.4.647. [DOI] [Google Scholar]
- Boles S, Biglan A, Smolkowski K. Relationships among negative and positive behaviours in adolescence. Journal of Adolescence. 2006;29:33–52. doi: 10.1016/j.adolescence.2005.01.007.. [DOI] [PubMed] [Google Scholar]
- Broidy LM, Nagin DS, Tremblay RE, Bates JE, Brame B, Dodge KA, et al. Developmental trajectories of childhood disruptive behaviors and adolescent delinquency: A six-site, cross-national study. Developmental Psychology. 2003;39:222–245. doi: 10.1037/0012-1649.39.2.222.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brooks-Gunn J, Furstenberg FF. Adolescent sexual behavior. The American Psychologist. 1989;44:249–257. doi: 10.1037/0003-066X.44.2.249.. [DOI] [PubMed] [Google Scholar]
- Browne MW, Cudeck R. Alternative ways of assessing model fit. In: Bollen KA, editor. Testing structural equation models. Newbury Park, CA: Sage; 1993. pp. 136–162. [Google Scholar]
- Cheung GW, Rensvold RB. Evaluating goodness-of-fit indexes for testing measurement invariance. Structural Equation Modeling. 2002;9:233–255. doi: 10.1207/S15328007SEM0902_5. [DOI] [Google Scholar]
- Cohen J. Statistical power analysis for the behavioral sciences. 2. Hillsdale, NJ: Lawrence Erlbaum; 1988. [Google Scholar]
- Conduct Problems Prevention Research Group (CPPRG) A developmental and clinical model for the prevention of conduct disorder: The FAST Track Program. Development and Psychopathology. 1992;4:509–527. [Google Scholar]
- Conduct Problems Prevention Research Group (CPPRG) Teacher rating of student adjustment. Technical report. 1995 Available at: www.fasttrackproject.org.
- Conduct Problems Prevention Research Group (CPPRG) School adjustment—parent report. Technical report. 1997 Available at: www.fasttrackproject.org.
- Crockett LJ, Raffaelli M, Shen Y. Linking self-regulation and risk proneness to risky sexual behavior: Pathways through peer pressure and early substance use. Journal of Research on Adolescence. 2006;16:503–525. doi: 10.1111/j.1532-7795.2006.00505.x. [DOI] [Google Scholar]
- Crockett LJ, Bingham CR, Chopak JS, Vicary JR. Timing of first sexual intercourse: The role of social control, social learning, and problem behavior. Journal of Youth and Adolescence. 1996;25:89–111. doi: 10.1007/BF01537382. [DOI] [PubMed] [Google Scholar]
- Dearing E, Hamilton LC. Contemporary advances and classic advice for analyzing mediating and moderating variables. Monographs of the Society for Research in Child Development. 2006;71:88–104. doi: 10.1111/j.1540-5834.2006.00406.x.. [DOI] [Google Scholar]
- Dishion T, French D, Patterson G. The development and ecology of antisocial behavior. In: Cicchetti D, Cohen D, editors. Manual of developmental psychopathology. Now York: Wiley; 1997. pp. 421–471. [Google Scholar]
- Doljanac RF, Zimmerman MA. Psychosocial factors and high-risk sexual behavior: Race differences among urban adolescents. Journal of Behavioral Medicine. 1998;21:451–467. doi: 10.1023/A:1018784326191. [DOI] [PubMed] [Google Scholar]
- Elliot DS, Morse BJ. Drug use, delinquency, and sexual activity. In: Jones C, McAnarney E, editors. Drug abuse and adolescent sexual activity, pregnancy, and parenthood. Washington, DC: US Government Printing Office; 1987. pp. 32–60. [Google Scholar]
- Farrell AD, Danish SJ, Howard CW. Relationship between drug use and other problem behaviors in urban adolescents. Journal of Consulting and Clinical Psychology. 1992;60:705–712. doi: 10.1037/0022-006X.60.5.705. [DOI] [PubMed] [Google Scholar]
- Fergusson DM, Horwood LJ, Ridder EM. Show me the child at seven: The consequences of conduct problems in childhood for psychosocial functioning in adulthood. Journal of Child Psychology and Psychiatry, and Allied Disciplines. 2005;46:837–849. doi: 10.1111/j.1469-7610.2004.00387.x. [DOI] [PubMed] [Google Scholar]
- Flory K, Molina BSG, Pelham WE, Jr, Gnagy E, Smith B. Childhood ADHD predicts risky sexual behavior in young adulthood. Journal of Clinical Child and Adolescent Psychology. 2006;35:571–577. doi: 10.1207/s15374424jccp3504_8.. [DOI] [PubMed] [Google Scholar]
- Furstenberg FF, Morgan SP, Moore KA, Peterson JL. Race differences in the timing of adolescent intercourse. American Sociological Review. 1987;52:511–518. doi: 10.2307/2095296. [DOI] [Google Scholar]
- Guttmacher Institute. Facts on American Teens’ Sexual and Reproductive Health. 2006 Available at: http://www.guttmacher.org/pubs/fb_ATSRH.html.
- Hollingshead AB. Four Factor Index of Social Status. New Haven, CT: Yale University; 1975. Unpublished manuscript. [Google Scholar]
- Holmbeck G. Toward terminological, conceptual, and statistical clarity in the study of mediators and moderators: Examples from the child-clinical and pediatric psychology literatures. Journal of Consulting and Clinical Psychology. 1997;65:599–610. doi: 10.1037/0022-006X.65.4.599. [DOI] [PubMed] [Google Scholar]
- Holmbeck G. Post-hoc probing of significant moderational and meditational effects in studies of pediatric populations. Journal of Pediatric Psychology. 2002;27:87–96. doi: 10.1093/jpcpsy/27.1.87. [DOI] [PubMed] [Google Scholar]
- Huizinga D, Elliott D. Reassessing the reliability and validity of self-report delinquency measures. Journal of Quantitative Criminology. 1986;2:293–327. [Google Scholar]
- Jessor R. Risk behavior in adolescence: A psychosocial framework for understanding and action. The Journal of Adolescent Health. 1991;12:597–605. doi: 10.1016/1054-139X(91) 90007-K. [DOI] [PubMed] [Google Scholar]
- Kotchick BA, Shaffer An, Forehand R, Miller KS. Adolescent sexual risk behavior: A multi-system perspective. Clinical Psychology Review. 2001;21:493–519. doi: 10.1016/S0272-7358(99)00070-7. [DOI] [PubMed] [Google Scholar]
- Lanctot N, Smith CA. Sexual activity, pregnancy, and deviance in a representative urban sample of African American girls. Journal of Youth and Adolescence. 2001;30:349–372. doi: 10.1023/A:1010496229445.. [DOI] [Google Scholar]
- Leitenberg H, Saltzman H. A statewide survey of age at first intercourse for adolescent females and age of their male partners: Relation to other risk behaviors and statutory rape implications. Archives of Sexual Behavior. 2000;29:203–215. doi: 10.1023/A:1001920212732.. [DOI] [PubMed] [Google Scholar]
- Martin A, Ruchkin V, Caminis A, Vermeiren R, Henrich CC, Schwab-Stone M. Early to bed: A study of adaptation among sexually active urban adolescent girls younger than age sixteen. Journal of the American Academy of Child and Adolescent Psychiatry. 2005;44:358–367. doi: 10.1097/01.chi.0000153226.26850.fd. [DOI] [PubMed] [Google Scholar]
- Miller BC, Norton MC, Curtis T, Hill EJ, Schvaneveldt P, Young MH. The timing of sexual intercourse among adolescents: Family, peer, and other antecedents. Youth & Society. 1997;29:54–83. doi: 10.1177/0044118X97029001003.. [DOI] [Google Scholar]
- Miller-Johnson S, Winn D, Coie JD, Malone PS, Lochman J. Risk factors for adolescent pregnancy reports among African American males. Journal of Research on Adolescence. 2004;14:471–495. doi: 10.1111/j.1532-7795.2004.00083.x. [DOI] [Google Scholar]
- Moffitt TE. Adolescence-limited and life-course-persistent antisocial behavior: A developmental taxonomy. Psychological Review. 1993;100:674–701. doi: 10.1037/0033-295X.100.4.674.. [DOI] [PubMed] [Google Scholar]
- Nadeau KG, Littman EB, Quinn PO. Understanding girls with attention deficit hyperactivity disorder. Silver Spring, MD: Advantage; 1999. [Google Scholar]
- Pedersen W, Samuelsen SO, Wichstrom L. Intercourse debut age: Poor resources, problem behavior, or romantic appeal? A population-based longitudinal study. Journal of Sex Research. 2003;40:333–345. doi: 10.1080/00224490209552199. [DOI] [PubMed] [Google Scholar]
- Phinney VG, Jensen LC. The relationship between early development and psychosexual behaviors in adolescent females. Adolescence. 1990;25:321–333. [PubMed] [Google Scholar]
- Ramrakha S, Bell ML, Paul C, Dickson N, Moffitt TE, Caspi M. Childhood behavior problems linked to sexual risk taking in young adulthood: A birth cohort study. Journal of the American Academy of Child and Adolescent Psychiatry. 2007;46:1272–1279. doi: 10.1097/chi.0b013e3180f6340e. [DOI] [PubMed] [Google Scholar]
- Resnick MD, Bearman PS, Blum RW, et al. Protecting adolescents from harm: Findings from the National Longitudinal Study of Adolescent Health. Journal of the American Medical Association. 1997;278:823–832. doi: 10.1001/jama.278.10.823.. [DOI] [PubMed] [Google Scholar]
- Silverthorn P, Frick PJ. Developmental pathways to antisocial behavior: The delayed-onset pathway in girls. Development and Psychopathology. 1999;11:101–126. doi: 10.1017/S0954579499001972.. [DOI] [PubMed] [Google Scholar]
- Sobel ME. Some new results on indirect effects and their standard errors in covariance structure models. In: Tuma N, editor. Sociological methodology. Washington, DC: American Sociological Association; 1986. pp. 159–186. [Google Scholar]
- Udry JR, Kovenock J, Morris NM, van den Berg BJ. Childhood precursors of age at first intercourse for females. Archives of Sexual Behavior. 1995;24:329–337. doi: 10.1007/BF01541603. [DOI] [PubMed] [Google Scholar]
- Werthamer-Larsson L, Kellam SG, Wheeler L. Effects of first grade classroom environment on shy behavior, aggressive behavior, and concentration problems. American Journal of Community Psychology. 1991;19:585–602. doi: 10.1007/BF00937993. [DOI] [PubMed] [Google Scholar]
- Whitbeck LB, Yoder KA, Hoyt DR, Conger RD. Early adolescent sexual activity: A developmental study. Journal of Marriage and the Family. 1999;61:934–946. doi: 10.2307/354014. [DOI] [Google Scholar]
- Willoughby T, Chalmers H, Busseri MA. Where is the syndrome? Examining co-occurrence among multiple problem behaviors in adolescence. Journal of Consulting and Clinical Psychology. 2004;72:1022–1037. doi: 10.1037/0022-006X.72.6.1022.. [DOI] [PubMed] [Google Scholar]
- Woodward LJ, Ferguson DM. Early conduct problems and later risk of teenage pregnancy in girls. Development and Psychopathology. 1999;11:127–141. doi: 10.1017/S0954579499001984. [DOI] [PubMed] [Google Scholar]
- Zimmer-Gembeck MJ, Siebenbruner J, Collins WA. A prospective study of intraindividual and peer influences on adolescents’ heterosexual romantic and sexual behavior. Archives of Sexual Behavior. 2004;33:381–394. doi: 10.1023/B:ASEB.0000028891.16654.2c.. [DOI] [PubMed] [Google Scholar]
- Zweig JM, Lindberg LD, McGinley KA. Adolescent health risk profiles: The co-occurrence of health risks among females and males. Journal of Youth and Adolescence. 2001;30:707–728. doi: 10.1023/A:1012281628792. [DOI] [Google Scholar]