

Abstract
A case of large aneurysm arising from the distal end of an azygous A2 segment is presented. Multiple clip application inadvertently tore the aneurysmal neck, resulting in near avulsion of a right pericallosal artery origin. After an unsuccessful attempt to repair the avulsion, it was treated by occlusion of the origin of the pericallosal artery and an A4-A4 anterior cerebral artery in situ bypass without neurological deficits. The surgical technique and previous reports on side-to-side in situ bypass are discussed.
Keywords: Aneurysm, Azygous anterior cerebral artery, In situ bypass procedure, Pericallosal artery
INTRODUCTION
The ideal treatment of a cerebral aneurysm is complete exclusion of the sac from the arterial circulation, while preserving the parent vessels. However, the application of multiple clips near the neck of a large aneurysm can cause an accidental tear at the neck. While a minor tear at the aneurysmal neck can be repaired using microvascular sutures or a wrap-clipping technique, a large tear developing into subtotal avulsion of the parent artery warrants trapping the tear and immediate revascularization procedure.
This report covers a case where the neck clipping of a large aneurysm arising from the distal end of the azygous A2 segment of the anterior cerebral artery (ACA) caused near avulsion of a pericallosal artery origin. The iatrogenic avulsion of the pericallosal artery was rescued by trapping and revascularization using an A4-A4 side-to-side anastomosis.
CASE REPORT
A 73-year-old woman presented to the emergency room with the sudden onset of a severe headache. She had no neurological abnormalities, and her Glasgow Coma Scale score was 14.
Examination. A computed tomography (CT) scan revealed a diffuse subarachnoid hemorrhage in the basal cisterns and anterior interhemispheric fissure (Fisher grade 3). Meanwhile, cerebral angiography and three-dimensional CT angiography demonstrated an azygous ACA, a large multi-lobulated saccular aneurysm at the junction of the azygous ACA and bilateral pericallosal arteries, and aplastic left A1 segment (Fig. 1). Plus, the venous phase of the right carotid angiogram showed a large frontal parasagittal bridging vein over the site of the aneurysm.
Fig. 1.

Initial cerebral angiography (A) and three-dimensional computed tomography angiography (B), demonstrating azygous anterior cerebral artery (ACA), large multi-lobulated saccular aneurysm at junction of azygous ACA and bilateral pericallosal arteries.
Operation. The patient underwent an anterior interhemispheric approach using a bicoronal scalp incision and right-sided paramedian craniotomy on the day of admission. A large parasagittal bridging vein was in the way of access to the aneurysm, yet was carefully preserved during the operation.
The aneurysm was 20 mm in diameter and involved the origins of both pericallosal arteries. After applying a temporary clip to the distal part of the azygous ACA, the ruptured fundus of the aneurysm was occluded using a long straight clip and fenestrated clip. However, while applying another fenestrated clip was applied to occlude a remnant of the aneurysm, the aneurysmal neck adjoining the origin of the right pericallosal artery was inadvertently torn, causing near avulsion of the right pericallosal artery. At first, primary repair of the avulsion was attempted with microsutures and clip application, yet this failed. Thus, trapping the avulsion based on clipping the origin of the right pericallosal artery and adjoining aneurysmal neck became unavoidable.
Immediate attention was then given to the more distal pericallosal arteries bilaterally, just behind the aneurysm and the large parasagittal bridging vein. These supracallosal (A4) segments were dissected and repositioned side by side, and a rubber dam was placed under the vessels. After placing temporary clips on either side of each vessel, linear arteriotomies of equal size, approximately 5 mm long, were then made on the medial aspects of both vessels. The back walls were sutured first using an inside-out technique in a running fashion, starting with a short (5 cm long) 10-0 nylon suture to avoid entanglement, then once the row was completed, the running suture was tightened. Thereafter, the front walls were sutured with interrupted 10-0 nylon sutures. Before the last suture was tied, the lumen was flushed with heparinized saline. After removing the temporary clips, the blood flow through both pericallosal arteries was confirmed using Doppler flowmetry (Fig. 2), and normal perfusion obtained 40 minutes after the occlusion of the right pericallosal artery origin. An elevated arterial pressure was maintained during the procedure for enhanced cerebral collateralization.
Fig. 2.
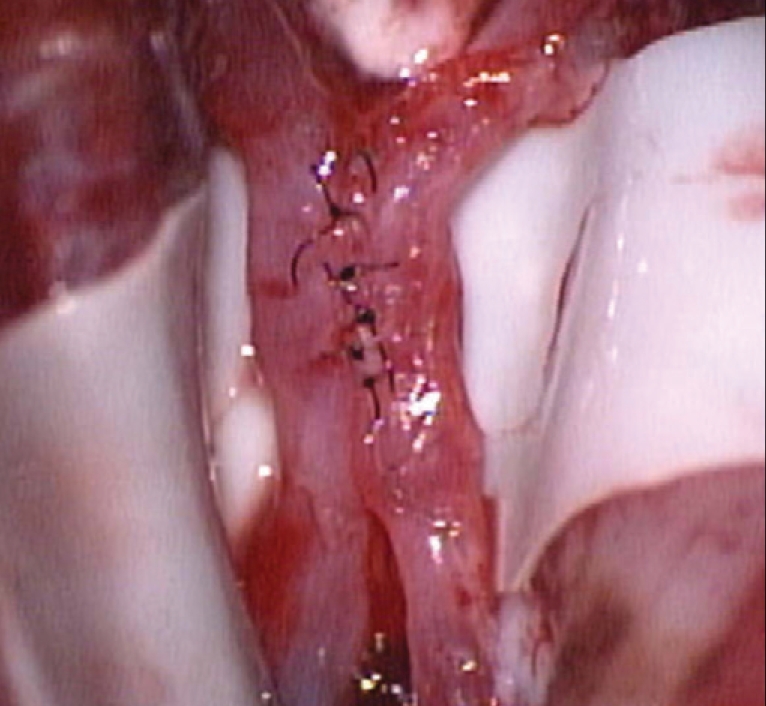
Intraoperative photograph of completed A4-A4 side-to-side anastomosis. The back walls of the pericallosal arteries were sutured first using an inside-out technique in a running fashion. The front walls were then sutured using interrupted 10-0 nylon sutures.
Postoperative course. The patient did very well after the operation although a postoperative CT scan demonstrated a small infarct in the right prefrontal area. At several weeks following the subarachnoid hemorrhage, the patient underwent a ventriculoperitoneal shunting for hydrocephalus. Postoperative conventional angiography and three-dimensional CT angiography both demonstrated the patency of the anastomotic connection (Fig. 3). The patient was neurologically intact at one-year follow-up.
Fig. 3.

Postoperative angiograms. Conventional angiography (A) and three-dimensional computed tomography angiography (B), demonstrating patency of anastomotic connection (straight arrows). Note the occlusion of the origin of the right pericallosal artery (curved arrow).
DISCUSSION
For elderly patients with a complex large aneurysm, less than complete occlusion of the aneurysm is acceptable and can be preferred to reduce the chance of parent artery insufficiency and aneurysmal neck damage, and to decrease temporary occlusion time of the proximal artery and brain retraction. However, in the case of a fragile aneurysmal neck or inadvertent clip application that cause tearing of the aneurysmal neck, primary repair using a microsuture technique or the application of a clip to the ruptured neck including the wall of the parent artery is warranted. If the primary repair is difficult due to extensive tearing or avulsion of the aneurysmal neck, trapping the lesion and a bypass procedure is the last resort.
Revascularization of the ACA is a challenge for neurosurgeons5,11), as the A2 to A4 segments of the ACA are located deep in the interhemispheric fissure, and there is no suitable donor artery nearby. The superficial temporal artery (STA) is not long enough to reach the distal ACA, requiring an interposition graft involving a saphenous vein, cephalic vein, or radial artery from the cervical carotid or STA artery5). A case of intended occlusion of the bilateral pericallosal arteries was reported in association with a unilateral STA bypass using an A3-radial artery graft and an A3-A3 side-to-side anastomosis4).
An in situ side-to-side bypass is appealing in an emergency situation, like the present case, as there is no need to harvest an extracranial donor vessel, thereby minimizing the ischemic time. Yet, a major concern with this procedure is the exposure of an intact contralateral pericallosal artery to the risk of infarction. Thus, technical proficiency in performing microanastomoses in a deep operative field is mandatory. The in situ side-to-side bypass technique has rarely been applied to several anatomical sites where the vessels are naturally close to each other. The distal ACAs from A2 to A4 in the interhemispheric fissure, secondary trunks (M2) of the MCA at the entrance to the insular cistern, the anterior temporal artery to the M2 segment, the posterior cerebral artery to the superior cerebellar artery in the ambient cistern, and the posterior inferior cerebellar arteries in the cisterna magna are all suitable vessels for a side-to-side anastomosis1-3,6-10,12,13).
According to previous experimental work on the carotid arteries of rats by Ikeda et al.3), arteriotomies larger than twice the vessel diameter and interrupted sutures in the front walls of the vessels are recommended for better patency. Although continuous sutures produce a purse-string effect, leading to the stenosis of arteriotomies, this problem can be solved by closely spacing the stitches.
Temporary occlusion of two major intracranial arteries during the side-to-side anastomosis requires some methods to increase tolerance to cerebral ischemia. Induced hypertension, barbiturates, and mild hypothermia are known methods for brain protection.
Endovascular coil embolization is also a viable option in elderly patients with subarachnoid hemorrhage. However, coil embolization was not considered suitable for the present case as the aneurysm had a wide neck and a working projection separating both pericallosal arteries from the aneurysmal neck was not achieved in angiographic evaluation.
CONCLUSION
Although cautious clip application not to damage an aneurysmal neck is most important, inadvertent major injury of an aneurysmal neck can be rescued by trapping and in situ side-to-side anastomosis when the primary repair is not successful.
References
- 1.Ausman JI, Diaz FG, Mullan S, Gehring R, Sadasivan B, Dujovny M. Posterior inferior to posterior inferior cerebellar artery anastomosis combined with trapping for vertebral artery aneurysm. Case report. J Neurosurg. 1990;73:462–465. doi: 10.3171/jns.1990.73.3.0462. [DOI] [PubMed] [Google Scholar]
- 2.Bederson JB, Spetzler RF. Anastomosis of the anterior temporal artery to a secondary trunk of the middle cerebral artery for treatment of a giant M1 segment aneurysm: case report. J Neurosurg. 1992;76:863–866. doi: 10.3171/jns.1992.76.5.0863. [DOI] [PubMed] [Google Scholar]
- 3.Ikeda A, Okada T, Shibuya M, Noda S, Sugiura M, Iguchi I, et al. Revascularization of the anterior cerebral artery. Report of two cases. J Neurosurg. 1985;62:603–606. doi: 10.3171/jns.1985.62.4.0603. [DOI] [PubMed] [Google Scholar]
- 4.Inoue T, Tsutsumi K, Ohno H, Shinozaki M. Revascularization of the anterior cerebral artery with an A3-A3 anastomosis and a superficial temporal artery bypass using an A3-radial artery graft to trap a giant anterior communicating artery aneurysm : technical case report. Neurosurgery. 2005;57(1) Suppl:E207. doi: 10.1227/01.neu.0000163682.31075.28. discussion E207. [DOI] [PubMed] [Google Scholar]
- 5.Ishii R, Koike T, Takeuchi S, Ohsugi S, Tanaka R, Konno K. Anastomosis of the superficial temporal artery to the distal anterior cerebral artery with interposed cephalic vein graft. Case report. J Neurosurg. 1983;58:425–429. doi: 10.3171/jns.1983.58.3.0425. [DOI] [PubMed] [Google Scholar]
- 6.Kim LJ, Albuquerque FC, McDougall C, Spetzler RF. Combined surgical and endovascular treatment of a recurrent A3-A3 junction aneurysm unsuitable for stand-alone clip ligation or coil occlusion. Technical note. Neurosurg Focus. 2005;18:E6. doi: 10.3171/foc.2005.18.2.7. [DOI] [PubMed] [Google Scholar]
- 7.Lemole GM, Jr, Henn J, Javedan S, Deshmukh V, Spetzler RF. Cerebral revascularization performed using posterior inferior cerebellar artery-posterior inferior cerebellar artery bypass. Report of four cases and literature review. J Neurosurg. 2002;97:219–223. doi: 10.3171/jns.2002.97.1.0219. [DOI] [PubMed] [Google Scholar]
- 8.Mabuchi S, Kamiyama H, Kobayashi N, Abe H. A3-A3 side-to-side anastomosis in the anterior communicating artery aneurysm surgery : report of four cases. Surg Neurol. 1995;44:122–127. doi: 10.1016/0090-3019(95)00047-x. [DOI] [PubMed] [Google Scholar]
- 9.Quinones-Hinojosa A, Lawton MT. In situ bypass in the management of complex intracranial aneurysms : technique application in 13 patients. Neurosurgery. 2005;57(1) Suppl:140–145. doi: 10.1227/01.neu.0000163599.78896.f4. discussion 140-145. [DOI] [PubMed] [Google Scholar]
- 10.Sekhar LN, Kalavakonda C, Elahi F. Cerebral revascularization. In: Sekhar LN, Fessler RG, editors. Atlas of neurosurgical techniques. Brain. New York: Thieme Medical Publishers Inc; 2006. pp. 339–378. [Google Scholar]
- 11.Smith RR, Parent AD. End-to-end anastomosis of the anterior cerebral artery after excision of a giant aneurysm. Case report. J Neurosurg. 1982;56:577–580. doi: 10.3171/jns.1982.56.4.0577. [DOI] [PubMed] [Google Scholar]
- 12.Steiger HJ, Ito S, Schmid-Elsässer R, Uhl E. M2/M2 side-to-side rescue anastomosis for accidental M2 trunk occlusion during middle cerebral artery aneurysm clipping : technical note. Neurosurgery. 2001;49:743–747. doi: 10.1097/00006123-200109000-00041. discussion 747-748. [DOI] [PubMed] [Google Scholar]
- 13.Sundt TM, Jr, Campbell JK, Houser OW. Transpositions and anastomoses between the posterior cerebral and superior cerebellar arteries. Report of two cases. J Neurosurg. 1981;55:967–970. doi: 10.3171/jns.1981.55.6.0967. [DOI] [PubMed] [Google Scholar]