

Abstract
This study examined the impact of an adaptive approach to family intervention in public schools on academic outcomes from age 11 to 17. Students were randomly assigned to the three-session Family Check-Up (FCU), which is designed to motivate change in parenting practices by using an assessment-driven approach and strengths-based feedback. All services were voluntary, and approximately 25% of the families engaged in the FCU. Compared with matched controls, adolescents whose parents received the FCU maintained a satisfactory GPA into high school, and intervention engagement was associated with improved attendance. The highest-risk families were the most likely to engage in the family-centered intervention, suggesting the efficacy of integrating supportive services to families in the context of other schoolwide approaches to promote the success and achievement of vulnerable students.
Keywords: Family intervention, Dosage, GPA, School absence, Early adolescence
A cornerstone of an ecological perspective on child and adolescent development is that children's experiences in one relationship context can affect development across settings (Bronfenbrenner 1989). Parent–child interaction in general and family management skills in particular are robust predictors of a variety of child behavior problems and negative outcomes for youth across multiple settings (Loeber and Dishion 1983; Patterson and Dishion 1988; Peterson et al. 1994). Patterns of interaction learned in the context of parent–child exchanges are typically generalized to school settings, leading to the development of later behavior problems, academic difficulties, and school dropout (Dishion and Loeber 1985; Loeber et al. 1993; Patterson et al. 1989). Considerable evidence supports a developmental model that links key family management skills such as low levels of parental monitoring with childhood antisocial behavior, academic failure, peer rejection, and emotional distress (e.g., Patterson and Stouthamer-Loeber 1984; Pettit et al. 1993; Stormshak et al. 2000; Webster-Stratton 1993). As children develop into adolescents, parents' and limit-setting practices may exacerbate existing behavior problems and academic difficulties and failure (Dishion and McMahon 1998).
Parents play a critical role in promoting academic success through parent–school involvement, stimulation of cognitive growth at home, and promotion of values consistent with academic achievement (Greenwood and Hickman 1991; McMahon et al. 1996). Parents' academic and school involvement is related to reduced behavior problems and academic achievement over time (Hill et al. 2004). In adolescence, low academic achievement is associated with a variety of health risk behaviors, including substance abuse, teen sexual activity, depression, and violence (Hawkins 1997; Larson and Ham 1993). Given the link between parenting proficiency and student success, it would seem plausible that interventions targeting family management skills will both reduce problem behavior and increase academic achievement.
Some may find it puzzling that very few intervention programs that directly target family management skills show evidence of improving academic achievement and school-related outcomes, particularly in adolescence. There are several potential reasons for this lack of findings. First, it may be that most intervention research is not funded to follow children long enough to measure changes in academic achievement. Collecting school data for an extended time is expensive and difficult. It may also be that many family-centered parenting programs focus too narrowly on parenting at home and place little emphasis on school problem behavior. The parenting interventions that are delivered and studied vary widely: Some focus on overall school achievement, and others are more limited in scope (Mattingly et al. 2002).
Multiple intervention trials undertaken during the elementary school years have specifically targeted both youth academic skills and family skills in an effort to enhance youth academic achievement (Hawkins et al. 1992; Tolan et al. 2004). These programs typically include delivery of a parenting intervention, academic tutoring, or reading support. Programs that include a parenting intervention in a larger, multifaceted intervention package have had a positive impact on school-related outcomes or achievement-related constructs such as self-regulation and school engagement. For example, the Fast Track program was delivered to children and families starting in the first grade and extending through high school. Youth in the program received academic tutoring, peer tutoring, and support for social skills, and their families engaged in an extensive parenting program. After 3 years in the program, children who participated showed a reduction in special education referrals. They were less likely to have an individualized education plan or be identified with a learning or behavioral problem (CPPRG 2002). These positive academic achievement outcomes may have resulted from the individual tutoring that each child received or from the parenting program and parent–school involvement intervention components.
Similarly, multifaceted intervention programs that include parent training as well as youth social skills and academic support have been shown to reduce self-regulation problems and increase school engagement, outcomes that are directly linked to academic skills at school (August et al. 2001; Hawkins et al. 2001). These results could be attributed to the parenting component of the program or to other components that more directly targeted academic success. It is impossible to tease apart the effects of individual intervention components in a multifaceted intervention, and therefore it remains unclear whether or not parenting interventions directly affect academic outcomes.
For adolescents, very few research programs have combined direct academic support with parent-training interventions within one intervention package. Recently, Spoth et al. (2008) published results of a family competency-training intervention program. They found that the family-based intervention in 6th grade through 12th grade had a positive impact on outcomes such as risk of substance use, school engagement, and academic performance through a key mediator: parenting competencies.
In a developmental–ecological model of intervention, transitions represent critical points for intervention efficacy (Cicchetti and Toth 1992; Sameroff 2000). The goal of targeting youth during a critical transition is to maintain development on a positive trajectory and to reduce risks typically associated with the transition. We are particularly interested in the transition from middle school to high school as a point of intervention because of its twofold nature. First, changing school contexts presents a demand on youth to increase self-regulation and autonomy. Clearly, the demands of the high school setting pose additional risks for underachieving youth. Expectations include increased self-monitoring of homework and school responsibilities and increased self-management of behavior. Eccles and colleagues (1993, 1995) have discussed the poor fit between the organizational structure of high schools and the needs of young adolescents. In general, the increased complexity of the typical middle school structure demands more self-regulation and involves less tracking and supervision by school personnel.
The second level to the middle school transition is the onset of puberty and children's increasing attention to and potential influence by peers (Brown 1989). The pull of biologically based motivations and the increased complexity of the school environment make it difficult for parents to track adolescents and to have a positive impact on their academic success, affiliation with peers, and even school attendance. Youth involved in problem behavior, in particular, will actively discourage parent involvement and tracking so as to create more unsupervised time with peers, which in turn will amplify problem behavior and school problems (Dishion et al. 2004; Stoolmiller 1994). Changes in peer group composition and increased unsupervised time with peers pose additional risks for youth, especially those already at risk (Dishion and Stormshak 2007). Given these considerations, early adolescence is a critical transition point in which a family-centered intervention may provide opportunities to alter developmental trajectories of risk for adolescent problem behavior and school failure (Coie et al. 1993). The Family Check-Up (FCU) intervention was designed to address these risk factors during the transition to high school by embedding a family-centered model of intervention into the middle school system (Dishion and Stormshak 2007).
The Family Check-Up Intervention Model
The FCU, described in detail by Dishion and Stormshak (2007), is a preventive intervention based on a health maintenance model that is appropriate for high-risk youth. The FCU targets parental engagement and motivates parents to improve their parenting practices. Following the FCU, a menu of family-centered interventions is offered to support effective family management practices and promote the well-being and improved behavior of children and adolescents (Dishion and Kavanagh 2003). Accordingly, the FCU is designed to link intervention services in the school and community. It actively promotes self-selection into the most appropriate intervention services on the basis of systematic assessments, available resources, and parents' motivation and skills. Across numerous randomized controlled intervention trials, the FCU has been shown to reduce teacher-reported risk behavior, arrest rates, substance use, depression, and antisocial behavior (Connell and Dishion 2008; Connell et al. 2007; Dishion et al. 2003; Stormshak et al. 2005). Interestingly, these outcomes have been mediated by an increase in family management skills, including parental monitoring (Dishion et al. 2003). This model of intervention has also been effective in early childhood; we have found that the FCU is related to reductions in early problem behavior and increases in positive parenting (Dishion et al. 2008a, b; Lunkenheimer et al. 2008).
Although each of these behavioral outcomes is theoretically linked to academic achievement, we have yet to systematically examine the long-term impact of the FCU intervention on academic achievement and school attendance. In this study we examined the impact of the FCU intervention on both these constructs over time during the transition from middle to high school. We hypothesize that our intervention will have a positive impact on both academic achievement and school attendance into the high school years.
The impact of adaptive interventions is complex to evaluate for a variety of reasons. Most critical is that adaptive interventions attempt to target individuals most in need of the intervention and ignore those who are not. In addition, motivation for engaging in an intervention may not fit well with the assessed need. Common analytic approaches such as per-protocol analysis, which excludes nonparticipating families, or as-treated analysis, which groups individuals by the intervention actually received, disrupt randomization and have great potential for bias (Little and Yau 1998). A critical step in evaluating the impact of an adaptive, tailored intervention is to identify a subset of the randomized control group who resemble those who do actively engage in a voluntary intervention. This group of control families should provide the most accurate picture of how youth receiving the FCU would have developed without intervention.
Fortunately, recently developed statistical techniques for the analysis of randomized intervention designs, referred to as complier average causal effect analyses (CACE; Imbens and Rubin 1997; Jo 2002; Little and Yau 1998), provide a way to systematically analyze treatment compliance as an index of engagement. CACE analysis was developed to address the problem of intervention noncompliance, which can be a major threat to randomized interventions and can lead to biased estimates of intervention effects and limited power to detect significant effects when they do exist (Angrist et al. 1996). There are several ways to apply CACE analysis. Recently, it has been integrated into a general framework for person- and variable-centered analyses, in an approach referred to as mixture modeling, using Mplus statistical software (Muthén 2004; Muthén and Muthén 2008). Jo (2002) applied the mixture-modeling framework to identify the optimal comparison group from the control condition to compare with intervention engagers in the intervention condition. Briefly, this application of mixture modeling permits the modeling of two aspects of intervention process: the prediction of intervention engagement and examination of the differential outcomes.
In this study, we used CACE analysis to identify predictors of intervention engagement, and to examine the effect of engagement with the selected and indicated levels of the Family Check-Up intervention on GPA and school absences from grades 6 through 11. In general, we predict that families with young adolescents at highest risk will be those most likely to engage in the intervention condition. Among those families who participate, we predict that receipt of the family intervention will be significantly associated with lower rates of school absences and higher GPA scores across adolescence.
Methods
Participants
Participants included 998 adolescents and their families, recruited in sixth grade from three middle schools in an ethnically diverse metropolitan community in the Northwest region of the USA. Parents of all sixth grade students in two cohorts were approached for participation using an active consent protocol, and 90% consented to participate in the school-based assessment (see Fig. 1). The sample included 526 males (52.7%) and 472 females (47.3%). By youth self-report, the group comprised 423 Caucasians (42.4%), 291 African Americans (29.2%), 68 Latinos (6.8%), 52 Asian Americans (5.2%), and 164 (16.4%) youth of other ethnicities (including biracial). Biological fathers were present in 585 families (58.6%). Youth were randomly assigned at the individual level to either control (498 youth) or intervention (500 youth) groups in the spring of sixth grade. Approximately 80% of the youth were retained across the longitudinal span of the current study (wave 2, n=857; wave 3, n=829; wave 4, n=820; wave 6, n=794).
Fig. 1.
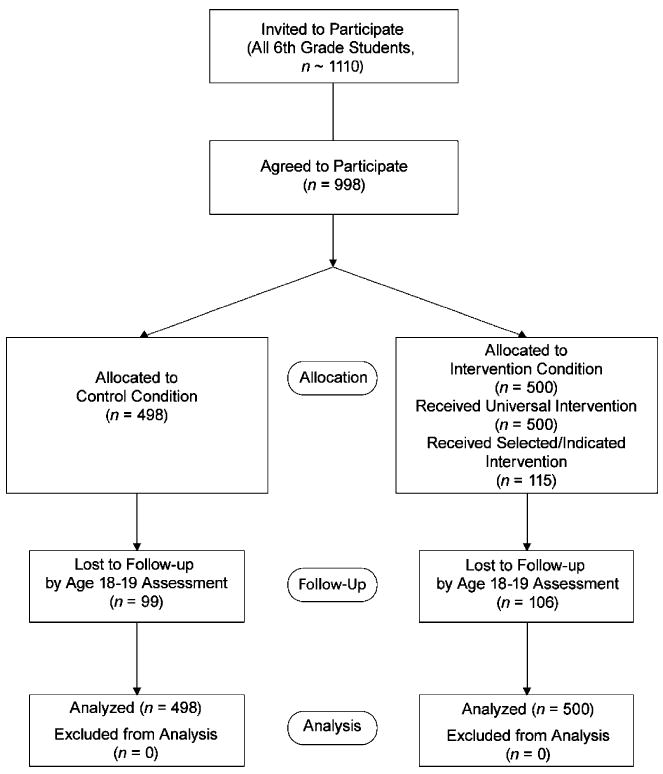
Flow of participants through study
Intervention Protocol
The FCU is part of the EcoFIT multilevel intervention program (Dishion et al. 2003; Dishion and Kavanagh 2003; Dishion and Stormshak 2007). The first level of the program, the universal intervention, was the development of a family resource center (FRC) in each of the three participating public middle schools. The parent-centered FRC services were available for the entire intervention group and included brief in-person consultations with parents, telephone consultations, feedback to parents about their student's behavior at school, and access to videotapes and books. The FRC services were designed to support positive parenting practices and to engage parents of high-risk youth for the selected intervention.
The selected intervention was the FCU, a brief, three-session intervention based on motivational interviewing and modeled on the Drinker's Check-Up (Miller and Rollnick 1991, 2002). Although all families could receive the FCU, families of youth at high risk, identified by teacher ratings, were specifically offered the FCU in seventh and eighth grades. The first session is an initial interview during which the therapist explores parent concerns and stage of change and motivates involvement in a family assessment. The second session is primarily an assessment process during which the family engages in a variety of assessment tasks and an in-home videotaped assessment of a parent–child interaction. The third session involves a strengths-based feedback session during which the therapist systematically summarizes the results of the assessment by using motivational interviewing strategies. An essential objective of the feedback session is to explore potential intervention services that support family management practices (see Dishion and Stormshak 2007).
An outcome of the FCU was a collaborative decision made between the parent and parent consultant regarding the indicated services most appropriate for the family. Services included empirically validated interventions such as a behaviorally oriented parent group intervention (Dishion and Andrews 1995; Forgatch and DeGarmo 1999), individually based behavior family therapy (Patterson 1975; Patterson et al. 1975), and multisystemic family therapy (Henggeler et al. 1998). Students who left the targeted schools were offered services if they remained in the county. When the students moved on to high school, FRC services were discontinued.
Services were delivered by parent consultants, including two master's-level therapists and one with a bachelor of science degree. Parent consultant ethnicity closely matched that of the participating families. Parent consultants were trained using a combination of strategies, including didactic instruction, role playing, and videotaped supervision throughout the 2 years of intervention activity.
In the intervention condition, 115 families (23%) elected to receive the FCU, and 88 of these families received further intervention services after the FCU. For Cohort 1, 46% of FCUs were completed following the seventh grade family assessment, 53% were completed following the eighth grade family assessment, and 1% was completed following the ninth grade family assessment. For cohort 2, 93% of FCUs were completed following the seventh grade family assessment, and 7% were completed following the eighth grade family assessment. Families who received the FCU had an average of 8.9 h of direct contact with the intervention staff during the course of the study (SD=9.42 h). Contrary to expectations, most families elected to receive brief consultations and periodic FCU meetings rather than more intensive forms of intervention.
Assessment Procedures
In the spring semester, from the 6th through 9th grades, and again in the 11th grade, student surveys were conducted using an instrument developed and reported by colleagues at the Oregon Research Institute (Metzler et al. 2001). Assessments were conducted primarily in the schools. If students moved out of their original schools, they were followed up at their new location. Each youth was paid $20 for completing each assessment.
Measures
Yearly Grade Point Average
Academic records were gathered from schools every year from 6th through 11th grade. When participating youth moved to a new school during the study, records were sought from those schools as well. Our study focused on cumulative GPA for each year, on a scale ranging from 0 to 4, with higher scores reflecting better grades (F=0, D=1, C=2, B=3, A=4). When possible, cumulative GPA for the entire academic year was provided by the school district and reflected the average grade across the child's academic courses. When youth attended multiple schools during the academic year, the cumulative GPA was calculated as the average of the available GPAs, weighted by the proportion of the school year they represented. If youth dropped out of school during the course of the study, their subsequent GPAs were coded as missing. Because of a change in the school district's record-keeping system, cohort 2 GPA data for 11th grade only were not available and were treated as missing.
Yearly School Absences
The total number of absences during each academic year was provided by the school district when possible. When youth attended multiple schools during the school year, records of absences for the part of the school year attended at each school were provided by the school districts, and the number of absences was summed across schools. If youth dropped out of school during the course of the study, their subsequent school absences were coded as missing.
Father Presence
Youth reports of biological father presence in their primary residence in sixth grade were coded as 0 = “biological father not present” and 1 = “biological father present.”
Teacher Report of Sixth Grade Risk Behavior
This measure was revised from an earlier version of a measure developed by Soberman (1994). Teachers were asked to use a 16-item questionnaire to rate their full roster of sixth grade students on a variety of risk behaviors associated with problem behavior in adolescence. The frequency with which youth engaged in a variety of problem behaviors was reported using a five-point scale ranging from 1 (never/almost never) to 5 (always/almost always). Items included aggression, oppositional behavior, peer relationship problems, disliking school, and moodiness. The sample mean=1.85 (SD = .85). High internal consistency reliability was found for this scale (alpha reliability=0.95). This variable was mean centered for use in analyses.
Substance Use in Sixth Grade
Youth reports about the frequency with which they had used alcohol or tobacco in the previous month was assessed in sixth grade. These items were summed for use in the current analyses.
Antisocial Behavior in Sixth Grade
Youth reports of engagement in problem behavior were measured averaging across six items. Items assessed the number of times in the past month teens reported having engaged in the following behaviors: (a) lying to parents, (b) skipping school, (c) staying out all night without permission, (d) stealing, (e) panhandling, and (f) carrying a weapon. Responses were given on a 6-point scale, ranging from 1 (never) to 6 (more than 20 times). Good internal reliability was found for this scale across assessments (alpha reliability ranged from 0.63 to 0.74 across years).
Deviant Peer Involvement in Sixth Grade
Youth reports of deviant peer involvement in sixth grade were measured averaging across four items. Items assessed children's reports of the number of times in the past week they had spent time with peers who (a) get into trouble, (b) fight a lot, (c) take things that don't belong to them, and (d) smoke cigarettes or chew tobacco. Responses ranged from 0 (never) to 7 (more than seven times). The sample mean=0.76 (SD=1.11). Good internal reliability was found for this scale (alpha reliability=0.79). Deviant peer involvement was mean centered for use in all analyses.
Family Conflict in Sixth Grade
Youth reports of family conflict in sixth grade were measured averaging across five items. Items reflected the frequency with which family members engaged in a variety of conflict behaviors during the past month (e.g., “got angry with each other,” “argued at the dinner table”). Responses ranged from 0 (never) to 7 (more than seven times). The sample mean=0.91 (SD=1.03). Good internal reliability was found for this scale (alpha reliability=0.81). This variable was mean centered for use in analyses.
Intervention Status
Random assignment was coded as 0 = “control” and 1 = “intervention.”
Engagement Status
Engagement status was coded to reflect family participation in the FCU (and further intervention services as warranted). Families in the intervention condition who elected to receive the FCU were coded 1 (n=115), and families in the intervention condition who did not receive the FCU were coded 0 (n=385). In the control condition, engagement status was coded as missing data.
Analytic Strategy
We used Mplus 5.1 to conduct CACE analyses as mixture models and used full information maximum likelihood estimation to account for missing data (Muthén and Muthén 2008), so that the N for all CACE models was 998. As described in detail by Jo (2002), CACE analysis is predicated on several assumptions that are necessary for CACE to provide an unbiased estimate of the intervention effect for compliers. These assumptions are (a) assignment to intervention is random; (b) potential outcomes for each participant are independent of the outcomes for other participants; (c) for noncompliers in either the intervention or control condition (i.e., never-takers or always-takers), the distribution of potential outcomes is independent of the intervention assignment; (d) there are no “defiers,” or individuals who will always do the opposite of instructions regardless of the instruction; and (e) the average causal effect of assignment to intervention on the actual receipt of services is not zero. The third assumption, known as the exclusion restriction, is typically the most questionable (Jo 2002), and we are confident of meeting the other four conditions. Violations of this assumption may lead to biased CACE estimates of intervention effects, particularly in the face of low engagement rates (Jo 2002). However, the potential effects of bias resulting from violations of the exclusion restriction can be ameliorated by the use of covariates to yield more precise estimates of engagement status. In the presence of significant predictors of engagement with intervention, analytic results provide unbiased estimates of the true CACE effect (for details see Jo 2002).
To examine the effect of adding covariates on the CACE estimate of the intervention effect, a series of analyses was conducted for each of the youth outcomes. First, a CACE model was examined that included only intervention assignment as a predictor. Intervention assignment was allowed to predict only the slope of problem behavior in the compliers class, but not the slope in the nonengagers class, the intercept in any class, or class membership. Second, this model was extended to include covariates, which were allowed to predict intercept and slope in both classes, along with class membership. Because there were no substantial differences in the magnitude of the CACE estimates of intervention effects across the above-described models for either outcome variable, we present here only the findings from the second model. Details of the full series of models are available upon request. In all models, engagement status was used as a training variable for class membership determination, which was known in the intervention group but missing in the control group. The intercept growth parameter represents the initial level of GPA or school absences in sixth grade. The final model is shown in Fig. 2.
Fig. 2.

CACE model with covariates and categorical outcomes
Note: Dashed lines indicate that effect of intervention on growth parameter is 0 if c=0
Results
Descriptive Analyses
Descriptive statistics for GPA and school absences from grades 6 through 11 are shown in Table 1, and correlations between variables are presented in Table 2. As expected, during the transition to high school there is a general decline in GPA and increase in absence rate. Both GPA and absence rate are correlated in the expected direction with the predictors in Table 2.
Table 1.
Descriptive statistics for GPA and school absences
| 6th grade | 7th grade | 8th grade | 9th grade | 10th grade | 11th grade | ||
|---|---|---|---|---|---|---|---|
| Control | GPA | 2.65 | 2.48 | 2.59 | 2.16 | 2.19 | 2.38 |
| Mean (SD) | (0.89) | (1.00) | (1.00) | (1.12) | (1.07) | (1.04) | |
| Absences | 13.14 | 13.52 | 13.82 | 12.89 | 14.68 | 14.14 | |
| Mean (SD) | (11.96) | (11.90) | (12.78) | (13.10) | (14.74) | (16.69) | |
| Intervention nonengagers | GPA | 2.79 | 2.64 | 2.62 | 2.86 | 2.35 | 2.45 |
| Mean (SD) | (0.90) | (1.00) | (1.18) | (1.05) | (1.18) | (1.18) | |
| Absences | 11.61 | 12.61 | 13.22 | 12.52 | 14.59 | 12.72 | |
| Mean (SD) | (11.41) | (11.93) | (13.24) | (15.57) | (16.48) | (13.32) | |
| Intervention engagers | GPA | 2.56 | 2.33 | 2.42 | 1.97 | 2.15 | 2.32 |
| Mean (SD) | (0.80) | (0.91) | (1.00) | (1.08) | (1.06) | (1.09) | |
| Absences | 12.64 | 13.93 | 13.09 | 13.46 | 15.9 | 13.89 | |
| Mean (SD) | (10.13) | (11.62) | (12.63) | (13.03) | (17.43) | (16.57) |
Table 2.
Correlations between predictors and GPA or school absences
| 6th grade GPA | 7th grade GPA | 8th grade GPA | 9th grade GPA | 10th grade GPA | 11th grade GPA | |
|---|---|---|---|---|---|---|
| Intervention assignment | 0.05 | 0.04 | −0.01 | 0.02 | 0.05 | 0.02 |
| Child gender | 0.19* | 0.22* | 0.17* | 0.13* | 0.12* | 0.15* |
| Ethnicity | −0.32* | −0.27* | −0.28* | −0.31* | −0.28* | −0.21* |
| Family conflict | −0.24* | −0.20* | −0.20* | −0.18* | −0.12* | −0.11* |
| Deviant peers | −0.30* | −0.28* | −0.24* | −0.21* | −0.18* | −0.12* |
| Teacher risk | −0.60* | −0.53* | −0.50* | −0.42* | −0.42* | −0.31* |
| Biological father presence | 0.26* | 0.21* | 0.20* | 0.19* | 0.22* | 0.19* |
| Antisocial behavior | −0.37* | −0.33* | −0.33* | −0.26* | −0.25* | −0.17* |
| Substance use | −0.18* | −0.18* | −0.15* | −0.14* | −0.11* | −0.08 |
| 6th grade absences | 7th grade absences | 8th grade absences | 9th grade absences | 10th grade absences | 11th grade absences | |
| Intervention assignment | −0.05 | −0.02 | −0.03 | −0.01 | 0.01 | −0.04 |
| Child gender | −0.01 | 0.02 | 0.00 | 0.02 | 0.08* | 0.02 |
| Ethnicity | 0.14* | 0.12* | 0.14* | 0.12* | 0.15* | 0.09* |
| Family conflict | 0.14* | 0.11* | 0.10* | 0.12* | 0.13* | 0.09* |
| Deviant peers | 0.23* | 0.27* | 0.16* | 0.14* | 0.13* | 0.05 |
| Teacher risk | 0.28* | 0.29* | 0.17* | 0.16* | 0.15* | 0.05 |
| Biological father presence | −0.19* | −0.14* | −0.19* | −0.12* | −0.18* | −0.09* |
| Antisocial behavior | 0.24* | 0.24* | 0.20* | 0.18* | 0.16* | 0.05 |
| Substance use | 0.16* | 0.18* | 0.12* | 0.13* | 0.14* | 0.03 |
Preliminary analyses focused on discriminating the families within the intervention group who engaged in the FCU from those who did not (engagers versus nonengagers). As shown in Table 3, observed engagement with intervention in the intervention condition was significantly related to the likelihood of biological fathers being absent from the home, youth reports of elevated family conflict and deviant peer affiliation, and teacher reports of elevated risk behaviors at school. The analysis of covariates of engagement suggests that those parents most likely to engage in the FCU were the most vulnerable and experiencing the most difficulty.
Table 3.
Comparison of engager and nonengager families, for families randomly assigned to the intervention condition
| Nonengagers (n=385) | Compliers (n=115) | Omnibus test | |
|---|---|---|---|
| Female gender (%) | 44.9 | 51.3 | χ2 (df=1)=1.44, ns |
| Ethnic minority status (%) | 55.6 | 62.6 | χ2 (df=1)=1.78, ns |
| Biological dad present (%) | 60 | 40 | χ2 (df=1) = 14.72, p<0.05 |
| 6th grade parental monitoring (M, SD) | 3.97 (.98) | 3.97 (1.06) | F(1,489)=0.00, n.s. |
| 6th grade deviant peers (M, SD) | 0.84 (.94) | 1.25 (1.28) | F(1,488) = 13.81, p<0.05 |
| 6th grade substance use (M, SD) | 0.00 (.88) | 0.16 (1.06) | F(1,488)=2.71, n.s. |
| 6th grade family conflict (M, SD) | 0.66 (1.05) | 1.01 (1.26) | F(1,489)=9.05, p<0.05 |
| 6th grade antisocial behavior (M, SD) | 1.41 (.65) | 1.51 (.56) | F(1,489)=1.96, n.s. |
| 6th grade teacher report of risk (M, SD) | 1.79 (.85) | 2.13 (.91) | F(1,498) = 14.17, p<0.05 |
Only participants randomly assigned to the intervention are included in these analyses, because engagement status is not observable in the control condition.
Unconditional latent growth models were examined for both GPA and school absences to determine the parameters needed to adequately describe change trajectories. For both GPA and school absences, models with intercept, slope, and quadratic slope parameters provided good fit to the data. The unconditional GPA model yielded significant intercept (estimate=2.80, SE=0.04) and slope (estimate=–0.10, SE=0.02) parameters and a nonsignificant quadratic slope parameter (estimate=0.003, SE=0.004). Significant residual variation in all three parameters was found (intercept estimate=0.65, SE=0.06; slope estimate=0.06, SE=0.02; quadratic slope estimate=0.003, SE=0.001), indicating significant variability that could be related to covariates in subsequent models.
The unconditional school absence model yielded a significant intercept (estimate=12.59, SE=0.38) parameter but nonsignificant slope (estimate=0.51, SE=0.33) and quadratic slope (estimate=–0.05, SE=0.06) parameters. Significant residual variation in all three parameters was found (intercept estimate=84.99, SE=8.72; slope estimate= 43.46, SE=5.87; quadratic slope estimate=1.92, SE=0.24), indicating significant variability that could be related to covariates in subsequent models.
CACE Model Results
Because CACE analysis is a mixture model, typical estimates of model fit such as the chi-square test are not available. One index of the quality of classification of the trajectory groups within the model is represented by entropy, which is a summary measure of the probability of membership in the most-likely class for each individual (i.e., in the engager or nonengager class). Possible values range from 0 to 1.0, with values closer to 1.0 representing better classification (Muthén and Muthén 2008). Nagin (2005) has recommended a cutoff value of .70 as indicative of acceptable entropy. In the current analyses, entropy was good (entropy=0.92). Results for predictors of engagement status are shown in Table 4, and the results for within-class variation in GPA and school absence trajectories are shown in Tables 5 and 6, respectively.
Table 4.
Final CACE model results for the prediction of compliance class membership
| Class membership Engager vs. nonengager Logit (SE) | |
|---|---|
| Intervention status | Fixed at 0 |
| Gender | −0.28 (.21) |
| Ethnicity: European American | 0.11 (.30) |
| Ethnicity: African American | 0.00 (.32) |
| Ethnicity: Hispanic | 0.42 (.51) |
| Biological dad present (6th grade) | 0.70 (0.21)* |
| Parental monitoring (6th grade) | −0.10 (0.13) |
| Deviant peers (6th grade) | −0.14 (0.10) |
| Substance use (6th grade) | 0.00 (0.03) |
| Family conflict (6th grade) | −0.20 (0.09)* |
| Teacher report of risk (6th grade) | −0.28 (0.13)* |
| Antisocial behavior (6th grade) | −0.04 (0.23) |
| Parameter threshold | 2.11 (0.47)* |
p<.05
Table 5.
Final CACE model results for grade point averages
| Within-class variation | ||||||
|---|---|---|---|---|---|---|
| Nonengager class | Engager class | |||||
| InterceptEst. (SE) | SlopeEst. (SE) | Slope2Est. (SE) | InterceptEst. (SE) | SlopeEst. (SE) | Slope2Est. (SE) | |
| Intervention status | Fixed at 0 | Fixed at 0 | Fixed at 0 | Fixed at 0 | −.30 (.14)* | .12 (.03)* |
| Gender | 0.10 (0.05)* | −0.01 (0.04) | 0.00 (0.01) | 0.24 (0.13) | −0.05 (0.09) | 0.02 (0.02) |
| Ethnicity: European American | 0.08 (0.06) | −0.03 (0.05) | 0.00 (0.01) | 0.14 (0.17) | −0.06 (0.12) | 0.02 (0.03) |
| Ethnicity: African American | −0.32 (0.07)* | 0.00 (0.06) | 0.01 (0.01) | 0.01 (0.17) | 0.07 (0.11) | −0.02 (0.03) |
| Ethnicity: Hispanic | −0.43 (0.10)* | −0.04 (0.10) | 0.01 (0.02) | −0.38 (0.37) | 0.48 (0.28) | −0.12 (0.06)* |
| Biological dad present (6th grade) | 0.19 (0.05)* | −0.03 (0.05) | 0.01 (0.01) | 0.23 (0.14) | −0.14 (0.10) | 0.02 (0.02) |
| Parental monitoring (6th grade) | 0.14 (0.03)* | −0.04 (0.03) | 0.01 (0.01) | 0.17 (0.06)* | 0.06 (0.05) | −0.01 (0.01) |
| Deviant peers (6th grade) | −0.01 (0.03) | −0.01 (0.03) | 0.00 (0.01) | −0.07 (0.07) | 0.05 (0.05) | −0.01 (0.01) |
| Substance use (6th grade) | −0.01 (0.01) | −0.01 (0.01) | 0.00 (0.00) | 0.02 (0.02) | 0.01 (0.02) | 0.00 (0.00) |
| Family conflict (6th grade) | −0.06 (0.03)* | 0.03 (0.03) | −0.01 (0.01) | −0.03 (0.06) | −0.03 (0.05) | 0.00 (0.01) |
| Teacher report of risk (6th grade) | −0.50 (0.03)* | −0.03 (0.03) | 0.02 (0.01)* | −0.38 (0.08)* | −0.03 (0.06) | 0.01 (0.01) |
| Antisocial behavior (6th grade) | −0.04 (0.06) | −0.04 (0.07) | 0.01 (0.01) | 0.03 (0.12) | −0.03 (0.12) | 0.01 (0.03) |
| Parameter intercept | 3.67 (0.12)* | −0.12 (0.11) | −0.03 (0.02) | 2.95 (0.24)* | 0.25 (0.24) | −0.14 (0.05)* |
| Parameter residual variance | 0.32 (0.03)* | 0.09 (0.02)* | 0.003 (0.001)* | 0.32 (0.03)* | 0.09 (0.02)* | 0.003 (0.001)* |
Slope2 refers to the quadratic slope parameter
p<.05
Table 6.
Final CACE model results for school absences
| Within-class variation | ||||||
|---|---|---|---|---|---|---|
| Nonengager class | Engager class | |||||
| InterceptEst. (SE) | SlopeEst. (SE) | Slope2Est. (SE) | InterceptEst. (SE) | SlopeEst. (SE) | Slope2Est. (SE) | |
| Intervention status | Fixed at 0 | Fixed at 0 | Fixed at 0 | Fixed at 0 | 8.26 (1.70)* | −3.36 (.49)* |
| Gender | 1.10 (0.77) | 0.33 (0.72) | −0.07 (0.15) | 2.54 (2.21) | 0.69 (1.51) | −0.38 (0.33) |
| Ethnicity: European American | 1.07 (0.91) | −1.76 (1.02) | 0.27 (0.20) | 0.55 (3.72) | 0.53 (2.28) | −0.29 (0.38) |
| Ethnicity: African American | 2.17 (0.131) | −1.76 (1.27) | 0.21 (0.24) | −1.84 (4.01) | −0.51 (2.49) | 0.30 (0.38) |
| Ethnicity: Hispanic | 3.77 (1.93) | −0.65 (2.38) | 0.19 (0.45) | 0.84 (4.69) | −5.06 (3.14) | 1.53 (0.66)* |
| Biological dad present (6th grade) | −1.96 (0.89)* | −1.09 (0.83) | 0.20 (0.16) | −4.48 (2.73) | 1.31 (1.62) | −0.10 (0.33) |
| Parental monitoring (6th grade) | −0.85 (0.51)* | 0.67 (0.48) | −0.13 (0.10) | 0.23 (1.18) | −0.19 (0.64) | 0.06 (0.12) |
| Deviant peers (6th grade) | 0.36 (0.63) | 0.41 (0.63) | −0.11 (0.12) | 2.77 (2.05) | −1.12 (0.94) | 0.10 (0.14) |
| Substance use (6th grade) | 0.32 (0.20) | −0.11 (0.22) | 0.01 (0.04) | −0.20 (0.35) | 0.42 (0.23) | −0.04 (0.05) |
| Family conflict (6th grade) | 0.58 (0.56) | −0.17 (0.55) | 0.06 (0.11) | −2.48 (1.61) | 1.20 (0.81) | −0.15 (0.15) |
| Teacher report of risk (6th grade) | 3.12 (.75)* | −.25 (.73) | −.05 (.14) | 2.63 (1.57)* | −.83 (1.16) | .05 (.21) |
| Antisocial behavior (6th grade) | 0.26 (1.45) | 1.55 (1.30) | −0.41 (0.24) | 0.61 (2.60) | 0.33 (2.15) | −0.24 (0.42) |
| Parameter intercept | 4.83 (2.11)* | 1.58 (2.35) | 0.06 (0.46) | 11.25 (5.86)* | −9.45 (4.56)* | 3.99 (.87)* |
| Parameter residual variance | 58.40 (10.86)* | 30.91 (8.19)* | 1.13 (.31)* | 58.40 (10.86)* | 30.91 (8.19)* | 1.13 (.31)* |
Slope2 refers to the quadratic slope parameter
p<.05
Predictors of Engagement
Results for predictors of engagement followed a logistic regression framework, and the extent to which variables discriminate membership in the engager versus nonengager classes was examined. Engagement was predicted by greater likelihood of biological father absence from the youth's home, more frequent family conflict, and elevated teacher reports of risk in sixth grade.
Predictors of Within-Class Variation
It is particularly important to note that random assignment to the intervention condition was predictive of the level of change in both GPA and school absences. The effects of the intervention on grades and absences for families defined as engagers are presented in Figs. 3 and 4. As shown, within the engager class, family participation in the FCU reduced growth in school absences as well as declines in GPA from sixth through 11th grade.
Fig. 3.

CACE results of intervention effect on changes in GPA
Fig. 4.
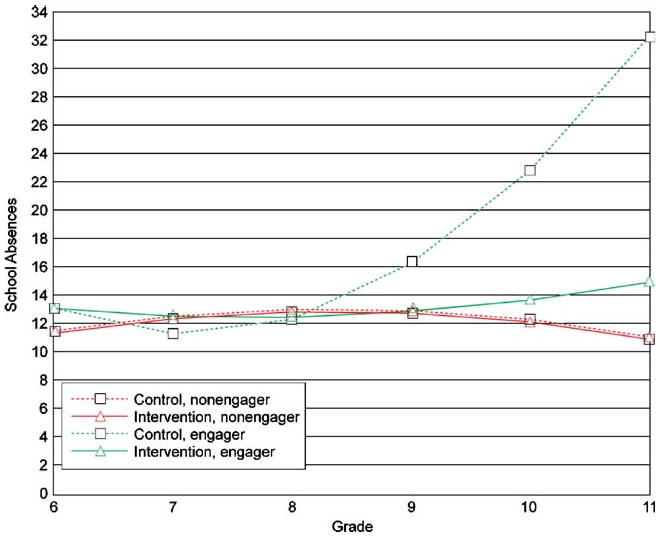
CACE results of intervention effect on changes in school absences
Additional results are important to highlight for each domain of academic performance. For GPA, sixth grade GPA in the nonengager class was positively related to male gender, the presence of biological fathers in the home (i.e., youth residing with biological fathers had higher initial GPAs), and to parental monitoring efforts. Conversely, sixth grade GPA was negatively related to African American or Hispanic ethnicity, elevated family conflict, and teacher perceptions of engagement in risky behavior. Sixth grade GPA in the engager class was negatively related only to teachers' perceptions of school-risk behavior. In the engager class, the quadratic slope for GPA was negatively related to Hispanic ethnicity (i.e., Hispanic youth showed greater declines in GPAs over time, relative to non-Hispanic youth).
For school absences, sixth grade absences in the nonengager class were negatively related to the presence of biological fathers in the home and to parental monitoring, and were positively related to teachers' reports of school risk in sixth grade. In the engager class, sixth grade school absences were positively related only to teachers' reports of risk behavior, and the quadratic slope was positively related to Hispanic ethnicity (i.e., Hispanic youth showed greater acceleration in the number of school absences over time, relative to non-Hispanic youth).
Follow-up analyses examined the potential for high-influence cases to affect the analytic results by inspecting the log-likelihood distance influence measure for each case (Cook and Weisberg 1982). Although there are no fixed cutoff values for determining high-influence cases, we identified five cases whose influence values were clearly outliers with respect to the distribution of log-likelihood distance values. Analyses were rerun with these cases removed from these data sets, and results were nearly identical.
Discussion
This study focused on the long-term academic outcomes associated with the FCU intervention model that included a comprehensive family assessment, support for family management skills, and interventions targeted at helping parents reduce youth high-risk behavior. We found that over time, our family-centered, school-based approach to intervention had a positive impact on both academic achievement and attendance in school. In particular, youth whose families received our intervention showed a GPA that remained stable from middle school to high school. GPA for youth in our high-risk control group declined substantially during the transition to high school and into the high school years. Similarly, the high-risk control group showed a substantial growth in absence rate from middle school to high school, whereas in our intervention group an acceleration in absence rate was prevented.
These results have important implications for the delivery of parenting interventions to at-risk and high-risk youth. Ample research supports the implementation of parenting skills interventions across early, middle, and late childhood as a means to reduce problem behavior and enhance family management skills (Kazdin 2003). Parenting programs that focus on enhancing the skills of parents as a means to reduce child problem behavior are the most successful empirically based interventions for youth and families (Weiss et al. 1995). Parenting skills training can be administered as an individual-level intervention, a group intervention, or a school-based intervention. Evidence in the literature supports each of these approaches to service delivery. Our results suggest that family-centered interventions can have an impact not only on problem behaviors at home, but also on school behaviors such as attendance and academic achievement. As schools are faced with increasing rates of mental health problems and limited resources, the infusion of family-centered approaches to mental health problems may be the most effective way to reduce problem behavior and increase school engagement.
In each model tested, we entered predictors of engagement to examine the risk factors associated with participation in intervention. Consistent with our other published findings from this body of research (Connell et al. 2007; Stormshak et al. 2005), we found that families who engaged most regularly in our intervention were those with a number of risk factors, including single parenting, elevated family conflict, and elevated number of teacher ratings of risk. Given our adaptive approach to intervention, this finding is important because it suggests that our model did motivate and target the at-risk and high-risk portion of our sample.
Interestingly, we did not find that ethnicity predicted engagement in intervention. These findings are also significant because they suggest that our intervention did successfully engage diverse families into the intervention program. Providing interventions that are culturally competent is significant to maintaining engagement of diverse families (Hudley and Taylor 2006). This is particularly critical when working with parenting and family management skills, which are tightly linked to family values, communities, and culture (Yasui and Dishion 2007). Our EcoFIT approach to intervention is tailored to individual family strengths, areas of growth, and parenting values and allows adaptation of content to meet the needs of diverse families (Dishion and Stormshak 2007).
Previous family-centered intervention research has made little effort to examine academic outcomes, especially those in the adolescent years. There are a variety of reasons for this lack of findings, including that longitudinal academic data are time consuming and expensive to collect. In light of these challenges, many parenting programs have focused their resources on measuring proximal outcomes such as improved parenting over more distal outcomes such as academic achievement. Intervention programs that have included academic tutoring or other academic support along with parent skills training have reported significant results (e.g., Leve and Chamberlain 2005; Tolan et al. 2004). Outcomes associated with different intervention components cannot be tested in a multifaceted intervention model, and in this literature these circumstances have limited our ability to understand the impact of parenting interventions on school engagement. Because we did not provide additional academic tutoring or other interventions to support academic engagement, our results suggest that a family-centered intervention focused on improving parenting skills can have a positive impact on academic outcomes.
Engaging Families in Family-Centered Interventions
Engaging high-risk youth and their families in an intervention directed at changing parenting skills and family management can be a challenging endeavor. In this project, we successfully engaged 25% of our intervention group in the FCU intervention, which is a selected intervention for at-risk and high-risk families. Although a low rate of participation is expected when the goal is to provide intervention to at-risk and high-risk families, our tailored approach to intervention enhanced the rates. For many families, considerations such as childcare, work schedules, and the time commitment required to attend parenting groups can reduce or prohibit participation, and although some parenting programs offer monetary compensation, food, and childcare to parents, amenities such as these are costly for schools or community agencies. In addition, parents' own interpersonal problems such as depression, substance use, and limited resources can affect intervention participation and outcomes (Smith et al. 2005; Webster-Stratton and Hammond 1990). Recruitment and attendance concerns such as these have led to the development of brief parenting interventions (Lim et al. 2005; Stormshak et al. 2002) and tailored, individualized family interventions (Dishion and Stormshak 2007).
School-Based Mental Health
The provision of health and mental health services in schools has been increasing during the past 20 years, and a significant amount of literature now exists about a range of school-based mental health programs. Unfortunately most of the programs focus exclusively on youth and neglect the contribution of the family to mental health problems, and they overlook empirically based interventions (Shirk and Jungbluth 2008). Furthermore, school conditions, support from school staff, and teachers' skill level all affect the quality and implementation of mental health programs in schools (Atkins et al. 2008; Hughes et al. 2005; Payne et al. 2006). In light of these challenges, school-based mental health research supports the implementation of tailored, empirically based family interventions in schools to efficiently address the mental health needs of at-risk youth.
Limitations and Future Directions
In this study, we assume that the underlying mechanism for change was the impact our intervention had on parenting strategies such as homework monitoring, implementing skills to alleviate family conflict, and positive parenting. One limitation of this study was insufficient opportunity to directly test this mediational model; however, we have found in previous research that our intervention improves positive parenting strategies (Dishion et al. 2003). We were also limited in our ability to run separate models by race and gender and to test the intervention separately across these groups. In addition, some of the risk indices are not ideal. Most important, more sensitive measures of family configuration were not collected, and the “paternal presence” variable used in this study is not a clear indicator of the role of fathers in the lives of these youth. Given that this family configuration variable emerges as an important predictor of family engagement in treatment, it is important for future studies to examine with more sensitivity the role of family configuration in the treatment engagement process. The “family conflict” variable is also broad and is limited by having used only youth self-report as a measure. Future studies could differentiate between interparental conflict and conflict between parents and youth.
Finally, it is regrettable that a change in the district's record keeping precluded the collection of 11th grade GPA for the second cohort of youth in this study. Our confidence in the intervention effects on GPA is buttressed by the fact that (a) differences in the two cohorts were not found at earlier waves of data collection, and (b) school absence data were not affected by the changes in record keeping, yet also revealed intervention effects in the expected direction.
These findings are quite relevant for policy decisions regarding the potential viability of delivering mental health services in the public school context, especially when those services are family centered, brief, and focused on empowering parents to promote academic success. Clearly, mental health services in public school settings that establish collaborative linkages between parents and teachers will be enhanced by school structural changes and improved communication systems and technology (e.g., Internet), which will ultimately optimize success for both children and their families for generations to come.
Acknowledgments
This project was supported by grants DA07031 and DA13773 from the National Institute on Drug Abuse and DA018760 from the National Institutes of Health to the third author, and DA018374 to the first author. We acknowledge the contribution of the Project Alliance staff, Portland Public Schools, and the participating youth and families. We wish to thank Booil Jo, Ph.D., for consultation and insights on the analysis of intervention engagement.
Contributor Information
Elizabeth A. Stormshak, Email: bstorm@uoregon.edu, Counseling Psychology Program, Child and Family Center, University of Oregon, 195 West 12th Avenue, Eugene, OR 97401-3408, USA
Arin Connell, Email: arin.connell@case.edu, Psychology, Case Western Reserve University, Cleveland, OH, USA.
Thomas J. Dishion, Email: dishion@uoregon.edu, Psychology and School Psychology, Child and Family Center, University of Oregon, 195 West 12th Avenue, Eugene, OR 97401-3408, USA
References
- Angrist J, Imbens G, Rubin D. Identification of causal effects using instrumental variables. Journal of the American Statistical Association. 1996;91:444–455. doi: 10.2307/2291629. [DOI] [Google Scholar]
- Atkins MS, Frazier SL, Leathers SJ, Graczyk PA, Talbott E, Jakobsons L, et al. Teacher key opinion leaders and mental health consultation in low-income urban schools. Journal of Consulting and Clinical Psychology. 2008;76:905–908. doi: 10.1037/a0013036. [DOI] [PubMed] [Google Scholar]
- August GJ, Realmuto GM, Hektner JM, Bloomquist ML. An integrated components preventive intervention for aggressive elementary school children: The Early Risers program. Journal of Consulting and Clinical Psychology. 2001;69:614–626. doi: 10.1037/0022-006X.69.4.614. [DOI] [PubMed] [Google Scholar]
- Bronfenbrenner U. Ecological systems theory. In: Vasta R, editor. Annals of child development: Vol 6 Six theories of child development: Revised formulations and current issues. London: JAI; 1989. pp. 187–249. [Google Scholar]
- Brown BB. The role of peer groups in adolescents' adjustment to secondary school. In: Berndt TJ, Ladd GW, editors. Peer relationships in child development. Oxford; England: Wiley: 1989. pp. 188–215. [Google Scholar]
- Cicchetti D, Toth SL. The role of developmental theory in prevention and intervention. Development and Psychopathology. 1992;4:489–493. doi: 10.1017/S0954579400004831. [DOI] [PubMed] [Google Scholar]
- Coie JD, Watt NF, West G, Hawkins JD, Asarnow JR, Markman HJ, et al. The science of prevention: A conceptual framework and some directions for a national research program. The American Psychologist. 1993;48:1013–1022. doi: 10.1037/0003-066X.48.10.1013. [DOI] [PubMed] [Google Scholar]
- Conduct Problems Prevention Research Group. Evaluation of the first 3 years of the Fast Track prevention trial with children at high risk for adolescent conduct problems. Journal of Abnormal Child Psychology. 2002;30:19–35. doi: 10.1023/A:1014274914287. [DOI] [PubMed] [Google Scholar]
- Connell A, Dishion TJ. Reducing depression among at-risk early adolescents: Three-year effects of a family-centered intervention embedded within schools. Journal of Family Psychology. 2008;22:574–585. doi: 10.1037/0893-3200.22.3.574. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Connell A, Dishion TJ, Yasui M, Kavanagh K. An adaptive approach to family intervention: Linking engagement in family-centered intervention to reductions in adolescent problem behavior. Journal of Consulting and Clinical Psychology. 2007;75:568–579. doi: 10.1037/0022-006X.75.4.568. [DOI] [PubMed] [Google Scholar]
- Cook R, Weisberg S. Residuals and influence in regression. New York: Chapman and Hall; 1982. [Google Scholar]
- Dishion TJ, Andrews D. Preventing escalations in problem behaviors with high-risk young adolescents: Immediate and 1-year outcomes. Journal of Consulting and Clinical Psychology. 1995;63:538–548. doi: 10.1037/0022-006X.63.4.538. [DOI] [PubMed] [Google Scholar]
- Dishion TJ, Kavanagh K. Intervening in adolescent problem behavior: A family-centered approach. New York: Guilford; 2003. [Google Scholar]
- Dishion TJ, Loeber R. Adolescent marijuana and alcohol use: The role of parents and peers revisited. The American Journal of Drug and Alcohol Abuse. 1985;11:11–25. doi: 10.3109/00952998509016846. [DOI] [PubMed] [Google Scholar]
- Dishion TJ, McMahon RJ. Parental monitoring and the prevention of problem behavior: A conceptual and empirical reformulation. Research meeting on drug abuse prevention through family interventions. In: Ashery RS, editor. NIDA research monograph. Vol. 177. Washington, DC: Government Printing Office; 1998. [Google Scholar]
- Dishion TJ, Stormshak E. Intervening in children's lives: An ecological, family-centered approach to mental health care. Washington, DC: APA Books; 2007. [Google Scholar]
- Dishion TJ, Nelson SE, Kavanagh K. The Family Check-Up for high-risk adolescents: Preventing early-onset substance use by parent monitoring. In: Lochman JE, Salekin R, editors. Behavior Therapy. Vol. 34. 2003. pp. 553–571. Behavior-oriented interventions for children with aggressive behavior and/or conduct problems [Special Issue] [Google Scholar]
- Dishion TJ, Nelson SN, Bullock BM. Premature adolescent autonomy: Parent disengagement and deviant peer process in the amplification of problem behavior. In: Kiesner J, Kerr M, editors. Journal on Adolescence. Vol. 27. 2004. pp. 515–530. Peer and family processes in the development of antisocial and aggressive behavior [Special Issue] [DOI] [PubMed] [Google Scholar]
- Dishion TJ, Bullock BM, Kiesner J. Vicissitudes of parenting adolescents: Daily variations in parental monitoring and the early emergence of drug use. In: Kerr M, Stattin H, Engels RCME, editors. What can parents do? New insights into the role of parents in adolescent problem behavior. Chichester, England: Wiley; 2008a. pp. 113–133. [Google Scholar]
- Dishion TJ, Shaw DS, Connell AM, Gardner F, Weaver CM, Wilson MN. The Family Check-Up with high-risk indigent families: Preventing problem behavior by increasing parents' positive behavior support in early childhood. Child Development. 2008b;79:1395–1414. doi: 10.1111/j.1467-8624.2008.01195.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eccles JS, Midgley C, Wigfield A, Buchanan CM, Reuman D, Flanagan C, et al. Development during adolescence: The impact of stage–fit on adolescents' in schools and families. The American Psychologist. 1993;48:90–101. doi: 10.1037/0003-066X.48.2.90. [DOI] [PubMed] [Google Scholar]
- Eccles JS, Lord SE, Roeser RW. Round holes, square pegs, rocky roads, and sore feet: The impact of stage–environment fit on young adolescents' experiences in schools and families. In: Cicchetti D, Toth S, editors. Rochester Symposium on Developmental Psychopathology: Adolescence: Opportunities and challenges. Vol. 7. New York: University of Rochester Press; 1995. pp. 47–92. [Google Scholar]
- Forgatch MS, DeGarmo DS. Parenting through change: An effective prevention program for single mothers. Journal of Consulting and Clinical Psychology. 1999;67:711–724. doi: 10.1037/0022-006X.67.5.711. [DOI] [PubMed] [Google Scholar]
- Greenwood GE, Hickman CW. Research and practice in parent involvement: Implications for teacher education. The Elementary School Journal. 1991;91:279–287. doi: 10.1086/461655. [DOI] [Google Scholar]
- Hawkins JD. Academic performance and school success: Sources and consequences. In: Weissberg RP, Gullotta TP, Hampton RL, Ryan BA, Adams GR, editors. Healthy children 2010: Enhancing children's wellness. Thousand Oaks, CA: Sage; 1997. pp. 278–305. [Google Scholar]
- Hawkins JD, Catalano RF, Morrison DM, O'Donnell J, Abbott RD, Day LE. Effects of the first four years on protective factors and problem behaviors. In: McCord J, Tremblay RE, editors. The prevention of antisocial behavior in children. New York: Guilford; 1992. pp. 139–162. [Google Scholar]
- Hawkins JD, Guo J, Hill KG, Battin-Pearson S, Abbott RD. Long-term effects of the Seattle Social Development Intervention on school bonding trajectories. Applied Developmental Science. 2001;5:225–236. doi: 10.1207/S1532480XADS0504_04. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Henggeler S, Schoenwald S, Borduin C, Rowland M, Cunningham P. Multisystemic treatment of antisocial behavior in children and adolescents. New York: Guilford; 1998. [Google Scholar]
- Hill NE, Castellino DR, Lansford JE, Nowlin P, Dodge KA, Bates JE, Pettit GS. Parent academic involvement as related to school behavior, achievement, and aspirations: Demographic variations across adolescence. Child Development. 2004;75:1491–1509. doi: 10.1111/j.1467-8624.2004.00753.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hudley C, Taylor A. What is cultural competence and how can it be incorporated into preventive interventions? In: Guerra NG, Smith EP, editors. Preventing youth violence in a multicultural society. Washington, DC: American Psychological Association; 2006. pp. 249–269. [Google Scholar]
- Hughes JN, Cavell TA, Meehan BT, Zhang D, Collie C. Adverse school context moderates the outcomes of selective interventions for aggressive children. Journal of Consulting and Clinical Psychology. 2005;73:731–736. doi: 10.1037/0022-006X.73.4.731. [DOI] [PubMed] [Google Scholar]
- Imbens GW, Rubin DB. Estimating outcome distributions for compliers in instrumental variables models. The Review of Economic Studies. 1997;64:555–574. doi: 10.2307/2971731. [DOI] [Google Scholar]
- Jo B. Statistical power in randomized intervention studies with noncompliance. Psychological Methods. 2002;7:178–193. doi: 10.1037/1082-989X.7.2.178. [DOI] [PubMed] [Google Scholar]
- Kazdin AE. Problem-solving skills training and parent management training for conduct disorder. In: Kazdin AE, Weisz JR, editors. Evidence-based psychotherapies for children and adolescents. New York: Guilford; 2003. pp. 241–262. [Google Scholar]
- Larson R, Ham M. Stress and “storm and stress” in early adolescence: The relationship of negative events with dysphoric affect. Developmental Psychology. 1993;29:130–140. doi: 10.1037/0012-1649.29.1.130. [DOI] [Google Scholar]
- Leve LD, Chamberlain P. Association with delinquent peers: Intervention effects for youth in the juvenile justice system. Journal of Abnormal Child Psychology. 2005;33:339–347. doi: 10.1007/s10802-005-3571-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lim M, Stormshak EA, Dishion TJ. A one-session intervention for parents of young adolescents: Videotape modeling and motivational group discussion. Journal of Emotional and Behavioral Disorders. 2005;13:194–199. doi: 10.1177/10634266050130040101. [DOI] [Google Scholar]
- Little RJ, Yau LHY. Statistical techniques for analyzing data from prevention trials: Treatment of no-shows using Rubin's causal model. Psychological Methods. 1998;3:147–159. doi: 10.1037/1082-989X.3.2.147. [DOI] [Google Scholar]
- Loeber R, Dishion T. Early predictors of male delinquency: A review. Psychological Bulletin. 1983;94:68–99. doi: 10.1037/0033-2909.94.1.68. [DOI] [PubMed] [Google Scholar]
- Loeber R, Wung P, Keenan K, Giroux B, Stouthamer-Loeber M, van Kammen WB, et al. Developmental pathways in disruptive child behavior. Development and Psychopathology. 1993;5:103–133. doi: 10.1017/S0954579400004296. [DOI] [Google Scholar]
- Lunkenheimer ES, Dishion TJ, Shaw DS, Connell A, Gardner FM, Wilson MN, et al. Collateral benefits of the Family Check-Up on early childhood school readiness: Indirect effects of parents' positive behavior support. Developmental Psychology. 2008;44:1737–1752. doi: 10.1037/a0013858. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mattingly DJ, Prislin R, McKenzie TL, Rodriguez JL, Kayzar B. Evaluating evaluations: The case of parent involvement programs. Review of Educational Research. 2002;72:549–576. doi: 10.3102/00346543072004549. [DOI] [Google Scholar]
- McMahon RJ, Slough N . Conduct Problems Prevention Research Group. Family-based intervention in the fast Track Program. In: Peters RD, McMahon RJ, editors. Preventing childhood disorders, substance abuse, and delinquency. Thousand Oaks, CA: Sage; 1996. pp. 90–110. [Google Scholar]
- Metzler CW, Biglan A, Rusby JC, Sprague JR. Evaluation of a comprehensive behavior management program to improve school-wide positive behavior support. Education & Treatment of Children. 2001;24:448–479. [Google Scholar]
- Miller WR, Rollnick S. Motivational interviewing: Preparing people to change addictive behavior. New York: Guilford; 1991. [Google Scholar]
- Miller WR, Rollnick S. Motivational interviewing: Preparing people for change. 2nd. New York: Guilford; 2002. [Google Scholar]
- Muthén B. Latent variable analysis: Growth mixture modeling and related techniques for longitudinal data. In: Kaplan D, editor. Handbook of quantitative methodology for the social sciences. Newbury Park, CA: Sage; 2004. pp. 345–368. [Google Scholar]
- Muthén LK, Muthén BO. Mplus user's guide. 5th. Los Angeles, CA: Author; 2008. [Google Scholar]
- Nagin D. Group-based modeling of development. Cambridge, MA: Harvard University Press; 2005. [Google Scholar]
- Patterson GR. A guide for the professional for use with living with children and families. Champaign, IL: Research Press; 1975. [Google Scholar]
- Patterson GR, Dishion TJ. Multilevel family process models: Traits, interactions, and relationships. In: Hinde R, Stevenson-Hinde J, editors. Relationships and families: Mutual influences. Oxford, UK: Clarendon; 1988. pp. 283–310. [Google Scholar]
- Patterson GR, Stouthamer-Loeber M. The correlation of family management practices and delinquency. Child Development. 1984;55:1299–1307. doi: 10.2307/1129999. [DOI] [PubMed] [Google Scholar]
- Patterson G, Reid J, Jones R, Conger R. A social learning approach to family intervention: Families with aggressive children. Eugene, OR: Castalia; 1975. [Google Scholar]
- Patterson GR, DeBaryshe BD, Ramsey E. A developmental perspective on antisocial behavior. The American Psychologist. 1989;44:329–335. doi: 10.1037/0003-066X.44.2.329. [DOI] [PubMed] [Google Scholar]
- Payne AA, Gottfredson DC, Gottfredson GD. School predictors of the intensity of implementation of school-based prevention programs: Results from a national study. Prevention Science. 2006;7:225–237. doi: 10.1007/s11121-006-0029-2. [DOI] [PubMed] [Google Scholar]
- Peterson PL, Hawkins JD, Abbott RD, Catalano RF. Disentangling the effects of parental drinking, family management, and parent alcohol norms on current drinking by black and white adolescents. Journal of Research on Adolescence. 1994;4:203–277. doi: 10.1207/s15327795jra0402_3. [DOI] [Google Scholar]
- Pettit GS, Bates JE, Dodge KA. Family interaction patterns and children's conduct problems at home and school: A longitudinal perspective. School Psychology Review. 1993;22:403–420. [Google Scholar]
- Sameroff AJ. Dialectical processes in developmental psychopathology. In: Sameroff A, Lewis J, Miller SM, editors. Handbook of developmental psychopathology. 2nd. New York: Kluwer; 2000. pp. 23–40. [Google Scholar]
- Shirk SR, Jungbluth NJ. School-based mental health checkups: Ready for practical action. Clinical Psychology: Science and Practice. 2008;5:217–223. doi: 10.1111/j.1468-2850.2008.00131.x. [DOI] [Google Scholar]
- Smith KE, Landry SH, Swank PR. The influence of decreased parental resources on the efficacy of a responsive parenting intervention. Journal of Consulting and Clinical Psychology. 2005;73:711–720. doi: 10.1037/0022-006X.73.4.711. [DOI] [PubMed] [Google Scholar]
- Soberman LT. Psychometric validation of a brief teacher screening instrument. Eugene: University of Oregon; 1994. [Google Scholar]
- Spoth R, Randall GK, Shin C. Experimental support for a model of partnership-based family intervention effects on long-term academic success. School Psychology Quarterly. 2008;23:70–89. doi: 10.1037/1045-3830.23.1.70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stoolmiller MS. Antisocial behavior, delinquent peer association, and unsupervised wandering for boys: Growth and change from childhood to early adolescence. Multivariate Behavioral Research. 1994;29:263–288. doi: 10.1207/s15327906mbr2903_4. [DOI] [PubMed] [Google Scholar]
- Stormshak EA, Bierman KL, McMahon RJ, Lengua L Conduct Problems Prevention Research Group. Parenting practices and child disruptive behavior problems in early elementary school. Journal of Child Clinical Psychology. 2000;29:17–29. doi: 10.1207/S15374424jccp2901_3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stormshak EA, Kaminski R, Goodman MR. Enhancing the parenting skills of Head Start families during the transition to kindergarten. Prevention Science. 2002;3:223–234. doi: 10.1023/A:1019998601210. [DOI] [PubMed] [Google Scholar]
- Stormshak EA, Dishion TJ, Light J, Yasui M. Implementing family-centered interventions within the public middle school: Linking service delivery change to change in problem behavior. Journal of Abnormal Child Psychology. 2005;33:723–733. doi: 10.1007/s10802-005-7650-6. [DOI] [PubMed] [Google Scholar]
- Tolan P, Gorman-Smith D, Henry D. Supporting families in a high-risk setting: Proximal effects of the SAFE children preventive intervention. Journal of Consulting and Clinical Psychology. 2004;72:855–869. doi: 10.1037/0022-006X.72.5.855. [DOI] [PubMed] [Google Scholar]
- Webster-Stratton C. Strategies for helping early school-aged children with oppositional defiant and conduct disorders: The importance of home–school partnerships. School Psychology Review. 1993;22:437–457. [Google Scholar]
- Webster-Stratton C, Hammond M. Predictors of treatment outcome in parent training for families with conduct problem children. Behavior Therapy. 1990;21:319–337. doi: 10.1016/S0005-7894(05)80334-X. [DOI] [Google Scholar]
- Weiss JR, Weiss B, Han SS, Granger DA, Morton T. Effects of psychotherapy with children and adolescents revisited: A meta-analysis of treatment outcome studies. Psychological Bulletin. 1995;117:450–468. doi: 10.1037/0033-2909.117.3.450. [DOI] [PubMed] [Google Scholar]
- Yasui M, Dishion TJ. The ethnic context of child and adolescent problem behavior: Implications for child and family interventions. Clinical Child and Family Psychology Review. 2007;10:137–179. doi: 10.1007/s10567-007-0021-9. [DOI] [PubMed] [Google Scholar]