

Abstract
A number of techniques have been described to remove rectal foreign bodies. In this report, a novel endoscopic technique using a pneumatic dilatation balloon normally used in achalasia patients is presented. In addition, a systematic review of the literature was performed for non-operative methods to remove foreign bodies from the rectum. These results are summarised, presented as a practical at-a-glance overview and a flow chart is offered to guide the clinician in treatment decisions. The design of the flow chart was based on the aims to treat the patient preferably on an outpatient basis with minimally invasive techniques and if possible under conscious sedation rather than general anaesthesia.
Keywords: Foreign body, Rectum, Rectal, Removal, Review
INTRODUCTION
Intentional or unintentional insertion of rectal foreign bodies is not uncommon and often poses a serious challenge on the clinician. Objects can be inserted for diagnostic or therapeutic purposes, or self-treatment of anorectal disease, by criminal assault and accident or, most commonly, for sexual purposes. Most patients with rectal foreign bodies present to the emergency room usually after efforts to remove the object at home. Many endoscopic and surgical techniques to remove rectal foreign bodies have been described in the literature and the reported variety in foreign bodies is as large as the number of techniques used to remove them[1–46]. The descriptions in the available literature are anecdotic and consist largely of case reports or case series[1–46].
In this report, a novel endoscopic technique to remove rectal foreign bodies using a pneumatic dilatation balloon normally used in achalasia patients is presented. In addition, a systematic review of the literature was performed for non-operative methods to remove foreign bodies from the rectum. These results are summarized and a practical flow chart is presented to guide the clinician in his or her treatment decisions.
CASE REPORT
A 19-year-old man presented at the emergency department, 12 h after insertion of a high pressure container with tanning spray into his rectum. A plain abdominal radiograph (Figure 1) showed the container in the rectosigmoid region. There were no signs of perforation. A flexible sigmoidoscopy was performed under conscious sedation. The object was located just above the rectosigmoid junction. The container could not be extracted by bimanual manipulation. An attempt to remove the object with conventional endoscopic instruments, such as polypectomy snares, was unsuccessful.
Figure 1.

Plain abdominal radiograph showing the foreign body impacted in the rectosigmoid.
The sigmoidoscope could be passed alongside the foreign body to its proximal end. A guide wire was left behind with the sigmoidoscope removed. Subsequently, a 40 mm pneumatic dilatation balloon (Rigiflex®, Boston Scientific), normally used in achalasia patients, was inserted over the guide wire and inflated just above the container (Figure 2). For safety purposes, the sigmoidoscope was reintroduced alongside the catheter of the balloon to allow endoscopic visual control of the distal end of the container in the rectum. Gentle traction was exerted on the balloon catheter, and the container was successfully removed under fluoroscopic and endoscopic control (Figure 3).
Figure 2.

Lateral view of abdominal radiograph depicting the foreign body with the achalasia balloon inflated just above the container.
Figure 3.

The removed container.
DISCUSSION
A large number of surgical and non-surgical techniques have been described to remove rectal foreign bodies[1–46]. Our case illustrates that for removal of foreign bodies retained in the rectosigmoid, extraction with a pneumatic dilatation balloon, inflated above the foreign body, may be an elegant and safe alternative when conventional techniques fail. Our technique has not been described before as revealed by a systematic review of the literature. We performed a systematic PubMed search from 1966 to present, using the search terms ‘rectal’, ‘rectum’, ‘colorectal’, ‘foreign’, ‘bodies’ and ‘endoscopic’. Only reports in English were included. The results of the systematic search of the literature, specified for the type of foreign body, are summarized in Table 1[1–36]. Table 1 also summarizes endoscopic techniques and non-endoscopic techniques for removing foreign bodies. In addition to the reports presented in the Table 1, several case series have been published without detailed information on the techniques used to remove various foreign bodies[18,22,25,37–46].
Table 1.
Overview of reports on endoscopic and non-endoscopic removal of rectal foreign bodies
| Type foreign body | Technique | Anaesthesia | Author[Ref.] |
| Ballpoint pen | Polypectomy snare1 | - | Richter[1] |
| Water filled balloon | Puncture and forceps1 | - | Wolf[2] |
| Chicken bone | Polypectomy snare1 | - | Tarnasky[3] |
| Toothpick | Polypectomy snare1 | - | Over[4] |
| Apple | Defragmentation by APC1 | None | Glaser[5] |
| Glass bottle | Biopsy forceps1 | General | Huang[6] |
| Vibrator | Polypectomy snare1 | None | Huang[6] |
| Glass test tube | Inflated Sengstaken tube1 | - | Hughes[7] |
| Test tube | Polypectomy snare1 | - | Kantarian[8] |
| Enema tip | Polypectomy snare1 | - | Kantarian[8] |
| Vibrator | Polypectomy snare, biopsy forceps1 | - | Kantarian[8] |
| Pencil | Polypectomy snare1 | - | Vemula[9] |
| Iron bar | 2-channel colonoscope and wires1 | - | Ahmed[10] |
| Bottle neck | Inflated Foley cathether1 | General | Humes[11] |
| Spray container | Achalasia balloon1 | None | Present report |
| Spongy toy ball | Obstetric vacuum extractor | General | Feigelson[12] |
| Vibrator | Obstetrical forceps, anal dilation | Local | Haft[13] |
| Vibrator | Uterine vulsellum | Local | Levin[14] |
| Aftershave bottle | Rubber-shod bone olding clamp | Spinal | Siroospour[15] |
| Chicken bone | Digitally | None | Davies[16] |
| Aerosol-can Cap | Tenaculum forceps, anal dilatation | General | Aquino[17] |
| Vase | Filling with plaster | General | Couch[18] |
| Glass jar | Extraction with plaster rolls | Spinal | Graves[19] |
| Glass jar | Endotracheal tube, anal dilation | Local | Garber[20] |
| Apple | Bimanual manipulation | Local | Sharma[21] |
| Glass jar | Inflated Foley catheter | General | Yaman[22] |
| Glass bottle | Obstetric vacuum cup | General | MacKinnon[23] |
| Glass bulb | 3 inflated Foley catheters | - | Diwan[24] |
| Thermometer | Biopsy forceps | General | Huang[6] |
| Vibrator | Transanal Kocher clamps | Local | Huang[6] |
| Bowling bottle | Obstetric forceps | General | Huang[6] |
| Perfume bottle | Manually | Spinal | Busch[25] |
| Piece of wood | Manually | General | Jansen[26] |
| Toothbrush case | Inflated Fogarty catheter | - | Wigle[27] |
| Oven mitt | Forceps after anal dilation | General | Losanoff[28] |
| Sink waste pipe | Obstetric forceps | General | Peet[29] |
| Metallic boule | Electromagnet | General | Coulson[30] |
| Carrot | Myomectomy screw | - | Vashist[31] |
| Glass | Obstetric vacuum extractor | Spinal | Johnson[32] |
| Rubber ball | Manual extraction, anal dilation | General | Nivatvongs[33] |
| Wooden rod | Bimanually, anal dilation | Spinal | Nivatvongs[33] |
| Bottle | Manually after anal dilation | General | Gopal[34] |
| Dildo | Myomectomy screw | - | Clark[35] |
| Light bulb | Abdominal compression | Spinal | Konishi[36] |
-: No description; APC: Argon-plasma coagulation;
Endoscopic removal of rectal foreign bodies.
An algorithm was provided to guide the clinician in his or her treatment decisions, partly based on the methods presented in the Table 1 (Figure 4). We included only those methods most commonly used and excluded rare treatment variants.
Figure 4.
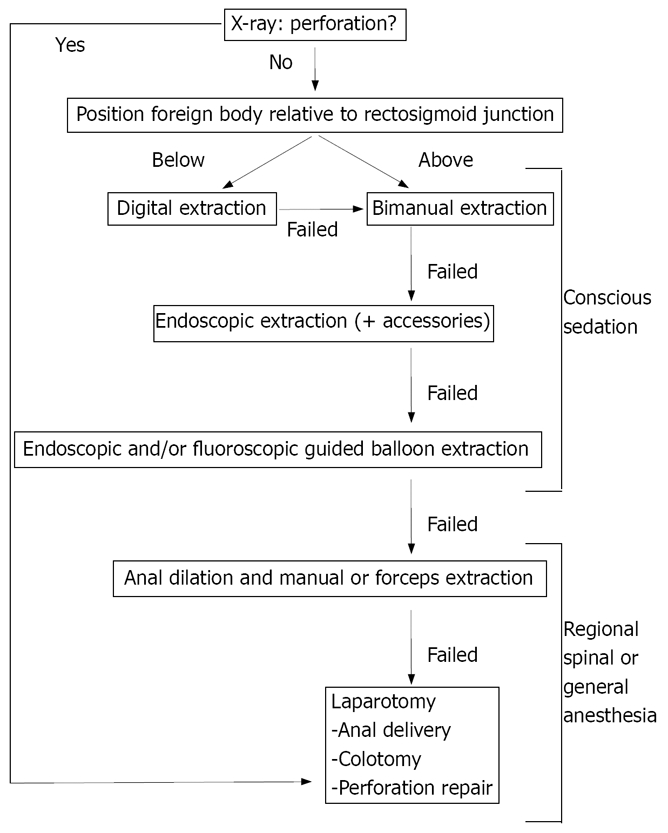
Algorithm for the removal of a colorectal foreign body.
The first step in the evaluation is that one should always be aware of the possibility of a large bowel perforation and perform radiological investigations. Plain abdominal radiography or water soluble contrast enemas may be helpful. An abdominal X-ray will also provide information on the localization of the foreign body, whether it is below or above the rectosigmoid junction. If perforation of the bowel has occurred, immediate laparotomy is warranted. If there are no signs of perforation, several management approaches can be tried. Our aim was to treat the patient on an outpatient basis with minimally invasive techniques and preferably under conscious sedation instead of general anaesthesia.
First, digital removal of the object should be attempted, if necessary with the patient at different positions. If this approach fails, one can try bimanual manipulation. The next step is the insertion of an endoscope with subsequent attempts to grasp the foreign body with regular endoscopy accessories like polypectomy snares. When this fails, it may be helpful to use devices that can be inflated in the rectosigmoid, such as a Foley catheter or an achalasia balloon. Such a device prevents a vacuum that might develop upon extraction of the foreign body and may also be directly used to remove the object.
If these interventions fail, we refer the patients to the operating theatre. Full relaxation of the anal sphincter muscles can be achieved by local, spinal or general anaesthesia. Sometimes, bimanual manipulation of the relaxed abdominal wall under spinal or general anaesthesia may evade surgery. Patients should be consented for a laparotomy prior to general anaesthesia should the manual or endoscopic removal fail.
Finally, when conservative measures fail, laparoscopic or laparotomic approaches are indicated. After removal, sigmoidoscopy is generally recommended to rule out perforations. In the largest series of patients with rectal foreign bodies described thus far (n = 93), it was found that objects retained for more than 2 days, those larger than 10 cm and those located proximal to the rectum increase the likelihood of surgery[37].
In conclusion, many techniques are available for the extraction of rectal foreign bodies. If possible, patients should be treated with minimally invasive techniques and preferably on an outpatient basis under conscious sedation.
Peer reviewer: Fabio Pace, Professor, “L. Sacco” University Hospital, Via G. B. Grassi, 74, Milano 20157, Italy
S- Editor Zhong XY L- Editor Wang XL E- Editor Zhang WB
References
- 1.Richter RM, Littman L. Endoscopic extraction of an unusual colonic foreign body. Gastrointest Endosc. 1975;22:40. doi: 10.1016/s0016-5107(75)73685-4. [DOI] [PubMed] [Google Scholar]
- 2.Wolf L, Geraci K. Colonscopic removal of balloons from the bowel. Gastrointest Endosc. 1977;24:41. doi: 10.1016/s0016-5107(77)73441-8. [DOI] [PubMed] [Google Scholar]
- 3.Tarnasky PR, Newcomer MK, Branch MS. Colonoscopic diagnosis and treatment of chronic chicken bone perforation of the sigmoid colon. Gastrointest Endosc. 1994;40:373–375. doi: 10.1016/s0016-5107(94)70079-6. [DOI] [PubMed] [Google Scholar]
- 4.Over HH, TOzUn N, AvSar E. Toothpick impaction: treatment by colonoscopy. Endoscopy. 1997;29:S60–S61. doi: 10.1055/s-2007-1004339. [DOI] [PubMed] [Google Scholar]
- 5.Glaser J, Hack T, Rubsam M. Unusual rectal foreign body: treatment using argon-beam coagulation. Endoscopy. 1997;29:230–231. doi: 10.1055/s-2007-1004178. [DOI] [PubMed] [Google Scholar]
- 6.Huang WC, Jiang JK, Wang HS, Yang SH, Chen WS, Lin TC, Lin JK. Retained rectal foreign bodies. J Chin Med Assoc. 2003;66:607–612. [PubMed] [Google Scholar]
- 7.Hughes JP, Marice HP, Gathright JB Jr. Method of removing a hollow object from the rectum. Dis Colon Rectum. 1976;19:44–45. doi: 10.1007/BF02590850. [DOI] [PubMed] [Google Scholar]
- 8.Kantarian JC, Riether RD, Sheets JA, Stasik JJ, Rosen L, Khubchandani IT. Endoscopic retrieval of foreign bodies from the rectum. Dis Colon Rectum. 1987;30:902–904. doi: 10.1007/BF02555435. [DOI] [PubMed] [Google Scholar]
- 9.Vemula NR, Madariaga J, Brand DL, Hershey H. Colonoscopic removal of a foreign body causing colocutaneous fistulas. Gastrointest Endosc. 1982;28:195–196. doi: 10.1016/s0016-5107(82)73057-3. [DOI] [PubMed] [Google Scholar]
- 10.Ahmed A, Cummings SA. Novel endoscopic approach for removal of a rectal foreign body. Gastrointest Endosc. 1999;50:872–874. doi: 10.1016/s0016-5107(99)70184-7. [DOI] [PubMed] [Google Scholar]
- 11.Humes D, Lobo DN. Removal of a rectal foreign body by using a Foley catheter passed through a rigid sigmoidoscope. Gastrointest Endosc. 2005;62:610. doi: 10.1016/s0016-5107(05)01575-0. [DOI] [PubMed] [Google Scholar]
- 12.Feigelson S, Maun D, Silverberg D, Menes T. Removal of a large spherical foreign object from the rectum using an obstetric vacuum device: a case report. Am Surg. 2007;73:304–306. [PubMed] [Google Scholar]
- 13.Haft JS, Benjamin HB, Wagner M. Vaginal vibrator lodged in rectum. Br Med J. 1976;1:626. doi: 10.1136/bmj.1.6010.626. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Levin SE, Cooperman H, Freilich M, Lomas M. The use of a curved uterine vulsellum for removal of rectal foreign bodies: report of a case. Dis Colon Rectum. 1977;20:532–533. doi: 10.1007/BF02586597. [DOI] [PubMed] [Google Scholar]
- 15.Siroospour D, Dragstedt LR 2nd. A large foreign body removed through the intact anus: report of a case. Dis Colon Rectum. 1975;18:616–619. doi: 10.1007/BF02587145. [DOI] [PubMed] [Google Scholar]
- 16.Davies DH. A chicken bone in the rectum. Arch Emerg Med. 1991;8:62–64. doi: 10.1136/emj.8.1.62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Aquino MM, Turner JW. A simple technique for removing an impacted aerosol-can cap from the rectum. Dis Colon Rectum. 1986;29:675. doi: 10.1007/BF02560339. [DOI] [PubMed] [Google Scholar]
- 18.Couch CJ, Tan EG, Watt AG. Rectal foreign bodies. Med J Aust. 1986;144:512–515. doi: 10.5694/j.1326-5377.1986.tb112273.x. [DOI] [PubMed] [Google Scholar]
- 19.Graves RW, Allison EJ Jr, Bass RR, Hunt RC. Anal eroticism: two unusual rectal foreign bodies and their removal. South Med J. 1983;76:677–678. [PubMed] [Google Scholar]
- 20.Garber HI, Rubin RJ, Eisenstat TE. Removal of a glass foreign body from the rectum. Dis Colon Rectum. 1981;24:323. [PubMed] [Google Scholar]
- 21.Sharma H, Banka S, Walton R, Memon MA. A novel technique for nonoperative removal of round rectal foreign bodies. Tech Coloproctol. 2007;11:58–59. doi: 10.1007/s10151-007-0328-z. [DOI] [PubMed] [Google Scholar]
- 22.Yaman M, Deitel M, Burul CJ, Shahi B, Hadar B. Foreign bodies in the rectum. Can J Surg. 1993;36:173–177. [PubMed] [Google Scholar]
- 23.Mackinnon RP. Removing rectal foreign bodies: is the ventouse gender specific? Med J Aust. 1998;169:670–671. doi: 10.5694/j.1326-5377.1998.tb123462.x. [DOI] [PubMed] [Google Scholar]
- 24.Diwan VS. Removal of 100-watt electric bulb from rectum. Ann Emerg Med. 1982;11:643–644. doi: 10.1016/s0196-0644(82)80218-7. [DOI] [PubMed] [Google Scholar]
- 25.Busch DB, Starling JR. Rectal foreign bodies: case reports and a comprehensive review of the world's literature. Surgery. 1986;100:512–519. [PubMed] [Google Scholar]
- 26.Jansen AA. Foreign body in the rectum. N Z Med J. 1969;70:174–175. [PubMed] [Google Scholar]
- 27.Wigle RL. Emergency department management of retained rectal foreign bodies. Am J Emerg Med. 1988;6:385–389. doi: 10.1016/0735-6757(88)90163-5. [DOI] [PubMed] [Google Scholar]
- 28.Losanoff JE, Kjossev KT. Rectal "oven mitt": the importance of considering a serious underlying injury. J Emerg Med. 1999;17:31–33. doi: 10.1016/s0736-4679(98)00116-4. [DOI] [PubMed] [Google Scholar]
- 29.Peet TN. Removal of impacted rectal foreign body with obstetric forceps. Br Med J. 1976;1:500–501. doi: 10.1136/bmj.1.6008.500. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Coulson CJ, Brammer RD, Stonelake PS. Extraction of a rectal foreign body using an electromagnet. Int J Colorectal Dis. 2005;20:194–195. doi: 10.1007/s00384-004-0629-x. [DOI] [PubMed] [Google Scholar]
- 31.Vashist MG, Arora AL, Salil Screwing a carrot out of the rectum. Indian J Gastroenterol. 1997;16:120. [PubMed] [Google Scholar]
- 32.Johnson SO, Hartranft TH. Nonsurgical removal of a rectal foreign body using a vacuum extractor. Report of a case. Dis Colon Rectum. 1996;39:935–937. doi: 10.1007/BF02053994. [DOI] [PubMed] [Google Scholar]
- 33.Nivatvongs S, Metcalf DR, Sawyer MD. A simple technique to remove a large object from the rectum. J Am Coll Surg. 2006;203:132–133. doi: 10.1016/j.jamcollsurg.2006.03.012. [DOI] [PubMed] [Google Scholar]
- 34.Gopal S. A bottle in the rectum. J Indian Med Assoc. 1974;62:24–25. [PubMed] [Google Scholar]
- 35.Clark SK, Karanjia ND. A cork in a bottle--a simple technique for removal of a rectal foreign body. Ann R Coll Surg Engl. 2003;85:282. doi: 10.1308/003588403766275060. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Konishi T, Watanabe T, Nagawa H. Impaction of a rectal foreign body: what is the final approach before surgery? Dis Colon Rectum. 2007;50:262–263; author reply 263. doi: 10.1007/s10350-006-0788-7. [DOI] [PubMed] [Google Scholar]
- 37.Lake JP, Essani R, Petrone P, Kaiser AM, Asensio J, Beart RW Jr. Management of retained colorectal foreign bodies: predictors of operative intervention. Dis Colon Rectum. 2004;47:1694–1698. doi: 10.1007/s10350-004-0676-4. [DOI] [PubMed] [Google Scholar]
- 38.Clarke DL, Buccimazza I, Anderson FA, Thomson SR. Colorectal foreign bodies. Colorectal Dis. 2005;7:98–103. doi: 10.1111/j.1463-1318.2004.00699.x. [DOI] [PubMed] [Google Scholar]
- 39.Rodriguez-Hermosa JI, Codina-Cazador A, Ruiz B, Sirvent JM, Roig J, Farres R. Management of foreign bodies in the rectum. Colorectal Dis. 2007;9:543–548. doi: 10.1111/j.1463-1318.2006.01184.x. [DOI] [PubMed] [Google Scholar]
- 40.Cohen JS, Sackier JM. Management of colorectal foreign bodies. J R Coll Surg Edinb. 1996;41:312–315. [PubMed] [Google Scholar]
- 41.Barone JE, Sohn N, Nealon TF Jr. Perforations and foreign bodies of the rectum: report of 28 cases. Ann Surg. 1976;184:601–604. doi: 10.1097/00000658-197611000-00011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Kouraklis G, Misiakos E, Dovas N, Karatzas G, Gogas J. Management of foreign bodies of the rectum: report of 21 cases. J R Coll Surg Edinb. 1997;42:246–247. [PubMed] [Google Scholar]
- 43.Eftaiha M, Hambrick E, Abcarian H. Principles of management of colorectal foreign bodies. Arch Surg. 1977;112:691–695. doi: 10.1001/archsurg.1977.01370060023003. [DOI] [PubMed] [Google Scholar]
- 44.Nehme Kingsley A, Abcarian H. Colorectal foreign bodies. Management update. Dis Colon Rectum. 1985;28:941–944. doi: 10.1007/BF02554312. [DOI] [PubMed] [Google Scholar]
- 45.Ooi BS, Ho YH, Eu KW, Nyam D, Leong A, Seow-Choen F. Management of anorectal foreign bodies: a cause of obscure anal pain. Aust N Z J Surg. 1998;68:852–855. doi: 10.1046/j.1440-1622.1998.01463.x. [DOI] [PubMed] [Google Scholar]
- 46.Viceconte G, Viceconte GW, Bogliolo G, Pietropaolo V, Dell' Anna A, Montori A. Endoscopic removal of foreign bodies in the large bowel. Endoscopy. 1982;14:176–177. doi: 10.1055/s-2007-1021614. [DOI] [PubMed] [Google Scholar]