

Abstract
This population-based study of high school seniors examines differences in the influence of several important determinants of smoking among white, African-American, Hispanic, and other teens. With national survey data for each year from 1976 to 2004, logistic regression is used to test for differences across race and ethnic groups (averaged over all years) in the effects on daily smoking of background factors such as living arrangements and parents’ education and social activities such as academic performance and religiosity. The results show similarity in effects across racial categories, but some determinants have weaker or reversed effects for African-American and Hispanic youth than for white youth. For example, high parents’ education increases smoking among Hispanic youth, has little influence among African Americans, and decreases smoking among whites. These results suggest that smoking patterns of minority teens differ in some ways from those of white teens.
Keywords: Smoking, Cigarette use, High school, Adolescence, African Americans, Hispanics
Introduction
After 30 years of changes, smoking among white, African-American, and Hispanic youth has come to differ in striking and surprising ways [1]. In general, youth smoking has fluctuated widely over the last several decades: It declined in the late 1970s, leveled off at new lows in the 1980s, rose to a new peak from 1992 to 1997, and then declined during the late 1990s and early 2000s [2–4]. However, according to figures computed from the Monitoring the Future (MTF) surveys, smoking among African Americans fell the most, smoking for whites fell the least, and smoking for Hispanics and others stayed somewhere between these two groups (see Fig. 1). In 1976, the percentage of daily smokers equaled 28 for whites, 27 for African Americans, and 21 for Hispanics—a gap of 7 percentage points between the highest and lowest. By 2004, however, the percentages equaled 17 for whites, 10 for Hispanics, and 5 for African Americans, and the gap increased to 12 percentage points. For both Hispanic and African-American youth, their current low smoking is surprising. Minority youth generally suffer more than whites from economic deprivation, poor schools, and involvement in serious crime [5], but cigarette smoking represents an exception to their disadvantage.
Fig. 1.
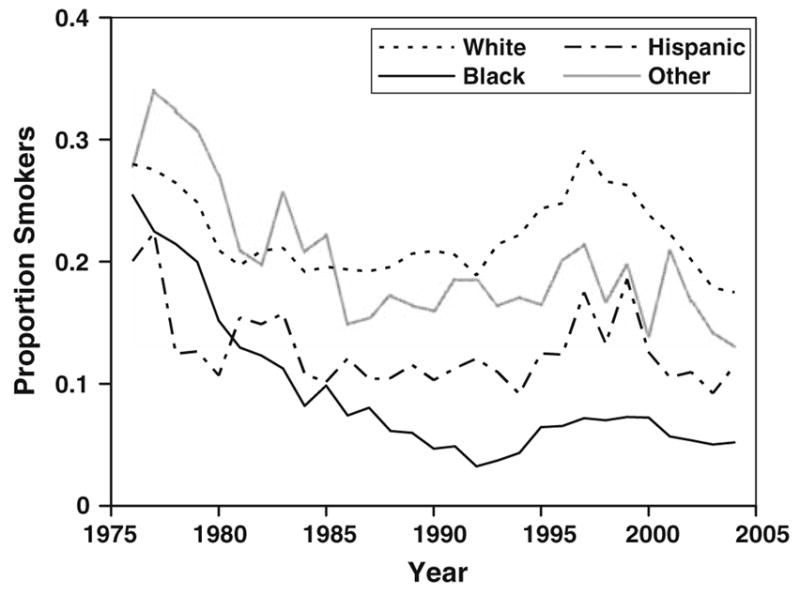
Proportion smokers by race and year: MTF data 1976–2004
Differences in exposure to risk factors for smoking do not account for the race and ethnic differences. Smoking is increased by characteristics such as low parental socioeconomic status (SES) [6–8], living in single-parent households [9], poor academic standing, and frequently going out at night [10–12]. Yet minorities generally face more such risks than whites, which would lead to higher rather than lower smoking [13, 14]. As a result, one analysis of MTF data through 1989 found that the different family background and lifestyle characteristics of Hispanic and African-American youth do not account for their lower levels of smoking [15]. Smoking patterns appear to result from something other than differences in the composition of race and ethnic populations [16].
Less is known about the sources of these differences, but some studies suggest that race and ethnic differences in smoking may come from varied responses to the same determinants [17, 18]. The processes leading to the use of cigarettes may differ such that the same risk factors do more to increase smoking among whites than Hispanics and African Americans. Stated conversely, the more disadvantaged backgrounds and difficult experiences of African-American and Hispanic youth may limit the importance of risk factors for smoking. Thus, one study finds weaker effects of education on smoking for African Americans than whites [19], and another study finds that added risk factors of low prestige occupation and poverty income do little to increase smoking of African-American men [20]. These results may stem from the experience of racial discrimination by high SES African Americans [21], which in turn leads to smoking among high as well as low SES groups [22]. Among teens, poor scholastic attitudes do less to encourage African-American smoking [23], perhaps because strong anti-smoking attitudes of parents and peers counterbalance risk factors for high smoking [24].
For Hispanics, other factors may reduce the impact of background factors on smoking. Hispanics born outside the United States or with parents born outside the United States may smoke less because they are more accustomed to lower use of cigarettes and more negative smoking norms in their country of origin [25, 26]. If so, factors such as low parental education and poor academic achievement may lead less often to smoking among Hispanic youth than among whites. Even if determinants for Hispanics who are more acculturated to American smoking norms have expected effects, the lower smoking among less acculturated Hispanic [27, 28] youth may weaken the overall effects.
Such claims need more detailed examination. This study compares the influence of family background and social activities on smoking of white, African American, Hispanic, and other high school seniors. It uses a large sample from yearly national surveys done by the Monitoring the Future project between 1976 and 2004. If differences in the determinants of smoking by race and ethnicity exist, they may provide useful information on targeting policies for minority groups and reducing health inequality early in the life course.
The combined attention to minority groups and teens, two vulnerable populations prone to disadvantage and social problems, has clear importance in the study of smoking [29, 30]. However, few studies have examined race and ethnic differences in teen smoking—particularly for Hispanics. Several studies describe differences among adults [25, 31, 32] but not among teens. Other studies examine levels of teen smoking for race and ethnic groups [15, 16] but not the differences in determinants. Moreover, studies of local samples may face problems of generality and comparability in findings [33]. A few studies directly compare race and ethnic groups, finding mostly common determinants and some differences, but they also face problems of small sample sizes for minority smokers [23, 34, 35].
Methods
Data
The data come from the Monitoring the Future (MTF) project, which has surveyed nationally-representative samples of high school seniors during the spring of each year from 1976 to 2004 [1]. Focused specifically on youth, the surveys not only ask questions about smoking but also about many background and lifestyle characteristics related to smoking. Other surveys of tobacco use among respondents of all ages seldom ask about family background, school performance, and social activities that relate to critical decisions to start smoking at young ages. Moreover, when pooled over the full time period, the MTF surveys have sufficient cases for analyses within race and ethnic groups.
To obtain a nationally representative sample of 12th-grade students, the MTF surveys use multi-stage sampling procedures for the 48 coterminous states. Each year the project first selects geographic areas, roughly 130 schools within the geographical areas, and about 400 students in each school (or the entire senior class if it has fewer than 400 students). From 65 to 80% of the schools have agreed to participate over the years and allowed the students to complete a self-administered questionnaire during a normal class period. Within schools, the response rate of 83% largely excludes those students absent on the day of collection (only about 1% refused to complete the questionnaire). An et al. [10] summarize the conclusions of a good deal of analysis of possible biases in the samples: “While both school and student response rates have varied somewhat over time, …adjustments for these differences indicate that any bias in overall prevalence rates is likely to be quite small and that variations in response rates over time are not a significant factor in explaining trends in cigarette use.”
The data allow for use of four race and ethnic categories: self-identified non-Hispanic whites, non-Hispanic African Americans, Hispanics, and others. Given privacy concerns, the data do not distinguish Mexican Americans, Puerto Ricans, Cuban Americans, and other Latinos from one another. The inability to attend to this diversity is a weakness, but the large sample size for study of Hispanics along with whites and African Americans is an asset. Also given privacy concerns, the data do not distinguish among Native Americans, Pacific Islanders, and Asian Americans that make up the other category. This category contains such disparate groups that it is difficult to make sense of their results, but for completeness it is analyzed along with the other, more meaningful race and ethnic categories.
A problem with the surveys of high school seniors is that they exclude absentees at the time of the survey (about 17% of the sample) and high school dropouts (about 15% of youth at high school ages). Analyses of the MTF data address the possible bias created by these missing groups [1]. Concerning the absentees, comparing survey respondents by the number of absences during the last 4 weeks indicates that those with many absences use substances and drugs more than those with few, but their absence depresses the estimates of smoking prevalence only slightly. Concerning dropouts, those who fail to complete high school likely have higher rates of tobacco use than those who graduate. However, differences in dropout rates do not account for differences across race and ethnic groups in smoking and drug use [33, 36]. Further support for this claim comes from studies of youth smoking based on household rather than high school surveys. Despite including all youth, both dropouts and students, data from the National Health Interview Survey and the National Household Survey on Drug Abuse reveal much the same trends as the MTF surveys [4].
Measures
Over the 29-year time span from 1976 to 2004, the MTF surveys have employed a set of core questions that all respondents answer. The core questions include basic background, lifestyle, and smoking variables and provide for consistent measures over the full period. A pooled sample for all years has been created with the following measures.
Smoking is measured by questions that ask about daily use of cigarettes over the last 30 days. As done in other studies [10], respondents are divided into two categories, those who smoked at least one cigarette a day over the last month, and those who did not. Compared to never smokers or occasional smokers, daily smokers have a high likelihood of continuing to smoke as adults [37] and are the key focus of the dependent variable. Self-report questions about cigarette use appear to be reliable and valid. Studies of carbon monoxide in blood and cotinine (a nicotine metabolite) in saliva find that self reports are largely valid [38], particularly when the surveys are completed in school, as is the case for the MTF data, rather than at home [4]. Not surprisingly, youth are less forthcoming about substance use in household surveys where their parents are nearby than in school where they have privacy from family members. Moreover, self-reports appear to be valid assessments of race and ethnic differences in smoking [36]. One report [33] notes, for example, that “no evidence indicates that the misclassification bias [of self-reported smoking] explains the substantial decline in smoking prevalence reported by African-American youths.”
Besides demographic variables such as sex, race, and ethnicity, the MTF data contain a variety of individual background and activity measures relevant to smoking. Parents’ education measures completed schooling for the respondent’s mother or father if available for only one parent, and an average score when data is available for both parents; a one unit change refers to single years of education from a minimum of 7 to a maximum of 18. Since the data do not include measures of country of birth or immigration status, parents’ education becomes a particularly important indicator of the family background of Hispanic youth. Living arrangements are measured with a dummy variable that codes respondents living with both parents as one and all others as zero. Community size consists of six categories in answer to the question of where the respondent grew up mostly: (1) farm, (2) country, (3) small town, (4) medium city or its suburb, (5) large city or its suburb, and (6) very large city or its suburb. Religiosity is measured by combining religious attendance (never, rarely, once or twice a month, and once a week or more) and the importance of religion (not important, a little important, pretty important, and very important) into a single scale (Chronbach’s alpha equals .736). School performance consists of a standardized scale (Chronbach’s alpha equals .670) that combines four items: self-assessed school ability compared to others the same age (ranging in seven categories from far below average to far above average), self-assessed intelligence compared to others the same age (using the same seven categories), days missed from cutting classes, and grade point average (for categories of A, A−, B+ and so on to D). Teen’s income is measured by a question on the money received per week (in tens of real dollars) from a job or other sources (allowances, etc.). Social activities are measured by a question about how many evenings the respondent goes out during a typical week for fun and recreation (ranging in six categories from less than one to six or seven).
Statistical Analysis
The analysis uses logistic regression to estimate the association of the predictors with the logged odds of the binary smoking outcome variable. The estimates come from fixed-effects models that include dummy variables for year. The time effects reflected in the coefficients for the year variables control for the changing environment of smoking from 1976 and 2004. The initial models combine all race and ethnic groups, but subsequent models examine the determinants separately for each group (which allows the dummy variable effects for year to reflect the different trends among the race and ethnic groups). To compare of the size and direction of the effects of the risk factors across race and ethnic groups, tests of significance for differences in coefficients are presented. The tests come from the z-ratios for interaction terms of race and ethnicity by each determinant in a combined model of smoking for all race and ethnic groups.
Weights are used to adjust for oversampling of minority students and to equalize the sample size for each year. After eliminating missing data on the variables, the weighted sample size for each year (n = 11,438) equals the unweighted total sample size for all years (N = 331,696) divided by the number of years (29). The MTF surveys also use stratification and clusters in the sample design but, to protect the anonymity of respondents, do not identify the sampling units needed to directly adjust for the deviation from simple random sampling in calculation of standard errors [39]. Combined with the huge sample size, this limitation warrants the conservative use of tests of significance and stringent levels of significance.
Results
Table 1 lists the means of the dependent and independent variables for the full sample and for each race and ethnic group. Averaged across all years, whites smoke most (22.2%), followed by others (19.3%), Hispanics (12.3%), and African Americans (9.1%). Whites and others have parents with higher education (13.6 and 13.5 years) than African Americans (12.8 years) and Hispanics (11.6 years). Otherwise, African Americans have low values on living with both parents and academic performance and high values on own income, all of which make them more prone to smoke; they also have high values on religiosity and low values on going out often that make them less prone to smoke. Hispanic youth have values on living with both parents and academic performance that make them prone to smoking.
Table 1.
Descriptive statistics by race
| Variables | Full sample |
White | Black | Hisp. | Other | Full sample |
||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | Mean | Mean | Mean | Min. | Max. | |
| Smoking | .201 | .400 | .222 | .091 | .123 | .193 | 0 | 1 |
| Sex: Female | .519 | .500 | .512 | .579 | .528 | .491 | 0 | 1 |
| Parents’ education | 13.4 | 2.45 | 13.6 | 12.8 | 11.6 | 13.5 | 7 | 18 |
| Lives with both parents | .751 | .433 | .796 | .470 | .682 | .735 | 0 | 1 |
| Size of community | 3.58 | 1.37 | 3.44 | 4.04 | 4.18 | 3.95 | 1 | 6 |
| Academic performance | .00 | .998 | .055 | −.198 | −.322 | −.037 | −4.93 | 2.54 |
| Own income | 4.87 | 3.82 | 4.84 | 5.13 | 4.87 | 4.69 | 0 | 26.9 |
| Religiosity | 2.77 | .934 | 2.71 | 3.82 | 2.86 | 2.64 | 1 | 4 |
| Frequency goes out | 3.53 | 1.33 | 3.61 | 3.22 | 3.27 | 3.26 | 1 | 6 |
N: full sample = 331,696, white = 254,184, black = 37,954, Hispanic = 19,829, other = 19,729
The logistic regression models in Table 2 describe the levels of smoking for the race, ethnic, and gender groups. With controls for year, no controls for background and lifestyle variables, and white males treated as the reference group, the odds ratios in column 1 and confidence intervals in column 2 summarize gross differences in smoking. White females have the highest smoking (16.1% higher than for white males). All other groups have lower smoking than white males. Males and females in the other category rank next in smoking (odds ratios of .930 and .919, respectively), then Hispanic males and females follow (odds ratios .624 and .478), and African-American males and females smoke least (odds ratios .444 and .333). Except among whites, males smoke more than females.
Table 2.
Odds ratios and 95% confidence intervals from logistic regressions of daily smoking on race, ethnicity, gender, background, and lifestyle determinants
| Independent variablesa | OR | 95% CI | OR | 95% CI | OR | 95% CI |
|---|---|---|---|---|---|---|
| Black male | .444 | .417–.472 | .358 | .336–.382 | .380 | .354–.406 |
| Hispanic male | .624 | .580–.671 | .497 | .461–.536 | .516 | .476–.558 |
| Other male | .930* | .876–.988 | .879 | .827–.934 | .891 | .833–.953 |
| White female | 1.161 | 1.136–1.187 | 1.141 | 1.117–1.167 | 1.503 | 1.468–1.540 |
| Black female | .333 | .315–.353 | .261 | .247–.277 | .424 | .399–.452 |
| Hispanic female | .478 | .444–.515 | .372 | .345–.402 | .535 | .493–.580 |
| Other female | .919 | .863–.978 | .854 | .801–.910 | 1.205 | 1.126–1.289 |
| Parents’ education | .927 | .923–.931 | .978 | .973–.982 | ||
| Size of community | 1.014 | 1.007–1.022 | .986 | .978–.995 | ||
| Lives with both parents (does not reference) | .664 | .649–.680 | .781 | .762–.801 | ||
| Academic performance | .608 | .601–.615 | ||||
| Own income | 1.064 | 1.061–.1.067 | ||||
| Religiosity | .721 | .713–.729 | ||||
| Frequency goes out | 1.367 | 1.355–1.379 | ||||
| Pseudo R2b | .021 | .032 | .126 |
Source: Monitoring the Future 12th graders 1976–2004, N = 331,696 (estimates weighted for sample design with STATA 8.0)
Controls for year dummy variables are included, but the coefficients are not presented
Pseudo R2 = (log likelihood − baseline log likelihood)/baseline log likelihood
P < .01; for all other coefficients, P < .001
In columns 3–4, the background controls increase the differences across races. Having highly educated parents (odds ratio .927) and living with both parents (.664) reduce smoking, while size of community (1.014) slightly increases smoking. Comparing the odds ratios without and with the controls shows that the smoking of African-American and Hispanic youth falls relative to white youth. For example, the odds ratio for Hispanic males changes from .624 without controls to .497 with controls. Thus, African American and Hispanic youth would smoke less if not facing the pro-smoking circumstances of less educated parents, fewer two-parent families, and more urban residence. However, these background factors account for little additional pseudo-variance explained, which rises from 2.1 to 3.2%.
Controls for lifestyle variables tend to reduce race, ethnic, and gender differences. These lifestyle variables have more influence on smoking than the background factors, raising the pseudo-variance explained from 3.2 to 12.6%. As expected, school performance (odds ratio .608) and religiosity (.721) lower smoking, while going out often (1.367) and own income (1.064) increase smoking. The gap between white males and females of all races and ethnicities tends to decline with these controls. For example, the odds ratio for African American females changes from .261 to .424 with the lifestyle controls. Male differences tend to change less with these controls. However, large differences across race and ethnic groups remain.
Table 3 presents the logistic regression coefficients and odds ratios for models estimated separately for white, African-American, Hispanic, and other teens. The first column within each group lists the odds ratios and confidence interval, while the second column (for all but whites) lists the z-ratios for the differences of the coefficients between each group and whites. These z-ratios come from models that include interaction terms for race-ethnicity by each of the other predictors and indicate significant differences in effects. The equation for whites shows higher smoking for females (odds ratio 1.516) with high own income (1.070) and who go out often (1.377). Those with more educated parents (odds ratio .970), higher academic performance (.593), and greater religiosity (.723) smoke less.
Table 3.
Odds ratios, 95% confidence intervals, and difference-in-coefficients z and P-valuesa from logistic regressions of daily smoking on gender, background, and lifestyle determinants by race and ethnic group
| Independent variables b | White, OR (CI) | Black, OR (CI) | Black–White, z (P) | Hispan, OR (CI) | Hispan–White, z (P) | Other, OR (CI) | Other–White, z (P) |
|---|---|---|---|---|---|---|---|
| Female (male reference) | 1.516(1.480–1.553) | 1.015(.927–1.111) | −8.78 (.000) | 1.013(.908–1.131) | −7.02 (.000) | 1.342(1.222–1.473) | −2.29(.022) |
| Parents’ education | .970(.965–.976) | 1.010(.991–1.029) | −1.56(.118) | 1.049(1.029–1.070) | 7.92(.000) | .991(.974–1.008) | 3.21(.001) |
| Lives with both parents (does not reference) | .769(.747–.791) | .838(.768–.914) | 4.47(.000) | .863(.773–.963) | 1.83(.067) | .772(.698–.852) | −0.30(.763) |
| Size of community | .999(.990–1.009) | .925(.894–.957) | −4.99(.000) | .985(.945–1.027) | −0.58(.559) | .939(.908–.970) | −2.96(.003) |
| Academic performance | .593(.586–.601) | .729(.696–.764) | 8.63(.000) | .666(.630–.704) | 3.99(.000) | .675(.645–.706) | 5.71(.000) |
| Own income | 1.070(1.066–1.073) | 1.038(1.029–1.047) | −6.85(.000) | 1.051(1.039–1.063) | −2.94(.003) | 1.059(1.048–1.070) | −2.29(.022) |
| Religiosity | .723(.714–.733) | .700(.665–.738) | −0.49(.625) | .723(.681–.768) | 0.13(.893) | .766(.730–.803) | 1.98(.048) |
| Frequency goes out | 1.377(1.364–1.391) | 1.249(1.211–1.288) | −5.74(.000) | 1.300(1.243–1.351) | −2.85(.004) | 1.402(1.354–1.451) | 0.98(.325) |
| Pseudo R2c | .122 | .105 | .082 | .118 |
Source: Monitoring the Future 12th graders 1976–2004, N = 331,696 (estimates weighted for sample design with STATA 8.0)
z-Ratio for difference in coefficients for each race and ethnic group compared to whites
Controls for year dummy variables are included, but the coefficients are not presented
Pseudo R2 = (log likelihood − baseline log likelihood)/baseline log likelihood
As shown in columns 2–3 in Table 3, the determinants of smoking have less influence among African Americans than whites. Differences by sex and parents’ education fall to insignificance among African-American youth, while the influence of living arrangements, academic performance, own income, and going out are all significantly smaller than for whites. For example, the odds ratios for academic performance equal .593 for whites and .729 for African Americans. A test of significance shows a z-value for the race difference of 8.63. Only community size has larger effects among African-American youth, as their smoking declines more in large cities than for white youth. With lower smoking levels and greater disadvantage, the background and lifestyle determinants generally do less to distinguish smokers and non-smokers among African-American youth than white youth.
Hispanics also show generally weaker effects of the determinants than whites (columns 4–5). Sex, academic performance, own income, and going out have less influence on smoking among Hispanic youth than white youth. More important, parents’ education changes direction altogether. While highly educated parents reduce smoking among whites (odds ratio .970), they increase smoking among Hispanics (odds ratio 1.049). For example, for a 4-year difference in education, say between parents with a college degree and a high school degree, the odds ratios are .886 for whites and 1.211 for Hispanics. This effect may reflect the low education and low smoking of immigrant and less acculturated Hispanic parents. Despite the difference in direction, however, the odds ratios fall close to the one for both groups and indicate that these statistically significant differences are not large.
The other category, although lacking the clear identity of the African-American and Hispanic categories, also shows weaker effects than for whites. Of the significantly different coefficients, only the one for community size is stronger for the other category than for whites (columns 6–7).
Discussion
This analysis of survey data on high school seniors from 1976 to 2004 compared the influence of family background and social activities on smoking of race and ethnic groups. Consistent with previous studies, it found that differences in smoking across race and ethnic groups do not result simply from the composition of the groups or their levels of risk factors. To the contrary, controlling for the background factors often increased rather than eliminated race and ethnic differences in smoking. However, the results also indicated that the size of the effects sometimes varied across the groups. In general, the determinants had less influence on minority groups than whites and, in some cases, differed in direction. For example, high parents’ education increased smoking among Hispanic youth, had little influence on African-American youth, and decreased smoking among white youth. In many cases, the determinants had similar influences across race and ethnic groups, but the differences demonstrate that race and ethnic groups sometimes respond in varied ways to the same characteristics. However, because the observed differences across groups are not large, these findings need to be duplicated in other settings and with other data before accepting their validity.
Even controlling for differences in levels of the risk factors and their influence on smoking, most variation in smoking across race and ethnic groups remained unexplained. This suggests that social and cultural forces affecting all members of minority groups play an important role in patterns of cigarette use. The low smoking of African-American teens likely relates in some ways to norms and values that treat the behavior as undesirable [36]. These norms and values appear to change at older ages, as late adoption of cigarettes by African Americans equalizes race differences in the 20 s and 30 s [40–43]. The lower levels of smoking among Hispanic teens likely relate to the lower levels of smoking among immigrant than native groups [25, 26, 28]. Again, anti-smoking norms and values lead some Hispanics to resist the habit when young, but these norms and values may change among more acculturated Hispanic youth and increase their smoking.
Whatever the source of the differences, these results suggest that, in some cases, policies and anti-smoking programs may benefit from understanding the special characteristics of minority teen smokers. Despite many similarities, African-American and Hispanic youth do not always respond to risk factors just as white teens do. Kandel et al. argue that the similarities across race and ethnic groups are large enough to warrant use of the similar anti-smoking programs [23]. Efforts to lower teen smoking with restrictions on purchase, anti-smoking advertising, limiting marketing and promotion efforts of tobacco companies, and increasing prices have benefits for diverse groups of smokers [44–46]. Indeed, the lower smoking of African-American and Hispanic youth suggests that current tobacco programs may have worked well for these minority groups. At the same time, some added benefit may come from attention to the special characteristics of minority youth, who are less influenced by background factors such as parents’ education and lifestyle factors such as academic performance. For example, recommendations for anti-smoking programs to target high-risk youth from disadvantaged backgrounds and doing poorly in academics may efficiently identify white smokers in need of help [33]. However, the weaker relationships of smoking with socioeconomic background and academic performance mean such an approach may work less well for African Americans and Hispanics.
As other papers have examined changes over time in the levels and determinants of smoking by teens [10, 47–49], the analysis controlled for year in the models but did not directly examine changes in effects. However, some preliminary tests for interactions between year and the determinants of smoking among African-American and Hispanic youth indicate that the effects of the determinants do not change significantly over time. In other words, trends in smoking for these minority groups have affected all subgroups similarly rather than having speeded the decline among some more than others. The tables thus included controls for changes in the trend in smoking but presented effects of family background and social activities averaged across time.
These results face several limitations. To maintain compatibility across surveys over a long time span, the MTF data include only a subset of potential determinants of smoking. Measures of the smoking status of parents and teen peers would no doubt do much to account for patterns of smoking among youth (although they would not account for why the smoking of parents and friends differs across race and ethnic groups). Measures involving concern about weight, exposure to cigarette marketing efforts, and the experience with media or school anti-smoking campaigns would likely prove important as well.
Also, the sample would be improved if high school dropouts could be included. Dropout rates for Hispanics are higher than for whites and may bias the findings for high school students on the influence of risk factors. For example, such selection bias may constrain the variation in SES more for Hispanics and African Americans than whites and thereby limit the effects SES can have on smoking. However, the standard deviations of parental education for African Americans and Hispanics are as large as or larger than for whites, principally because fewer whites have parents with low education; sufficient variation remains in parental education for it to affect smoking among minority groups. Still, if high-smoking Hispanics with low educated parents are particularly likely to drop out of school, it would weaken the relationship between parental education and smoking. The influence of such bias cannot be dismissed.
In addition, the results are limited by the use of cross-sectional data for 12th graders. The MTF cross-sectional data do not allow one to trace life-course pathways that lead to and follow from smoking while a high school senior [50]. This means that the cross-sectional results for 12th graders may not reflect relationships at younger ages or patterns of early initiation among race and ethnic groups. It also means that the results may not reflect smoking that begins at older ages. For example, because a greater percentage of African Americans than whites start smoking after age 18 [33], the results for 12th graders may not capture the determinants of these late starters and may not present a complete picture of racial differences in smoking. These limitations in the cross-sectional data will weaken true relationships but likely not eliminate them altogether. Since the vast majority of smokers start before 12th grade, studying seniors allows for meaningful, although still incomplete, findings.
Acknowledgments
This research was supported by grant R03CA101498 from the National Cancer Institute. The data come from Jerald G. Bachman, Lloyd D. Johnston, and Patrick M. O’Malley. Monitoring the Future: A Continuing Study of American Youth (12th-Grade Survey), 1976–2004 [Computer files], conducted by the University of Michigan, Survey Research Center (Ann Arbor, MI: Inter-university Consortium for Political and Social Research [producer and distributor]).
References
- 1.Johnston LD, O’Malley PM, Bachman JG, Schulenberg JE. Monitoring the Future national survey results on drug use 1975–2004: volume 1, secondary school students. Bethesda, MD: National Institute on Drug Abuse; 2005. Available online at http://www.monitoringthefuture.org/pubs.html. [Google Scholar]
- 2.Crump C, Packer L. Incidence of initiation of cigarette smoking—United States, 1965–1996. MMWR. 1998;47:837–40. [PubMed] [Google Scholar]
- 3.DHHS. Women, smoking: a report of the surgeon general. Rockville, MD: DHHS; 2001. p. 60. [Google Scholar]
- 4.Nelson DE, Giovino GA, Shoplan DR, Mowery PD, Mills SL, Eriksen MP. Trends in cigarette smoking among U.S. adolescents, 1974 through 1991. Am J Pub Health. 1995;85:34–40. doi: 10.2105/ajph.85.1.34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Peterson RD, Krivo LJ, Hagen J, editors. Many colors of crime: inequalities of race, ethnicity, and crime in America. New York: New York University Press; 1996. [Google Scholar]
- 6.Jacobson P, Lantz PM, Warner KE, Wasserman J, Pollack HA, Ahlstrom AA. Combating teen smoking: research and policy strategies. Ann Arbor: University of Michigan; 2001. p. 93. [Google Scholar]
- 7.Jefferies BJ, Power C, Graham H, Manor O. Effects of childhood socioeconomic circumstances on persistent smoking. Am J Pub Health. 2004;94:279–85. doi: 10.2105/ajph.94.2.279. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Soteriades ES, DiFranza JR. Parent’s socioeconomic status, adolescents’ disposable income, and adolescents’ smoking status in Massachusetts. Am J Pub Health. 2003;93:1155–60. doi: 10.2105/ajph.93.7.1155. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Griesbach D, Amos A, Currie C. Adolescent smoking and family structure in Europe. Soc Sci Med. 2003;56:41–52. doi: 10.1016/s0277-9536(02)00014-x. [DOI] [PubMed] [Google Scholar]
- 10.An LC, O’Malley PM, Schulenberg JE, Bachman JG, Johnston LD. Changes at the high end of risk in cigarette smoking among U.S. high school seniors, 1976–1995. Am J Pub Health. 1999;89:699–705. doi: 10.2105/ajph.89.5.699. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Bachman JG, Wadsworth KN, O’Malley PM, Johnston LD, Schulenberg JE. Smoking, drinking, drug use in young adulthood. Mahwah, NJ: Lawrence Erlbaum; 1997. [Google Scholar]
- 12.Safron DJ, Schulenberg JE, Bachman JG. Part-time work and hurried adolescence: the links among work intensity, social activities, health behaviors and substance use. J Health Soc Behav. 2001;42:425–49. [PubMed] [Google Scholar]
- 13.Wallace JM, Forman TA, Guthrie B. The epidemiology of alcohol, tobacco and other drug use among black youth. J Studies Alcohol. 1999;60:800–99. doi: 10.15288/jsa.1999.60.800. [DOI] [PubMed] [Google Scholar]
- 14.Faulkner DL, Escobedo LG, Zhu BP, Chrismon JH, Merritt RK. Race and the incidence of cigarette smoking among adolescents in the United States. J Natl Cancer Inst. 1996;88:1158–60. doi: 10.1093/jnci/88.16.1158. [DOI] [PubMed] [Google Scholar]
- 15.Bachman JG, Wallace JM, O’Malley PM, Johnston LD, Kurth CL, Neighbors HW. Racial/ethnic differences in smoking, drinking, and illicit drug use among American high school seniors, 1976–1989. Am J Pub Health. 1991;81:372–7. doi: 10.2105/ajph.81.3.372. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Wallace JM, Bachman JG. Explaining racial/ethnic differences in adolescent drug use: the impact of background and lifestyle. Soc Problems. 1991;38:333–55. [Google Scholar]
- 17.Johnson RA, Hoffman JP. Adolescent cigarette smoking in U.S. racial/ethnic subgroups: findings from the national education longitudinal study. J Health Soc Behav. 2000;41:392–407. [PubMed] [Google Scholar]
- 18.Anderson C, Burns DM. Patterns of adolescence smoking initiation rates by ethnicity and sex. Tob Control. 2000;9:4–8. doi: 10.1136/tc.9.suppl_2.ii4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Kiefe CI, Williams OD, Lewis CE, Allison JJ, Sekar P, Wagenknecht LE. Ten-year changes in smoking among young adults: are racial differences explained by socioeconomic factors in the Cardia study? Am J Pub Health. 2001;91:213–8. doi: 10.2105/ajph.91.2.213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Barbeau E, Krieger N, Soobader M-J. Working class matters: socioeconomic disadvantage, race/ethnicity, gender, and smoking in NHIS 2000. Am J Pub Health. 2004;94:269–78. doi: 10.2105/ajph.94.2.269. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Williams DR. The health of U.S. racial and ethnic populations. J Geront: Series B. 2005;60B(Special Issue II):53–62. doi: 10.1093/geronb/60.special_issue_2.s53. [DOI] [PubMed] [Google Scholar]
- 22.Bennett GG, Wolin KW, Robinson EL, Fowler S, Edwards CL. Perceived racial/ethnic harassment and tobacco use among African American young adults. Am J Pub Health. 2005;95:238–40. doi: 10.2105/AJPH.2004.037812. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Kandel DB, Kiros G-E, Schaffran C, Hu M-C. Racial/ethnic differences in cigarette smoking initiation and progression to daily smoking: a multilevel analysis. Am J Pub Health. 2004;94:128–35. doi: 10.2105/ajph.94.1.128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Ellickson PL, Orlando M, Tucker JS, Klein DJ. From adolescence to young adulthood: racial/ethnic disparities in smoking. Am J Pub Health. 2004;94:293–9. doi: 10.2105/ajph.94.2.293. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Wilkinson AV, Spitz MR, Strom SS, Prokhorov AV, Barcenas CH, Cao Y, Saunders KC, Bondy ML. Effects of nativity, age at migration, and acculturation on smoking among adult Houston residents of Mexican descent. Am J Pub Health. 2005;95:1043–9. doi: 10.2105/AJPH.2004.055319. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Singh GK, Siahpush M. Ethnic-immigrant differentials in health behaviors, morbidity and cause-specific mortality in the United States: an analysis of two national databases. Hum Biol. 2002;74:83–109. doi: 10.1353/hub.2002.0011. [DOI] [PubMed] [Google Scholar]
- 27.Dusenbery L, Epstein JA, Botvin GJ, Diaz T. The relationship between language spoken and smoking among Hispanic-Latino youth in New York City. Pub Health Rep. 1994;109:421–7. [PMC free article] [PubMed] [Google Scholar]
- 28.Kapan CP, Nápoles-Springer A, Stewart SL, Pérez-Stable EJ. Smoking acquisition among adolescents and young Latinas: the role of socioenvironmental and personal factors. Addict Behav. 2001;26:531–50. doi: 10.1016/s0306-4603(00)00143-x. [DOI] [PubMed] [Google Scholar]
- 29.Fagan P, King G, Lawrence D, Petrucci SA, Robinson RG, Banks D, Marable S, Grana R. Eliminating tobacco-related health disparities: directions for future research. Am J Pub Health. 2004;94:211–7. doi: 10.2105/ajph.94.2.211. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.National Cancer Institute. Changing adolescent smoking prevalence: where it is and why. Bethesda, MD: National Cancer Institute; 2001. [Google Scholar]
- 31.Escobedo LG, Peddicord JP. Smoking prevalence in U.S. birth cohorts: the influence of gender and education. Am J Pub Health. 1996;86:231–6. doi: 10.2105/ajph.86.2.231. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Osypuk TL, Kawachi I, Subramanian SV, Acevedo-Garcia D. Are state patterns of smoking different for different racial/ethnic groups? An application of multilevel analysis. Pub Health Rep. 2006;121:563–77. doi: 10.1177/003335490612100512. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.DHHS. Tobacco use among U.S. racial/ethnic minority groups: a report of the Surgeon General. Rockville, MD: DHHS; 1998. p. 56.p. 269. [Google Scholar]
- 34.Griesler PC, Kandel DB. Ethnic differences in correlates of adolescent cigarette smoking. J Adol Health. 1998;23:147–80. doi: 10.1016/s1054-139x(98)00029-9. [DOI] [PubMed] [Google Scholar]
- 35.Griesler PC, Kandel DB, Davies M. Ethnic differences in predictors of initiation and persistence of adolescent cigarette smoking in the National Longitudinal Survey of Youth. Nic Tob Res. 2002;4:79–93. doi: 10.1080/14622200110103197. [DOI] [PubMed] [Google Scholar]
- 36.Wallace JM, Bachman JG, O’Malley PM, Johnston LD. Racial/ethnic differences in adolescent drug use: exploring possible explanations. In: Botvin GJ, Schinke S, Orlandi MA, editors. Drug abuse prevention with multiethnic youth. Thousands Oaks, CA: Sage Publications; 1995. pp. 59–80. [Google Scholar]
- 37.DHHS. Preventing tobacco use among young people: a report of the Surgeon General. Rockville, MD: DHHS; 1994. [PubMed] [Google Scholar]
- 38.Patrick DL, Cheadle A, Thompson DC, Diehr P, Koepsell T, Kinne S. The validity of self-reported smoking: a review and meta-analysis. Am J Pub Health. 1994;84:1086–93. doi: 10.2105/ajph.84.7.1086. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Johnston LD, O’Malley PM, Bachman JG, Schulenberg JE. Appendix C: estimation of sampling errors. Bethesda, MD: National Institute on Drug Abuse; 2005. Monitoring the Future national survey results on drug use 1975–2004: volume 1, secondary school students. [Google Scholar]
- 40.Moon-Howard J. African-American women and smoking: starting later. Am J Pub Health. 2003;93:418. doi: 10.2105/ajph.93.3.418. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Gardiner RS National Cancer Institute. Changing adolescent smoking prevalence: where it is and why. Bethesda, MD: National Cancer Institute; 2001. African American teen cigarette smoking: a review; pp. 213–25. [Google Scholar]
- 42.Trinidad DR, Gilpin EA, Lee L, Pierce JP. Has there been a delay in the age of regular smoking onset among African Americans? Ann Behav Med. 2004;28:152–7. doi: 10.1207/s15324796abm2803_2. [DOI] [PubMed] [Google Scholar]
- 43.King G, Bendel R, Delaronde SR. Social heterogeneity in smoking among African Americans. Am J Pub Health. 1998;88:1081–5. doi: 10.2105/ajph.88.7.1081. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Farrelly MC, Davis KC, Haviland ML, Messeri P, Healton CG. Evidence of a dose-response relationship between “truth” anti-smoking ads and youth smoking. Am J Pub Health. 2005;95:425–31. doi: 10.2105/AJPH.2004.049692. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Gilpin EA, Lee L, Pierce JP. Trends in adolescent smoking initiation in the United States: is tobacco marketing an influence? Tob Control. 1997;6:122–7. doi: 10.1136/tc.6.2.122. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Ross H, Chaloupka FJ. The effect of cigarette prices on youth smoking. Health Econ. 2003;12:217–30. doi: 10.1002/hec.709. [DOI] [PubMed] [Google Scholar]
- 47.Gilpin EA, Lee L, Pierce JP. How have smoking risk factors changed with recent declines in California adolescent smoking? Addiction. 2005;100:117–25. doi: 10.1111/j.1360-0443.2005.00938.x. [DOI] [PubMed] [Google Scholar]
- 48.Johnston LD, O’Malley PM, Bachman JG, Schulenberg JE. Monitoring the Future Occasional Paper No. 61. Ann Arbor, MI: Institute for Social Research; 2005. Demographic subgroup trends for various licit and illicit drugs, 1975–2004. Available online at http://monitoringthefuture.org. [Google Scholar]
- 49.Brown TN, Schulenberg JE, Bachman JG, O’Malley PM, Johnston LD. Are risk and protective factors for substance use consistent across historical time? national data from the high school classes of 1976 through 1997. Prev Sci. 2001;2:29–43. doi: 10.1023/a:1010034912070. [DOI] [PubMed] [Google Scholar]
- 50.Bachman JG, O’Malley PM, Schulenberg JE, Johnston LD, Bryant AL, Merlin AC. The decline of substance use in young adulthood: changes in social activities, roles, beliefs. Mahwah, NJ: Lawrence Erlbaum; 2002. [Google Scholar]