

Abstract
Purpose of review
Chronic obstructive pulmonary disease (COPD) is the fifth cause of mortality in the world. This article reviews diet as a risk or protective factor for COPD, mechanisms of malnutrition, undernutrition consequences on body functioning and how to modulate nutritional status of COPD patients.
Recent findings
Different dietary factors (dietary pattern, foods, nutrients) have been associated with COPD and the course of the disease. Mechanical disadvantage, energy imbalance, disuse muscle atrophy, hypoxemia, systemic inflammation and oxidative stress have been reported to cause systemic consequences such as cachexia and compromise whole body functioning. Nutritional intervention makes it possible to modify the natural course of the disease provide that it is included in respiratory rehabilitation combining bronchodilators optimization, infection control, exercise and in some patients correction of hypogonadism.
Summary
Diet, as a modifiable risk factor, appears more as an option to prevent and modify the course of COPD. Reduction of mechanical disadvantage, physical training and anabolic agents should be used conjointly with oral nutrition supplements to overcome undernutrition and might change the prognosis of the disease in some cases. Major research challenges address the role of systemic inflammation and the best interventions for control it besides smoking cessation.
Keywords: Cachexia; physiopathology; prevention & control; therapy; Diet; Humans; Inflammation; physiopathology; prevention & control; therapy; Inflammation Mediators; metabolism; Nutritional Status; Nutritional Support; methods; Oxidative Stress; Pulmonary Disease, Chronic Obstructive; etiology; physiopathology; prevention & control; therapy; Risk Factors
Keywords: Nutrition disorders, COPD, inflammation, pulmonary rehabilitation, enteral feeding, oral nutrition supplement, anabolic agents, diet
1. Introduction
Nutritional status has been associated with respiratory function in COPD with complex interplays between environmental and genetic factors (Fig. 1) [1•]. Studies have shown that malnutrition served as negative prognostic factor in COPD. Conversely, diet could be a protective or a harmful factor regarding the risk of incident COPD and modifying factor in established disease [2–4]. The question is how we could intervene with nutritional factors to improve prognosis. This review will discuss diet as a risk factor in COPD, mechanisms of malnutrition, consequences of undernutrition on body functioning and how to modulate nutritional status of these patients.
Figure 1.
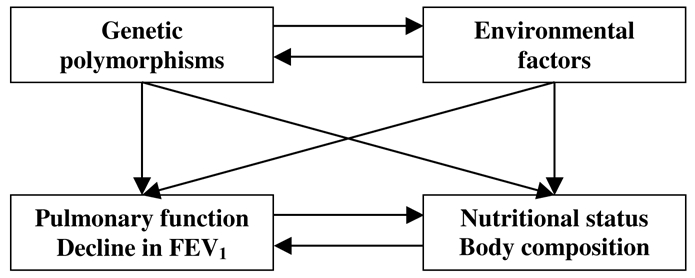
Gene-environnement interactions on body composition and the risk of COPD
2. Diet as a risk factor for COPD
Cigarette smoking is the most important risk factor for COPD, but up to one third of patients with COPD have never smoked [5]. These suggest that other factors, such as diet, also are involved. In the last decade, there has been a growing interest in identifying foods related to lung function or COPD symptoms [5,6,7••]. Nutritional epidemiologists propose to assess overall diet instead of the individual foods or nutrients due to interaction between nutrients [8]. This approach has been used in three recent studies which has used dietary patterns to assess diet in relation with respiratory phenotypes [6,7••,9].
Among the Chinese Singaporeans, a ‘meat-dim sum’ pattern (meat, dim sum foods, and noodle dish) was associated with an increased risk of incident cough with phlegm [9]. In both a large cohort of US men and US women, a “prudent” pattern (high intake of fruits, vegetables, fish and whole grain products) was associated with a decrease risk of newly diagnosed COPD whereas a Western pattern (high intake of refined grains, cured and red meats, desserts and French fries) was associated with an increase of COPD [6,7••].
Most investigations have focused on the possibility that fruits and vegetables exert beneficial effects on lung health and a very little attention has been paid to other foods or nutrients. Recently, it has been suggested that dietary fibre was independently associated with better lung function and reduced prevalence COPD [10,11]. Previous studies have mostly focused on the potentially protective effects of foods rich in antioxidants, and not on foods with a potential deleterious effect. However, it was recently reported both in three longitudinal surveys [7••,12,13] and in a cross-sectional survey[14] that frequent consumption of cured meats was associated with higher prevalence and incidence of COPD. All these studies provide additional support to the hypothesis that diet, a modifiable risk factor, is associated with respiratory diseases. Nutritional epidemiology may play an important role in advancing our understanding of the relevant pathophysiological mechanisms involved in the development and progression of respiratory diseases.
3. Epidemiology and mechanisms of nutritional depletion in COPD
Malnutrition in COPD is one of negative predictive factors and mechanisms of nutritional depletion are multifactorial processes that will be described in the next following paragraphs.
3.1. Epidemiology
Weight loss in COPD was already recognized as a clinical finding and it is more frequent in emphysematous patients as contrary to the blue bloaters [15]. The prevalence of nutritional depletion was about 20–35% in outpatients COPD and up to 70% in patients with acute respiratory failure or in patients awaiting a lung transplantation [4,16–18].
3.2. Mechanisms of nutrition depletion
Nutrition depletion occurs by including several factors such as energy imbalance, disuse atrophy of the muscles, hypoxemia, systemic inflammation, oxidative stress and hypogonadism in some patients.
3.2.1. Energy imbalance and metabolism changes
The largest component of energy expenditure (EE) is the basal metabolic rate (BMR), which is the energy needed for basic processes of life and it accounts for 60–70% of total daily EE [19]. Increased energy expenditure due to mechanic disadvantage, metabolic inefficiency with some fibre type shift in skeletal muscle from type I to type II, together with systemic inflammation may be determinants of an hypermetabolic state that may not be balanced by dietary intake [20••]. In COPD patients, resting energy expenditure (REE) has been reported to be 15–20% above predicted values due to the increased energy required for breathing [21,22]. Total daily expenditure was also higher in COPD patients compared to healthy subjects and it may be caused by increased level of non-resting daily expenditure [23]. Energy expenditure changes due to impaired mechanical efficiency may be partially reversed by reducing hyperinflation with medication, breathing techniques or lung volume reduction. This could reduced oxygen cost for breathing and increased oxygen availability which favours carbohydrate metabolism and recovery in body composition with lower fat and and higher fatfree masses [24–26].
Chronic obstructive lung disease may induce insulin resistance and changes glucose metabolism [27]. Data from the Third National Health and Nutrition Examination Survey showed that impaired glucose regulation was associated with impaired lung function [28]. Glucose plasma concentrations were similar in non-hypoxemic COPD patients and healthy subjects. Abnormal glucose metabolism may be a risk factor for cardiovascular disease and type II diabetes in COPD [29].
Some data showed that increased proteolysis in cystic fibrosis (CF) patients was related to impaired glucose tolerance due to resistance to the anabolic effects of insulin on proteolysis [30]. High catecholamine level in COPD may induce hypermetabolic response which causes increased EE and muscle-protein catabolism [31,32]. These findings suggested some role of insulin resistance in FFM (fat free mass) depletion.
COPD patients often have dyslipidemia related to metabolic syndrome (abdominal obesity, increased triglycerides, dyslipidemia) and it is due to some changes in lipid metabolism. [33]. Jackobsson et al found a decrease in lipolysis and increased glucose levels in patients with advanced COPD with chronic respiratory failure, signaling a role of insulin resistance in the reduction of lipolysis [34]. These findings suggested that FM (fat mass) relatively preserved or increased due to decrease lipolysis.
3.2.2. Disuse atrophy of muscles
Patients with very severe COPD are very inactive as compare to healthy people of the same advanced age [35]. Several studies have shown that these patients have an increased protein breakdown pathways, in particular the NF-kB-activated ubiquitin/proteasomal pathway and apoptosis [36].
3.2.3. Hypoxemia
It has been suggested that the hypoxemia of COPD is one causative factor for cachexia. Hypoxemia may increase the generation of ROS and TNF-α which in turn may give rise to inflammatory changes leading to cachexia [37]. It may stimulate the sympathetic nervous system and this has been shown to produce systemic inflammation [38].
3.2.4. Systemic inflammation and oxidant stress
Systemic inflammation has important metabolic consequences and become the primary focus of research into the genesis of cachexia in COPD. The molecules receiving the greatest amount of attention are TNF-α, IL-1β, IL-6, CRP, and ROS and reactive nitrogen species (see ref.20 for review) and may play a role in cachexia. COPD has been proposed in this context a new syndrome called “chronic systemic inflammatory syndrome” including at least 3 out 6 following factors: age older than 40, more than 10 year-smoking history, symptoms and pulmonary functions compatible with COPD, chronic heart failure, insulin resistance, and increased plasma CRP [39••,40]. There may be also a link between inflammation and leptin levels. Nevertheless, major gaps persist related to environmental and genetic factors underlying cachexia susceptibility, to sequential molecular steps [20••].
3.2.4. Hypogonadism
There is evidence that insufficiency of one or more of three hormones may contribute to cachexia. Creutzberg et al have provided an overview of endocrine factors in COPD [41]. Low levels of circulating hormones do not prove cause and effect in cachexia in COPD. Inversely, anabolic hormones replacement may have a role in selected patients as reported in various publications.
4. Impacts of malnutrition in COPD
Impact of malnutrition in COPD on body functioning will be emphasized on body composition, on lung parenchyma, respiratory function, respiratory mechanics, physical capacity, and also morbidity and mortality.
4.1. Body composition
Patients with COPD are known to be generally underweight and have reduced FFM as showed by several studies [42,43]. Study by Sergi et al showed that COPD patients had a lower FFM as compared to healthy subjects (38% versus 31%) [42]. In a large out-patient population of patients with COPD in Netherlands, they found prevalence of normal BMI and low FFMI was 15%, and of low BMI and low FFMI 11% [17].
4.2. Lung parenchyma, respiratory function and respiratory mechanics
Massaro et al described loss of pulmonary alveoli in calorie restriction and regenerated after ad libitum refeeding [44]. Undernutrition led to lung and chest wall mechanical changes, such as distorted structure of diaphragm and intercostals, reduction of surfactant and decrease in elastic fibre content of pulmonary parenchyma [45]. Inspiratory muscle weakness and maximum inspiratory pressure generation was an independent determinant of survival in severe COPD [46]. The diaphragm as a main inspiratory muscle is suffered from muscle protein degradation and loss of contractile protein [47]. In study by Cano et al the degree of respiratory impairment (FEV1, FVC and 6-min walking test) was correlated with nutritional status especially FFM [48].
4.3. Physical capacity
Daily physical activity can be considered as “the totality of voluntary movement produced by skeletal muscles during everyday functioning” [49]. It is widely known that in patients with COPD, lower levels of physical activity in daily life are related to higher risk of hospital readmission and shorter survival. The effect of skeletal muscle dysfunction contributes to declining body functioning as we defined as physical activity. Physical activity greatly influences patient outcomes because level of physical activities was shown to predict the risk for hospitalization [50,51]. Overall impairment of body functioning can be described in Figure 2 as adapted from International Classification of Functioning (ICF) [52].
Figure 2.
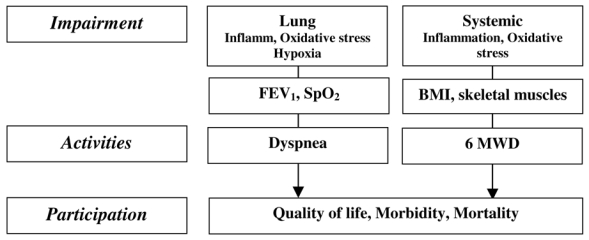
COPD as systemic disease in the context of the International Classification of Functioning, ICF-2, WHO 2001[52,83]
Abbreviations: BMI: body mass index, 6MWT : 6 minutes walking test, FEV1%: percentage of predicted FEV1
4.4. Morbidity and mortality
Mortality of COPD patients and occurrence of acute exacerbation requiring hospitalization are higher in underweight patients. During hospitalization, COPD patients are most likely to loose weight because of the higher metabolic demand due to increased ventilatory disadvantage or infection and underweight patients also had a higher risk of new exacerbation [53]. Landbo et al described that in mild to moderate COPD the best prognosis was found in normal weight or overweight subjects, whereas in severe COPD, overweight or obese patients were associated with a better survival. These patients may be somehow protected from weight loss because of higher energy reserves [54].
5. How to intervene
The questions on how to intervene in these patients exist and we will discuss how and possible methods to modify disease progression or prognosis.
5.1. Nutrition requirements
The question on how much we should give nutritional repletion still remains. In the study by Planas et al, it was described that total daily energy intake of REE x 1.3 was preferable than REE x 1.7 in mild stable COPD patients. They found that administration of nutritional supplements, high in proteins, with predominance of carbohydrates over fat, and enriched in antioxidants to achieve total daily defined energy intake in patients in group REE x 1.3 was followed by a significant improvement of body weight, handgrip strength, decrease airflow limitation and increase quality of life [55]. Total calories being administered as 20% proteins seemed to be the optimal in nutritional supplements for stable malnourished COPD patients. Small portion of carbohydrate and protein-rich supplementation seemed to have an impact on weight gain after 8 weeks when compared to normal size supplements of similar macronutrient composition, probably because many patients still usually took ordinary meals outside the supplementation [56]. High load of portion will compromise diaphragm movement and caused postprandial dyspnea because it will prevent the diaphragm to move easily due to gastric filling pressure [57].
5.2. Methods
Metabolic syndrome carries a lot of consequences in managing nutrition in COPD patients because of glucose level, hypertension, atherogenic dyslipidemia or other co-morbidities such as congestive heart failure. Methods that are known for nutritional intervention in COPD patients varied between studies.
5.2.1. Oral nutrition supplements
Nutritional support includes food enrichments, oral nutritional supplements, tube feeding and parenteral nutrition.[58] There is limited evidence that wasting COPD patients will benefit only with enteral nutrition as showed by meta-analysis by Ferreira et al[59] and reported in ESPEN recommendations in 2006[57]. Table I described some nutritional supplementation studies in COPD patients which were integrated or non-integrated with pulmonary rehabilitation. Refeeding in malnourished COPD patients is not easy and difficult to maintain due to many factors. The 2005 Cochrane Review on nutritional supplementation for stable COPD had some important limitations relative to the small numbers of patients included, 214 in supplement arm versus 205 in control group, the non-integration of nutritional intervention in a pulmonary rehabilitation process, the short duration of intervention between 2 weeks to 3 months, and the lack of relevant endpoints to measure the effects of nutrition supplementation as quality of life, body composition or exercise capacity [57,68]. These limitations should encourage larger studies with a multimodality approaches and clinically relevant end-points.
Table I.
Nutritional supplementation studies with more than 2 weeks supplementation in COPD patients, integrated (filled in grey) and non integrated with rehabilitation programme (includes only studies after year 1990)
| Author, year | Patient’s characteristics, settings | Study design | n, supplementation group/control, intervention | Judgements criteria Results |
|---|---|---|---|---|
| Faager et al, 2006[58] | COPD patients with FEV1 < 70%, outpatients | Randomized, double-blind, placebo-controlled study | 23, 13/10, creatine supplementation & exercise training | Physical performance, lung function test No significant improvement |
| Fuld et al, 2005[59] | Moderate to severe COPD, outpatients | Randomized double-blind, placebo-controlled study | 38, 20/18, creatine nutritional supplementation, pulmonary rehabilitation | Fat-free mass, peripheral muscle strength and endurance, health status Significant improvement in all parameters, except exercise capacity |
| Matsuyama et al, 2005[60] | COPD patients FEV1 < 60% | Randomized, double-blind controlled study | 64, 32/32, nutritional support with omega-3 PUFA-rich diets | Leukotriene B4 levels, tumor necrosis factor-alpha and interleukin-8 levels Decreased significantly in the n-3 group |
| Pison, 2004[61] | Chronic respiratory failure at home, on NIV and/or LTOT | 3-month randomized, controlled study, at home | 122, 60/62, health education + pulmonary rehabilitation + androgens + oral nutritional supplements, 560 kcal/day versus health education alone | 6MWD, quality of life, body composition, exercise capacity, exacerbation rate, survival Inclusions completed, results pending |
| Vermeeren et al, 2004[62] | Nutritionally depleted COPD patients, hospitalized patients | Randomized double-blind, placebo-controlled study | 57, Energy and protein-rich nutritional supplements during hospitalization for an acute exacerbation | Body composition, respiratory and skeletal muscle strength, lung function and symptoms No significant improvements in lung function or muscle strength |
| Steiner, 2003[63] | Nutritionally depleted COPD patients, outpatients | Prospective, controlled study | 85, 42/43, oral supplementation, 570 kcal/j, pulmonary rehabilitation | Body weight, body composition, quality of life (CRQ), quadriceps muscle forces, hand grip, shuttle test Improvement of shuttle test and quality of life |
| Creutzberg, 2003[64] | Nutritionally depleted COPD patients, outpatients | Prospective, controlled study | 69/28, oral supplementation 570 kcal/day, pulmonary rehabilitation | Body weight, body composition, lung function, hand grip, respiratory muscle forces, maximal exercice test, quality of life Improvements of body weight, fat free mass, hand grip, respiratory muscle forces |
| Rogers, 1992[65] | Malnourished COPD patients, hospitalized then outpatients | Prospective, controlled study | Oral supplementation, no pulmonary rehabilitation | Body weight, respiratory muscle forces, hand grip, lung function, 6MWT Improvement of body weight, hand grip, respiratory muscle forces, 6MWT |
| Fuenzalida, 1990[66] | Nutritionally depleted, hospitalized then outpatients | Prospective, controlled study | 9, 5/4, oral supplementation, 1080 kcal/day, no pulmonary rehabilitation | Body weight, anthropometry, immune response Improvement of imuunity status |
| Whittaker, 1990[67] | Nutritionally depleted, hospitalized | Prospective, controlled study | 10, 6/4, nasogastric tube supplementation + 1000 kcal versus + 100 kcal, 16 days, no rehabilitation | Body weight, respiratory muscle forces, hand grip, lung function Improvement of body weight and respiratory muscle forces |
Abbreviations: PImax: maximal inspiratory mouth pressure; PEmax: maximal expiratory mouth pressure; MVV: Maximal Voluntary Ventilation; 6MWT: 6 minutes walking test; REE: Resting Energy Expenditure
5.2.2. Exercise
Physical training will also have positive effects as anabolic process as it can increase FFM and functional status although it did not directly correlated [69]. Some others studies showed that physical training only will cause negative energy balance because of increase total energy expenditure, but this effect can be overcome by giving supplementation rich in carbohydrate. Glycogen storage is low in muscle of COPD patients and therefore carbohydrate can serve as better energy source [70].
5.2.3. Anabolic agents
Anorexia is one of many factors contributes to cachexia in COPD. The use of appetite stimulating therapy in cachexia COPD patients is now getting more attention [71]. Progestogens (megestrol acetate) can be used to treat anorexia-cachexia. This agent can stimulate appetite and has antagonist effects of pro-inflammatory cytokines [72]. Androgenic hormones has been reported with some successes when combined with exercise, but problems of extra physiologic doses remain [73] (Table II)
Table II.
Effects of anabolic agents in COPD patients integrated (filled in grey) and non-integrated with rehabilitation programme
| Author, year | Patient’s characteristics, settings | Study design | n, supplementation group/control, intervention | Judgements criteria Results |
|---|---|---|---|---|
| Casaburi, 2004[74] | FEV1 of 60% predicted or less, FEV1 to vital capacity ratio of 60% or less, outpatients | Prospective, randomized, controlled, double-blind study, rehabilitation in 2 out 4 groups | 47, 100 mg/week testosterone enanthate in sesame oil | Body weight, body composition, respiratory muscle function Significant increased lean body mass |
| Creutzberg, 2003[75] | FEV1 < 70% predicted, FEV1increase ≤ 10% after inhalation β2-agonist, outpatient | Prospective, randomized, controlled, double-blind study Pulmonary rehabilitation |
63, 33/30, 50 mg of nandrolone decanoate IM | Body composition, muscle function, exercise capacity, health status, erythropoietic parameters, laboratory parameters Improvements in muscle function and exercise capacity |
| Yeh, 2002[76] | FEV1 < 50% predicted, FEV1/FVC ratio < 70%, weight≤90% ideal body weight, outpatient | Prospective, open-label, 4-month clinical trial | 128, oxandrolone, 10 mg bid | Body weight, body composition, spirometry, 6MWT Significant weight gain |
| Ferreira, 1998[77] | BMI below 20 kg/m2, the maximal inspiratory pressure (PImax) was below 60% of the predicted value, outpatient | Prospective, randomized, controlled, double-blind study Pulmonary rehabilitation |
17, 7/10, 250 mg of testosterone IM at baseline and 12 mg of oral stanozolol a day for 27 weeks | Body mass index (BMI), lean body mass, anthropometric measures, respiratory muscle strength, and functional exercise capacity Increases in BMI, lean body mass, and anthropometric measures of arm and thigh circumference |
| Burdet, 1997[78] | FEV1/FVC ratio ≤ 70% predicted, FEV1increase ≤ 10% after albuterol inhalation, BMI ≤ ideal body weight, outpatient | Prospective, randomized, double blind, controlled study Pulmonary rehabilitation |
16, 8/8, subcutaneous injection of 0.15 IU/kg rhGH | Nutritional status, resting metabolism, muscle strength, exercise tolerance, dyspnea Increases lean body mass in underweight patients |
5.2.4. Multimodality approaches
A holistic approaches such as the combination of adequate nutritional support with reduction of mechanical insufficiency (with drugs, lung volume reduction, breathing technique), physical activity, anabolic agents or appetite stimulants and non-invasive ventilation will give these patients potential improvements strategy [24,25,79].
5.2.5. New tools
Studies also have shown encouraging effects of n-3 polyunsaturated fatty acids (PUFAs) on cytokine release, markers of immune function, on exercise capacity and FFM of COPD patients [80]. Therefore nutrition support with PUFA can be considered to give positive effect for these patients. Oxygen supplementation could reduce dynamic hyperinflation at rest and during or after exercise due to changes in ventilatory pattern [81]. A significant weight gain was observed in malnourished COPD patients after NPPV initiation due to reduce hyperinflation which can help diaphragm to work more efficiently and avoid dyspnea when eating (gastric filling) [82]. A better knowledge of molecular steps and targets involved in systemic consequences of COPD is of paramount importance to have better treatments. As an example, it appeared that the peroxisome proliferator-activated receptors (PPARs) are involved in cachexia, decreased oxidative muscle metabolism, oxidative stress and systemic inflammation suggesting role for PPARs agonists [83].
Conclusion and non-answered questions
Nutritional depletion has been widely reported in COPD patients. Diet may also play a role both in the development and the progression of the disease. Holistic management for these patients should include nutritional modulation beside reduction of mechanical disadvantage with long-acting bronchodilators, lung volume reduction, physical activity, anabolic agents or appetite stimulants and non-invasive ventilation. Furthermore, metabolic syndrome must be considered in the management of COPD in order to avoid any co-morbidities complication.
References and recommended reading
Papers of particular interest, published within the annual period of review, have been highlighted as:
• of special interest attention only for publication in 2007–2008
•• of outstanding interest idem
- 1•.Rabe KF, Hurd S, Anzueto A, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2007;176:532–555. doi: 10.1164/rccm.200703-456SO. Guideline for management of patients with COPD. [DOI] [PubMed] [Google Scholar]
- 2.Schols AM, Broekhuizen R, Weling-Scheepers CA, et al. Body composition and mortality in chronic obstructive pulmonary disease. Am J Clin Nutr. 2005;82:53–59. doi: 10.1093/ajcn.82.1.53. [DOI] [PubMed] [Google Scholar]
- 3.Vestbo J, Prescott E, Almdal T, et al. Body mass, fat-free body mass, and prognosis in patients with chronic obstructive pulmonary disease from a random population sample findings from the Copenhagen City Heart Study. Am J Respir Crit Care Med. 2006;173:79–83. doi: 10.1164/rccm.200506-969OC. [DOI] [PubMed] [Google Scholar]
- 4.Hallin R, Gudmundsson G, Suppli Ulrik C, et al. Nutritional status and long-term mortality in hospitalised patients with chronic obstructive pulmonary disease (COPD) Respir Med. 2007;101:1954–1960. doi: 10.1016/j.rmed.2007.04.009. [DOI] [PubMed] [Google Scholar]
- 5.Viegi G, Pistelli F, Sherrill DL, et al. Definition, epidemiology and natural history of COPD. Eur Respir J. 2007;30:993–1013. doi: 10.1183/09031936.00082507. [DOI] [PubMed] [Google Scholar]
- 6.Varraso R, Fung TT, Barr RG, et al. Prospective study of dietary patterns and chronic obstructive pulmonary disease among US women. Am J Clin Nutr. 2007;86:488–495. doi: 10.1093/ajcn/86.2.488. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7•.Varraso R, Jiang R, Barr RG, et al. Prospective study of cured meats consumption and risk of chronic obstructive pulmonary disease in men. Am J Epidemiol. 2007;166:1438–1445. doi: 10.1093/aje/kwm235. A new risk factor in COPD. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Hu F. Dietary pattern analysis: a new direction in nutritional epidemiology. Curr Opin Lipidol. 2002;13:3–9. doi: 10.1097/00041433-200202000-00002. [DOI] [PubMed] [Google Scholar]
- 9.Butler LM, Koh W-P, Lee H-P, et al. Prospective study of dietary atterns and persistent cough with phlegm among Chinese Singaporeans. Am J Respir Crit Care Med. 2006;173:264–270. doi: 10.1164/rccm.200506-901OC. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Kan H, Stevens J, Heiss G, et al. Dietary fiber, lung function, and chronic obstructive pulmonary disease in the atherosclerosis risk in communities study. Am J Epidemiol. 2007;167:570–578. doi: 10.1093/aje/kwm343. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Romieu I. Nutrition and lung health. Int J Tuberc Lung Dis. 2005;9:362–374. [PubMed] [Google Scholar]
- 12.Butler LM, Koh W-P, Lee H-P, et al. On Previous Findings Concerning Preserved Meat Intake and Respiratory Disease. Am J Respir Crit Care Med. 2007;176:315. doi: 10.1164/ajrccm.176.3.315. [DOI] [PubMed] [Google Scholar]
- 13.Jiang R, Camargo C, Varraso R, et al. Consumption of cured meats and prospective risk of chronic obstructive pulmonary disease in women. In Am J Clin Nutr. 2008 doi: 10.1093/ajcn/87.4.1002. Edited by. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Jiang R, Paik DC, Hankinson JL, et al. Cured meat consumption, lung function, and chronic obstructive pulmonary disease among United States dults. Am J Respir Crit Care Med. 2007;175:798–804. doi: 10.1164/rccm.200607-969OC. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Wouters EF. Nutrition and metabolism in COPD. Chest. 2000;117:274S–280S. doi: 10.1378/chest.117.5_suppl_1.274s. [DOI] [PubMed] [Google Scholar]
- 16.Budweiser S, Meyer K, Jorres RA, et al. Nutritional depletion and its relationship to respiratory impairment in patients with chronic respiratory failure due to COPD or restrictive thoracic diseases. Eur J Clin Nutr. 2007;62:436–437. doi: 10.1038/sj.ejcn.1602708. [DOI] [PubMed] [Google Scholar]
- 17.Vermeeren MAP, Creutzberg EC, Schols AMWJ, et al. Prevalence of nutritional depletion in a large out-patient population of patients with COPD. Respiratory Medicine. 2006;100:1349–1355. doi: 10.1016/j.rmed.2005.11.023. [DOI] [PubMed] [Google Scholar]
- 18.Schwebel C, Pin I, Barnoud D, et al. Prevalence and consequences of nutritional depletion in lung transplant candidates. Eur Respir J. 2000;16:1050–1055. doi: 10.1034/j.1399-3003.2000.16f05.x. [DOI] [PubMed] [Google Scholar]
- 19.Steele B, Holt L, Belza B, et al. Quantitating physical activity in COPD using a triaxial accelerometer. Chest. 2000;117:1359–1367. doi: 10.1378/chest.117.5.1359. [DOI] [PubMed] [Google Scholar]
- 20••.Wagner P. Possible mechanisms underlying the development of cachexia in COPD. Eur Respir J. 2008;31:492–501. doi: 10.1183/09031936.00074807. The most recent review on mechanisms of cachexia in COPD. [DOI] [PubMed] [Google Scholar]
- 21.Hugli O, Schutz Y, Fitting JW. The daily energy expenditure in stable chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1996;153:294–300. doi: 10.1164/ajrccm.153.1.8542132. [DOI] [PubMed] [Google Scholar]
- 22.Ezzell L, Jensen GL. Malnutrition in chronic obstructive pulmonary disease. Am J Clin Nutr. 2000;72:1415–1416. doi: 10.1093/ajcn/72.6.1415. [DOI] [PubMed] [Google Scholar]
- 23.Baarends EM, Schols AM, Pannemans DL, et al. Total free living energy expenditure in patients with severe chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1997;155:549–554. doi: 10.1164/ajrccm.155.2.9032193. [DOI] [PubMed] [Google Scholar]
- 24.O’Donnell D, Sciurba F, Celli B, et al. Effect of fluticasone propionate/salmeterol on lung hyperinflation and exercise endurance in COPD. Chest. 2006;130:647–656. doi: 10.1378/chest.130.3.647. [DOI] [PubMed] [Google Scholar]
- 25.Mineo TC, Pompeo E, Mineo D, et al. Resting energy expenditure and metabolic changes after lung volume reduction surgery for emphysema. Ann Thorac Surg. 2006;82:1205–1211. doi: 10.1016/j.athoracsur.2006.05.030. [DOI] [PubMed] [Google Scholar]
- 26.Vaughan P, Oey IF, Steiner MC, et al. A prospective analysis of the inter-relationship between lung volume reduction surgery and body mass index. Eur J Cardiothorac Surg. 2007;32:839–842. doi: 10.1016/j.ejcts.2007.09.016. [DOI] [PubMed] [Google Scholar]
- 27.Sauerwein HP, Schols AM. Glucose metabolism in chronic lung disease. Clin Nutr. 2002;21:367–371. doi: 10.1054/clnu.2002.0561. [DOI] [PubMed] [Google Scholar]
- 28.McKeever TM, Weston PJ, Hubbard R, et al. Lung function and glucose metabolism: An analysis of data from the third National Health and Nutrition Examination Survey. Am J Epidemiol. 2005;161:546–556. doi: 10.1093/aje/kwi076. [DOI] [PubMed] [Google Scholar]
- 29.Bolton CE, Evans M, Ionescu AA, et al. Insulin resistance and inflammation- a further systemic complication of COPD. COPD. 2007;4:121–126. doi: 10.1080/15412550701341053. [DOI] [PubMed] [Google Scholar]
- 30.Hardin DS, LeBlanc A, Lukenbaugh S, et al. Proteolysis associated with insulin resistance in cystic fibrosis. Pediatrics. 1998;101:433–437. doi: 10.1542/peds.101.3.433. [DOI] [PubMed] [Google Scholar]
- 31.Hofford J, Milakofsky L, Vogel W, et al. The nutritional status in advanced emphysema associated with chronic bronchitis. A study of amino acid and catecholamine levels. Am Rev Respir Dis. 1990;141:902–908. doi: 10.1164/ajrccm/141.4_Pt_1.902. [DOI] [PubMed] [Google Scholar]
- 32.Herndon DN, Hart DW, Wolf SE, et al. Reversal of catabolism by beta-blockade after severe burns. N Engl J Med. 2001;345:1223–1229. doi: 10.1056/NEJMoa010342. [DOI] [PubMed] [Google Scholar]
- 33.Marquis K, Maltais F, Duguay V, et al. The metabolic syndrome in patients with chronic obstructive pulmonary disease. J Cardiopulm Rehabil. 2005;25:226–232. doi: 10.1097/00008483-200507000-00010. discussion 233–224. [DOI] [PubMed] [Google Scholar]
- 34.Jakobsson E, Jorfeldt L. Blood fuel metabolites at rest and during exercise in patients with advanced chronic obstructive pulmonary disease with and without chronic respiratory failure. Respiration. 1990;57:304–309. doi: 10.1159/000195861. [DOI] [PubMed] [Google Scholar]
- 35.Pitta F, Troosters T, Spruit MA, et al. Characteristics of physical activities in daily life in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2005;171:972–977. doi: 10.1164/rccm.200407-855OC. [DOI] [PubMed] [Google Scholar]
- 36.Agusti A, Morla M, Sauleda J, et al. NF-kappaB activation and iNOS upregulation in skeletal muscle of patients with COPD and low body weight. Thorax. 2004;59:483–487. doi: 10.1136/thx.2003.017640. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Takabatake N, Nakamura H, Abe S, et al. The relationship between chronic hypoxemia and activation of the tumor necrosis factor-alpha system in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2000;161:1179–1184. doi: 10.1164/ajrccm.161.4.9903022. [DOI] [PubMed] [Google Scholar]
- 38.Andreas S, Anker SD, Scanlon PD, et al. Neurohumoral activation as a link to systemic manifestations of chronic lung disease. Chest. 2005;128:3618–3624. doi: 10.1378/chest.128.5.3618. [DOI] [PubMed] [Google Scholar]
- 39••.Fabbri L, Rabe K. From COPD to chronic systemic inflammatory syndrome? Lancet. 2007;370:797–799. doi: 10.1016/S0140-6736(07)61383-X. Proposition to include COPD in a new syndrome: chronic systemic inflammatory syndrome. [DOI] [PubMed] [Google Scholar]
- 40.Agusti A. Systemic effects of chronic obstructive pulmonary disease: what we know and what we don’t know (but should) Proc Am Thorac Soc. 2007;4:522–525. doi: 10.1513/pats.200701-004FM. [DOI] [PubMed] [Google Scholar]
- 41.Creutzberg EC, Casaburi R. Endocrinological disturbances in chronic obstructive pulmonary disease. Eur Respir J Suppl. 2003;46:76s–80s. doi: 10.1183/09031936.03.00004610. [DOI] [PubMed] [Google Scholar]
- 42.Sergi G, Coin A, Marina S, et al. Body composition and resting energy expenditure in elderly male patients with chronic obstructive pulmonary disease. Respiratory Medicine. 2006;100:1918–1924. doi: 10.1016/j.rmed.2006.03.008. [DOI] [PubMed] [Google Scholar]
- 43.Schols A, Slangen J, Volovics L, et al. Weight loss is a reversible factor in the prognosis of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1998;157:1791–1797. doi: 10.1164/ajrccm.157.6.9705017. [DOI] [PubMed] [Google Scholar]
- 44.Massaro D, Massaro GD, Baras A, et al. Calorie-related rapid onset of alveolar loss, regeneration, and changes in mouse lung gene expression. Am J Physiol Lung Cell Mol Physiol. 2004;286:L896–906. doi: 10.1152/ajplung.00333.2003. [DOI] [PubMed] [Google Scholar]
- 45.Chamberlain JS. Cachexia in Cancer-Zeroing in on myosin. N Engl J Med. 2004;351:2124–2125. doi: 10.1056/NEJMcibr042889. [DOI] [PubMed] [Google Scholar]
- 46.Ottenheijm CAC, Heunks LMA, Dekhuijzen PNR. Diaphragm muscle fiber dysfunction in chronic obstructive pulmonary disease: Toward a pathophysiological concept. Am J Respir Crit Care Med. 2007;175:1233–1240. doi: 10.1164/rccm.200701-020PP. [DOI] [PubMed] [Google Scholar]
- 47.Ottenheijm CAC, Heunks LMA, Sieck GC, et al. Diaphragm dysfunction in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2005;172:200–205. doi: 10.1164/rccm.200502-262OC. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Cano NJM, Roth H, Court-Fortune I, et al. Nutritional depletion in patients on long-term oxygen therapy and/or home mechanical ventilation. Eur Respir J. 2002;20:30–37. doi: 10.1183/09031936.02.01812001. [DOI] [PubMed] [Google Scholar]
- 49.Pitta F, Troosters T, Probst VS, et al. Quantifying physical activity in daily life with questionnaires and motion sensors in COPD. Eur Respir J. 2006;27:1040–1055. doi: 10.1183/09031936.06.00064105. [DOI] [PubMed] [Google Scholar]
- 50.Watz H, Waschki B, Boehme C, et al. Extrapulmonary effects of chronic obstructive pulmonary disease on physical activity. Am J Respir Crit Care Med. 2007:200707–201011OC. doi: 10.1164/rccm.200707-1011OC. [DOI] [PubMed] [Google Scholar]
- 51.Cano NJ, Pichard C, Roth H, et al. C-reactive protein and body mass index predict outcome in end-stage respiratory failure. Chest. 2004;126:540–546. doi: 10.1378/chest.126.2.540. [DOI] [PubMed] [Google Scholar]
- 52.World Health Organization. Towards a Common Language for Functioning, Disability and Health: ICF. Geneva: 2002. [Accessed on 12 February 2008]. Available from: http://www3.who.int/icf/beginners/bg.pdf. [Google Scholar]
- 53.Hallin R, Koivisto-Hursti U-K, Lindberg E, et al. Nutritional status, dietary energy intake and the risk of exacerbations in patients with chronic obstructive pulmonary disease (COPD) Respiratory Medicine. 2006;100:561–567. doi: 10.1016/j.rmed.2005.05.020. [DOI] [PubMed] [Google Scholar]
- 54.Landbo C, Prescott EVA, Lange P, et al. Prognostic value of nutritional status in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1999;160:1856–1861. doi: 10.1164/ajrccm.160.6.9902115. [DOI] [PubMed] [Google Scholar]
- 55.Planas M, Alvarez J, Garcia-Peris PA, et al. Nutritional support and quality of life in stable chronic obstructive pulmonary disease (COPD) patients. Clinical Nutrition. 2005;24:433–441. doi: 10.1016/j.clnu.2005.01.005. [DOI] [PubMed] [Google Scholar]
- 56.Broekhuizen R, Creutzberg EC, Weling-Scheepers CA, et al. Optimizing oral nutritional drink supplementation in patients with chronic obstructive pulmonary disease. Br J Nutr. 2005;93:965–971. doi: 10.1079/bjn20051437. [DOI] [PubMed] [Google Scholar]
- 57.Anker SD, John M, Pedersen PU, et al. ESPEN Guidelines on Enteral Nutrition: Cardiology and pulmonology. Clin Nutr. 2006;25:311–318. doi: 10.1016/j.clnu.2006.01.017. [DOI] [PubMed] [Google Scholar]
- 58.Lochs H, Allison SP, Meier R, et al. Introductory to the ESPEN guidelines on enteral nutrition: Terminology, definitions and general topics. Clinical Nutrition. 2006;25:180–186. doi: 10.1016/j.clnu.2006.02.007. [DOI] [PubMed] [Google Scholar]
- 59.Ferreira IM, Brooks D, Lacasse Y, et al. Nutritional supplementation for stable chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2005:CD000998. doi: 10.1002/14651858.CD000998.pub2. [DOI] [PubMed] [Google Scholar]
- 60.Franssen FM, Broekhuizen R, Janssen PP, et al. Effects of whole-body exercise training on body composition and functional capacity in normal-weight patients with COPD. Chest. 2004;125:2021–2028. doi: 10.1378/chest.125.6.2021. [DOI] [PubMed] [Google Scholar]
- 61.Steiner MC, Barton RL, Singh SJ, et al. Nutritional enhancement of exercise performance in chronic obstructive pulmonary disease: a randomised controlled trial. Thorax. 2003;58:745–751. doi: 10.1136/thorax.58.9.745. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Koehler F, Doehner W, Hoernig S, et al. Anorexia in chronic obstructive pulmonary disease-- association to cachexia and hormonal derangement. Int J Cardiol. 2007;119:83–89. doi: 10.1016/j.ijcard.2006.07.088. [DOI] [PubMed] [Google Scholar]
- 63.Femia RA, Goyette RE. The science of megestrol acetate delivery: potential to improve outcomes in cachexia. BioDrugs. 2005;19:179–187. doi: 10.2165/00063030-200519030-00004. [DOI] [PubMed] [Google Scholar]
- 64.Casaburi R, Bhasin S, Cosentino L, et al. Effects of testosterone and resistance training in men with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2004;170:870–878. doi: 10.1164/rccm.200305-617OC. [DOI] [PubMed] [Google Scholar]
- 65.Anker SD, John M, Pedersen PU, et al. ESPEN guidelines on enteral nutrition: cardiology and pulmonology. Clin Nutr. 2006;25:311–318. doi: 10.1016/j.clnu.2006.01.017. [DOI] [PubMed] [Google Scholar]
- 66.Broekhuizen R, Wouters EFM, Creutzberg EC, et al. Polyunsaturated fatty acids improve exercise capacity in chronic obstructive pulmonary disease. Thorax. 2005;60:376–382. doi: 10.1136/thx.2004.030858. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Budweiser S, Heinemann F, Fischer W, et al. Long-term reduction of hyperinflation in stable COPD by non-invasive nocturnal home ventilation. Respiratory Medicine. 2005;99:976–984. doi: 10.1016/j.rmed.2005.02.007. [DOI] [PubMed] [Google Scholar]
- 68.Budweiser S, Heinemann F, Meyer K, et al. Weight gain in cachectic COPD patients receiving noninvasive positive-pressure ventilation. Respir Care. 2006;51:126–132. [PubMed] [Google Scholar]
- 69.Remels AH, Schrauwen P, Broekhuizen R, et al. Peroxisome proliferator-activated receptor expression is reduced in skeletal muscle in COPD. Eur Respir J. 2007;30:245–252. doi: 10.1183/09031936.00144106. [DOI] [PubMed] [Google Scholar]
- 70.Faager G, Söderlund K, Sköld C, et al. Creatine supplementation and physical training in patients with COPD: a double blind, placebo-controlled study. Int J Chron Obstruct Pulmon Dis. 2006;1:445–453. doi: 10.2147/copd.2006.1.4.445. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Fuld JP, Kilduff LP, Neder JA, et al. Creatine supplementation during pulmonary rehabilitation in chronic obstructive pulmonary disease. Thorax. 2005;60:531–537. doi: 10.1136/thx.2004.030452. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Matsuyama W, Mitsuyama H, Watanabe M, et al. Effects of Omega-3 Polyunsaturated Fatty Acids on Inflammatory Markers in COPD. Chest. 2005;128:3817–3827. doi: 10.1378/chest.128.6.3817. [DOI] [PubMed] [Google Scholar]
- 73.Pison C, Cano N, Cherion C, et al. Effects of home pulmonary rehabilitation in patients with chronic respiratory failure and nutritional depletion. Rev Mal Respir. 2004;21:573–582. doi: 10.1016/s0761-8425(04)71362-5. [DOI] [PubMed] [Google Scholar]
- 74.Vermeeren MA, Wouters EF, Geraerts-Keeris AJ, et al. Nutritional support in patients with chronic obstructive pulmonary disease during hospitalization for an acute exacerbation; a randomized controlled feasibility trial. Clin Nutr. 2004;23:1184–1192. doi: 10.1016/j.clnu.2004.03.008. [DOI] [PubMed] [Google Scholar]
- 75.Creutzberg EC, Wouters EF, Mostert R, et al. Efficacy of nutritional supplementation therapy in depleted patients with chronic obstructive pulmonary disease. Nutrition. 2003;19:120–127. doi: 10.1016/s0899-9007(02)00841-9. [DOI] [PubMed] [Google Scholar]
- 76.Rogers R, Donahoe M, Constantino J. Physiologic effects of oral supplementation feeding in malnourished patients with COPD: a randomized control study. Am Rev Respir Dis. 1992;146:1511–1517. doi: 10.1164/ajrccm/146.6.1511. [DOI] [PubMed] [Google Scholar]
- 77.Fuenzalida CE, Petty TL, Jones ML, et al. The immune response to short-term nutritional intervention in advanced chronic obstructive pulmonary disease. Am Rev Respir Dis. 1990;142:49–56. doi: 10.1164/ajrccm/142.1.49. [DOI] [PubMed] [Google Scholar]
- 78.Whittaker JS, Ryan CF, Buckley PA, et al. The effects of refeeding on peripheral and respiratory muscle function in malnourished chronic obstructive pulmonary disease patients. Am Rev Respir Dis. 1990;142:283–288. doi: 10.1164/ajrccm/142.2.283. [DOI] [PubMed] [Google Scholar]
- 79.Creutzberg EC, Wouters EF, Mostert R, et al. A role for anabolic steroids in the rehabilitation of patients with COPD? A double-blind, placebo-controlled, randomized trial. Chest. 2003;124:1733–1742. doi: 10.1378/chest.124.5.1733. [DOI] [PubMed] [Google Scholar]
- 80.Yeh S-s, DeGuzman B, Kramer T. Reversal of COPD-Associated Weight Loss Using the Anabolic Agent Oxandrolone*. Chest. 2002;122:421–428. doi: 10.1378/chest.122.2.421. [DOI] [PubMed] [Google Scholar]
- 81.Ferreira IM, Verreschi IT, Nery LE, et al. The influence of 6 months of oral anabolic steroids on body mass and respiratory muscles in undernourished COPD patients. Chest. 1998;114:19–28. doi: 10.1378/chest.114.1.19. [DOI] [PubMed] [Google Scholar]
- 82.Burdet L, de Muralt B, Schutz Y, et al. Administration of growth hormone to underweight patients with chronic obstructive pulmonary disease. A prospective, randomized, controlled study. Am J Respir Crit Care Med. 1997;156:1800–1806. doi: 10.1164/ajrccm.156.6.9704142. [DOI] [PubMed] [Google Scholar]
- 83.Agusti A, Soriani J. Dynamic hyperinflation and pulmonary inflammation: a potentially relevant relationship. Eur Resp Rev. 2006;100:68–71. [Google Scholar]