

Abstract
In his theory of emotional inhibition Pennebaker [44] proclaimed that the disclosure of stressful or traumatic experiences reduces the probability of detrimental health effects. In his experimental paradigm disclosure was induced by asking the participants to write about their deepest thoughts and feelings relating to a stressful event during 3 to 4 writing sessions of 15 to 20 minutes. Based on a meta-analysis of 13 studies Smyth [58] reported an average effect size of d=0.47 for various health related variables. Considering the great number of studies published since then, the aim of our study was to update the state of evidence regarding the effects of expressive writing on health, including only randomized controlled trials in our analysis. From 42 trials fulfilling the inclusion criteria 30 could be used for the meta-analysis. Neither regarding somatic nor psychological health variables significant effect sizes were found. Various exploratory analyses (e.g. restriction to clinical samples) also resulted in non-significant effect sizes, except for one rendering a very small effect size. Results of our meta-analysis lead to the conclusion that expressive writing has minor or no effects on the subject’s health contrary to earlier findings.
Keywords: emotional inhibition, expressive writing, disclosure, meta-analysis
Abstract
In der Theorie der emotionalen Inhibition von Pennebaker [44] wird angenommen, dass "disclosure" (Selbstöffnung) bzgl. traumatischer Erlebnisse die Wahrscheinlichkeit negativer Auswirkungen der Hemmung auf die Gesundheit verringert. Eines der Hauptparadigmen der Selbstöffnung war das sog. "expressive Schreiben". Hierbei wurden Teilnehmer von Untersuchungen gebeten über ihre tiefsten Gedanken und Gefühle bezogen auf das belastende Erlebnis zu schreiben, wobei zumeist 3-4 Schreibsitzungen von 15-20 Minuten angesetzt wurden. In einer Metaanalyse von Smith [58] wurde eine Effektstärke von d=0,47 für die verschiedenen gesundheitsbezogenen Variablen berichtet. Inzwischen ist eine große Anzahl von Untersuchungen zu diesem Thema erschienen. Die Studie hat zum Ziel zu überprüfen, ob die Ergebnisse der ersten Metaanalyse unter der Berücksichtigung neuerer Forschungsergebnisse bestätigt werden können.
Es wurden Literaturrecherchen in den wesentlichen nationalen und internationalen Datenbanken und Fachzeitschriften unternommen. Es wurden nur randomisierte Kontrollgruppenstudien berücksichtigt. Von 43 Studien, die die Einschlusskriterien erfüllten, konnten 30 in die Metaanalyse eingeschlossen werden.
Es wurden zwei Outcome-Bereiche getrennt analysiert: Variablen psychischer und somatischer Gesundheit. Unter Anwendung des Random Effect Modells konnten keine signifikanten Effektstärken bezüglich der beiden Gesundheitsbereiche gefunden werden. Verschiedene andere explorative Analysen (z.B. Limitierung der Studienstichprobe auf solche mit klinischen Probandensamples) erbrachten bis auf eine Ausnahme auch keine signifikanten Ergebnisse. Die Ergebnisse unserer Metaanalyse führen zur der Schlussfolgerung, dass Expressives Schreiben als Intervention zur Gesundheitsförderung bzw. zur Verhinderung negativer gesundheitlicher Wirkungen belastender Erfahrungen nicht geeignet scheint. Die Ergebnisse der vorgelegten Studie werden von anderen Metaanalytischen Untersuchungen gestützt [30], [18]. Die Propagierung des Verfahrens des Expressiven Schreibens in der Öffentlichkeit (vgl. "Writing to Heal" [45]) wird kritisch betrachtet.
Introduction
The expression of emotions by writing about one's deepest thoughts and feelings, especially regarding stressful or traumatic experiences, has long been a means of coping with emotional strain. Anne Frank, a German Jewish girl, persecuted by the Nazi regime and hiding for a long time from its prosecutors in a small room in the Netherlands, wrote into her diary:
"I hope, I can confide things to you which I never could do to another person and I hope you will be a great support to me." (Tagebuch der Anne Frank, 1993, S. 10, Fischer Verlag, translation by the authors.)
The common assumption that expressive writing about adverse experiences is salutary to " body and soul ", was transformed into a subject of systematic scientific research by Pennebaker et al. [44], [41].
In his theory of emotional inhibition [44], Pennebaker suggests that a person, when confronted with a negative, or even traumatic event, feels the need to share his/her experience with others, expecting social support. The consequence of confiding one's deepest thoughts and feelings to others, however, can - depending on the response of the counterpart - also be detrimental to one's self-esteem, making the person feel ashamed, ridiculed or rejected. Individuals thus often inhibit the expression of negative emotions, which leads to continuously heightened autonomic arousal. In the long run, sustained inhibition has a detrimental impact on well-being by increasing the probability of all kinds of health hazards [5], [40], [61], [1].
Disclosure by expressive writing does not imply the social risk of rejection or disapproval, but should help to alleviate the emotional burden and reduce the risk of developing psychosomatic problems [43].
In their cognitive theory of trauma processing, Ehlers et al. [8] describe, besides other mechanisms, the process of re-experiencing and verbalising the trauma as a path to elaboration and integration of the experience into one's conscious autobiographical memory. If inhibition is no longer maintained, unpleasant and upsetting intrusions cease. Thus writing about one's deepest feelings and thoughts regarding a negative event should improve health by abolishing inhibition.
In a paradigmatic experimental design Pennebaker et al. began to systematically examine the effects of expressive writing on the participants' psychological and physical health. In a series of experiments (e.g. [36], [37], [38], [11]) the research group was able to show that in order to obtain positive effects on the subjects' health, the writing instructions had to focus the subject on the emotional evaluation of his or her experience beyond the factual description of events. The typical experimental setup consisted of 3 to 4 short sessions of writing (15 to 20 minutes each) on an individually selected upsetting experience or a predetermined stressful situation (e.g. entry into college).
The effects of this brief and rather simple intervention puzzled the research community. The results showed long-term positive effects on health (e.g. documented in a lower number of health care visits, physical symptoms or even an improvement of immunological functioning or psychological well-being). Pennebaker's research inspired a number of subsequent studies by different authors using his paradigm of expressive writing. In 1998 Smyth [58] presented a meta-analysis of 13 studies, including 8 of the Pennebaker group, examining the long-term health effects of disclosure in healthy populations. He reported an overall effect size of d=0.47, indicating a significant, yet medium sized, effect of this brief and economic intervention, which suggested its usefulness as a tool for health promotion.
A large number of studies have been conducted since, expanding the application of the intervention from normal healthy subjects to individuals with specific health risks and clinical samples [12], as well as varying experimental parameters of the original design (number and duration of sessions, type of outcome data, instructions, time of follow-up assessment etc.) The large number of currently published studies makes it difficult to evaluate the state of evidence regarding the physical and psychological consequences of the expressive writing intervention.
The objective of our study was to determine the long-term effects of expressive writing particularly on physical and psychological health as studied in methodologically adequate studies (randomized controlled trials; RCTs). A meta-analysis was conducted to answer the following research questions:
Is expressive writing efficacious in improving health and what is the size of the effects?
Does efficacy differ regarding physical and psychological health parameters as outcome variables?
Methods
Literature search
Relevant studies were located by searching the following data bases: PsychInfo, Psyndex, PubMed, Medline and the Cochrane Library. The keywords used for the search were selected on the basis of the previous meta-analyses by Smyth [58] and Frisina et al. [12] using the following terms: Pennebaker, self-disclosure, disclosure and writing, self-disclosure and health, writing and stressful life events, critical life events and writing, written emotional expression, emotive writing, emotional expression and writing, and the German keywords "Selbstöffnung” and “Trauma and Schreiben". The computer search was supplemented by a manual search in relevant journals, having frequently published papers on disclosure, and by examining various reviews [22], [55], [12], [58].
Furthermore e-mail contact was established with different authors in the field in order to identify undiscovered or non-published studies (e.g. J.W. Pennebaker, J.M. Smyth, R. Rosenthal, D.M. Sloan, B.P. Marks). This strategy resulted in 10 more papers. In total, the search resulted in 216 identified studies, which were then examined for relevance.
Inclusion criteria
Only randomized controlled trials were included in meta-analysis, which ensures a high degree of internal validity of the results. The conceptual and interventional similarity to the disclosure paradigm, developed by Pennebaker et al., was ensured by the following criteria:
The experimental group is instructed to write on an experienced stressful or traumatic life event.
The control group is instructed to write on a neutral factual event/topic. No instructions or interventions which foster verbal or motor expression of emotions or emotional thoughts in the control group were performed.
If the experimental group received some further intervention in addition to expressive writing (e.g. psychotherapy), this also had to be carried out in the control group.
Only long-term effects of disclosure were analyzed, defined by an interval of at least 4 weeks between the last writing session and the follow-up assessment.
In the post-follow-up period, no contacts with the experimenter were allowed.
Each specific data set was considered only once (in spite of multiple publications).
The study had to comprise at least 10 subjects per group.
The study had to be reported in English or German language.
The application of these criteria reduced the number of studies to be included in the meta-analysis to 42. In order to be able to calculate effect sizes, studies had to report means and standard deviations, F-Scores, t-scores or significance levels including the number of subjects.
Coding of variables
A coding manual (i=53) was compiled according to Lipsey`s [29] suggestions including variables related to external characteristics of the study (e.g. year of publication), so called substantial characteristics (like data relevant to the topic of research) and biasing characteristics (e.g. randomization). To ensure interrater reliability two authors (1 and 2) independently coded 4 randomly selected studies for training purposes and then discussed the cases of non-correspondence. After that, 8 studies were randomly selected to determine interrater reliability, Cohen's Kappa for multinomial data and intraclass coefficients for rank and interval data [51]. The mean inter-rater reliability was "excellent" (Kappa=0.85, see [34]). Very few items had a Kappa lower than 0.40 (i=4). All items with low inter-rater reliability were not substantial to the conduction of the meta-analysis and interpretation of the results.
Effect size calculation
All outcome variables related to health were categorized into 3 classes:
Somatic health including physiological parameters (e.g. killer cell count) and somatic symptoms (e.g. headache, dizziness).
Psychological health (e.g. depressiveness, anxiety, PTSD symptoms, negative affect and mood).
Miscellaneous (e.g. grades, self efficacy).
The 3rd category was analysed for comparative reasons in a separate analysis and is not included in the test of general health effects.
Hedges' <g> was used as measure of effect size [19], which differs from the conventional <d> by dividing the difference of means, by the pooled standard deviation. To offset bias produced by small sample sizes, a correction formula was applied as suggested by Hedges & Olkin [19]. Data used for effect size calculation was entered into the computer program "Study Input" [52].
If categorical data was presented, odds ratios were calculated, which were then transformed into g by a strategy suggested by Fleiss [10]. If only probability levels were reported, effect size was set to zero in case of non-significance. Only one effect size for each category of variables per study (mean) was entered into the meta-analysis. If a study contained more than one disclosure group or more than one control group, effect sizes were averaged. All measures were scored in such a way that if the experimental group was superior to the control group, a positive effect size resulted.
Model of analysis
Effect sizes of single studies are commonly integrated into one score, which represents an estimate of the "true" effect. In the fixed effects model (FEM) it is assumed that all original study effect sizes estimate a common population effect, best defined by the mean effect size of all studies. Deviations in single studies are attributed to a sampling error. To examine this assumption a test on homogeneity has to be performed [54]. The implication of this model is a limited generalization of the results to other studies. Therefore the random effects model (REM [6]) was used in the main analyses.
The REM accounts for a certain component of variance (random effects variance), which is not part of the sampling error, but is created by systematic factors of the study design (e.g. different assessment procedures, different intervention formats), and is tested regarding its significance [51]. If the variance deviates significantly from zero (≥0.05), a test for moderators of effect size is suggested [48]. The desirable implication of REM is that the results of meta-analysis can be generalized to the universe of studies on the topic (with some limitations: e.g. only RCT studies). To ensure this generalisability of results it is suggested to include at least 15 studies into meta-analysis [9]. If markedly fewer studies are included, random effect tests should be regarded as only approximate [20].
Sensitivity analyses [16] are carried out to test whether different decisions regarding the procedure of meta-analysis (integration of effects) lead to different results.
Furthermore, results of a meta-analysis can be distorted by a publication bias, assuming that the under-representation of non-published studies leads to an overestimation of effect size. Orwin's "fail safe n" statistic [33] assesses the stability of meta-analytic results by estimating the number of null results necessary to lower an effect size to a specific level of significance.
Results
Of the 42 relevant studies 30 presented data which could be used for the meta-analysis (Table 1 (Tab. 1)). Seven of the 42 studies had to be excluded because they did not report adequate information for effect size calculation and the respective authors did not react to our contact efforts. Another 5 studies had to be excluded because they failed to meet the inclusion criteria, which became apparent only after closer inspection of the published papers.
Table 1. Studies included in the meta-analysis.
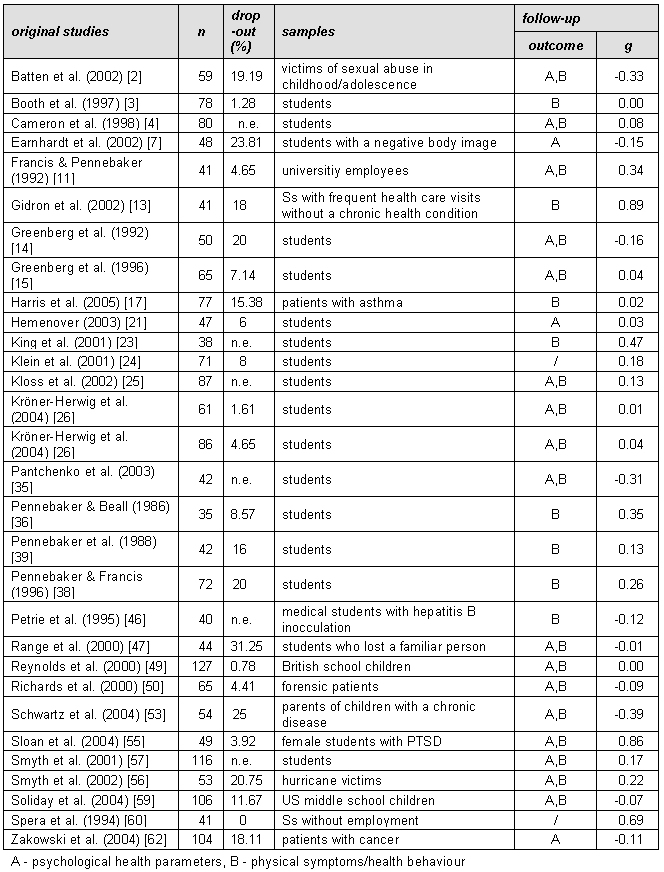
Of all 30 studies 27 used pure randomization for the allocation of Ss to conditions and 3 used a matching procedure prior to randomization. 20 studies were published after 2000, only 3 before 1990. The mean age of Ss was 27 years, most of them were female (64.7%). In 17 studies students were involved, 8 studies included "high risk" samples (Ss who had experienced an adverse event that made them vulnerable, e.g. victims of a hurricane, early sexual abuse). Four studies included clinical samples (e.g. Ss with asthma, PTSD) (Table 1 (Tab. 1)). The number of sessions for expressive writing varied between 1 and 5 (mean 3.2 with a duration between 15 and 20 minutes). The follow-up period for the assessment of long-term health effects varied between 4 weeks and 8 months. The average number of Ss was 64 and the mean drop-out rate 12.1%.
For the examination of baseline differences between experimental and control groups effect sizes were computed and integrated for each study. The FE model was used in this case because of a smaller confidence interval. Two studies had to be excluded from this analysis, since they did not present adequate data on baseline variables.
None of the studies had a positive/negative effect size with a confidence interval of 95% not comprising zero. Thus a non-significant effect of g=-0.07 (σ2=0.00), CI95=-0.16-0.03) results. A test on the subset of psychological health variables from 14 studies leads to a similar result (g=-0.12, σ2=0.00, CI95=-0.25-0.00). The analysis of somatic health variables also renders non-significant results regarding baseline differences (K=20; g=0.05, σ2=0.0, CI95=-0.16-0.06).
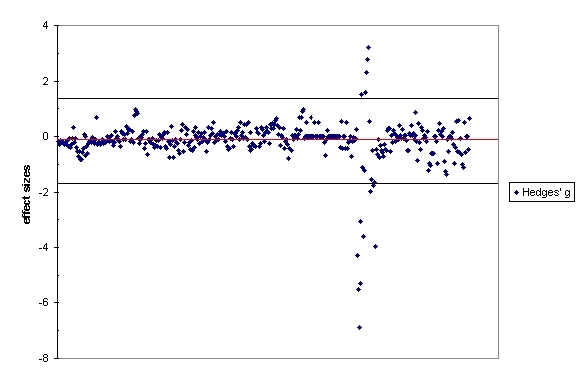
Before meta-analyses regarding efficacy of the expressive writing interventions (difference between experimental and control group) were conducted, an outlier analysis was performed. The study of Greenberg et al. [15] showed a large number of effect sizes that lay more than 2 standard deviations above/below the mean of all effect sizes (Figure 1 (Fig. 1)) and was hence eliminated from further analysis.
Figure 1. Effect sizes of all studies (K=30) .
We used the RE model to calculate the effect sizes for the expressive writing intervention with respect to all health related variables. This yielded a non-significant effect size (K=27, g=0.04, σ2=0.003, σθ2=0.01, CI95= -0.08-0.15). The RE variance did not reach significance.
The subset of psychological variables (K=19) was analysed separately, resulting in an effect size of g=0.01 (σ 2=0.01, σθ2=0.01, CI95=-0.17-0.19), which did not reach significance.
The analysis of somatic health variables (K=24) rendered an effect size of g=0.07 (σ2=0.00, σθ2=0.01, CI95=-0.06-0.19), which is not significant. The critical difference of chi2 3.84 at a≤0.05 between the categories of health related variables was not reached. Thus, no significant differences between outcome categories regarding efficacy can be detected.
Furthermore a series of exploratory analyses were performed. The analysis of effects of health behaviour variables (K=16, e.g. visits to physicians or health care centres, sick days, drug use, smoking, alcohol consumption, sleeping and eating habits, sports) yielded a significant effect size of g=0.2 (σ2=0.02, σθ2=0.1, CI95=0.04-0.36).
Also all self-reported somatic health symptoms and all objective physical variables (e.g. immune parameters, breathing parameters) were analysed separately. Both analyses rendered non-significant results (K=14, g=-0.05, σ2=0.00, CL95=-0.18-0.09; K=4, g=0.01, σ2= 0.02, CL95=-0.27-0.29)
Because of its special relevance regarding the concept of expressive writing, an exploratory analysis (K=6) with respect to posttraumatic symptoms was conducted in order to test for a specific effect on the symptoms of arousal, intrusion and avoidance. The effect size turned out to be insignificant g=-0.10 (σ2=0.02, σθ2=0.04, CI95=-0.25-0.46).
A last exploratory analysis was conducted separating studies with "high risk" and "normal" samples. An insignificant g analysed over all health variables was found in both analyses (students: K=16, g=0.07, σ2=0.00, CI95=-0.03-0.22/high risk: K=7, g=-0.03, σ2=0.01, CI95=-0.06-0.20). The 4 studies on clinical samples were also analysed, resulting in a g=0.08 (σ2=0.01, CI95=-0.15-0.31).
The group of studies presenting variables not directly related to health (see "miscellaneous", K=8) was also examined and revealed a g=0 (σ2=0.01, σθ2=0.01, Cl95=-0.19-0.26).
Sensitivity analyses were carried out by separately analysing studies, where effect size computations were based on means, sd, n, or on significance reports only. No difference of any importance was found. An analysis including the study of Greenberg et al. [15] led to the same negative results regarding effect sizes as well. The significant g of 0.2 (health behaviour) equals the lowest relevant effect size to be tested against [33], thus the fail safe n statistic could not be calculated.
Discussion
Our meta-analysis including 30 studies using a randomized controlled design presents effect sizes regarding the long-term efficacy of expressive writing with respect to somatic and psychological health. The long-term effects regarding the different outcome categories do not differ from one-another. When averaging over all outcome categories, again no significant effect size is found. These negative results cannot be explained by differences between experimental and control groups at baseline, since no differences could be detected. Thus, our analysis does not support the hypothesized beneficial effect of disclosure by writing about stressful or traumatic experiences as it was originally suggested by Pennebaker.
None of the additional exploratory or sensitivity analyses led to a detection of significant effects, with the exception of the category of health behaviours. The observed effect size is very small, with the confidence interval at the lower end exceeding zero just marginally. PTSD symptoms, which should be very sensitive to the impact of disclosure, were not decreased after the intervention. Furthermore, it was of no importance whether "high risk", clinical or normal samples were involved.
In the light of the relatively high number of original studies that were incorporated in all main analyses (>13), these results are deemed to be very robust. As the RE model was applied in all main analyses, generalisability of results is warranted.
Thus our study leads us to a conclusion which is contrary to the one derived from the analysis performed by Smyth [58], who obtained an average effect size of a medium level, varying dependent on the analysed outcome category between d=0.03 (health behaviours) and d=0.66 (psychological well-being). When considering possible explanations for the differences between these analyses, it is evident that our analysis is based on markedly more original studies than the previous one (included studies 13 vs. 30), with 8 of our studies also being part of Smyth's analysis. In contrast to the earlier study, our analysis could fulfil, at least regarding the general health effects, the criterion of 15 analysed studies and can, therefore, claim generalisability of results. Also, our rather conservative methodology may have contributed to the different outcome (use of g, correction formula for small n).
In a recent study Frisina et al. [12] examined 9 studies on the health outcomes in "clinical populations". Similar to our study, the authors included only RCTs. The mean effect size the authors obtained was different from zero (d=0.19, p<0.05), but markedly smaller than that found by Smyth. The results show that the disclosure intervention was significantly more effective regarding physical health than psychological health (d=0.07 vs. d=0.21), or rather that a beneficial effect of expressive writing could only be detected regarding physical health variables. However, direct comparability of Frisina's et al. analysis and ours is limited. Because of different selection criteria, only one of their 9 original studies was included in our analysis. Their finding of a general efficacy, however, even below the suggested standard for "small" efficacy (d=0.2) could not be replicated in the present meta-analysis, which included mainly non-clinical studies.
The assumption that clinical samples might profit more than non-clinical samples by emotional writing is not corroborated by our explorative analysis. However, the number of clinical trials included in our study is small.
The results of our analyses give no reason to believe that emotional writing about stressful experiences in a structured setting - as used in the disclosure paradigm - is an effective tool for the reduction of health risks supposed to be the sequelae of emotional inhibition.
However, it cannot be excluded that under particular context conditions and in particular groups of Ss positive outcome reflected in selected parameters of health may be observed (see e.g. [55], [13], [26]). However these conditions cannot be specified at the moment and only speculations can be offered. It has already been proposed that only individuals stressed by adverse bio-psychosocial conditions may profit from expressive writing. Additional instructions accompanying the standard emotional writing procedure could be crucial, e.g. instructions that foster self-regulatory coping, self-efficacy or helping others (see e.g. [28], [27], [4], [13], [31]).
Since in most studies pre-experimental extent of "disclosure" in the individual is not controlled, this might be a relevant condition. The type of the trauma concerned could be a relevant factor as well as the fact of whether it is still prevailing or a past experience (see [58]).
According to the theory of memory elaboration it should be examined whether the cognitive-emotional quality of the written essays is predictive of health improvement. There have mostly been only very basic attempts to determine the content of the essays (e.g. [38], [32]), but a more sophisticated method of determining the extent of "self-exploration", based on Carl Roger's theory did not yield any promising perspective [26].
In this meta-analysis a search for moderators of effect sizes was not performed since minimal or no significant effect sizes were found and the detected variance did not reach a size suggesting this procedure.
The validity of our findings is supported by a meta-analysis by Meads et al. [30], which came to our knowledge after our study had been planned and conducted. The authors incorporated even more original studies than the current analysis, since they did not restrict their analysis to emotional writing but also included other forms of disclosure. Similar to our study they excluded non-randomized studies, but differed regarding the definition of long-term outcome. They included follow-up data assessed at a minimum interval of one week whereas we used a one month criterion. Also, they included studies into their analysis with samples of n<10. In spite of these differences, the authors come to the same conclusion: "There is no clear evidence to demonstrate the efficacy of the intervention reviewed." (see executive summary, [30]).
One further meta-analysis by Harris [18], which has been published just recently, examined whether expressive writing affects health care utilization behaviours. Based on 13 studies Harris finds a small but significant effect only in healthy samples (g=0.16) but not in samples defined by medical diagnoses or exposure to stress or other psychological factors.
Thus all recent meta-analyses lead to the same general conclusion: Expressive Writing or other forms of disclosure do not lead to long term momentous positive health effects. The results of our review do not allow one to recommend the procedure of expressive writing to individuals having experienced stressful or traumatic experiences to avert negative consequences on their health. The findings, documented in these reviews, either call into question the intervention formats inducing disclosure used so far, or suggest a revision of the theory of emotional inhibition and disclosure. Books titled “Opening Up: The Power of Healing.” [42] or “Writing to Heal: A Guided Journal for Recovering from Trauma and Emotional Upheaval” [45] are qualified to misdirect the public since they induce expectations and hopes not likely to be met.
Notes
Conflicts of interest: none declared
References
- 1.Appel MA, Holroyd KA, Gorkin L. Anger and the etiology and progression of physical illness. In: Temoshok L, van Dyke C, Zegans LS, editors. Emotions in health and illness. New York: Grune & Straton; 1983. pp. 73–88. [Google Scholar]
- 2.Batten SV, Follette VM, Rasmussen-Hall ML, Palm KM. Physical and psychological effects of written disclosure among sexual abuse survivors. Behav Ther. 2002;33:107–122. [Google Scholar]
- 3.Booth RJ, Petrie KJ. Changes in circulating lymphocyte numbers following emotional disclosure: evidence of buffering? Stress Med. 1997;13:23–29. [Google Scholar]
- 4.Cameron LD, Nicholls G. Expression of stressful experiences through writing: effects of a self-regulation manipulation for pessimists and optimists. Health Psychol. 1998;17:84–92. doi: 10.1037//0278-6133.17.1.84. [DOI] [PubMed] [Google Scholar]
- 5.Cooper CL, Faragher EB. Psychosocial stress and breast cancer. The inter-relationship between stress events, coping stategies and personality. 3. Psychol Med. 1993;23(3):653–662. doi: 10.1017/s0033291700025435. [DOI] [PubMed] [Google Scholar]
- 6.Cooper H, Hedges LV. Potentials and limitations of research synthesis. In: Cooper H, Hedges LV, editors. The Handbook of Research Synthesis. New York: Russell Sage Foundation; 1994. pp. 521–529. [Google Scholar]
- 7.Earnhardt JL, Martz DM, Ballard ME, Curting L. A writing intervention for negative body image: Pennebaker fails to surpass the placebo. Journal of College Student Psychotherapy. 2002;17:19–35. [Google Scholar]
- 8.Ehlers A, Hackmann A, Michael T. Intrusive re-experiencing in post-traumatic stress disorder: phenomenology, theory, and therapy. Memory. 2004;12:403–415. doi: 10.1080/09658210444000025. [DOI] [PubMed] [Google Scholar]
- 9.Field AP. Meta-analysis of correlation coefficients: a Monte Carlo comparison of fixed and random-effects methods. Psychol Methods. 2001;6:161–180. doi: 10.1037/1082-989x.6.2.161. [DOI] [PubMed] [Google Scholar]
- 10.Fleiss JL. Measures of effect size for categorical data. In: Cooper H, Hedges LV, editors. The Handbook of Research Synthesis. New York: Russell Sage Foundation; 1994. pp. 245–260. [Google Scholar]
- 11.Francis ME, Pennebaker JW. Putting stress into words: The impact of writing on physiological, absentee, and self-reported emotional well-being measures. Am J Health Promot. 1992;6:280–287. doi: 10.4278/0890-1171-6.4.280. [DOI] [PubMed] [Google Scholar]
- 12.Frisina PG, Borod JC, Lepore SJ. A meta-analysis of the effects of written emotional disclosure on the health outcomes of clinical populations. J Nerv Ment Dis. 2004;192:629–634. doi: 10.1097/01.nmd.0000138317.30764.63. [DOI] [PubMed] [Google Scholar]
- 13.Gidron Y, Duncan E, Lazar A, Biderman A, Tandeter H, Shvartzman P. Effects of guided written disclosure of stressful experiences on clinic visits and symptoms in frequent clinic attenders. Fam Pract. 2002;19:161–166. doi: 10.1093/fampra/19.2.161. [DOI] [PubMed] [Google Scholar]
- 14.Greenberg MA, Stone AA. Emotional disclosure about traumas and its relation to health: Effects of previous disclosure and trauma severity. J Pers Soc Psychol. 1992;63:75–84. doi: 10.1037//0022-3514.63.1.75. [DOI] [PubMed] [Google Scholar]
- 15.Greenberg MA, Wortman CB, Stone AA. Emotional expression and physical health: revising traumatic memories or forstering self-regulation. J Pers Soc Psychol. 1996;71:588–602. doi: 10.1037//0022-3514.71.3.588. [DOI] [PubMed] [Google Scholar]
- 16.Greenhouse JB, Iyengar S. Sensitivity analysis and diagnostics. In: Cooper H, Hedges LV, editors. The Handbook of Research Synthesis. New York: Russell Sage Foundation; 1994. pp. 383–398. [Google Scholar]
- 17.Harris AHS, Thoresen CE, Humphreys K, Faul J. Does writing affect asthma? A randomized trial. Psychosom Med. 2005;67:130–136. doi: 10.1097/01.psy.0000146345.73510.d5. [DOI] [PubMed] [Google Scholar]
- 18.Harris AHS. Does expressive writing reduce health care utilization? A meta-analysis of randomized trials. J Consult Clin Psychol. 2006;74:243–252. doi: 10.1037/0022-006X.74.2.243. [DOI] [PubMed] [Google Scholar]
- 19.Hedges LV, Olkin I. Statistical methods for meta-analysis. New York: Academic Press; 1985. [Google Scholar]
- 20.Hedges LV, Vevea JL. Fixed- and random-effects models in meta-analysis. Psychol Method. 1998;3:486–504. [Google Scholar]
- 21.Hemenover SH. The good, the bad, and the healthy: Impacts of emotional disclosure of trauma on resilient self-concept and psychological distress. Pers Soc Psychol Bull. 2003;29:1236–1244. doi: 10.1177/0146167203255228. [DOI] [PubMed] [Google Scholar]
- 22.Horn AB, Mehl MR. Expressives Schreiben als Coping-Technik: Ein Überblick über den Stand der Forschung. Verhaltenstherapie. 2004;14:274–283. [Google Scholar]
- 23.King LA. The health benefits of writing about life goals. Pers Soc Psychol Bull. 2001;27:798–807. [Google Scholar]
- 24.Klein K, Boals A. Expressive writing can increase working memory capacity. J Exp Psychol. 2001;130:520–533. doi: 10.1037//0096-3445.130.3.520. [DOI] [PubMed] [Google Scholar]
- 25.Kloss JD, Lisman SA. An exposure-based examination of the effects of written emotional disclosure. Br J Health Psychol. 2002;7:31–47. doi: 10.1348/135910702169349. [DOI] [PubMed] [Google Scholar]
- 26.Kröner-Herwig B, Linkemann A, Morris L. Selbstöffnung beim Schreiben über belastende Lebensereignisse. Z Klin Psychol Psychother. 2004;33:183–195. [Google Scholar]
- 27.L'Abate L, Baggett MS, editors. Manual. Distance writing and computer assisted training in mental health. Atlanta, G.A.: Institute for Life and Empowerment; 1997. [Google Scholar]
- 28.L'Abate L, editor. Programmed writing: a self-administered approach for interventions with individuals, couples and families. Pacific Grove, CA: Brooks/Cole; 1992. [Google Scholar]
- 29.Lipsey MW. Identifying potentially interesting variables and analysis opportunities. In: Cooper H, Hedges LV, editors. The Handbook of Research Synthesis. New York: Russell Sage Foundation; 1994. pp. 111–123. [Google Scholar]
- 30.Meads C, Lyons A, Carroll D. The impact of the emotional disclosure intervention on physical and psychological health - a Systematic Review. 2003. (West Midlands Health Technology Assessment Collaboration Report; 43). [Google Scholar]
- 31.Morris L, Linkemann A, Kröner-Herwig B. Writing your way to health? The effects of disclosure in German students. In: Abelian ME, editor. Focus on Psychotherapy Research. New York: Nova Science; 2005. pp. 219–239. [Google Scholar]
- 32.Murray EJ, Segal DL. Emotional processing in vocal and written expression of feelings about traumatic experiences. J Trauma Stress. 1994;7:391–405. doi: 10.1007/BF02102784. [DOI] [PubMed] [Google Scholar]
- 33.Orwin RG. A fail-safe N for effect size in meta-analysis. Journal of Educational Statistics. 1983;8:157–159. [Google Scholar]
- 34.Orwin RG. Evaluating coding decisions. In: Cooper H, Hedges LV, editors. The Handbook of Research Synthesis. New York: Russell Sage Foundation; 1994. pp. 139–162. [Google Scholar]
- 35.Pantchenko T, Lawson M, Joyce MR. Verbal and non-verbal disclosure of recalled negative experiences: relation to well-being. Psychol Psychother. 2003;76(Pt3):251–265. doi: 10.1348/147608303322362488. [DOI] [PubMed] [Google Scholar]
- 36.Pennebaker JW, Beall SK. Confronting a traumatic event: toward an understanding of inhibition and disease. J Abnorm Psychol. 1986;95:274–281. doi: 10.1037//0021-843x.95.3.274. [DOI] [PubMed] [Google Scholar]
- 37.Pennebaker JW, Colder M, Sharp LK. Accelerating the coping process. J Pers Soc Psychol. 1990;58:528–537. doi: 10.1037//0022-3514.58.3.528. [DOI] [PubMed] [Google Scholar]
- 38.Pennebaker JW, Francis ME. Cognitive, emotional, and language processes in disclosure. Cogn Emot. 1996;10:601–626. [Google Scholar]
- 39.Pennebaker JW, Kiecolt-Glaser R, Glaser R. Disclosure of traumas and immune function:Health implications for psychotherapy. J Consult Clin Psychol. 1988;56:239–245. doi: 10.1037//0022-006x.56.2.239. [DOI] [PubMed] [Google Scholar]
- 40.Pennebaker JW, O'Heeron R. Confiding in others and illness rates among spouses of suicide and accidental death victims. J Abnorm Psychol. 1984;93:473–476. doi: 10.1037//0021-843x.93.4.473. [DOI] [PubMed] [Google Scholar]
- 41.Pennebaker JW. Confession, inhibition, and disease. In: Berkowitz L, editor. Advances in Experimental Social Psychology. Vol. 22. Academic Press; 1989. pp. 211–224. [Google Scholar]
- 42.Pennebaker JW. Opening up: the healing power of expressing emotions. New York: Guilford Publications; 1997. [Google Scholar]
- 43.Pennebaker JW. Putting stress into words: health, linguistic and therapeutic implications. Behav Res Ther. 1993;31:539–548. doi: 10.1016/0005-7967(93)90105-4. [DOI] [PubMed] [Google Scholar]
- 44.Pennebaker JW. Traumatic experience and psychosomatic disease: Exploring the roles of behavioural inhibition, obsession, and confiding. Can Psychol. 1985;26:82–95. [Google Scholar]
- 45.Pennebaker JW. Writing to heal: a guided journal for recovering from trauma and emotional upheavel. Oakland: New Harbinger Publications; 2004. [Google Scholar]
- 46.Petrie KJ, Booth RJ, Pennebaker JW, Davison KP, Thomas MG. Disclosure of trauma and immune response to a hepatitis B vaccination program. J Consult Clin Psychol. 1995;63:787–792. doi: 10.1037//0022-006x.63.5.787. [DOI] [PubMed] [Google Scholar]
- 47.Range LM, Kovac SH, Marion MS. Does writing about the bereavement lessen grief following sudden, unintentional death? Death Stud. 2000;24:115–135. doi: 10.1080/074811800200603. [DOI] [PubMed] [Google Scholar]
- 48.Raudenbush SW. Random effects models. In: Cooper H, Hedges LV, editors. The Handbook of Research Synthesis. New York: Russell Sage Foundation; 1994. pp. 301–321. [Google Scholar]
- 49.Reynolds M, Brewin CR, Saxton M. Emotional disclosure in school children. J Child Psychol Psychiatry. 2000;41:151–159. [PubMed] [Google Scholar]
- 50.Richards JM, Beall WE, Seagal JD, Pennebaker JW. Effects of disclosure of traumatic events on illness behavior among psychiatric prison inmates. J Abnorm Psychol. 2000;109:37–53. doi: 10.1037//0021-843x.109.1.156. [DOI] [PubMed] [Google Scholar]
- 51.Rustenbach SJ. Metaanalyse: Eine anwendungsorientierte Einführung. Bern: Verlag Hans Huber; 2003. [Google Scholar]
- 52.Schäfer K, Mitte K. The statistical program "Study Input 2.08". University of Jena, Germany; 2003. [Google Scholar]
- 53.Schwartz L, Drotar D. Effects of written emotional disclosure on caregivers of children and adolescents with chronic illness. J Pediatr Psychol. 2004;29:105–118. doi: 10.1093/jpepsy/jsh014. [DOI] [PubMed] [Google Scholar]
- 54.Shadish WR, Haddock CK. Combining estimates of effect Size. In: Cooper H, Hedges LV, editors. The Handbook of Research Synthesis. New York: Russell Sage Foundation; 1994. pp. 261–281. [Google Scholar]
- 55.Sloan DM, Marx BP. A closer examination of the structured written disclosure procedure. J Consult Clin Psychol. 2004;72:165–175. doi: 10.1037/0022-006X.72.2.165. [DOI] [PubMed] [Google Scholar]
- 56.Smyth JM, Hockemeyer J, Anderson C, Strandberg K, Koch M, O'Neill HK, McCammon S. Structured writing about a natural disaster buffers the effect of intrusive thoughts on negative affect and physical symptoms. The Australian Journal of Disaster and Trauma Studies. 2002;6 [Google Scholar]
- 57.Smyth JM, True N, Souto J. Effects of writing about traumatic experiences: The necessity for narrative structuring. J Soc Clin Psychol. 2001;20:161–172. [Google Scholar]
- 58.Smyth JM. Written emotional expression: Effect sizes, outcome types, and moderating variables. J Consult Clin Psychol. 1998;66:174–184. doi: 10.1037//0022-006x.66.1.174. [DOI] [PubMed] [Google Scholar]
- 59.Soliday E, Garofalo JP, Rogers D. Expressive writing intervention for adolescents somatic symptoms and mood. J Clin Child Adolesc Psychol. 2004;20:161–172. doi: 10.1207/s15374424jccp3304_14. [DOI] [PubMed] [Google Scholar]
- 60.Spera SP, Buhrfeind ED, Pennebaker JW. Expressive writing and coping with job loss. Acad Manage J. 1994;37:722–733. [Google Scholar]
- 61.Temoshok L. Biopsychosocial studies on cutaneous malignant melanoma: Psychosocial factors associated with prognostic indicators, progression, psychophysiology and tumor-host response. Soc Sci Med. 1985;20:833–840. doi: 10.1016/0277-9536(85)90338-7. [DOI] [PubMed] [Google Scholar]
- 62.Zakowski SG, Ramati A, Morton C. Written emotional disclosure buffers the effects of social constraints on distress among cancer patients. Health Psychol. 2004;23:555–556. doi: 10.1037/0278-6133.23.6.555. [DOI] [PubMed] [Google Scholar]