

Abstract
Background
Colorectal cancer (CRC) family history is a known risk factor for CRC development; however, effects of CRC family history on survival after CRC diagnosis are less well defined. Our population-based analysis investigates whether familial CRC cases exhibit improved survival compared to sporadic CRC cases.
Methods
Cases enrolled in the University of California Irvine Gene-Environment Study of Familial Colorectal Cancer from 1994–1996 were analyzed, with follow-up through December 2006. Cases were categorized as familial or sporadic based on self-reported CRC family history in a first-degree relative. Univariate and multivariate survival analyses with Cox proportional hazards ratios were performed for overall survival (OS) and CRC-specific survival (CRC-SS).
Results
1154 CRC cases were analyzed, including 781 colon cancer and 373 rectal cancer cases. 19% of colon cases had family history of CRC in a first degree relative, compared with 16% of rectal cancer cases. No statistically significant differences between familial and sporadic colon or rectal cancer cases were detected for age, gender, ethnicity, stage, tumor location, histology, tumor grade, or stage-specific treatment rendered. Among colon cancer cases, family history of CRC (vs. no family history as a referent group) was associated with improved OS (adjusted HR = 0.760; 95% CI 0.580–0.997), but not with CRC-SS (HR = 0.880, 95% CI 0.621–1.246). No OS or CRC-SS differences were detected for rectal cancer cases.
Conclusions
CRC cases with family history of the disease have improved overall survival compared with sporadic CRC cases, a finding that is independent of other relevant clinical factors.
INTRODUCTION
Colorectal cancer (CRC) is the third most common cancer in the United States, accounting for 10% of all cancer diagnoses, and is the second leading cause of cancer-related death, accounting for 8% of all cancer deaths among men and 9% of all cancer deaths among women (1). A positive family history of CRC (defined as the presence of CRC in one or more first- and/or second-degree relatives) is a well-recognized risk factor for CRC. Individuals are at varying degrees of increased risk depending on age of the affected family member, number of affected relatives, and closeness of the relative. Similarly, individuals with a family history of CRC are at a higher risk to develop colorectal polyps. This is most likely due to the contribution of several genes, in addition to environmental factors. It is estimated that 10–30% of CRC cases demonstrate familial clustering (2, 3).
The clearest examples of familial risk for CRC are the autosomal dominantly inherited genetic cancer predisposition syndromes familial adenomatous polyposis (FAP) and hereditary nonpolyposis colorectal cancer (HNPCC). FAP, characterized by the presence of more than 100 colorectal polyps, is associated with a >90% lifetime risk to develop CRC (4), while individuals with HNPCC have about an 82% cumulative risk to develop CRC (5). However, well-characterized, highly penetrant genetic syndromes account for approximately 1% of CRC cases (6).
Despite convincing evidence that family history of CRC is a risk factor for colorectal polyps and cancer (7–10), conflicting reports have emerged on the association of family history with survival after CRC diagnosis. Family history of CRC has been reported to have no association with survival after CRC diagnosis in the Melbourne CRC cohort study (11) and in a study of CRC cases in the Utah Population Database (12). In a recent analysis of women enrolled in the Nurses Health Study, increased overall and cancer-specific mortality were noted for CRC cases having a family history of CRC (13). However, in a Japanese population-based study, CRC family history was associated with improved 5-year survival rates among colon cancer cases (14). Recently, an analysis of stage III colon cancer patients enrolled in an adjuvant chemotherapy clinical trial revealed that family history of CRC was associated with improved disease-free survival and recurrence-free survival, but not overall survival (15).
In the context of these varying reports, the role of CRC family history on survival among colon and rectal cancer cases is still unclear. Therefore we designed the present study to determine if family history of CRC predicts improved survival among colon and rectal cancer cases using data from the University of California Irvine Gene-Environment Study of Familial Colorectal Cancer.
METHODS
Case Ascertainment and Description of the Parent Study Population
Incident cases of invasive CRC from the University of California Irvine Gene-Environment Study of Familial Colorectal Cancer were analyzed (6). Participants were identified through the population-based cancer registries of the Cancer Surveillance Program of Orange County (CSPOC)/San Diego Imperial Organization for Cancer Control (SANDIOCC), using the February 2007 data file. In the parent study (6), all subjects with CRC diagnosed at all ages in Orange County, CA from 1994 to 1996 were ascertained. All subjects diagnosed in San Diego and Imperial Counties, CA at less than 65 years of age between 1994 and 1995 were also ascertained. Cases were then contacted if they were eligible for the study (alive at the time ascertained and having a contact address) and if their physicians did not deny permission to contact. At the time of study entry, subjects signed a consent form allowing for blood draws and the release of medical information, including access to pathology reports and tissue blocks. This study was approved by the UC Irvine Institutional Review Board (#93–257).
Demographic and Clinical Data
Clinical and demographic data were obtained from the aforementioned cancer registry databases, as previously reported (16, 17). Recorded data include demographic information (e.g. age, gender, ethnicity), site within the colon/rectum, stage at presentation, tumor histology and grade. Stage at diagnosis was derived in adherence to TNM criteria using the available SEER Extent of Disease descriptor in CCR, as previously described (18). Tumor histology and site were coded according to criteria specified by the World Health Organization in International Classification of Diseases for Oncology (ICD-O) (19). Histology codes included: adenocarcinoma (8140, 8144, 8210, 8260–8263, 8380, 8490), mucinous adenocarcinoma (8470, 8480, 8481), carcinoma (8010, 8020, 8070, 8071, 8124, 8240), and not otherwise specified (8000, 8041, 8042, 8120, 8130, 8243, 8246, 8560, 8570, 8722). Only invasive cases of cancer were included in the analysis. Primary site code was searched using the Surveillance, Epidemiology and End Results (SEER) site code for colon (21041, 21043–21048) and rectum (21051–21052). Appendiceal cancers were excluded. Therapeutic information related to the first course of treatment was abstracted from medical and laboratory records by trained tumor registrars according to Cancer Reporting in California: Vol. 1, Abstracting and Coding Procedures for Hospitals (20). This included surgical treatment rendered at the primary site (i.e., any surgical resection, including total/subtotal/partial colectomy, unknown type of colectomy, and local excision), treatment with radiation therapy, and the use of chemotherapy.
Standard therapy is defined according to the National Comprehensive Cancer Network (NCCN) practice guidelines as follows: resection alone for stage I disease in both colon and rectal cancer; surgical resection alone or with adjuvant chemotherapy for stage II colon cancers; surgical resection followed by adjuvant chemotherapy for stage III colon cancers. Stage II and III rectal cancers typically require treatment with neoadjuvant (i.e., up-front) chemoradiation followed by surgery and additional chemotherapy, while stage IV colon and rectal cancers are treated with systemic chemotherapy (21).
Family History Assessment
Family history of cancer was ascertained by self-reporting during a telephone interview at time of study enrollment. Cases with family history of CRC in a first-degree relative (hereafter referred to as “familial CRC cases”) were recognized as those having at least one first-degree relative (parent, sibling, or offspring) with CRC. Family history in second-degree relatives was not assessed in the present analysis. Accuracy of self-reporting was reported to be 90% in a prior validation study involving these CRC cases (22). Twenty-two cases with HNPCC, as defined by Amsterdam criteria, in addition to one case with clinically diagnosed FAP, were excluded from analysis. The remaining sporadic and familial CRC cases (n = 1174) were included for analysis.
Follow-up
Hospital registrars contacted cases regularly, and registry staff reviewed state death certificates to identify deceased registry cases. Cause of death was recorded according to the International Classification of Diseases criteria in effect at the time of death (23). Major causes of death were grouped into five categories: CRC, heart disease, lung cancer, other cause, and missing. Follow-up data through December 2006 were available at the time of analysis. The last date of follow-up was either the date of death or the last date the case was contacted.
Cause of Death and Survival Analyses
Overall survival was defined as mortality from any cause. Thus, censoring events were created for those alive at the end of the follow-up period and cases lost to follow-up. CRC-specific survival was defined as mortality from CRC itself, such that censoring events were created for those alive at the end of the follow-up period, cases lost to follow-up, and cases that died from any cause other than CRC.
Survival curves for CRC, colon cancer, and rectal cancer cases were constructed using the Kaplan-Meier method and analyzed with the log rank test for univariate CRC-specific and overall survival. Univariate stratified survival analyses were also performed for colorectal, colon, and rectal cancer cases across strata for TNM stage (i.e., I, II, III, IV). Cox proportional hazards modeling was performed using time since diagnosis to profile the adjusted risk of overall and CRC-specific mortality based on family history of CRC. Variables known to predict survival in CRC were included in the multivariate survival model, including age, gender, ethnicity, stage at presentation, site within the colon/rectum, tumor histology, surgical treatment rendered at the primary site, radiation therapy, and chemotherapy, with adjustment for family history.
Statistical Analysis
Analyses were performed for colon and rectal cancer cases, stratified by the presence or absence of family history. Comparisons of demographic, clinical, and pathologic variables among colon and rectal cancer cases were performed using Pearson chi-square statistic or Fisher’s exact test for nominal variables and Student t-test for continuous variables. All descriptive analyses were conducted using SAS 9.1 statistical software (SAS Institute, Cary, NC). Statistical significance was assumed for a two-tailed p-value less than 0.05.
We proposed a 10% or greater difference in CRC-specific survival based on family history of CRC for our sample size calculations. Thus, at least 684 total subjects were needed to detect a statistically significant 10% difference in 10-year CRC-specific survival between the two groups: 60% in sporadic CRC cases vs. 70% in familial CRC cases.
RESULTS
Descriptive Analysis
A total of 1174 CRC cases were identified from the UC Irvine Gene-Environment Study of Familial Colorectal Cancer during the specified time period, with a median follow-up duration of 9.3 years. Seven hundred eighty one (66%) of these were colon cancer cases, 373 (32%) were rectal cancer cases, and 20 (2%) were unspecified and thus excluded from further analysis. Clinicopathologic data for the colon and rectal cancer groups are presented in Table 1.
Table 1.
Descriptive Comparisons for Colon and Rectal Cancer Cases
| Colon Cancer |
Rectal Cancer |
|||||||
|---|---|---|---|---|---|---|---|---|
| Total n = 781 | Familial n = 148 | Sporadic n = 633 | P Value* | Total n=373 | Familial n = 60 | Sporadic n = 313 | P Value* | |
| Median Age (years, with range) | 64.0 (22–99) | 64.5 (32–90) | 64.0 (22–99) | 0.66 | 62.0 (24–99) | 65.0 (37–93) | 61.0 (24–99) | 0.0085 |
| Gender | ||||||||
| Male | 416 (53%) | 80 (54%) | 336 (53%) | 215 (58%) | 35 (58%) | 180 (58%) | ||
| Female | 365 (47%) | 68 (46%) | 297 (47%) | 0.83 | 158 (42%) | 25 (42%) | 133 (42%) | 0.91 |
| Ethnicity | ||||||||
| Caucasian | 659 (84%) | 131 (89%) | 528 (83%) | 0.53 | 316 (85%) | 53 (88%) | 263 (84%) | 0.80 |
| African-American | 13 (2%) | 1 (<1%) | 12 (2%) | 5 (1%) | 1 (2%) | 4 (1%) | ||
| Hispanic | 60 (8%) | 9 (6%) | 51 (8%) | 28 (8%) | 3 (5%) | 25 (8%) | ||
| Asian | 46 (6%) | 7 (5%) | 39 (6%) | 24 (6%) | 3 (5%) | 21 (7%) | ||
| Other | 3 (<1%) | 0 (0%) | 3 (<1%) | 0 (0%) | 0 (0%) | 0 (0%) | ||
| Stage at Diagnosis | ||||||||
| I | 201 (26%) | 49 (34%) | 152 (24%) | 0.070 | 140 (39%) | 29 (51%) | 111 (37%) | 0.22 |
| II | 250 (33%) | 43 (30%) | 207 (33%) | 85 (24%) | 9 (16%) | 76 (25%) | ||
| III | 199 (26%) | 29 (20%) | 170 (27%) | 87 (24%) | 13 (23%) | 74 (25%) | ||
| IV | 116 (15%) | 24 (17%) | 92 (15%) | 44 (12%) | 6 (11%) | 38 (13%) | ||
| Tumor Location | ||||||||
| Proximal/transverse | 425 (54%) | 84 (57%) | 341 (54%) | 0.45 | -- | --- | --- | 0.15 |
| Descending | 51 (7%) | 12 (8%) | 39 (6%) | -- | --- | --- | ||
| Sigmoid | 305 (39%) | 52 (35%) | 253 (40%) | -- | --- | --- | ||
| Rectosigmoid | -- | --- | --- | 137 (37%) | 27 (45%) | 110 (35%) | ||
| Rectum | -- | --- | --- | 236 (63%) | 33 (55%) | 203 (65%) | ||
| Histologic Subtype | ||||||||
| Adenocarcinoma | 692 (89%) | 130 (88%) | 562 (89%) | 0.73 | 341 (91%) | 53 (88%) | 288 (92%) | 0.31 |
| Mucinous adenoca | 82 (11%) | 17 (11%) | 65 (10%) | 12 (3%) | 2 (3%) | 10 (3%) | ||
| Carcinoma | 3 (<1%) | 0 (0%) | 3 (<1%) | 16 (4%) | 5 (8%) | 11 (4%) | ||
| Not specified | 3 (<1%) | 1 (<1%) | 2 (<1%) | 4 (1%) | 0 (0%) | 4 (1%) | ||
| Tumor Grade | ||||||||
| 1 | 98 (13%) | 23 (17%) | 75 (13%) | 0.45 | 44 (13%) | 5 (10%) | 39 (14%) | 0.099 |
| 2 | 496 (68%) | 86 (64%) | 410 (69%) | 237 (71%) | 39 (75%) | 198 (70%) | ||
| 3 | 132 (18%) | 26 (19%) | 106 (18%) | 51 (15%) | 7 (13%) | 44 (16%) | ||
| 4 | 2 (<1%) | 0 (0%) | 2 (<1%) | 1 (<1%) | 1 (2%) | 0 (0%) | ||
| Initial Treatment | ||||||||
| Surgery | 753 (97%) | 147 (99%) | 606 (96%) | 0.039 | 348 (93%) | 58 (97%) | 290 (93%) | 0.25 |
| Radiation therapy | 23 (3%) | 4 (3%) | 19 (3%) | 0.85 | 133 (36%) | 19 (32%) | 114 (36%) | 0.48 |
| Chemotherapy | 304 (41%) | 53 (37%) | 251 (42%) | 0.26 | 172 (48%) | 22 (40%) | 150 (50%) | 0.19 |
P-value indicates comparisons between familial and sporadic cases by each listed variable
From the 1154 analyzed cases, 946 sporadic cases and 208 familial cases were identified (183 cases with CRC history in one 1st degree family member, 19 with two affected family members, and 6 with >2 affected family members). Among colon cancer cases, 148 (19%) were considered familial and 633 (81%) were sporadic. Among all rectal cancer cases, 60 (16%) were considered familial and 313 cases (84%) were sporadic. Clinical comparisons between familial and sporadic cases (separately for colon, and rectum) revealed no significant differences in distribution by gender, ethnicity, site within the colon, histologic subtype, or tumor grade (Table 1). While the median age was similar for colon cancer cases regardless of family history, familial rectal cancer cases were younger (median = 61.0 years; range = 24–99 years) than sporadic cases (median = 65 years; range = 37–93 years; p = 0.0085). Familial colon cases presented at an earlier stage than sporadic cases, with more familial cases diagnosed with stage I colon cancer, although this finding did not reach significance (p = 0.070). Individuals with familial colon cancer were also more likely to receive surgical treatment (p = 0.039), while radiation therapy and chemotherapy use were similar for familial and sporadic colon cancer cases (Table 1).
Because of the observed difference in the proportion of familial compared to sporadic colon cancer cases receiving surgery and near significant differences in stage at diagnosis (Table 1), the first course of treatment was further examined for familial and sporadic colon cancer cases, stratified by stage at presentation (Table 2). Among colon cancer cases, surgery, radiation therapy, and chemotherapy use were similar between familial and sporadic colon cancer cases within each stage.
Table 2.
First Course of Treatment for Colon Cancer Cases by Stage and Family History
| Stage at Presentation | |||||
|---|---|---|---|---|---|
| I | II | III | IV | ||
| Surgery | Familial | 49/49 (100%) | 43/43 (100%) | 29/29 (100%) | 23/24 (96%) |
| Sporadic | 149/152 (98%) | 203/207 (98%) | 170/170 (100%) | 77/92 (84%) | |
| P-Value | 0.32 | 0.36 | --- | 0.12 | |
| Radiation | Familial | 0/49 (0%) | 2/43 (5%) | 1/29 (3%) | 1/24 (4%) |
| Sporadic | 0/152 (0%) | 6/207 (3%) | 6/170 (4%) | 7/92 (8%) | |
| P-Value | --- | 0.55 | 0.98 | 0.55 | |
| Chemotherapy | Familial | 0/49 (0%) | 15/42 (36%) | 20/27 (74%) | 17/22 (77%) |
| Sporadic | 4/148 (3%) | 63/196 (32%) | 116/154 (75%) | 65/86 (76%) | |
| P-Value | 0.25 | 0.65 | 0.89 | 0.87 | |
Survival of Colon and Rectal Cancer Cases
Of the 1154 colon or rectal cancer cases combined, 603 (52%) were deceased at the time of analysis. 96 of these were familial cases and 507 were sporadic. Among the 603 deceased CRC cases, cause of death was available for 557 cases (92%). Cause of death was available for 91 of 96 (94.8%) familial and 466 of 507 (91.9%) sporadic cases (P = 0.33). 365 (81%) cases died from CRC. Univariate survival analysis revealed no difference in 10-year CRC-specific survival between familial and sporadic CRC cases (69% vs. 66%; P = 0.51) or 10-year overall survival (55% vs. 49%; P = 0.075). However, in the univariate analyses of colon cancer cases, statistically significant overall survival differences by family history were observed among those with non-metastatic stage at presentation (i.e., TNM stage I, II, or III): 66% 10-year OS for familial colon cancer cases compared to 56% 10-year OS for sporadic colon cancer cases (P=0.021) (Figure 1).
Figure 1.
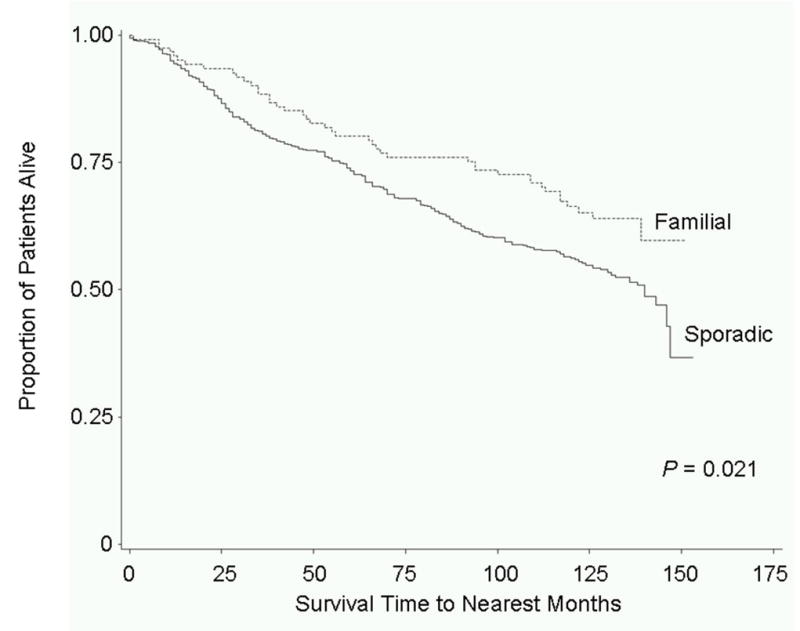
Overall survival by family history of colorectal cancer among non-metastatic colon cancer cases enrolled in the UC Irvine Gene Environment Study of Familial Colorectal Cancer. Cases were diagnosed during 1994–1996 with follow-up through December 2006. Familial colon cancer cases, stage I-III (121 cases, 43 deaths), 10-year OS= 66%; sporadic colon cancer cases, stage I-III (529 cases, 253 deaths), 10-year OS=56%.
For the 781 colon cancer cases, 415 (53%) were deceased at the time of analysis. 67 of these were familial cases and 348 were sporadic. Among the 415 deceased colon cancer cases, cause of death was available for 383 cases (92%). Cause of death was available for 64 of 67 (95.5%) familial and 319 of 348 (91.7%) sporadic cases (P = 0.28). 241 (79%) of these cases died from CRC, 55 (18%) died from cardiac disease, and there were no differences between familial and sporadic colon cancer cases in the distribution of cause-specific deaths (CRC, 81% vs. 78%, heart disease, 19% vs. 18%; P = 0.30).
Of the 373 rectal cancer cases, 188 (50%) were deceased at the time of analysis. 29 of these were familial cases and 159 were sporadic. Among the 188 deceased rectal cancer cases, cause of death was available for 174 cases (92.5%). Cause of death was available for 27 of 29 (93.1%) familial and 147 of 159 (92.5%) sporadic cases (P = 0.90). 124 cases (86%) died from CRC, 19 (13%) died from cardiac disease, and there were no differences between familial and sporadic colon cancer cases in the distribution of cause-specific deaths (CRC, 83% vs. 86%, heart disease, 17% vs. 12%; P = 0.68).
Statistically significant differences in CRC-specific survival were not observed between familial compared to the referent sporadic colon cancer cases in unadjusted analysis, or in the adjusted analysis accounting for age, gender, ethnicity, stage, tumor site, histology, and treatment with surgery, radiation, and chemotherapy (Table 3). However, family history was an independent predictor of overall survival for colon cancer (HR = 0.760, 95% CI 0.580–0.997; P = 0.047) in the adjusted analysis, and a borderline significant difference was detected in the unadjusted analysis (HR = 0.773, 95% CI 0.594–1.005; P = 0.054). Multivariate overall survival analysis for confounding of colon cancer cases by CRC family history revealed that adjusting for stage at diagnosis is the key variable that makes family history become significant. The P-value for family history in the Cox model goes from P = 0.054 in the unadjusted model to P = 0.053 after adjustment for age, then P = 0.034 after additional adjustment for stage at presentation.
Table 3.
Univariate and multivariate adjusted overall survival analysis, and CRC-specific survival analysis for colon cancer cases by self-reported family history of CRC.
| Colon Cancer | Rectal Cancer | |||
|---|---|---|---|---|
| Family History of CRC | Family History of CRC | |||
| No | Yes | No | Yes | |
| Overall Mortality | ||||
| Number of events | 348 | 67 | 159 | 29 |
| Number at risk | 633 | 148 | 313 | 60 |
| Unadjusted HR (95% CI) | 1 (Reference) | 0.773 (0.595–1.005) | 1 (Reference) | 0.937 (0.631–1.392) |
| Adjusted HR (95% CI)* | 1 (Reference) | 0.760 (0.580–0.997) | 1 (Reference) | 0.920 (0.610–1.386) |
| CRC-Specific Mortality | ||||
| Number of events | 197 | 44 | 105 | 19 |
| Number at risk | 633 | 148 | 313 | 60 |
| Unadjusted HR (95% CI) | 1 (Reference) | 0.906 (0.654–1.257) | 1 (Reference) | 0.938 (0.575–1.529) |
| Adjusted HR (95% CI)* | 1 (Reference) | 0.880 (0.621–1.246) | 1 (Reference) | 1.067 (0.641–1.774) |
Includes adjustment for age (years), gender, ethnicity, TNM stage, site within the colorectum, histology, treatment with surgery, radiation therapy, and chemotherapy.
In the analysis of rectal cancer cases, no differences in CRC-specific survival were observed between familial compared to sporadic colon cancer cases in unadjusted analysis, or in the adjusted analysis (HR = 0.920, 95% CI 0.610–1.386; P = 0.69) (Table 3). Family history was not an independent predictor of overall survival for rectal cancer in the adjusted or unadjusted analysis.
Subset analyses of colon cancer were performed to assess the association of family history (vs. no family history of CRC as a referent group) on overall survival stratified by gender, and separately by stage at diagnosis. In the gender-stratified analyses of colon cancer cases, CRC family history was associated with improved overall survival for males (HR = 0.624, 95% CI 0.423–0.920), but not females (HR = 0.937, 95% CI 0.631–1.392). In the multivariate analysis of overall survival by stage, hazards estimates for family history of CRC were as follows: stage I (HR = 0.56, 95% CI 0.28–1.13), stage II (HR = 0.75, 95% CI 0.43–1.30), stage III (HR = 0.82, 95% CI 0.47–1.41), stage IV (HR = 0.77, 95% CI 0.46–1.29).
DISCUSSION
In our analysis, family history of CRC was an independent predictor of overall survival among colon cancer cases but was not associated with CRC-specific survival (Table 3). No disparities in treatment rendered by stage were apparent to explain the decreased overall mortality among familial colon cancer cases in this study.
Our results are most consistent with the report of Kirchhoff et al. in their analysis cohort of 1,469 women (24). That study revealed a significant overall survival benefit among familial CRC cases when compared to sporadic and a non-significant trend toward improved CRC-specific survival among familial compared to sporadic patients (24). Our population consisted of 68% colon and 32% rectal cancer cases, in comparison to the Kirchhoff study, which was comprised of 82% colon and 18% rectal cancer patients (24). Our conclusions are also aligned with results published by the Japanese Research Society for Cancer of the Colon and Rectum; this group detected improved survival among familial colon cancer cases when compared to sporadic cases. However, it is unclear whether overall or CRC-specific mortality was analyzed in this work (14). The recent study by Chan et al revealed significant improvements in disease-free survival and recurrence-free survival, and a non-significant overall survival benefit (HR = 0.75, 95% CI 0.57–1.04) for stage III colon cancer cases with family history of CRC. Although the sample of colon cancer cases available was larger than ours (1087 vs. 781), follow-up time was substantially less (median follow-up of 5.6 years vs. 9.3 years). It is possible, then, that the improved overall survival difference for familial patients will become significant with additional events over the course of follow-up. Thus, our results are generally supportive of the prior research available from these three major studies.
Our results are inconsistent with those reported in the analysis of CRC and CRC family history in the Utah Population Database (12). Among colon cancer patients in that study, a positive family history of the disease did not affect colon cancer-specific or overall survival. Moreover, when their cohort was stratified by age at diagnosis, gender, and type of relative affected, family history appeared to have a negative effect on survival, particularly among younger males who had siblings with colon cancer (12). Our analyses were adjusted for age at diagnosis and gender but were not further stratified by specific type of family member affected with CRC.
Bass et al. reported that women with a family history of CRC were at increased risk both of CRC-specific mortality and death from any cause, and women with more than one affected relative were even more likely to die from CRC or from any cause (13). Finally, among stage IV CRC patients, significant decreases in CRC-specific and overall survival were observed for familial compared to sporadic cancer cases (13). Their cohort was comprised of 73% colon cancer, 26% rectal cancer, and 2% unspecified CRC patients (i.e., similar to our study) (13). Our conclusions may differ from those of Bass et al. because our study population included both males and females. Interestingly, in our gender-stratified analyses of colon cancer cases, the association of CRC family history with improved overall survival was significant for males (HR = 0.624, 95% CI 0.423–0.920) but not females (HR = 0.937, 95% CI 0.631–1.392). Consistent with these data are the stratified analyses from the Chan et al. study, demonstrating that family history was associated with decreased risk of disease recurrence among men but not women (15). Thus, it is possible that the overall survival effects of CRC family history are more pronounced among males than females with colon cancer; however, this gender-specific difference was not detected in CRC-specific survival analyses in our study (data not shown), and improved overall survival was detected in the aforementioned Kirchhoff study (all females) (24). Perhaps the gender-stratified overall survival results in our study merely reflect gender-specific differences in competing risks (discussed below) for familial vs. sporadic colon cancer cases.
Kune et al. observed no survival difference between familial and sporadic CRC cases. However, survival rates were reported after only a 5-year follow-up period (11), while our study investigated mortality after more than 9 years and in a larger cohort. Additionally, the population analyzed by Kune et al. consisted of a lower ratio of colon to rectal cases, with rectal cancer patients accounting for 45% of the total cohort (11). Thus, the large proportion of rectal cases may have negated any effect of family history on survival among colon cancer cases in their analysis.
Variability in adherence to surveillance monitoring, genetic differences, or competing risks could explain our finding that CRC family history is independently associated with improved overall survival among colon cancer cases. Individuals with a family history of the disease may be more likely to undergo regular CRC surveillance or pursue more aggressive treatments once diagnosed with CRC, thereby affecting survival. Differences in microsatellite instability (MSI) and expression of mismatch repair (MMR) proteins between familial and sporadic colon cancer cases could underlie our findings; however, two factors mitigate against this possibility. In the aforementioned study of survival among stage III colon cancer patients, the improvement in survival for familial patients was independent of MSI or MMR status (15). Additionally, we restricted our analyses to non-HNPCC cases, as defined by Amsterdam criteria, thus presumably limiting our analysis of familial cases to those without this genetically-inherited syndrome which has been shown to be highly associated with MSI (6). Thus, additional genetic factors implicated in heterogeneity of response to treatment, such as loss of chromosome 18 in the primary tumor specimen of patients receiving adjuvant chemotherapy (25, 26), must be investigated to explain the observed survival differences among individuals with familial and sporadic colon cancer (27). Differences in competing risks among familial vs. sporadic CRC cases would explain differences in overall survival but not CRC-specific survival, as observed here. If familial CRC cases are less likely to suffer death from competing illnesses (i.e., cardiac disease, pulmonary disease, diabetes mellitus, etc), they might exhibit OS differences without having differences in CRC-SS. Although we cannot entirely account for this in our study design, at least for cardiac-related deaths, observed rates were similar (11.2%–17.5%) between familial and sporadic cases of the colon and rectum.
Family history appears to have no influence on CRC-specific or overall mortality among rectal cancer cases, as shown in Table 2. Although interpretation is limited by small sample size, results are substantiated by a similar finding in the Japanese Research Society for Cancer of the Colon and Rectum analysis (14). Biologic differences in subsite location within the colorectum have been reported previously. Variation in CRC incidence by tumor site and its association to geography, age, and gender led to the concept of distinct CRC diseases based on proximal or distal location in the large bowel (28). Differences by subsite location within the colorectum have been reported for tumor suppressor genes, point mutations, and genetic instability (29–32). Specifically, it has been noted that left sided colon lesions have a higher rate of chromosomal instability whereas right sided colon lesions more often show microsatellite instability (MSI) (33–39). Azzoni et al. studied distinct molecular features of sporadic CRC patients and felt that the different patterns observed according to subsite could reflect different genetic pathways of carcinogenesis (40). Certain environmental factors such as fatty diets and increased bile acid exposure, whether secondary to cholecystectomy or increased fat intake, together with genetic risk factors, may increase the risk of proximal CRC (28, 41–44). However, the consequences of these various derangements on survival after CRC diagnosis are unknown, and these areas remain fertile ground for further exploration.
Our study is retrospective in nature and shares limitations of other population-based studies. Performance status and comorbidity data are not available in this analysis. Differences in the observed age at diagnosis for sporadic and familial rectal cancer may be due to sampling bias in the parent study, as previously described (6). Information on disease progression and site of CRC recurrence to calculate recurrence-free survival are not available through CCR. However, CRC-specific survival is a reasonable approximation of relapse free survival, since the majority of CRC is incurable upon progression. Since all stage CRC cases were included, a lack of CRC-specific events (particularly among cases with early stage tumors) limits the interpretation of these results. The greater proportion of familial colon cancer cases receiving surgery may have influenced our survival analysis, despite adjustment for stage and surgery in the multivariate survival analysis. However, our analysis of treatment by stage reveals that within each stage, no differences in the proportion receiving surgery were observed between familial and sporadic colon cancer cases. Similar proportions of familial and sporadic colon cancer cases received standard therapy in our stage-specific analysis. Surgical resection rates are high in this study, due in part to the fact that we analyzed surgery as any type of surgical procedure directed at the primary tumor. Factors not so easily accounted for may also explain our findings, including differences in institutional treatment standards, physician preferences, and patient beliefs.
Our results support prior reports that CRC family history has a role in colon, but not rectal, cancer mortality. Clinical, genetic, biologic, and behavioral differences to explain this epidemiologic finding are postulated, but conclusive mechanisms underlying our observations are unknown. In the current age of therapeutic advances in CRC management, and with the ever-increasing number of cancer survivors (45), understanding such mechanisms is critical, and may lead to targeted approaches to prevention of recurrent or relapsed disease among CRC survivors.
Acknowledgments
Source of funding: NCI CA-63706 (Anton-Culver) and CA-67151 (Anton-Culver), UC Irvine Department of Epidemiology, Division of Hematology/Oncology, Dept. of Medicine, and the Lon V. Smith Foundation Grant # LVS-18840
References
- 1.Jemal A, Siegel R, Ward E, Hao Y, Xu J, Murray T, Thun MJ. Cancer Statistics, 2008. A Cancer Journal for Clinicians. 2008 doi: 10.3322/CA.2007.0010. [DOI] [PubMed] [Google Scholar]
- 2.Burt RW. Colon cancer screening. Gastroenterology. 2000;119:837–853. doi: 10.1053/gast.2000.16508. [DOI] [PubMed] [Google Scholar]
- 3.Burt RW, Neklason DW. Genetic testing for inherited colon cancer. Gastroenterology. 2005;128:1696–1716. doi: 10.1053/j.gastro.2005.03.036. [DOI] [PubMed] [Google Scholar]
- 4.Burt RW, DiSario JA, Cannon-Albright L. Genetics of colon cancer: Impact of inheritance on colon cancer risk. Annual Review of Medicine. 1995;46:371–379. doi: 10.1146/annurev.med.46.1.371. [DOI] [PubMed] [Google Scholar]
- 5.Aarino M, Sankila R, Pukkala E, Salovaara R, Aaltonen LA, Chapelle Adl, Peltomaki P, Mecklin JP, Jarvinen HJ. Cancer risk in mutation carriers of DNA-mismatch-repair genes. International Journal of Cancer. 1999;81:214–218. doi: 10.1002/(sici)1097-0215(19990412)81:2<214::aid-ijc8>3.0.co;2-l. [DOI] [PubMed] [Google Scholar]
- 6.Peel DJ, Ziogas A, Fox EA, Gildea M, Laham B, Clements E, Kolodner RD, Anton-Culver H. Characterization of hereditary nonpolyposis colorectal cancer families from a population-based series of cases. Journal of the National Cancer Institute. 2000;92:1517–1522. doi: 10.1093/jnci/92.18.1517. [DOI] [PubMed] [Google Scholar]
- 7.Fuchs CS, Giovannucci EL, Colditz GA, Hunter DJ, Speizer FE, Willett WC. A prospective study of family history and the risk of colorectal cancer. N Engl J Med. 1994;331:1669–74. doi: 10.1056/NEJM199412223312501. [DOI] [PubMed] [Google Scholar]
- 8.Johns LE, Houlston RS. A systematic review and meta-analysis of familial colorectal cancer risk. Am J Gastroenterol. 2001;96:2992–3003. doi: 10.1111/j.1572-0241.2001.04677.x. [DOI] [PubMed] [Google Scholar]
- 9.Potter JD, Slattery ML, Bostick RM, Gapstur SM. Colon cancer: a review of the epidemiology. Epidemiol Rev. 1993;15:499–545. doi: 10.1093/oxfordjournals.epirev.a036132. [DOI] [PubMed] [Google Scholar]
- 10.Slattery ML, Kerber RA. Family history of cancer and colon cancer risk: the Utah Population Database. J Natl Cancer Inst. 1994;86:1618–26. doi: 10.1093/jnci/86.21.1618. [DOI] [PubMed] [Google Scholar]
- 11.Kune GA, Kune S, Watson LF. The effect of family history of cancer, religion, parity and migrant status on survival in colorectal cancer. European Journal of Cancer. 1992;28:1484–1487. doi: 10.1016/0959-8049(92)90549-h. [DOI] [PubMed] [Google Scholar]
- 12.Slattery ML, Kerber RA. The impact of family history of colon cancer on survival after diagnosis with colon cancer. International Journal of Epidemiology. 1995;24:888–896. doi: 10.1093/ije/24.5.888. [DOI] [PubMed] [Google Scholar]
- 13.Bass AJ, Meyerhardt JA, Chan JA, Giovannucci EL, Fuchs CS. Family history and survival after colorectal cancer diagnosis. Cancer. 2008;112:1222–1229. doi: 10.1002/cncr.23294. [DOI] [PubMed] [Google Scholar]
- 14.Registry Committee J. R. S. f. C. o. t. C. a. R. Clinical and pathological analyses of patients with a family history of colorectal cancer. Japanese Journal of Clinical Oncology. 1993;23:342–349. [PubMed] [Google Scholar]
- 15.Chan JA, Meyerhardt JA, Niedzwiecki D, Hollis D, Saltz LB, Mayer RJ, Thomas J, Schaefer P, Whittom R, Hantel A, Goldberg RM, Warren RS, Bertagnolli M, Fuchs CS. Association of family history with cancer recurrence and survival among patients with stage III colon cancer. JAMA. 2008;299:2515–23. doi: 10.1001/jama.299.21.2515. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Zell JA, Ignatenko NA, Yerushalmi HF, Ziogas A, Besselsen DG, Gerner EW, Anton-Culver H. Risk and risk reduction involving arginine intake and meat consumption in colorectal tumorigenesis and survival. International Journal of Cancer. 2007;120:459–468. doi: 10.1002/ijc.22311. [DOI] [PubMed] [Google Scholar]
- 17.Zell JA, McEligot AJ, Ziogas A, Holcombe RF, Anton-Culver H. Differential effects of wine consumption on colorectal cancer outcomes based on family history of the disease. Nutrition and Cancer. 2007;59:36–45. doi: 10.1080/01635580701413926. [DOI] [PubMed] [Google Scholar]
- 18.Le H, Ziogas A, Lipkin SM, Zell JA. Effects of Socioeconomic Status and Treatment Disparities in Colorectal Cancer Survival. Cancer Epidemiol. Biomarkers Prev. Accepted and in production. 2008 doi: 10.1158/1055-9965.EPI-07-2774. Slated for Publication August. [DOI] [PubMed] [Google Scholar]
- 19.Fritz AG, Percy C, Jack A, Sobin LH, Parkin DM, Whelan S. International Classification of Diseases for Oncology (ICD-O) 3. Geneva: World Health Organization; 2000. [Google Scholar]
- 20.Fisher B, Redmond C, Brown A, Fisher ER, Wolmark N, Bowman D, Plotkin D, Wolter J, Bornstein R, Legaultpoisson S, Saffer EA. Adjuvant Chemotherapy with and Without Tamoxifen in the Treatment of Primary Breast-Cancer - 5-Year Results from the National Surgical Adjuvant Breast and Bowel Project Trial. Journal of Clinical Oncology. 1986;4:459–471. doi: 10.1200/JCO.1986.4.4.459. [DOI] [PubMed] [Google Scholar]
- 21.NCCN Colon Cancer Clinical Practice Guidelines in Oncology; Version 2.2008. National Comprehensive Cancer Network, Inc; 2006. [Accessed August 6, 2008]. Available at: http://www.nccn.org. [Google Scholar]
- 22.Ziogas A, Anton-Culver H. Validation of family history data in cancer family registries. Am J Prev Med. 2003;24:190–8. doi: 10.1016/s0749-3797(02)00593-7. [DOI] [PubMed] [Google Scholar]
- 23.ICD-9-CM, International Classification of Diseases, Ninth Revision, Clinical Modification. Color Coded. 5. 1, 2, and 3. Los Angeles: Practice Management Information Corporation; 1997. [Google Scholar]
- 24.Kirchhoff AC, Newcomb PA, Trentham-Dietz A, Nichols HB, Hampton JM. Family history and colorectal cancer survival in women. Familial Cancer. 2008 doi: 10.1007/s10689-008-9190-z. [DOI] [PubMed] [Google Scholar]
- 25.Watanabe T, Wu TT, Catalano PJ, Ueki T, Satriano R, Haller DG, Benson AB, 3rd, Hamilton SR. Molecular predictors of survival after adjuvant chemotherapy for colon cancer. N Engl J Med. 2001;344:1196–206. doi: 10.1056/NEJM200104193441603. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Barratt PL, Seymour MT, Stenning SP, Georgiades I, Walker C, Birbeck K, Quirke P. DNA markers predicting benefit from adjuvant fluorouracil in patients with colon cancer: a molecular study. Lancet. 2002;360:1381–91. doi: 10.1016/s0140-6736(02)11402-4. [DOI] [PubMed] [Google Scholar]
- 27.Pasche B. Familial colorectal cancer: a genetics treasure trove for medical discovery. JAMA. 2008;299:2564–5. doi: 10.1001/jama.299.21.2564. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Bufill JA. Colorectal cancer: evidence for distinct genetic categories based on proximal or distal tumor location. Ann Intern Med. 1990;113:779–88. doi: 10.7326/0003-4819-113-10-779. [DOI] [PubMed] [Google Scholar]
- 29.Zhou CZ, Peng ZH, Zhang F, Qiu GQ, He L. Loss of heterozygosity on long arm of chromosome 22 in sporadic colorectal carcinoma. World J Gastroenterol. 2002;8:668–73. doi: 10.3748/wjg.v8.i4.668. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Wiencke JK, Zheng S, Lafuente A, Lafuente MJ, Grudzen C, Wrensch MR, Miike R, Ballesta A, Trias M. Aberrant methylation of p16INK4a in anatomic and gender-specific subtypes of sporadic colorectal cancer. Cancer Epidemiol Biomarkers Prev. 1999;8:501–6. [PubMed] [Google Scholar]
- 31.Gervaz P, Bouzourene H, Cerottini JP, Chaubert P, Benhattar J, Secic M, Wexner S, Givel JC, Belin B. Dukes B colorectal cancer: distinct genetic categories and clinical outcome based on proximal or distal tumor location. Dis Colon Rectum. 44:364–72. doi: 10.1007/BF02234734. discussion 372–3, 2001. [DOI] [PubMed] [Google Scholar]
- 32.Lindblom A. Different mechanisms in the tumorigenesis of proximal and distal colon cancers. Curr Opin Oncol. 2001;13:63–9. doi: 10.1097/00001622-200101000-00013. [DOI] [PubMed] [Google Scholar]
- 33.Delattre O, Olschwang S, Law DJ, Melot T, Remvikos Y, Salmon RJ, Sastre X, Validire P, Feinberg AP, Thomas G. Multiple genetic alterations in distal and proximal colorectal cancer. Lancet. 1989;2:353–6. doi: 10.1016/s0140-6736(89)90537-0. [DOI] [PubMed] [Google Scholar]
- 34.Breivik J, Lothe RA, Meling GI, Rognum TO, Borresen-Dale AL, Gaudernack G. Different genetic pathways to proximal and distal colorectal cancer influenced by sex-related factors. Int J Cancer. 1997;74:664–9. doi: 10.1002/(sici)1097-0215(19971219)74:6<664::aid-ijc18>3.0.co;2-5. [DOI] [PubMed] [Google Scholar]
- 35.Ionov Y, Peinado MA, Malkhosyan S, Shibata D, Perucho M. Ubiquitous somatic mutations in simple repeated sequences reveal a new mechanism for colonic carcinogenesis. Nature. 1993;363:558–61. doi: 10.1038/363558a0. [DOI] [PubMed] [Google Scholar]
- 36.Lothe RA, Peltomaki P, Meling GI, Aaltonen LA, Nystrom-Lahti M, Pylkkanen L, Heimdal K, Andersen TI, Moller P, Rognum TO, et al. Genomic instability in colorectal cancer: relationship to clinicopathological variables and family history. Cancer Res. 1993;53:5849–52. [PubMed] [Google Scholar]
- 37.Reichmann A, Levin B, Martin P. Human large-bowel cancer: correlation of clinical and histopathological features with banded chromosomes. Int J Cancer. 1982;29:625–9. doi: 10.1002/ijc.2910290605. [DOI] [PubMed] [Google Scholar]
- 38.Lengauer C, Kinzler KW, Vogelstein B. Genetic instability in colorectal cancers. Nature. 1997;386:623–7. doi: 10.1038/386623a0. [DOI] [PubMed] [Google Scholar]
- 39.Haydon AM, Jass JR. Emerging pathways in colorectal-cancer development. Lancet Oncol. 2002;3:83–8. doi: 10.1016/s1470-2045(02)00649-6. [DOI] [PubMed] [Google Scholar]
- 40.Azzoni C, Bottarelli L, Campanini N, Di Cola G, Bader G, Mazzeo A, Salvemini C, Morari S, Di Mauro D, Donadei E, Roncoroni L, Bordi C, Sarli L. Distinct molecular patterns based on proximal and distal sporadic colorectal cancer: arguments for different mechanisms in the tumorigenesis. Int J Colorectal Dis. 2007;22:115–26. doi: 10.1007/s00384-006-0093-x. [DOI] [PubMed] [Google Scholar]
- 41.Le Marchand L, Wilkens LR, Hankin JH, Kolonel LN, Lyu LC. A case-control study of diet and colorectal cancer in a multiethnic population in Hawaii (United States): lipids and foods of animal origin. Cancer Causes Control. 1997;8:637–48. doi: 10.1023/a:1018406716115. [DOI] [PubMed] [Google Scholar]
- 42.Steinmetz KA, Potter JD. Food-group consumption and colon cancer in the Adelaide Case-Control Study. II. Meat, poultry, seafood, dairy foods and eggs. Int J Cancer. 1993;53:720–7. doi: 10.1002/ijc.2910530503. [DOI] [PubMed] [Google Scholar]
- 43.Lagergren J, Ye W, Ekbom A. Intestinal cancer after cholecystectomy: is bile involved in carcinogenesis? Gastroenterology. 2001;121:542–7. doi: 10.1053/gast.2001.27083. [DOI] [PubMed] [Google Scholar]
- 44.McMichael AJ, Potter JD. Host factors in carcinogenesis: certain bile-acid metabolic profiles that selectively increase the risk of proximal colon cancer. J Natl Cancer Inst. 1985;75:185–91. [PubMed] [Google Scholar]
- 45.Ganz PA. A teachable moment for oncologists: cancer survivors, 10 million strong and growing! J Clin Oncol. 2005;23:5458–60. doi: 10.1200/JCO.2005.04.916. [DOI] [PubMed] [Google Scholar]