

INTRODUCTION
Musculoskeletal disorders (MSDs) are an important public health issue because of their socio-economic consequences.[1–4]. In recent decades, research have helped to improve epidemiological knowledge and management of MSDs, particularly of the upper limb (MSDUL).
Less is known however about their impact on sick leave in industry. Studies focusing on workers compensation include only a portion of workers [5], because sick leave without claims for compensation for work-related injuries is frequent in countries such as France, where workers are compensated for disability leave regardless of whether the health problem is work-related.
Our objectives were to describe the sickness absence episodes for MSDUL in the French national power and gas company -EDF and Gaz de France (EDF-GDF)- and to study the associations with age, gender, and socio-economic status.
METHODS
Study population
The study population consisted of about 140 000 workers from EDF-GDF. EDF-GDF has its own medical insurance system handled by a department called Service Géneral de Médecine de Contrôle (SGMC). A specificity of this medical system is compulsory verification of any sick time off. All employees with sick leave must see a physician of SGMC’s medical department, who codes diagnoses according to a simplified version of the International Classification of Diseases of the World Health Organization. The information is then recorded in an epidemiology registry. The items available in that database include absences with diagnosis and duration, and the worker’s profile (age, gender, occupation, industrial sector).
Data collection and methods
The database of sick leave from January 2000 to December 2004 was reviewed to identify the absences that might be due to MSDUL. Long-term sick leave (one year or more) were excluded as available data suggested that an absence for MSDUL would rarely be so long. We anticipated that MSDULs would be coded as disease of the locomotor system, aponeuroses and tendons; arthroses or diseases of the nervous system not due to alcohol. A preliminary selection of these categories found 21 890 sickness absence episodes possibly due to MSDUL. For each, a questionnaire was sent to the company physician, who checked whether it was a MSDUL and coded the diagnoses according to a list derived from a European consensus [6]. Finally, 5543 sickness absence episodes were classified as MSDUL.
Annual incidence rates for sick leave due to MSDUL were calculated by gender, age, diagnosis, and socio-economic status (SES) coded according to the French classification [7]. The number of workers with at least one absence due to MSDUL was divided by the number of full-time equivalent workers aged 20–59 years in the corresponding category. Incidence rates according to SES were calculated only for 2004 since this information was not available for the other years.
The number of work days lost per diagnosis was calculated.
Differences in rates were tested using a chi square test. P-values below 0.05 were considered statistically significant throughout the analysis.
This study was made in accordance with ethical requirements for epidemiologic research in France.
RESULTS
Among the 5543 sickness absence episodes, rotator cuff syndrome was diagnosed most frequently, accounting for 31% of absences (Table 1). Other common diagnoses were carpal tunnel syndrome (16%), epicondylitis (14%), and neck MSD (11%). Less frequent diagnoses included extensor/flexor tendonitis and tenosynovitis (8%), elbow, wrist and fingers arthritis (3%), cubital tunnel syndrome (2%), De Quervain’s disease (1%), Guyon’s canal syndrome (0.6%), radial tunnel syndrome (0.4%) and neuropathy caused by vibrations (0.2%). “Other” MSDUL, coded as such because they did not match any of the diagnoses proposed in the questionnaire, accounted for 13%.
Table 1.
Diagnoses associated with sickness absence for MSDUL (1) and average duration of the sickness absences in the period [2000–2004]
| Diagnosis | Number of sickness absences | Average duration of a sickness absence (days) |
|---|---|---|
| Rotator cuff syndrome | 1722 | 30.77 |
| Carpal tunnel syndrome | 866 | 36.74 |
| Epicondilytis | 795 | 20.83 |
| Neck musculoskeletal disorders | 598 | 16.37 |
| Extensor/tensor tendonitis and tenosynivitis | 452 | 23.44 |
| Elbow, wrist and fingers arthrosis | 173 | 31.86 |
| Cubital tunnel syndrome | 94 | 42.68 |
| De Quervain’s disease | 61 | 19.82 |
| Guyon’s canal syndrome | 31 | 55.30 |
| Radial tunnel syndrome | 22 | 27.81 |
| Neuropathy caused by vibrations | 9 | 39.67 |
limited to the diagnoses proposed in the questionnaire
Among the frequent diagnoses, carpal tunnel syndrome and rotator cuff syndrome were associated with the longest sick leave durations (36.7 and 30.7 days respectively). Longer absences were found, however, for less frequent diagnoses, such as Guyon’s canal syndrome (55.3 days).
Most of the workers (77%) had a single sickness absence episode for MSDUL in the study period. For the others, the absences were most often several episodes with the same diagnosis.
The incidence rate of sickness absence spells due to MSDUL increased from 5.3 in 2000 to 6.3 per 1000 person-years in 2004.
Sick leave for MSDUL increased with age and incidence was higher for women than for men (6.5 and 5.7 per 1000 person-years respectively, P < 0.01).
Sick leave due to MSDUL was associated with SES (P < 0.001). Office and blue-collar workers had a higher risk than managers and professionals or intermediate white-collar occupations (Figure 1).
Figure 1.
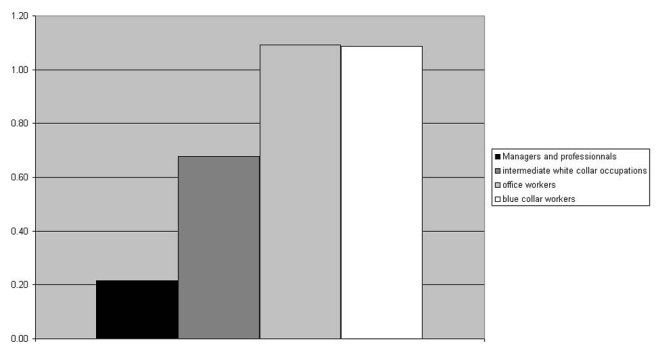
Annual incidence of sickness absence episodes due to MSDUL according to the socio-economic status (incidence per 1000 person-years, year 2004)
DISCUSSION
The study’s weaknesses are its retrospective design and the absence of a standardized clinical examination. Moreover, the shortest absence episodes were not always seen by the physicians (in 2006, 28% of episodes ≤ 7days were not checked). Nonetheless, probably few sick leaves due to MSDUL were missed, since their duration was usually longer (Table 1).
The higher incidence of sickness absence episodes for MSDUL among women, the increase with age and the association with SES are consistent with the literature.[8,9].
The annual incidence of sick leave due to MSDUL was about 6 per 1000 person-years. This result cannot be compared to another one since there is no publication reporting incidence of sick leave for MSDUL [10]. Absenteeism cannot be a surrogate for disease burden or incidence as it depends on attitudes to sick leave, which has many determinants; suffering from MSDUL does not necessarily induce sick leave. Nevertheless, absenteeism is one dimension of the severity of the disorders, a useful indicator for the company and an indicator of the societal cost.
CONCLUSION
The most common diagnoses of MSDUL in sick leaves were rotator cuff syndrome, carpal tunnel syndrome, epicondylitis and neck MSD. Sick leave due to MSDUL was associated with socio-economic status, women had a higher risk and the incidence increased with age. Absenteeism could be a useful indicator in the prevention of MSDUL, because it identifies the most disabling diagnoses as shoulder disorders and shows that older workers, especially manual and office workers, are those most at risk.
References
- 1.Morse TF, Dillon C, Warren N, Levenstein C, Warren A. The economic and social consequences of work-related musculoskeletal disorders: the Connecticut Upper-Limb Surveillance Project (CUSP) Int J Occup Environ Health. 1998;4:209–216. doi: 10.1179/oeh.1998.4.4.209. [DOI] [PubMed] [Google Scholar]
- 2.Thiehoff R. Economic significance of work disability caused by musculoskeletal disorders. Orthopade. 2002;31:949–956. doi: 10.1007/s00132-002-0350-9. [DOI] [PubMed] [Google Scholar]
- 3.Roux CH, Guillemin F, Boini S, et al. Impact of musculoskeletal disorders on quality of life: an inception cohort study. Ann Rheum Dis. 2005;64:606–611. doi: 10.1136/ard.2004.020784. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Morken T, Riise T, Moen B, et al. Frequent musculoskeletal symptoms and reduced health-related quality of life among industrial workers. Occup Med. 2002;52(2):91–98. doi: 10.1093/occmed/52.2.91. [DOI] [PubMed] [Google Scholar]
- 5.Hashemi L, Webster BS, Clancy EA, Courtney TK. Length of disability and cost of work-related musculoskeletal disorders of the upper limb. J Occup Environ Med. 1998;40:261–269. doi: 10.1097/00043764-199803000-00008. [DOI] [PubMed] [Google Scholar]
- 6.Sluiter JK, Rest KM, Frings-Dresen MH. Criteria document for evaluating the work-relatedness of upper-limb musculoskeletal disorders. Scand J Work Environ Health. 2001;27 (Suppl 1):1–102. [PubMed] [Google Scholar]
- 7.Institut National de la Statistique et des Etudes Economiques (INSEE) www.insee.fr.
- 8.Wijnhoven HA, de Vet HC, Picavet HS. Prevalence of musculoskeletal disorders is systematically higher in women than in men. Clin J Pain. 2006;22:717–724. doi: 10.1097/01.ajp.0000210912.95664.53. [DOI] [PubMed] [Google Scholar]
- 9.Melchior M, Krieger N, Kawachi I, et al. Work factors and occupational class disparities in sickness absence: findings from the GAZEL cohort study. Am J Public Health. 2005;95:1206–1212. doi: 10.2105/AJPH.2004.048835. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Huisstede BM, Bierma-Zeinstra SM, Koes BW, Verhaar JA. Incidence and prevalence of upper-extremity musculoskeletal disorders. A systematic appraisal of the literature. BMC Musculoskelet Disord. 2006 Jan 31;7:7. doi: 10.1186/1471-2474-7-7. [DOI] [PMC free article] [PubMed] [Google Scholar]