

Abstract
AIM: To investigate the effects of ketamine anesthesia on the motility alterations and tissue injury caused by ischemia/reperfusion in rats.
METHODS: Thirty male Wistar rats weighing 200-250 g were used. Ischemia was induced by obstructing blood flow in 25% of the total small intestinal length (ileum) with a vascular clamp for 45 min, after which either 60 min or 24 h of reperfusion was allowed. Rats were either anesthetized with pentobarbital sodium (50 mg/kg) or ketamine (100 mg/kg). Control groups received sham surgery. After 60 min of reperfusion, the intestine was examined for morphological alterations, and after 24 h intestinal basic electrical rhythm (BER) frequency was calculated, and intestinal transit determined in all groups.
RESULTS: The intestinal mucosa in rats that were anesthetized with ketamine showed moderate alterations such as epithelial lifting, while ulceration and hemorrhage was observed in rats that received pentobarbital sodium after 60 min of reperfusion. Quantitative analysis of structural damage using the Chiu scale showed significantly less injury in rats that received ketamine than in rats that did not (2.35 ± 1.14 vs 4.58 ± 0.50, P < 0.0001). The distance traveled by a marker, expressed as percentage of total intestinal length, in rats that received pentobarbital sodium was 20% ± 2% in comparison with 25.9% ± 1.64% in rats that received ketamine (P = 0.017). BER was not statistically different between groups.
CONCLUSION: Our results show that ketamine anesthesia is associated with diminished intestinal injury and abolishes the intestinal transit delay induced by ischemia/reperfusion.
Keywords: Ischemia/reperfusion, Ketamine, N-methyl-D-aspartate, Intestinal motility, Tissue damage
INTRODUCTION
Mesenteric ischemia is a clinical entity with a mortality rate between 60% and 100% that usually requires surgical resection of the necrotic intestinal segment[1]. Although there have been advancements in the treatment of ischemic injury, an ideal treatment has not been defined, and new options should be considered. A promising strategy is the use of anesthetic and sedative agents that might exert protective effects on the injured tissue. Ketamine is an agent that has been recommended for this purpose in clinical situations of sepsis, renal ischemia, cerebral ischemia and serious burn injuries[2-4].
The small intestine is very sensitive to ischemic insult[5]. Reperfusion causes additional damage through the release of free radicals, pro-inflammatory cytokines, leukotrienes and other related products[6]. Intestinal ischemia/reperfusion (I/R) damages the intestinal mucosa and alters gastrointestinal motility[7]. The histological damage induced by I/R includes alterations in capillary permeability, mucosal barrier dysfunction, necrosis, epithelial shredding. The damage is reversed in a period of approximately 24 h[8].
The NMDA (N-methyl-D-Aspartate) receptor family is a heterogeneous group of excitatory ionotropic voltage and ligand gate dependent receptors. Ketamine is a parenteral anesthetic that non-competitively blocks the NMDA receptor[9]. It has been shown that ketamine protects various tissues from I/R injury, such as brain[10], myocardium[11] and skeletal muscle[12]. To the best of our knowledge, no previous studies have evaluated the effects of ketamine on intestinal motility impairment and tissue damage induced by I/R.
MATERIALS AND METHODS
Procedures
Animal procedures were performed in accordance with the proper use and care of laboratory animals. Experiments were performed on 30 male Wistar rats weighing 200-250 g. Animals were maintained under standard conditions, such as stable room temperature (24 ± 3°C), a 12 h light/12 h dark cycle, and access to commercial rat pellets and water ad libitum.
Animal models
Briefly, after anesthesia with pentobarbital sodium (Anestesal, Pfizer Inc, Mexico) or ketamine (Anesket, Pisa Agropecuaria, Hidalgo, Mexico), midline laparotomy was performed, and the small intestine was externalized and kept wrapped in humid sterile gauze to prevent dehydration. Rats were placed over a heating mat to maintain constant core temperature (37°C). Intestinal I/R was induced by selective clamping of the vascular supply of an ileum segment consisting of 25% of the total intestinal length with microvascular clamps for 45 min (ischemia) followed by either 60 min or 24 h reperfusion. Ischemia was confirmed by absence of pulsations as well as characteristic changes in intestinal coloration.
Thirty male Wistar rats were randomized into 3 groups (n = 10) depending on the type of anesthetic used. Each group was then divided into 2 subgroups. In subgroup A (n = 5), reperfusion lasted 60 min, and tissue was obtained for histological examination only, while in subgroup B (n = 5) it was extended to 24 h and the animals used to evaluate intestinal transit and intestinal electrical activity.
The control group (n = 10) animals were anesthetized with pentobarbital sodium (50 mg/kg) and sham-operated (only midline laparotomy and gut manipulation). In the SK group (n = 10) animals were anesthetized with pentobarbital sodium (50 mg/kg) and intestinal I/R was induced as described. In the KET group (n = 10) animals were anesthetized with ketamine (100 mg/kg) and intestinal I/R was induced as described.
Intestinal transit and basic electrical rhythm
In subgroup B, after 24 h of reperfusion, animals were anesthetized with pentobarbital sodium (50 mg/kg), mid line laparotomy was performed, and 3 subserosal bipolar electrodes were used to record the electrical activity of the ileum segment that had been subjected to I/R injury using a Power Lab 4/20T (ADInstruments, USA) equipped with 3 DC pre-amplifiers (ADInstruments, USA) to analyze and calculate intestinal Basic Electrical Rhythm (BER). Immediately after 30 min, 2 mL/kg of a non-absorbable charcoal solution marker was instilled through a canula into the proximal end of the ileum segment studied, and after another 30 min the intestine was removed, and the distance traveled by the marker was registered. The distance traveled by a marker was then expressed as percentage of total intestinal length from pylorus to cecum. This was used as an indicator of intestinal transit. Finally, tissue samples were obtained for morphologic examination.
Morphological examination
After the I/R procedure, rats were sacrificed by exsanguination from the aorta. Immediately, tissue samples were obtained and fixed in 10% neutral buffered formalin and embedded in paraffin, then 5 micrometer-thick sections were stained with hematoxylin and eosin and examined under light microscope by a blinded pathologist. The Chiu scale[13] of mucosal injury was used to evaluate the degree of histological alteration on 10 sections of 1 mm each to complete 1 cm per animal and then averaged. The scale consists of values from 0 to 5, where 0 normal mucosa; 1, development of sub epithelial (Gruenhagen’s) spaces; 2, extension of the sub epithelial space with moderate epithelial lifting from the lamina propria; 3, extensive epithelial lifting with occasional denuded villi tips; 4, denuded villi with exposed lamina propria and dilated capillaries; and 5, disintegration of the lamina propria, hemorrhage, and ulceration.
Statistical analysis
Data were analyzed with SPSS 11.0 (SPSS Inc. Software, Chicago, Illinois, USA) statistical software using one-way analysis of variance (ANOVA) and with Tukey-Kramer test so as to determine comparison between groups, and differences between groups, respectively. All values were expressed as mean ± SD and P < 0.05 was considered statistically significant.
RESULTS
Morphological examination
Structural changes in intestinal mucosa in rats of group KET A (ketamine anesthesia) showed moderate alteration such as epithelial lifting, while ulceration, hemorrhage and villi disintegration was observed in rats of group SK A after 45 min of ischemia and 60 min of reperfusion (Figure 1). The results of the quantitative evaluation of structural damage using the Chiu scale were as follows: control A 0.7 ± 0.45, SK A 4.58 ± 0.50 and KET A 2.35 ± 1.14 (Figure 2). Damage in group KET A was significantly reduced in comparison with group SK A (P < 0.0001). However, the damage score in the KET A group did not reach control A group levels, indicating only moderate protection. The degree of mucosal damage after 24 h of reperfusion (subgroups KET B and SK B) was the same as in control rats and showed no statistical significance.
Figure 1.

A: Control A group showing normal mucosa; B: SK A. Changes in intestinal mucosa structure following 45 min of ischemia and 60 min reperfusion; C: KET A. Less damage was observed (all × 40).
Figure 2.
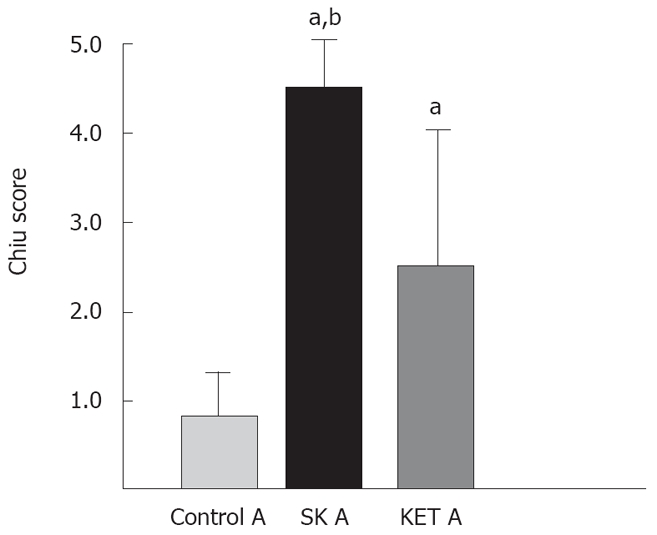
Bar diagram illustrating the Chiu score of mucosal injury after 60 min of reperfusion. Lower damage score was observed in a KET A group than in the SK A group. aP < 0.0001 vs control A; bP < 0.0001 vs KET A.
Intestinal transit and BER
The distance traveled by the marker, expressed as percentage of total intestinal length, in subgroup SK B was 20% ± 2% in comparison with subgroup KET B 25.9% ± 1.64%. In the control B group, the distance traveled was 27% ± 1.4% (Figure 3). Intestinal transit showed statistically significant delay in the SK subgroup compared with the other groups in this study (P = 0.0004). Group KET B showed no significant alteration in transit speed compared to the control B group. The frequency of the BER was not statistically different between any of the groups after 24 h reperfusion: Control B 11.5 ± 1.1/min; SK B 11.2 ± 0.5/min; KET B 11.75 ± 0.95/min.
Figure 3.
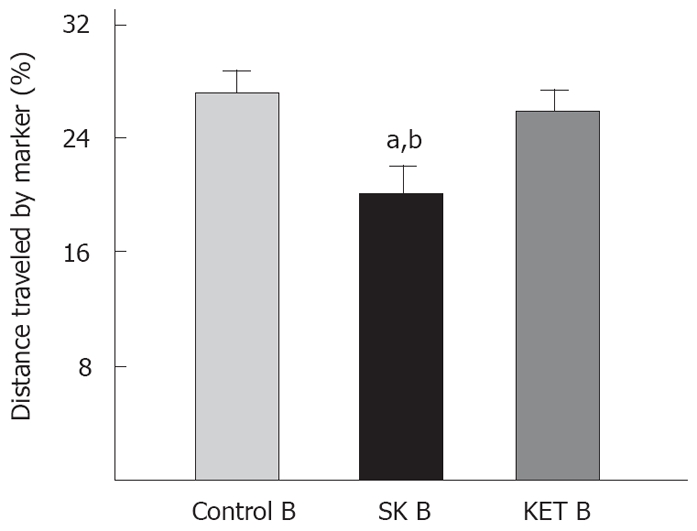
Bar diagram illustrating the distance travelled by the marker, expressed as a percentage of total intestinal length from pylorus to cecum. Intestinal I/R caused transit delay that was corrected by the administration of ketamine as anesthetic. aP = 0.00019 vs control B; bP = 0.0004 vs KET B.
DISCUSSION
The alterations on intestinal motility caused by I/R are directly related to the length of both ischemia and reperfusion[14]. The functional alterations caused by I/R have been previously identified[15]. These changes consist of reversible alterations in smooth muscle contractility and intestinal transit, as well as characteristic changes in electrical activity such as a decrease in BER frequency during ischemia[7,16]. Nitric oxide is one of the mediators thought to participate in the changes caused by I/R on intestinal motility in the rat[17].
The structural damage caused by ischemia is aggravated by the restitution of blood flow. The physiopathology of intestinal mucosal damage by I/R is not completely understood. But, it is believed that cytotoxic substances such as free radicals, nitric oxide, serotonin, complement, as well as neutrophil infiltration and nuclear transcription factors play important roles[18]. Macrophages have been also implicated in the initial damage caused by intestinal I/R[19]. I/R has also been shown to induce apoptosis[20]. Bacterial translocation and mucosal barrier dysfunction have been implicated in the damage caused by I/R in the gut[21]. This damage is also related to an increase in circulating levels of pro-inflammatory cytokines such as interleukin-6 and tumor necrosis factor alpha (TNF-alpha), liberated by the intestine itself[22].
Recently, anti-inflammatory properties of ketamine have been described in various experimental models. Interleukin-1, 6, 8 and TNF-alpha levels are reduced after the administration of ketamine[23-25]. Neutrophil adhesion, migration, and free radical release is inhibited by ketamine[26,27], as is nitric oxide production by macrophages[28]. Further studies are needed to determine whether one of these effects is responsible for the mucosal protection against I/R that we observed in this study.
Glutamate is an excitatory neurotransmitter in the central nervous system, and it participates in the modulation of intestinal function through the enteric nervous system, where NMDA receptors have been found[29]. It has been shown that the glutamate system is involved in the pathogenesis of I/R in brain and intestine[30]. Glutamate release and NMDA receptor activation induces nitric oxide, and other free radicals that cause tissue injury[31]. Glutamate release during I/R could also cause toxicity in the enteric nervous system, which could cause motility alterations[32]. One recent study found that intestinal I/R causes myenteric plexus ganglion cell reduction and death[33]. This suggests that the NMDA receptor could be related to the functional alterations induced in the intestine by I/R. In one study, the NMDA antagonist MK-801 diminished nitric oxide production, and prevented the changes in the intestinal transit caused by intestinal ischemia/reperfusion[34]. We showed that ketamine, an NMDA receptor antagonist, also corrects the intestinal transit delay caused by intestinal I/R, but we did not find any changes in the frequency of the BER after 24 h of reperfusion. Further studies are needed in order to determine whether our results are explained by ketamine acting as an NMDA receptor antagonist in the gut.
Ketamine protects the intestine against other types of non-ischemic insults. Ketamine has been shown to protect the gut against endotoxemia induced injury in rats through diminished pro-inflammatory cytokine release[35]. Ketamine also decreased enterocyte apoptosis in a model of thermal burn induced intestinal injury[36]. However, this is the first study to demonstrate that ketamine anesthesia reduces I/R induced injury in intestinal mucosa.
COMMENTS
Background
In intestinal diseases associated with ischemia and reperfusion, intestinal tissue is damaged and intestinal function is altered. In this study, the aim was to investigate the effects of ketamine anesthesia in rats in which intestinal ischemia/reperfusion was induced.
Research frontiers
The authors suggest that ketamine anesthesia may have beneficial effects that prevent the tissue damage and functional alterations that follow from intestinal ischemia/reperfusion.
Innovations and breakthroughs
This study is the first to show that ketamine anesthesia can reduce the intestinal tissue damage induced by ischemia reperfusion.
Applications
Ketamine should be further studied and the possibility of using ketamine as anesthetic in cases of intestinal ischemia should be considered.
Peer review
Methods and results are clear, but in order for the authors to come to the conclusion that ketamine is functioning as an NMDA receptor antagonist the following experiment needs to be done: Compare the effect of pentobarbital plus a selective NMDA antagonist vs. ketamine plus a selective NMDA antagonist. If the authors’ conclusion is correct the selective NMDA receptor antagonist should “nullify” the beneficial effect of ketamine.
Footnotes
Peer reviewer: Anthony J Bauer, PhD, Department of Medicine/Gastroenterology, University of Pittsburgh, S-849 Scaife Hall, 3550 Terrace Street, Pittsburgh 15261, United States
S- Editor Zhong XY L- Editor Alpini GD E- Editor Ma WH
References
- 1.Chang RW, Chang JB, Longo WE. Update in management of mesenteric ischemia. World J Gastroenterol. 2006;12:3243–3247. doi: 10.3748/wjg.v12.i20.3243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Statler KD, Alexander H, Vagni V, Dixon CE, Clark RS, Jenkins L, Kochanek PM. Comparison of seven anesthetic agents on outcome after experimental traumatic brain injury in adult, male rats. J Neurotrauma. 2006;23:97–108. doi: 10.1089/neu.2006.23.97. [DOI] [PubMed] [Google Scholar]
- 3.Lee HT, Ota-Setlik A, Fu Y, Nasr SH, Emala CW. Differential protective effects of volatile anesthetics against renal ischemia-reperfusion injury in vivo. Anesthesiology. 2004;101:1313–1324. doi: 10.1097/00000542-200412000-00011. [DOI] [PubMed] [Google Scholar]
- 4.Tsao CM, Wu CC, Wang JJ, Wong CS, Tsai SK, Ho ST. Intravenous anesthetics in sepsis. Acta Anaesthesiol Taiwan. 2005;43:153–163. [PubMed] [Google Scholar]
- 5.Tendler DA. Acute intestinal ischemia and infarction. Semin Gastrointest Dis. 2003;14:66–76. [PubMed] [Google Scholar]
- 6.Arumugam TV, Arnold N, Proctor LM, Newman M, Reid RC, Hansford KA, Fairlie DP, Shiels IA, Taylor SM. Comparative protection against rat intestinal reperfusion injury by a new inhibitor of sPLA2, COX-1 and COX-2 selective inhibitors, and an LTC4 receptor antagonist. Br J Pharmacol. 2003;140:71–80. doi: 10.1038/sj.bjp.0705402. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Ballabeni V, Barocelli E, Bertoni S, Impicciatore M. Alterations of intestinal motor responsiveness in a model of mild mesenteric ischemia/reperfusion in rats. Life Sci. 2002;71:2025–2035. doi: 10.1016/s0024-3205(02)01966-5. [DOI] [PubMed] [Google Scholar]
- 8.Haglund U, Bulkley GB, Granger DN. On the pathophysiology of intestinal ischemic injury. Clinical review. Acta Chir Scand. 1987;153:321–324. [PubMed] [Google Scholar]
- 9.Annetta MG, Iemma D, Garisto C, Tafani C, Proietti R. Ketamine: new indications for an old drug. Curr Drug Targets. 2005;6:789–794. doi: 10.2174/138945005774574533. [DOI] [PubMed] [Google Scholar]
- 10.Himmelseher S, Durieux ME. Revising a dogma: ketamine for patients with neurological injury? Anesth Analg. 2005;101:524–534, table of contents. doi: 10.1213/01.ANE.0000160585.43587.5B. [DOI] [PubMed] [Google Scholar]
- 11.Kato R, Foex P. Myocardial protection by anesthetic agents against ischemia-reperfusion injury: an update for anesthesiologists. Can J Anaesth. 2002;49:777–791. doi: 10.1007/BF03017409. [DOI] [PubMed] [Google Scholar]
- 12.Salman AE, Dal D, Salman MA, Iskit AB, Aypar U. The effect of ketamine on acute muscular ischaemia reperfusion in rats. Eur J Anaesthesiol. 2005;22:712–716. doi: 10.1017/s0265021505001171. [DOI] [PubMed] [Google Scholar]
- 13.Chiu CJ, McArdle AH, Brown R, Scott HJ, Gurd FN. Intestinal mucosal lesion in low-flow states. I. A morpho-logical, hemodynamic, and metabolic reappraisal. Arch Surg. 1970;101:478–483. doi: 10.1001/archsurg.1970.01340280030009. [DOI] [PubMed] [Google Scholar]
- 14.Pawlik WW, Thor P, Sendur R, Biernat J, Koziol R, Wasowicz P. Myoelectric bowel activity in ischemia/reperfusion damage. Role of sensory neurons. J Physiol Pharmacol. 1998;49:543–551. [PubMed] [Google Scholar]
- 15.Moore-Olufemi SD, Kozar RA, Moore FA, Sato N, Hassoun HT, Cox CS Jr, Kone BC. Ischemic preconditioning protects against gut dysfunction and mucosal injury after ischemia/reperfusion injury. Shock. 2005;23:258–263. [PubMed] [Google Scholar]
- 16.Ladipo JK, Seidel SA, Bradshaw LA, Halter S, Wikswo JP Jr, Richards WO. Histopathologic changes during mesenteric ischaemia and reperfusion. West Afr J Med. 2003;22:59–62. doi: 10.4314/wajm.v22i1.27982. [DOI] [PubMed] [Google Scholar]
- 17.Takahashi A, Tomomasa T, Kaneko H, Watanabe T, Tabata M, Morikawa H, Tsuchida Y, Kuwano H. Intestinal motility in an in vivo rat model of intestinal ischemia-reperfusion with special reference to the effects of nitric oxide on the motility changes. J Pediatr Gastroenterol Nutr. 2001;33:283–288. doi: 10.1097/00005176-200109000-00010. [DOI] [PubMed] [Google Scholar]
- 18.Cerqueira NF, Hussni CA, Yoshida WB. Pathophysiology of mesenteric ischemia/reperfusion: a review. Acta Cir Bras. 2005;20:336–343. doi: 10.1590/s0102-86502005000400013. [DOI] [PubMed] [Google Scholar]
- 19.Chen Y, Lui VC, Rooijen NV, Tam PK. Depletion of intestinal resident macrophages prevents ischaemia reperfusion injury in gut. Gut. 2004;53:1772–1780. doi: 10.1136/gut.2003.034868. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Noda T, Iwakiri R, Fujimoto K, Matsuo S, Aw TY. Programmed cell death induced by ischemia-reperfusion in rat intestinal mucosa. Am J Physiol. 1998;274:G270–G276. doi: 10.1152/ajpgi.1998.274.2.G270. [DOI] [PubMed] [Google Scholar]
- 21.Chang JX, Chen S, Ma LP, Jiang LY, Chen JW, Chang RM, Wen LQ, Wu W, Jiang ZP, Huang ZT. Functional and morphological changes of the gut barrier during the restitution process after hemorrhagic shock. World J Gastroenterol. 2005;11:5485–5491. doi: 10.3748/wjg.v11.i35.5485. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Grotz MR, Deitch EA, Ding J, Xu D, Huang Q, Regel G. Intestinal cytokine response after gut ischemia: role of gut barrier failure. Ann Surg. 1999;229:478–486. doi: 10.1097/00000658-199904000-00005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Kawasaki T, Ogata M, Kawasaki C, Ogata J, Inoue Y, Shigematsu A. Ketamine suppresses proinflammatory cytokine production in human whole blood in vitro. Anesth Analg. 1999;89:665–669. doi: 10.1097/00000539-199909000-00024. [DOI] [PubMed] [Google Scholar]
- 24.Taniguchi T, Kanakura H, Takemoto Y, Kidani Y, Yamamoto K. Effects of ketamine and propofol on the ratio of interleukin-6 to interleukin-10 during endotoxemia in rats. Tohoku J Exp Med. 2003;200:85–92. doi: 10.1620/tjem.200.85. [DOI] [PubMed] [Google Scholar]
- 25.Taniguchi T, Yamamoto K. Anti-inflammatory effects of intravenous anesthetics on endotoxemia. Mini Rev Med Chem. 2005;5:241–245. doi: 10.2174/1389557053175407. [DOI] [PubMed] [Google Scholar]
- 26.Weigand MA, Schmidt H, Zhao Q, Plaschke K, Martin E, Bardenheuer HJ. Ketamine modulates the stimulated adhesion molecule expression on human neutrophils in vitro. Anesth Analg. 2000;90:206–212. doi: 10.1097/00000539-200001000-00041. [DOI] [PubMed] [Google Scholar]
- 27.Nishina K, Akamatsu H, Mikawa K, Shiga M, Maekawa N, Obara H, Niwa Y. The inhibitory effects of thiopental, midazolam, and ketamine on human neutrophil functions. Anesth Analg. 1998;86:159–165. doi: 10.1097/00000539-199801000-00032. [DOI] [PubMed] [Google Scholar]
- 28.Shimaoka M, Iida T, Ohara A, Taenaka N, Mashimo T, Honda T, Yoshiya I. Ketamine inhibits nitric oxide production in mouse-activated macrophage-like cells. Br J Anaesth. 1996;77:238–242. doi: 10.1093/bja/77.2.238. [DOI] [PubMed] [Google Scholar]
- 29.Liu MT, Rothstein JD, Gershon MD, Kirchgessner AL. Glutamatergic enteric neurons. J Neurosci. 1997;17:4764–4784. doi: 10.1523/JNEUROSCI.17-12-04764.1997. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Xu L, Sun J, Lu R, Ji Q, Xu JG. Effect of glutamate on inflammatory responses of intestine and brain after focal cerebral ischemia. World J Gastroenterol. 2005;11:733–736. doi: 10.3748/wjg.v11.i5.733. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Said SI, Berisha HI, Pakbaz H. N-methyl-D-aspartate receptors outside the central nervous system: activation causes acute lung injury that is mediated by nitric oxide synthesis and prevented by vasoactive intestinal peptide. Neuroscience. 1995;65:943–946. doi: 10.1016/0306-4522(95)00021-a. [DOI] [PubMed] [Google Scholar]
- 32.Kirchgessner AL, Liu MT, Alcantara F. Excitotoxicity in the enteric nervous system. J Neurosci. 1997;17:8804–8816. doi: 10.1523/JNEUROSCI.17-22-08804.1997. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Linhares GK, Martins JL, Fontanezzi F, Patricio Fdos R, Montero EF. Do lesions of the enteric nervous system occur following intestinal ischemia/reperfusion? Acta Cir Bras. 2007;22:120–124. doi: 10.1590/s0102-86502007000200008. [DOI] [PubMed] [Google Scholar]
- 34.Calcina F, Barocelli E, Bertoni S, Furukawa O, Kaunitz J, Impicciatore M, Sternini C. Effect of N-methyl-d-aspartate receptor blockade on neuronal plasticity and gastrointestinal transit delay induced by ischemia/reperfusion in rats. Neuroscience. 2005;134:39–49. doi: 10.1016/j.neuroscience.2005.03.052. [DOI] [PubMed] [Google Scholar]
- 35.Sun J, Wang XD, Liu H, Xu JG. Ketamine suppresses endotoxin-induced NF-kappaB activation and cytokines production in the intestine. Acta Anaesthesiol Scand. 2004;48:317–321. doi: 10.1111/j.0001-5172.2004.0312.x. [DOI] [PubMed] [Google Scholar]
- 36.Yagmurdur H, Aksoy M, Arslan M, Baltaci B. The effects of propofol and ketamine on gut mucosal epithelial apoptosis in rats after burn injury. Eur J Anaesthesiol. 2007;24:46–52. doi: 10.1017/S0265021506000986. [DOI] [PubMed] [Google Scholar]