

Abstract
AIM: To evaluate the role of pentavalent Tc-99m dimercaptosuccinic acid [Tc-99m (V) DMSA] in the diagnosis of ischemic colitis.
METHODS: Fourteen patients with endoscopically and histologically confirmed ischemic colitis were included in the study. Tc-99m (V) DMSA scintigraphy was performed within 2 d after colonoscopy. Images were considered positive when an area of increased activity was observed in the region of interest and negative when no abnormal tracer uptake was detected.
RESULTS: In 3 out of the 14 patients, Tc-99m (V) DMSA images showed moderate activity in the bowel. The scintigraphic results corresponded with the endoscopic findings. In the other 11 patients, no abnormal tracer uptake was detected in the abdomen.
CONCLUSION: Besides the limited number of patients, Tc-99m (V) DMSA could not be considered as a useful imaging modality for the evaluation of ischemic colitis.
Keywords: Scintigraphy, Technetium-99m pentavalent dimercaptosuccinic acid, Ischemic colitis, Intestinal ischemia, Diagnosis
INTRODUCTION
Ischemic colitis (IC) initially was described by Boley et al in 1963[1] and represents the most common form of gastrointestinal ischemia[2]. It is presented either as an occlusive or a nonocclusive form, usually seen in the elderly population with associated co-morbid factors[2-4]. Its pathophysiologic characteristic is the sudden loss of blood flow and the extent of damage is proportional to the degree and the duration of tissue hypoxia[5,6]. Moreover the disruption of the mucosal barrier may lead to inflow of intraluminal bacteria and toxins from the gut[3]. The clinical spectrum ranges from transient self-limited ischemia with brief episodes of abdominal pain and rectal bleeding to fulminant transmural necrosis, perforation and death[5,6]. The histological findings include mucosal necrosis and ulcerations, submucosal edema and haemorrhage or transmural infarction[2,3,5].
The identification of colonic ischemia is highly dependent upon clinical suspicion[2,7]. Although invasive, colonoscopy and colonic biopsies have become the standard for diagnosing ischemic colitis[6,8].
The radionuclide imaging in IC is an area under investigation. Since mucosal inflammatory changes often coexist with bowel ischemia, radiotracers used to localise inflammation could probably play an important role in the diagnosis of IC. A few reports of the scintigraphic findings using radionuclide labelled leukocytes have been published[9-12]. Moreover, recently pentavalent Tc-99m dimercaptosuccinic acid [Tc-99m (V) DMSA] has been successfully used in the identification of intestinal inflammation[13-15]. To our knowledge, its role in the diagnosis of intestinal ischemia has not been yet reported in the literature.
The aim of the present study was to determine whether Tc-99m (V) DMSA scintigraphy could provide an alternative non-invasive imaging modality in the diagnosis of IC.
MATERIALS AND METHODS
Patients
We examined fourteen patients, (5 males and 9 females, mean age 70.6 years) with clinically, endoscopically and histologically confirmed IC. All patients included were admitted at the Department of Gastroenterology of the University Hospital Heraklion, Crete, Greece, within two days after the onset of symptoms. The patients were non-surgically treated and non-received medical therapy that would interfere with scintigraphic results. Half of the patients reported daily tobacco use. Endoscopic assessment was performed the day following the hospital admission in all cases.
Concerning the disease type, transient IC was the most frequent presenting in 9 patients (62.4%) followed by reversible ischemic colopathy in 3 patients (21.4%), chronic ulcerative IC in 1 patient (7.1%) and ischemic colonic stricture in 1 patient (7.1%).
The lesions were distributed depending on their locations: splenic flexure in 8 patients (57.1%), rectosigmoid in 3 patients (21.4%), right colon in 2 patients (14.2% and extensive IC in 1 patient (7.1%)
All patients were subjected to standard laboratory tests such as red and white blood cell counts, haemoglobin and hematocrit level, platelet count, albumin level, erythrocyte sedimentation rate and C-reactive protein level. Colonoscopy with biopsies was performed in all patients. The endoscopic findings for each bowel segment were evaluated by blinded specialists.
The study was approved by the ethics committee and patients were provided with an informed consent.
Scintigraphic imaging
Tc-99m (V) DMSA scintigraphy was performed in fourteen patients with IC. In all patients scintigraphy was performed within 2 d after colonoscopy, in order to avoid any variation in disease activity. Imaging was performed after intravenous administration of 555 MBq (15 mCi) of Tc-99m (V) DMSA. A gamma-camera (Millenium; GE Medical Systems, Milwaukee, Wis) equipped with a low energy all purpose collimator was used. With the patient in the supine position, planar views of the abdomen were obtained 4 hours after radiotracer injection. Before scanning patients were asked to void their bladders to avoid false results.
The bowel was divided to five segments: small bowel (A), ascending colon (B), transverse colon (C), descending colon (D) and rectosigmoid (E). Images were considered positive when an area of increased uptake was observed and negative when no abnormal tracer uptake was detected in any of the five segments. In the event of a positive result, semi quantitative measurements were included with reference to the uptake in the iliac crest and was graded as: 0: No uptake in the region of interest, 1: Faint uptake less than the iliac crest bone marrow, 2: Moderate uptake similar to that of the iliac crest, 3: Severe uptake greater than the iliac crest bone marrow.
Scintigrams were blindly evaluated by three nuclear medicine physicians (MIS, SIK, NSK) and the results were compared with endoscopic and clinical data.
RESULTS
No patients showed adverse events during or after scintigraphy. A total of fourteen patients were included in this study. In all patients, endoscopy revealed characteristic findings suggestive of IC, which was histologically confirmed. In three out of the fourteen patients, the Tc-99m (V) DMSA scintigraphy demonstrated moderate uptake in the bowel (Figure 1A). Compared to endoscopic findings, radionuclide images were in agreement with the segments concerned. In the other eleven patients, Tc-99m (V) DMSA revealed no increased uptake in the bowel at all (Figure 1B).
Figure 1.
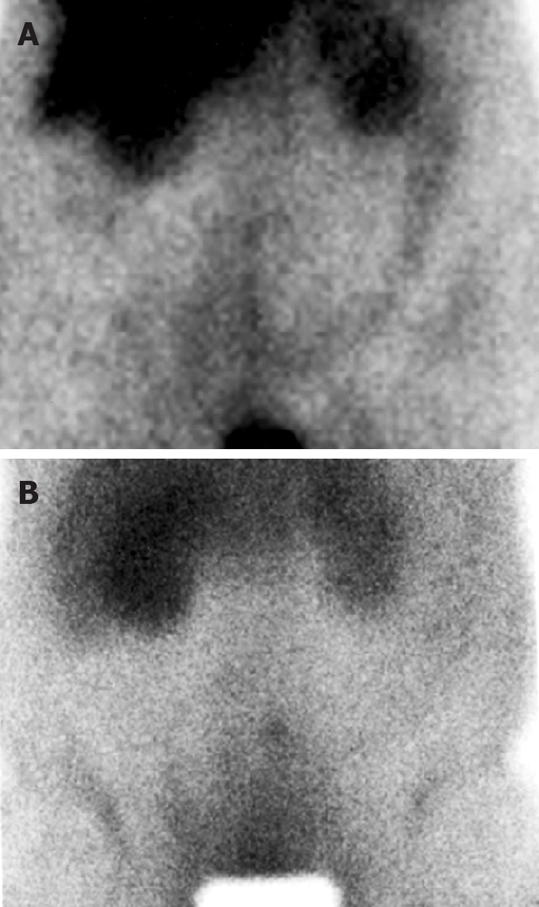
Anterior Tc-99m (V) DMSA scintigram in a patient with ischemic colitis: Moderate uptake of the radiotracer in the splenic flexure and the descending colon (A) and no uptake of the radiotracer in the bowel (B).
Positive cases included one case with localization in the splenic flexure, one with ischemic rectosigmoiditis and one with extensive IC. Concerning the disease type among positive cases there were two cases with transient IC and one with chronic ulcerative IC. The small number of cases does not permit further statistical analysis.
The calculated sensitivity was only 21.4%. Owing to the low sensitivity and the false-negative results the study was stopped.
DISCUSSION
The most important finding in our study was that the majority of the patients with IC, who underwent Tc-99m (V) DMSA scintigraphy, yielded false- negative results. Only three of them showed increased tracer uptake in the regions of interest which corresponded with the findings at colonoscopy.
The pathophysiologic basis of IC is the sudden loss of blood supply. Localized low flow states involve mostly the splenic flexure and the rectosigmoid junction while systemic low flow states involve mostly the right colon, follow a relatively benign course and may affect younger patients[4,5,7,8].
Colonic ischemia may be precipitated by several conditions, such as shock, colon cancer, surgical intervention on the aorta or the mesenteric vessels, autoimmune disease, coagulopathies, long-distance running, constipation, illicit drug use and medications[2,4,6]. Recent studies have suggested a role of prothrombotic disorders in the development of IC[16,17].
No test specific for IC has yet been developed. The diagnosis of IC depends on the clinical evaluation of the patient in association with the biochemical, radiological, endoscopic and histologic assessment[18]. Most laboratory tests will be normal usually, yet in the event of abnormal results they have been found nonspecific[3,5,8].
Radiological evidence includes a wide spectrum of findings, which are frequently nonspecific, insensitive, and often they cannot easily differentiate ischemic from other forms of colitis[5,7,8].
Endoscopic assessment is the most sensitive and specific method of evaluating the colon for ischemic injury. The visual inspection and the ability to biopsy the mucosa allow the clinician in the majority of cases to make a firm diagnosis[6,8].
CT imaging has been employed in the evaluation of patients with abdominal pain of unknown etiology. Besides its limitations, it may be used to detect abnormalities and suggest the diagnosis, exclude other serious medical conditions and narrow the differential diagnosis[19-21].
Non-invasive Doppler sonography has been used as well. Although a high specificity has been reported, it is limited by overlying bowel gas, operator dependent quality and poor sensitivity for low flow vessel disease[3,5,8].
More recently, scintigraphic methods have been used in the diagnosis of IC. In-111 or Tc-99m labeled leukocyte scintigraphy has been studied and demonstrated successful imaging of bowel infarction, yet the localization mechanism still remains unclear. It is suggested that the presence of polymorphonuclear leukocytes in the inflammatory response to tissue ischemia, as a result of reperfusion injury may play the primary role[9-12]. However, the time-consuming preparation procedure, the handling and the reinjection of blood constitute shortcomings of radiotracer labeled leukocyte imaging.
Tc-99m (V) DMSA is a low-molecular weight complex that has been used successfully in the scintigraphic diagnosis of inflammation[22,23]. The suggested mechanisms of uptake by inflammatory lesions is either the infiltration into the interstitial space caused by increased capillary permeability or its similar behavior to phosphate ion since it seems to accumulate in areas where calcification is present[22,23].
Its role in the evaluation of intestinal inflammation has been already reported[13,14], moreover when compared to Tc-99m HMPAO labeled leukocytes, it seems to provide a useful, non-invasive, practical, easy to prepare and accurate alternative method for the assessment of disease activity in patients with IBD[15].
Based on the simultaneous presence of inflammatory response to tissue ischemia, we assumed that Tc-99m (V) DMSA could localize successfully the ischemic bowel and assist in the detection and diagnosis of IC.
The results of our study stand in contrast with the aforesaid assumption. The expected abnormally increased uptake was detected only in three out of the fourteen patients with IC while all other cases yielded false-negative scintigraphic results which were probably due to the presence of a milder degree of inflammatory response compared to the positive ones. It is possible that in the false negative cases of our study there was mainly a transient mucosal congestion and the chronic inflammation was not sufficient to provide successful bowel uptake of the radiotracer.
In conclusion, our data suggest that Tc-99m (V) DMSA has no possible role in the detection and diagnosis of IC.
COMMENTS
Background
Pentavalent Tc-99m dimercaptosuccinic acid [Tc-99m (V) DMSA] has been proved advantageous in the imaging of various inflammatory lesions, intestinal inflammation included.
Research frontiers
Tc-99m (V) DMSA could successfully localize the ischemic bowel and assist in the diagnosis of IC due to the simultaneous presence of inflammatory response to tissue ischemia.
Innovations and breakthroughs
We examined fourteen patients, (5 males and 9 females, mean age 70.6 years) with clinically, endoscopically and histologically confirmed IC. In all patients scintigraphy was performed within 2 d after colonoscopy, in order to avoid any variation in disease activity. In three out of the fourteen patients, the Tc-99m (V) DMSA scintigraphy demonstrated moderate uptake in the bowel however in the other eleven patients, Tc-99m (V) DMSA revealed no increased uptake in the bowel at all (false negative results).
Applications
Despite the fact that Tc-99m (V) DMSA scintigraphy has been used successfully in the evaluation of intestinal inflammation it seems to have no role in the diagnosis of ischemic colitis.
Peer review
The present study is relevant as it emphasizes the role of radionuclide imaging in IC and the focus of interest in future studies.
Footnotes
Peer reviewers: Rami Eliakim, Professor, Department of Gastroenterology, Rambam Medical Center, PO Box 9602, Haifa 31096, Israel; Wallace F Berman, MD, Professor, PO Box 3009 DUMC, Durham, NC 27710, United States
S- Editor Zhong XY L- Editor Alpini GD E- Editor Lin YP
References
- 1.Boley SJ, Schwartz S, Lash J, Sternhill V. Reversible vascular occlusion of the colon. Surg Gynecol Obstet. 1963;116:53–60. [PubMed] [Google Scholar]
- 2.Scharff JR, Longo WE, Vartanian SM, Jacobs DL, Bahadursingh AN, Kaminski DL. Ischemic colitis: spectrum of disease and outcome. Surgery. 2003;134:624–629; discussion 629-630. doi: 10.1016/s0039-6060(03)00308-8. [DOI] [PubMed] [Google Scholar]
- 3.MacDonald PH. Ischaemic colitis. Best Pract Res Clin Gastroenterol. 2002;16:51–61. doi: 10.1053/bega.2001.0265. [DOI] [PubMed] [Google Scholar]
- 4.Arnott ID, Ghosh S, Ferguson A. The spectrum of ischaemic colitis. Eur J Gastroenterol Hepatol. 1999;11:295–303. doi: 10.1097/00042737-199903000-00014. [DOI] [PubMed] [Google Scholar]
- 5.Sreenarasimhaiah J. Diagnosis and management of ischemic colitis. Curr Gastroenterol Rep. 2005;7:421–426. doi: 10.1007/s11894-005-0013-1. [DOI] [PubMed] [Google Scholar]
- 6.Anon R, Bosca MM, Sanchiz V, Tosca J, Almela P, Amoros C, Benages A. Factors predicting poor prognosis in ischemic colitis. World J Gastroenterol. 2006;12:4875–4878. doi: 10.3748/wjg.v12.i30.4875. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Sreenarasimhaiah J. Diagnosis and management of intestinal ischaemic disorders. BMJ. 2003;326:1372–1376. doi: 10.1136/bmj.326.7403.1372. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Baixauli J, Kiran RP, Delaney CP. Investigation and management of ischemic colitis. Cleve Clin J Med. 2003;70:920–921, 925-926, 928-930 passim. doi: 10.3949/ccjm.70.11.920. [DOI] [PubMed] [Google Scholar]
- 9.Bell D, Jackson M, Connaughton JJ. Indium-111 neutrophil imaging in ischemic colitis. J Nucl Med. 1986;27:1782–1783. [PubMed] [Google Scholar]
- 10.Moallem AG, Gerard PS, Japanwalla M. Positive In-111 WBC scan in a patient with ischemic ileocolitis and negative colonoscopies. Clin Nucl Med. 1995;20:483–485. doi: 10.1097/00003072-199506000-00001. [DOI] [PubMed] [Google Scholar]
- 11.Vijayakumar V, Bekerman C, Blend MJ. Preoperative prediction of extent and severity of ischemic colitis by imaging with in-111 labeled leukocytes. Clin Nucl Med. 1991;16:98–102. doi: 10.1097/00003072-199102000-00007. [DOI] [PubMed] [Google Scholar]
- 12.Hyun H, Pai E, Blend MJ. Ischemic colitis: Tc-99m HMPAO leukocyte scintigraphy and correlative imaging. Clin Nucl Med. 1998;23:165–167. doi: 10.1097/00003072-199803000-00008. [DOI] [PubMed] [Google Scholar]
- 13.Lee BF, Chiu NT, Wu DC, Tsai KB, Liu GC, Yu HS, Wang ST. Use of 99mTc (V) DMSA scintigraphy in the detection and localization of intestinal inflammation: comparison of findings and colonoscopy and biopsy. Radiology. 2001;220:381–385. doi: 10.1148/radiology.220.2.r01au30381. [DOI] [PubMed] [Google Scholar]
- 14.Koutroubakis IE, Koukouraki SI, Dimoulios PD, Velidaki AA, Karkavitsas NS, Kouroumalis EA. Active inflammatory bowel disease: evaluation with 99mTc (V) DMSA scintigraphy. Radiology. 2003;229:70–74. doi: 10.1148/radiol.2291020692. [DOI] [PubMed] [Google Scholar]
- 15.Stathaki MI, Koutroubakis IE, Koukouraki SI, Karmiris KP, Moschandreas JA, Kouroumalis EA, Karkavitsas NS. Active inflammatory bowel disease: head-to-head comparison between 99mTc-hexamethylpropylene amine oxime white blood cells and 99mTc(V)-dimercaptosuccinic acid scintigraphy. Nucl Med Commun. 2008;29:27–32. doi: 10.1097/MNM.0b013e3282f1bc37. [DOI] [PubMed] [Google Scholar]
- 16.Koutroubakis IE, Sfiridaki A, Theodoropoulou A, Kouroumalis EA. Role of acquired and hereditary thrombotic risk factors in colon ischemia of ambulatory patients. Gastroenterology. 2001;121:561–565. doi: 10.1053/gast.2001.27227. [DOI] [PubMed] [Google Scholar]
- 17.Koutroubakis IE, Theodoropoulou A, Sfiridaki A, Kouroumalis EA. Low plasma protein Z levels in patients with ischemic colitis. Dig Dis Sci. 2003;48:1673–1676. doi: 10.1023/a:1025441405688. [DOI] [PubMed] [Google Scholar]
- 18.Robert JH, Mentha G, Rohner A. Ischaemic colitis: two distinct patterns of severity. Gut. 1993;34:4–6. doi: 10.1136/gut.34.1.4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Balthazar EJ, Yen BC, Gordon RB. Ischemic colitis: CT evaluation of 54 cases. Radiology. 1999;211:381–388. doi: 10.1148/radiology.211.2.r99ma28381. [DOI] [PubMed] [Google Scholar]
- 20.Thoeni RF, Cello JP. CT imaging of colitis. Radiology. 2006;240:623–638. doi: 10.1148/radiol.2403050818. [DOI] [PubMed] [Google Scholar]
- 21.Wiesner W, Mortele KJ, Glickman JN, Ji H, Khurana B, Ros PR. CT findings in isolated ischemic proctosigmoiditis. Eur Radiol. 2002;12:1762–1767. doi: 10.1007/s00330-001-1288-8. [DOI] [PubMed] [Google Scholar]
- 22.Lee BF, Chiu NT, Chang JK, Liu GC, Yu HS. Technetium-99m(V)-DMSA and gallium-67 in the assessment of bone and joint infection. J Nucl Med. 1998;39:2128–2131. [PubMed] [Google Scholar]
- 23.Ercan MT, Gulaldi NC, Unsal IS, Aydin M, Peksoy I, Hascelik Z. Evaluation of Tc-99m(V) DMSA for imaging inflammatory lesions: an experimental study. Ann Nucl Med. 1996;10:419–423. doi: 10.1007/BF03164803. [DOI] [PubMed] [Google Scholar]