

Advances in brain imaging techniques have provided a significant opportunity for the study of brain development in humans. Functional magnetic resonance imaging (fMRI) is the most promising and broadly used imaging technology that is also safe for use in pediatric populations. Insights gained from the veritable explosion of research in this area have significant applications in issues concerning courtrooms and classrooms, as described in the target article (Fenton et al. 2009). The current ethical debate focuses on the experience of participating in volunteer-based research and the application of research results to real-life situations. In this commentary, I analyze the experience of children who participate in non-clinical fMRI research and consider aspects that improve the experience for children.
A child who comes into the research laboratory participates for any of a number of reasons. Most often, one or both parents have identified a research opportunity at a university, college, or medical center, and have presented that opportunity to their child. The child will sign an assent form specific to that research study that outlines the risks and benefits of participation. This form also emphasizes the point that the child may discontinue involvement at any time and for any reason. For more discussion of issues of medical consent and assent in children see Hinton 2002; Rosen and Gur 2002.
ORIENTATION
For fMRI studies with children, it is common practice to bring the child in for an orientation and sometimes screening session prior to scheduling the scan session. In our laboratory, children watch a 12-minute video prepared especially for research taking place at our scan center. The video follows a young girl as she arrives at the scan center with her mother, where she is taught the game she will play inside of the scanner, prepared for scanning (no metal in pockets, no jewelry, for example), placed in the scanner, scanned, and is given the opportunity to look at pictures of her brain at the end of the study.
After the video is shown, the experimenter spends time discussing and reiterating what was learned in the video. Other laboratories that use fMRI to collect neural data in children tend to use similar videos, or they may use pictures or provide the child with physical practice inside a scan simulator or mock scanner. The mock scanner may include recorded MRI sounds, a screen for stimulus presentation/movie viewing, supine positioning of the child on a moving table, and button box for the child to key in responses. Some mock scanners measure movement of children to provide the children with feedback about their movement and effectively train them to stay still while being scanned.
Orientation to the fMRI session is one of the strongest determinants of how positive that experience will be for the child. A child must be given the information necessary to make the decision to participate, and that decision must not be rushed. After orientation in our laboratory, we typically encourage parents and children to go home and talk about whether or not they would like to participate in the study. This gives them the chance to absorb what they learned and let it ‘settle in’ before making a commitment.
MOVEMENT
We explain to children that one of the greatest challenges to participating in fMRI research is remaining still for the duration of the scan. We explain that we would like them to be in exactly the same position from the start of the study all the way through, until we are finished. This is an important concept for children to grasp for successful data collection, and also for their comfort.
Children cannot merely be told to stay still; they need to be told how still is still, and they must be told why this matters. If not told why, children may imagine that if they move they will be shocked or hurt or that they will break the machine. We do not leave children to speculate about why it matters that they do not move. Children are told that even a few millimeters of movement (defined for the child as smaller than a pencil eraser) is too much. They are told that if they move more than this amount, the pictures of their brain will be blurry and the data for the experiment may be unfit for use.
Children want to be successful; therefore, the message that follows naturally is how the researcher will help them to achieve this goal. Children are told that to help them stay still, they will lay their head inside of a helmet with ample padding, and they will bite into a dental wax so they can keep their mouth in the same spot. They are told that these things will help them and that they must also remain aware of staying still at all times.
Once children have the bite bar in, we have them practice coughing, talking, and swallowing before starting the scan. Helping them to feel less constricted and know their capabilities is helpful to their comfort.
ANXIETY
A number of articles have reported that children experience greater anxiety or fear during MRI scanning than do adults (Davidson et al. 2003; Rosenberg et al. 1997). To address this question, our laboratory collected data to test the reliability of these observations in a healthy cross-section of children that volunteered for non-clinical research.
During the study, we asked 50 children and adolescents and 43 adults to respond to an online survey after undergoing a fMRI scan as part of a cognitive behavior/neuroimaging study. Questions were organized into six topics, including physical comfort, emotional comfort, enjoyment/enthusiasm, alertness/engagement, perceived task performance, and researcher interaction.
Significant differences and a trend were obtained between children and adults for alertness/engagement, researcher comfort, and enjoyment/enthusiasm; interestingly, in these three categories, it was children who gave the most positive ratings. There were no significant differences between children and adults in measures of physical comfort, emotional comfort, or perception of performance (Thomason, unpublished data). It appears, therefore, that children do not report significantly greater emotional distress than do adults. Indeed, to the contrary, children report greater enjoyment of being scanned. These data highlight the positive side of enrolling children in research studies. We attribute these differences to the added care with which children are ushered through the research study.
MOTIVATION
We performed a study of children’s motivations for participating in MRI research. We asked children to rank, by importance, the reasons they chose to participate in our study. The top four statements endorsed by children (in order) were: 1) “I wanted to earn some money;” 2) “It sounded like it would be fun;” 3) “I wanted to help scientists learn about the brain;” and 4) I wanted to see pictures of my brain.”
CONCLUSION
As neuroimaging healthy children becomes more common, it is important to remember that the comfort needs of children are different than those of adults and to adjust for them. In this commentary, I have described some of the alterations to adult protocols that are particularly important.
Children benefit from participating in neuroimaging research studies, particularly when researchers use the experience as a teaching tool. In fMRI research studies, children have the rare opportunity to interact with a cutting-edge technology, gain exposure to potential career choices, and contribute to critically needed research. These are striking benefits that are sometimes overshadowed during discourse on the apparent vulnerability of this special population (Figure 1).
Figure 1.
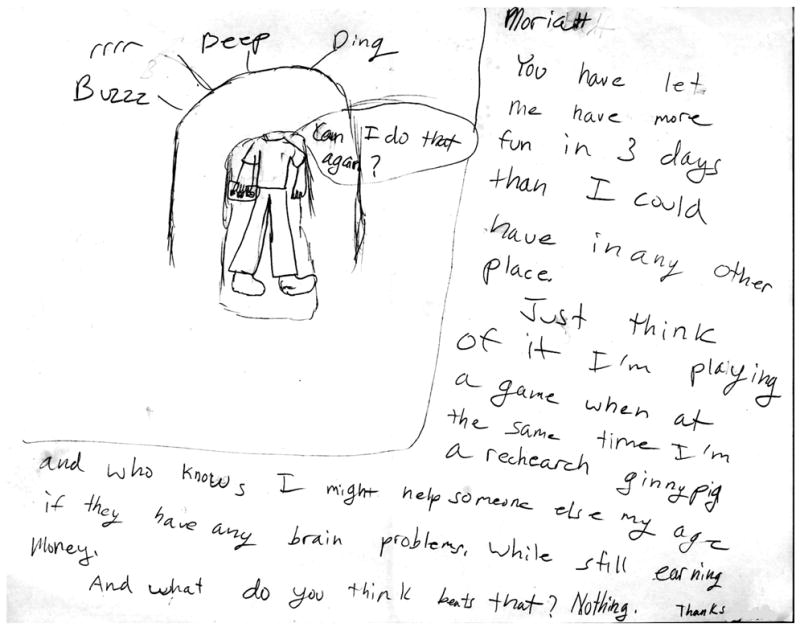
Drawing spontaneously submitted to the research team after 9-year-old female participated in her third fMRI research scan as part of a multi-session study. She relates well her enthusiasm, thanks, and feelings about her potential for helping other children.
References
- Davidson MC, Thomas KM, Casey BJ. Imaging the developing brain with fMRI. Mental Retardation and Developmental Disabilities Research Reviews. 2003;9(3):161–167. doi: 10.1002/mrdd.10076. [DOI] [PubMed] [Google Scholar]
- Fenton A, Meynell L, Baylis F. Ethical challenges and interpretive difficulties with non-clinical applications in pediatric fMRI. American Journal of Bioethics (AJOB Neuroscience) 2009;9(1):3–13. doi: 10.1080/15265160802617829. [DOI] [PubMed] [Google Scholar]
- Hinton VJ. Ethics of neuroimaging in pediatric development. Brain and Cognition. 2002;50(3):455–468. doi: 10.1016/s0278-2626(02)00521-3. [DOI] [PubMed] [Google Scholar]
- Rosen AC, Gur RC. Ethical considerations for neuropsychologists as functional magnetic imagers. Brain and Cognition. 2002;50(3):469–481. doi: 10.1016/s0278-2626(02)00535-3. [DOI] [PubMed] [Google Scholar]
- Rosenberg DR, Sweeney JA, Gillen JS, Kim J, Varanelli MJ, O’Hearn KM, et al. Magnetic resonance imaging of children without sedation: Preparation with simulation. Journal of the American Academy of Child & Adolescent Psychiatry. 1997;36(6):853–859. doi: 10.1097/00004583-199706000-00024. [DOI] [PubMed] [Google Scholar]