

Abstract
In recent years, dynamic contrast enhanced MRI (DCE-MRI) has altered the clinical management for women with breast cancer. In March 2007, the American Cancer Society (ACS) issued a new guideline recommending annual MRI screening for high-risk women. This guideline is expected to substantially increase the number of women each year who receive breast MRI. The diagnosis of breast MRI involves the description of morphological and enhancement kinetics features. To standardize the communication language, the Breast Imaging-Reporting and Data System (BI-RADS) MRI lexicon was developed by the American College of Radiology (ACR). In this article, we will review various appearances of breast lesions on MRI using the standardized terms of ACR BI-RADS MRI lexicon. The purpose is to familiarize all medical professionals with the breast MRI lexicon, since the use of this imaging modality is rapidly growing in the field of breast disease. Using this common language, a comprehensive analysis of both morphological and kinetic features used in image interpretation will help radiologists and other clinicians to communicate more clearly and consistently. This may in turn help physicians and patients to jointly select an appropriate management protocol for each patient’s clinical situation.
Keywords: DCE-MRI, breast MRI, BI-RADS MRI lexicon, breast cancer, breast lesions
INTRODUCTION
In March 2007 the American Cancer Society (ACS) issued a new guideline recommending annual screening for high-risk women using breast magnetic resonance imaging (MRI). MRI is recommended as an adjunct to mammography for women with lifetime risk of 20–25% or greater, which include women with a strong family history of breast or ovarian cancer and women who had been treated for Hodgkin disease.1 For women with a 15 to 20% lifetime risk, based on the analysis of multiple risk factors such as a personal history of breast cancer, carcinoma in situ, atypical hyperplasia, and extremely dense breasts on mammography, the ACS suggested that the screening decisions should be made on a case by case basis.2
Breast MRI can alter the clinical management for a sizable fraction of women with early-stage breast cancer, and helps in determining the optimal local treatment.3–6 Kuhl et al. concluded that MRI screening of women with a history of familial or hereditary breast cancer can achieve a significantly higher sensitivity and a more favorable stage of detection than mammography.7 Lehman et al. reported that MRI could detect clinically and mammographically occult breast cancer in the contralateral breast in 3.1% (30/969) of women with newly diagnosed breast cancer.8 Use of MRI to improve estimation of lesion extent and identification of multifocal and multicentric malignant lesions will affect the patient management decisions.9–13 Recently a large study has shown that MRI has a higher sensitivity than mammography for detecting ductal carcinoma in situ (DCIS), especially for high-grade DCIS.14
However, despite its high sensitivity, MRI also detects many benign lesions. A false positive report may lead to patient anxiety, unnecessary biopsies, and even over-treatment. Breast MRI studies have shown a wide range of diagnostic specificity. Combined analysis of morphologic appearance and enhancement kinetic features based on BI-RADS descriptors will facilitate better characterization of lesions and may have the potential to improve specificity without significant compromise in sensitivity.
To standardize breast MRI reporting, the American College of Radiology (ACR) began to develop the Breast Imaging-Reporting and Data System (BI-RADS) MRI lexicon in 1998.15 The familiar language already used by the ACR BI-RADS for mammography was incorporated, if it also applied to describe corresponding MRI features. For findings seen on MRI only without a correlate on mammography, new terms were developed for the breast MRI lexicon.16 Terms like non-mass-like enhancement, enhancement patterns and description of contrast enhancement kinetics were unique to breast MRI lexicon. The terminologies for breast composition, including fatty, scattered fibroglandular tissue, heterogeneously dense fibroglandular tissue, and extremely dense fibroglandular tissue were also adopted.16–20 During the development of MRI lexicon, many studies were undertaken using numerous morphologic and kinetic features.21–24 Eventually in 2003, the first edition of ACR BI-RADS MRI lexicon was published along with the updated version of ACR BI-RADS for mammography and breast ultrasound, all contained in a single volume.15 Besides providing an almost similar set of descriptors for lesions seen on mammography, breast ultrasound, and breast MRI, the other purpose of BI-RADS is to provide a framework for correlation of lesion appearance and management recommendation with clinical follow-up and biopsy outcomes.
The objective of the current article is to review various MRI patterns using the standardized terms of ACR BI-RADS MRI lexicon. Based on literature search we also correlate various MRI patterns with the commonly encountered breast pathologic types.
TECHNICAL ISSUES IN BREAST MRI
MRI scanners
In 2003 US FDA revised the guidelines for MRI examination and a magnetic field up to 8T is allowed for adults, children, and infants age > 1 month.25 Although imaging performed on 1.5-T MRI systems provides adequate spatial and temporal resolution, much imaging is now performed at 3.0 T due to increased signal-to-noise ratio (SNR) and higher spatial resolution achieved by the higher field strength scanners.26–27 It is recommended that 3.0T breast MRI must be interpreted with great caution, due to the higher magnetic field inhomogeneity which may result in reduction of lesion enhancement.28 However, the scan heterogeneity is not much of a problem if small field of view (FOV) breast imaging is acquired.
Image acquisition
Breast MRI must be performed with a dedicated breast surface coil. A standard protocol includes acquisition of high resolution T1 weighted images. A dynamic contrast enhanced (DCE) three dimensional (3D) gradient echo sequence (GRE), with multiple acquisition frames, is usually used to measure the kinetics of contrast agents in the lesion. In order to differentiate kinetic features of various breast lesions, a high temporal resolution in the order of 40–120 seconds per dynamic acquisition is required.26, 29–31 High spatial resolution is also highly desirable for assessing morphology such as margins and internal architecture.29 For unilateral breast imaging a small field of view (FOV) of 16–20 cm is used, while for bilateral imaging, the FOV has to increase to 30–35 cm. The spatial resolution can be acquired up to 512 in most clinical scanners.26 29–30, 32 Fat suppression is required to delineate contrast-enhanced lesions that become isointense with adjacent fatty tissue. Active fat suppression or subtraction method can be used.26, 32 The maximum intensity projections (MIPs) are commonly generated to demonstrate the enhancement distribution patterns.
A pre-contrast T2-weighted sequence is generally acquired to identify structures such as cysts, fibroadenomas, and lymph nodes.18 Diffusion weighted imaging (DWI) is increasingly being used to investigate its role on diagnosis and therapy monitoring.33–42 Recent studies have demonstrated the potential of DWI for distinguishing benign from malignant breast lesions.38–42
NORMAL BREAST MRI
Normal fibroglandular tissue generally exhibits low level of enhancement at an early time after contrast administration, and shows a gradual progressive, faint enhancement over time. Due to the hormonal responsiveness of the breast in premenopausal women, MRI enhancement varies with the phase of menstrual cycle. During weeks 1 and 4 of the menstrual cycle, enhancements may be stronger and more rapid, presenting a diffuse or focal pattern. It is therefore recommended that breast MRI is best performed during the second week of the menstrual cycle.26, 43–46 The nipple areolar complex may enhance intensely.
BREAST TUMOR ANGIOGENESIS AND ENHANCEMENT
The microvascular density plays a major role in determining the initial rate of contrast medium uptake and the heterogeneity of tumor enhancement.47–49
The steepest slope on a time signal intensity curve or the percentage of maximal signal increase correlates well with the micro-vessel count.47, 50 A higher ratio of micro-vessels in the tumor periphery than in the tumor center is more commonly seen in a high grade versus low grade tumors, and also in malignant lesions versus benign lesions. Early rim enhancement correlates well with a high ratio of peripheral-to-central micro-vessel density and peripheral vascular endothelial growth factor (VEGF) expression.51–55 Quantitative DCE-MRI measurements could be used as a marker to monitor tumor anti-angiogenic therapy.56–58
ACR BI-RADS MRI LEXICON
ACR BI-RADS MRI lexicon includes two major categories of descriptors: morphology and enhancement kinetics. Morphologically, lesions can be separated into focus/foci, mass, and non-mass-like enhancements. A focus is a breast lesion smaller than 5 mm. A mass is a 3 dimensional space-occupying lesion and is characterized by shape (round, oval, lobulated, irregular), margin (smooth, irregular, spiculated), and internal mass enhancement characteristics (homogeneous, heterogeneous, rim enhancement, dark internal septations, enhancing internal septations, and central enhancement). Non-mass-like enhancement is characterized by the distribution pattern (focal, linear, ductal, segmental, regional, multiple regions, and diffuse). The distribution pattern of non-mass-like enhancement can be further characterized by internal characteristics (homogeneous, heterogeneous, stippled/punctate, clumped, reticular/dendritic), and whether the enhancement is symmetric or asymmetric between both breasts (Figure 1). Other associated findings such as lymphadenopathy, and invasion of pectoralis muscle are reported as well.
Figure 1.

Depending on the dominant morphological features, lesions can be separated into focus/foci, mass, and non-mass-like enhancements. A focus can not be further characterized due to the small size. A mass is characterized by shape, margin, and the internal enhancement characteristics. A non-mass-like enhancement is characterized by the overall distribution pattern of enhancement, and further by the internal enhancement characteristics, and whether the enhancement is symmetric or asymmetric between both breasts.
Evaluation of enhancement kinetic curve is based on the temporal enhancement characteristics of the lesion over time. The initial enhancement phase refers to increase in signal intensity within the first 2 minutes after contrast injection, or when the curve starts to change. It is described as fast, medium, and slow, which is more qualitative than quantitative. The delayed enhancement phase refers to the signal intensity curve after 2 minutes or after curve starts to change, and it is described as persistent (continuously increasing enhancement), plateau (signal intensity remains constant after the initial peak), or wash-out (decrease in signal intensity) (Figure 2).15
Figure 2.

The descriptor for the enhancement kinetics is based on two different phases: the initial phase and the delayed phase. The kinetics showing rapid initial enhancement followed by wash-out or plateau is suspicious of malignancy; while that showing medium or slow initial enhancement followed by persistent enhancement is more likely benign.
MORPHOLOGICAL DESCRIPTORS
Mass
A mass is a space-occupying lesion ≥ 5mm. In general, a mass is composed of a three-dimensional pathological process. For a mass lesion, the major diagnostic consideration is either invasive breast cancer or a solid benign tumor such as a fibroadenoma.43
Shape and Margin
A “Round” mass is spherical, ball shaped or circular. An “Oval” mass is elliptical or egg-shaped. A “Lobulated” mass has an undulating or scalloped contour, while an “Irregular” mass is uneven in shape and cannot be characterized as either round, oval or lobulated.15 Margin refers to the border of the mass lesion with surrounding breast tissues. “Smooth” margin is well-defined and sharply demarcated. “Irregular” margin is uneven, ill-defined or indistinct and can have round or jagged edges but is not smooth or spiculated. “Spiculated” margin is characterized by radiating lines extending from the margin of the mass.15
Amongst various shapes, the highest inter-observer agreement was the irregular shape, which suggests cancer; and the lobulated shape, which suggests fibroadenoma.20
Internal Enhancement Characteristics
This describes the enhancement pattern within the abnormally enhancing structure. “Homogenous enhancement” shows confluent uniform enhancement within the entire mass. “Heterogeneous enhancement” is non-uniform with variable signal intensity. “Rim enhancement” shows more pronounced enhancement towards the periphery than the center. “Dark Internal Septations” are non-enhancing lines within a mass; while “Enhancing Internal Septations” are enhancing lines within a mass. The “Central Enhancement pattern” shows more pronounced enhancement at the center of the mass.15
Histopathological Association
Margin assessment is considered as one of the most important features with high positive predictive value in characterization of a breast mass.59 Masses with smooth margins strongly suggest benign disease.60 It was reported that 97 to 100% of masses with smooth margins were benign.61–63 Poorly enhanced lobulated masses and lobulated masses with non-enhancing septations were also benign features, predominantly representing fibroadenoma (Figure 3) or fibrocystic changes.30, 63–65 Fibroadenomas can exhibit variable enhancements, depending on their degree of fibrosis and if there is hormonal stimulation of the breast. In myxoid fibroadenomas, enhancement is typically strong but it persists into the late phase, which makes it different from the wash-out pattern commonly seen in cancer.26 A homogenous internal enhancement pattern has a high predictive value for a benign lesion such as a fibroadenoma.66 However, the pattern can also be a presentation of invasive cancer (Figure 4A). A lobulated mass with non-enhancing internal septations may also be seen in phyllodes tumor, which constitutes 0.3–1.0% of all breast tumors and has the potential to grow to a large size and become invasive.67 Phyllodes tumors tend to have more heterogeneous internal structures.
Figure 3.

Fibroadenoma in a 30 year-old (y/o) patient. (A) Pre-contrast, axial view T1 weighted image showing a well defined lobulated mass with smooth margin; (B) Contrast-enhanced T1 weighted image at 1.5 minute showing mild enhancement, suggesting a benign lesion. (C) Contrast-enhanced subtraction image clearly showing the enhancement of the lesion.
Figure 4.

(Left) pre-contrast axial view T1-weighted images, (Right) contrast-enhanced subtraction images. (A) Invasive ductal carcinoma in a 68 y/o patient. Note a round shaped mass with well defined and smooth margin showing strong enhancement; (B) Invasive lobular carcinoma in a 71 y/o patient. A lobulated mass in the right breast showing heterogeneous enhancement; (C) Invasive ductal carcinoma in a 47 y/o patient. Note an irregular shaped mass with spiculated margin and rim enhancement.
When correlated with biomarker status, the main morphological presentation in most triple negative breast cancers (negative for estrogen receptor, progesterone receptor, and HER-2 receptor) is mass (97%), reflecting its phenotype of being a ductal cancer.68 HER-2 positive cancer has been found to have more multiple mass lesions than its HER-2 negative counterparts (57% vs. 15%).69 Estrogen receptor positive breast cancer shows significantly more mass lesions compared to estrogen receptor negative breast cancer (100% vs. 82%); however, both cancer types do not show significant difference in lesion multiplicity.70
Lobulated mass without septations, mass with enhancing septations, or moderate to marked heterogeneous enhancement of a mass with wash-out kinetics is highly suggestive of malignancy; however, not specific to certain cancer types.30 They may be manifesting features of some invasive ductal carcinoma (IDC), invasive lobular cancer (ILC), medullary carcinoma, and colloid carcinoma (Figure 4B).63–64, 71 Irregular mass, and mass with spiculated margin or rim enhancement are also associated with high positive predictive value (80–100%) for malignancy,23, 59, 61–63, 66 usually representing IDC (Figure 4C).63, 72 The rim enhancement, when appears in a small tumor, is highly suggestive of cancer, but its prevalence is low (about 20%).30, 60 The rim enhancement is more frequently seen in invasive ductal cancers with a higher histological grade and larger size,73 where it may not be a necessary finding for imaging diagnosis.
Spiculated margins are usually associated with IDC and less commonly with tubular carcinoma. Spiculated margins can also be seen with some benign lesions such as radial scars, where assessment of enhancement kinetics may help to reach a conclusive diagnosis.43, 63 ILC or DCIS can also manifest as irregular mass or mass with spiculated margin.63
Focus/Foci
A focus is a focal enhancement smaller than 5mm; and because of the small size, it cannot be well characterized morphologically. Focus or foci (multiple separated spots) may cause a spurious result for analysis of the enhancement kinetic curve, due to volume averaging effect with the surrounding normal tissue in the selected ROI.15 A focus is usually due to a benign lesion such as focal fibrocystic change (Figure 5A), 74 papilloma, small fibroadenoma (Figure 5B), or intramammary lymph node, but although rarely, it may also represent a focal DCIS (Figure 5C) or a small invasive cancer (Figure 5D).26 In a retrospective study of 666 consecutive nonpalpable, mammographically occult lesions that had MRI-guided localization, Liberman et al. concluded that biopsy is rarely necessary for lesions smaller than 5 mm because of their low (3%) likelihood of cancer.75 Nevertheless, the management of a focus lesion should depend on other findings in the same or the opposite breast (such as symmetry), corresponding findings from mammography or ultrasound, as well as the risk status of the patient.26, 43
Figure 5.
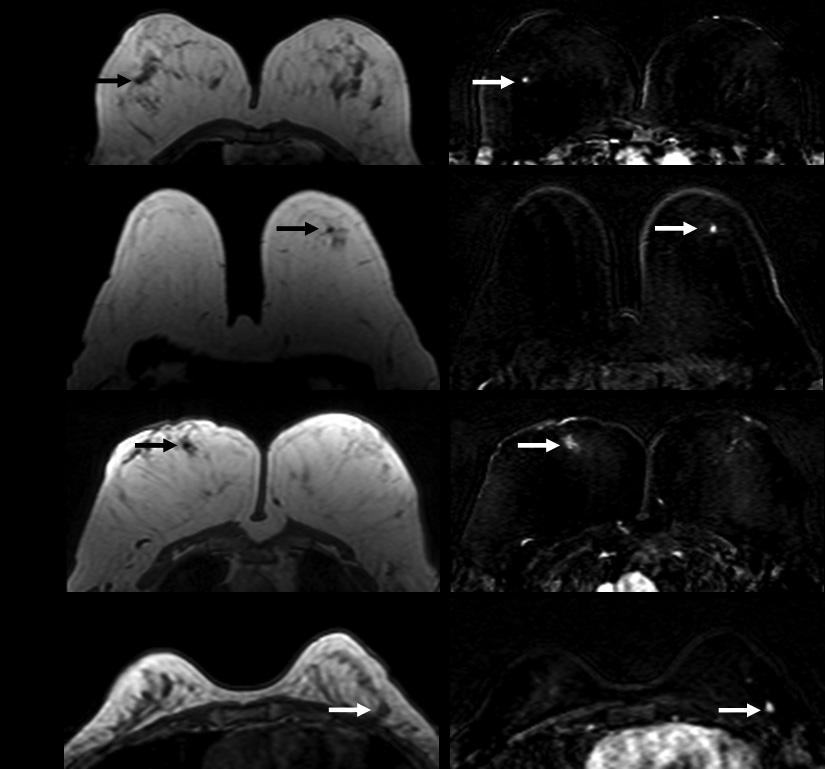
(Left) pre-contrast axial T1-weighted images showing hypointense foci; (Right) contrast-enhanced subtraction images showing strong enhancement. (A) Focal fibrocystic changes of the right breast in a 60 y/o patient. Note a single enhancing focus in the right breast; (B) Fibroadenoma in a 62 y/o patient; (C) Intermediate grade pure DCIS in a 79 y/o patient; (D) Invasive ductal carcinoma in a 52 y/o patient. All arrows indicate lesions.
Non-Mass-Like Enhancement
Non-mass-like enhancement is enhancement of an area that is neither a mass nor a blood vessel. The enhancement pattern is distinct from normal surrounding breast parenchyma. There is no space-occupying effect. Lesions that present as non-mass-like enhancement include DCIS, ILC, mastopathic changes (focal adenosis), fibrocystic changes due to hormonal stimulation, or inflammatory changes.26, 43, 76 Fewer than 20% of cases of estrogen receptor negative invasive ductal cancer shows non-mass-like enhancement, whereas no estrogen positive cancer shows such presentation.70
Distribution pattern
The distribution pattern can be described as: focal, linear, ductal, segmental, regional, multiple regions, and diffuse. A focal area of non-mass-like enhancement is defined as a single small, confined abnormal enhancing area occupying less than 25% of a breast quadrant. It is different from a focus, which by definition measures less than 5mm. A focal area of non-mass-like enhancement usually has fat or normal glandular tissue interspersed between the abnormally enhancing components except when it is a focal area of homogenous enhancement.15
Linear enhancement is enhancement along a line not conforming to a ductal pattern (Figure 6A). On a three dimensional image or on a coronal image it can be seen as a sheet rather than a line or may traverse the breast from left to right in a non-ductal distribution.15
Figure 6.

(Left) pre-contrast axial view T1-weighted images, (Right) contrast-enhanced subtraction images. (A) Invasive mammary carcinoma with ductal and lobular features in a 33 y/o patient. Note the linear band-like enhancement in right breast not conforming to ductal structure; (B) Invasive lobular carcinoma with focal lobular carcinoma in situ in a 43 y/o patient. Note ductal clumped pattern of enhancement in the left breast. (C) Invasive ductal carcinoma with multiple foci of ductal carcinoma in situ along with lymphatic invasion of nipple areolar complex in 55 y/o patient. Note the ductal branching pattern of non mass type enhancement merging towards nipple with skin thickening and enhancement. All arrows indicate lesions.
Ductal enhancement may be linear or linear branching corresponding to one or more ducts, usually radiating towards the nipple, and is suspicious for carcinoma (Figure 6B, 6C).15 Linear enhancement and ductal enhancement cannot always be well separated, and are often used together. Ductal enhancement is considered suspicious for cancer with a positive predictive value (PPV) ranging from 26% to 58.5%.59, 77 It is frequently seen in DCIS, accounting for 20% to 62% of all DCIS.78–79 The differential diagnosis of ductal enhancement may also include atypical ductal hyperplasia, lobular carcinoma in situ and other benign findings.77 Tozaki et al. reported that 50% of benign lesions with a non mass-like enhancement depicted a linear enhancement distribution.78, 80
Segmental enhancement is triangular or cone shaped with apex at nipple, representing involvement of a single branching duct system. Segmental enhancement has a high PPV ranging from 67% to 100% for carcinoma.59, 24, 81 Morakkabati-Spitz et al. reported that segmental or linear enhancement was the most frequent manifestation of DCIS on MRI, and in 17% of patients these features were visible when no abnormality was noted on mammogram. They found that although overall prevalence of a ductal or segmental enhancement on breast MRI is low, this finding has a high specificity of 96% and a moderate positive predictive value of 34% for intraductal neoplastic changes (Figure 7A).82 Liberman et al. also reported that among non-mass lesion, the frequency of carcinoma was highest in segmental enhancement (67% carcinoma) and ‘clumped linear and ductal’ enhancement (31% carcinoma).24 Segmental enhancement may also be occasionally seen in the ILC (Figure 7B, 7C).
Figure 7.

(Left) pre-contrast axial view T1-weighted images, (Right) contrast-enhanced subtraction images. (A) Ductal carcinoma in situ in a 51 y/o patient. Note the segmental clumped pattern of enhancement in the central third aspect of the right breast; (B) Invasive lobular carcinoma in a 50 y/o patient. Note the segmental pattern of the lesion toward the nipple in the left breast; (C) Invasive lobular carcinoma in a 55 y/o patient. Note the spiculated mass in the right breast with linear enhancement extending to the nipple. All arrows indicate lesions.
Regional enhancement involves a broader area not conforming to a ductal distribution, and is not as distinct from the surrounding tissues compared to patterns described previously. Regional enhancement may be geographic or patchy in appearance and lacks convex borders. It may represent normal or pathological change, which is more likely associated with a benign lesion such as fibrocystic changes (Figure 8A). In a small series reported by Van den Bosch et al., fibrocystic changes presented as regional distribution in 6 of 14 (43%) patients.83 Schnall et al., however, reported that regional enhancement had 21% likelihood of cancer.59 It is more often seen in DCIS or ILC, rarely in IDC (Figure 8B).63
Figure 8.

(Left) pre-contrast axial view T1-weighted images, (Right) contrast-enhanced subtraction images. (A) Fibrocystic change in a 31 y/o patient. Note a patch of faint regional enhancement in the right breast; (B) Invasive ductal carcinoma in the left breast in a 51 y/o patient. Note a regional area of clumped enhancement in the left breast. All arrows indicate lesions.
Multiple regions of enhancements refer to at least two or more large volume of tissues not conforming to ductal distribution, and separated by normal tissues or fat. Diffuse enhancement describes widely scattered and evenly distributed enhancements appearing throughout the fibroglandular tissue of the breast. Multiple regions of enhancements and diffuse enhancements are more characteristic of benign proliferative changes. Although multicentric carcinoma, such as IDC or ILC, may also exhibit such appearance, however, these findings are nearly always unilateral (Figure 9A).26, 83–84
Figure 9.

(Left) pre-contrast axial view T1-weighted images, (Right) contrast-enhanced subtraction images. (A) Invasive ductal carcinoma with skin invasion in a 36 y/o patient. Note the diffuse non mass type enhancement of left breast with involvement of skin as evident by skin thickening and bright enhancement; (B) Extensive ductal carcinoma in-situ with multicentric invasive ductal carcinoma in a 49 y/o patient. Note a large regional non-mass type area of clumped enhancement in the right breast; (C) Bilateral fibrocystic changes in a 45 y/o patient. Note symmetrical diffuse enhancement in the both breast. All arrows indicate lesions.
Internal Enhancement Patterns
The various internal enhancement patterns of non-mass-like enhancement can be further described as homogenous, heterogeneous, stippled/punctuate, clumped and reticular/dendritic.15 The specific internal enhancement patterns of non-mass-like enhancement combined with their distribution may contribute to improved diagnosis.
“Homogeneous” enhancement is a confluent, uniform enhancement while “Heterogeneous” enhancement is a non-uniform enhancement in a random pattern, separated by areas of normal breast parenchyma or fat.15
“Stippled/Punctate” enhancement refers to multiple 1–2 mm tiny, dot like, similar appearing enhancing punctuate foci scattered throughout an area of breast not conforming to a duct, and more likely represents normal breast tissues or fibrocystic changes. Among the non-mass-like enhancement patterns, stippled enhancement is most frequently associated with benign lesions and has a 25% incidence of malignancy while homogenous, heterogeneous and clumped enhancement have a higher cancer likelihood of 67%, 53%–69%, and 60%–88%, respectively.59, 80–81
“Clumped” enhancement refers to aggregate of enhancing masses or foci in a cobblestone pattern that may appear confluent; and this pattern is suspicious for DCIS or IDC (Figure 8B, 9B). Liberman et al. showed that MR imaging pattern of clumped enhancement had a PPV of 41% for carcinoma. Among cancers presenting as clumped enhancement, 89% were DCIS. The clumped (beaded) enhancement may represent irregularly heaped-up tumor cells expanding a duct containing DCIS.24
“Reticular/dendritic” enhancement occurs in the breast that has undergone some glandular tissue involution leaving strands of breast tissue among strands of fat.15
Symmetric or Asymmetric Non-mass-like enhancement
Symmetry is helpful for further characterization of non-mass-like enhancement. Symmetric enhancement is mirror image enhancement in both breasts; while asymmetric enhancement refers to enhancement that is more pronounced in one breast compared to the other. Bilateral symmetric non-mass-like enhancement in any distribution is highly suggestive of benign changes (Figure 9C).26
ASSOCIATED FINDINGS
Associated findings include nipple retraction or inversion, pre-contrast high ductal signal, skin retraction, skin thickening, skin invasion, edema, lymphadenopathy, pectoral muscle invasion and chest wall invasion, hematoma/blood, abnormal signal void (clip) artifact, and cyst.15
Paget’s disease shows abnormal asymmetric enhancement of the nipple areolar complex in the involved breast (Figure 10A).85–86 Tumor involvement of the pectoralis major muscles (Figure 10B), and extension of tumor into underlying chest wall is indicated by abnormal enhancement within these structures.87
Figure 10.

(A–C, left) pre-contrast T1 weighted axial view image, (A–C, right) contrast-enhanced subtraction images. (A) Paget’s disease of the left nipple with underlying high grade DCIS in a 62 y/o patient. Contrast-enhanced subtraction image shows an asymmetric enlarged left nipple with strong enhancement, which extends to the sub-areolar area; (B) Invasive ductal carcinoma with pectoris muscle invasion in a 50 y/o patient. Note the enhancement of the tumor and the involved muscle in the left breast; (C) Invasive ductal carcinoma with axillary lymph nodes in a 39 y/o patient. Note several round shape hypointense lymph nodes in the right axillary area. These lymph nodes show strong enhancements; (D) same patient as (C), showing lymph nodes on pre-contrast sagittal view T1-weighted images with a smaller field of view. All arrows indicate lesions.
MRI can detect lymph nodes (Figure 10C and 10D). Intra-mammary lymph nodes are found in 28% of breasts in histological studies of mastectomy specimens,88 whereas their incidence in mammography is only 5%.89 Characteristically these are seen in the upper-outer quadrant of breast on mammogram although 28% of intra-mammary lymph nodes are found in other locations.90 High vascularity of lymph nodes allows them to enhance intensely on breast MRI.46
The criteria to differentiate between metastatic and benign reactive lymph nodes are based on maximum transverse diameter, shape, thickened lobular cortex, displacement and/or absence of fatty hilus. These criteria vary widely and remain controversial.91–94 Luciani et al. reported a significant higher percentage of pathologically positive lymph nodes with short axis greater than 10mm, abnormal irregular contour, central hyperintensity on inversion recovery T2 weighted images and intense enhancement compared to pathologic negative lymph nodes. A few studies have shown ultra-small paramagnetic iron oxide particle (USPIO)-enhanced MRI as a potential diagnostic tool for preoperative nodal staging, with a sensitivity of 73% to 100%.91, 95
KINETIC ENHANCEMENT CURVE ASSESSMENT
The features in the enhancement kinetics curve are defined in two separate phases, and described as ‘slow’, ‘medium’, or ‘fast’ in the initial phase, and ‘persistent’, ‘plateau’ or ‘wash-out’ in the delayed phase. A kinetic curve showing wash-out or plateau after reaching the peak within 2–3 minutes is commonly observed in invasive breast cancer (Figure 11A); while a kinetic curve showing persistent enhancement continuing throughout the entire time period is commonly observed in benign diseases (Figure 11B).15 Bluemke et al, using either plateau (Figure 11C) or washout pattern as an indicator of malignancy, yielded a sensitivity of 63.2% and a specificity of 65.4% while persistent enhancement pattern yielded a diagnostic specificity of 71% for benign lesions.96 The percentage of maximal enhancement compared to pre-contrast signal intensity is, however, not clearly addressed in the ACR BI-RADS lexicon.
Figure 11.

Representative enhancement kinetic curves from three different patients. (A) moderate initial enhancement followed by a persistent enhancement in a fibrocystic change shown in Figure 8A; (B) rapid initial enhancement reaching to a plateau in an invasive lobular cancer shown in Figure 7C; (C) rapid initial enhancement followed by washout in an invasive ductal carcinoma shown in Figure 5D.
ILC with a diffuse growth pattern appearing as a non-mass-like enhancement may exhibit low magnitude and persistent enhancement kinetics (supposedly "benign"), possibly associated with a weak angiogenic activity.26, 84, 97 Hence enhancement kinetics for non-mass-like enhancement should be interpreted with caution and may be used with confidence for differential diagnosis, only in lesions showing rapid enhancement and washout pattern. Similarly the patterns of enhancement kinetics are unreliable for diagnosis of DCIS; only about 70% of DCIS exhibits fast initial enhancement, with variable delayed phase enhancement patterns.26 Schnall et al. reported that readers in a multi-institutional trial described the enhancement kinetics as persistent in 45% of lesions that proved to be cancer, and hence concluded that exclusion of cancer on this basis alone may lead to high false negative rates.59 Therefore, an analysis of both morphology and kinetic curve should be taken in to account in the interpretation.
MRI GUIDED BREAST BIOPSY
No discussion of breast MRI interpretation is complete without mention of MRI-guided biopsy procedures. Because the sensitivity of breast MRI is so high, many suspicious lesions detected by MRI will not have been seen on the mammography and ultrasound examinations, even when these examinations are performed and interpreted with retrospective knowledge of the MRI findings. Some of these can be seen on a second look ultrasound exam specifically directed to the area of MRI concern. However, many MRI-detected lesions may still not be demonstrated with confidence. For these later cases, MRI-directed core biopsy is the only way to perform sampling without excessive tissue removal from a much larger excisional biopsy. Given the relatively low specificity of breast MRI, the ability to perform an MRI-directed core biopsy is a highly desirable component of a breast MRI program. Thus to fulfill the second purpose of BI-RADS, it is necessary to develop equipments and methods for biopsy localization of lesions seen on MRI alone, in order to avoid the unnecessary surgical excisional biopsy due to limited specificity of contrast enhanced MRI.
Breast MRI biopsy is now being developed as part of voluntary ACR breast MRI accreditation program.98 MRI-guided percutaneous biopsy has become possible with the development of special breast biopsy coils.99–104 A vacuum assisted biopsy device106 can extract a larger tissue volume which allow for compensation of tissue shift during needle insertion and reduces the sampling error. It allows the verification of lesion removal by direct visualization on the post MRI biopsy images.105–106
REPORTING SYSTEM
The clinical history of the patient, comparison to old studies, and findings on mammography and ultrasound if available need to be mentioned. MR method used should be described. The type of post processing technique used needs to be mentioned. There should be succinct description of the morphological findings and kinetic enhancement characteristics. The lesion type, size, location, distribution, and associated findings need to be included.
Finally, based on the morphological and kinetic features, overall assessment of the lesion should be given, including category 0 -- need additional imaging evaluation; category 1 – negative findings; category 2 – benign findings; category 3 – probably benign finding – short-interval follow-up suggested; category 4 – suspicious abnormalities-biopsy should be performed; category 5 – highly suggestive of malignancy-appropriate action should be taken; and category 6 – known biopsy-proven malignancy-appropriate action should be taken.15, 107
CONCLUSION
ACR BI-RADS MRI lexicon has clearly defined different morphological and kinetic features of breast lesions shown on MRI. A comprehensive analysis of both morphological and kinetic features based on the common terminology of this lexicon will result in unambiguous MRI reports and facilitate appropriate diagnostic conclusions and clinical management recommendations, and more effective communications between radiologists, clinicians, and patients.
Acknowledgements
This study was supported in part by grants NIH/NCI No. CA90437, CA121568 and the California BCRP No. 9WB-0020.
REFERENCES
- 1.Much wider use of M.R.I.’s urged for breast exam, Health. The New York Times, By Denise Grady Published; 2007. Mar 28, [Google Scholar]
- 2.Saslow D, Boetes C, Burke W, et al. American Cancer Society Breast Cancer Advisory Group. American Cancer Society guidelines for breast screening with MRI as an adjunct to mammography. CA Cancer J Clin. 2007 Mar–Apr;57(2):75–89. doi: 10.3322/canjclin.57.2.75. [DOI] [PubMed] [Google Scholar]
- 3.Tillman GF, Orel SG, Schnall MD, et al. Effect of breast magnetic resonance imaging on the clinical management of women with early-stage breast carcinoma. J Clin Oncol. 2002 Aug 15;20(16):3413–3423. doi: 10.1200/JCO.2002.08.600. [DOI] [PubMed] [Google Scholar]
- 4.Bedrosian I, Mick R, Orel SG, et al. Changes in the surgical management of patients with breast carcinoma based on preoperative magnetic resonance imaging. Cancer. 2003 Aug 1;98(3):468–473. doi: 10.1002/cncr.11490. [DOI] [PubMed] [Google Scholar]
- 5.Hylton N. Magnetic resonance imaging of the breast: opportunities to improve breast cancer management. J Clin Oncol. 2005 Mar 10;23(8):1678–1684. doi: 10.1200/JCO.2005.12.002. [DOI] [PubMed] [Google Scholar]
- 6.Braun M, Pölcher M, Schrading S, et al. Influence of preoperative MRI on the surgical management of patients with operable breast cancer. Breast Cancer Res Treat. 2007 Sep 29; doi: 10.1007/s10549-007-9767-5. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 7.Kuhl CK, Schrading S, Leutner CC, et al. Mammography, breast ultrasound, and magnetic resonance imaging for surveillance of women at high familial risk for breast cancer. J Clin Oncol. 2005 Nov 20;23(33):8469–8476. doi: 10.1200/JCO.2004.00.4960. [DOI] [PubMed] [Google Scholar]
- 8.Lehman CD, Gatsonis C, Kuhl CK, et al. MRI evaluation of the contralateral breast in women with recently diagnosed breast cancer. N Engl J Med. 2007;356:1295–1303. doi: 10.1056/NEJMoa065447. [DOI] [PubMed] [Google Scholar]
- 9.Schelfout K, Van Goethem M, Kersschot E, et al. Contrast-enhanced MR imaging of breast lesions and effect on treatment. Eur J Surg Oncol. 2004;30:501–507. doi: 10.1016/j.ejso.2004.02.003. [DOI] [PubMed] [Google Scholar]
- 10.Zhang Y, Fukatsu H, Naganawa S, et al. The role of contrast-enhanced MR mammography for determining candidates for breast conservation surgery. Breast Cancer. 2002;9:231–239. doi: 10.1007/BF02967595. [DOI] [PubMed] [Google Scholar]
- 11.Esserman L, Hylton N, Yassa L, et al. Utility of magnetic resonance imaging in the management of breast cancer: evidence for improved preoperative staging. J Clin Oncol. 1999;17:110–119. doi: 10.1200/JCO.1999.17.1.110. [DOI] [PubMed] [Google Scholar]
- 12.Beatty JD, Porter BA. Contrast-enhanced breast magnetic resonance imaging: the surgical perspective. Am J Surg. 2007 May;193(5):600–605. doi: 10.1016/j.amjsurg.2007.01.015. [DOI] [PubMed] [Google Scholar]
- 13.Pediconi F, Catalano C, Padula S, et al. Contrast-enhanced magnetic resonance mammography: does it affect surgical decision-making in patients with breast cancer? Breast Cancer Res Treat. 2007 Nov;106(1):65–74. doi: 10.1007/s10549-006-9472-9. [DOI] [PubMed] [Google Scholar]
- 14.Kuhl CK, Schrading S, Bieling HB, et al. MRI for diagnosis of pure ductal carcinoma in situ: a prospective observational study. Lancet. 2007 Aug 11;370(9586):485–492. doi: 10.1016/S0140-6736(07)61232-X. [DOI] [PubMed] [Google Scholar]
- 15.American College of Radiology. Breast imaging reporting and data system (BI-RADS) 4th ed. Reston Va: American College of Radiology; 2003. [Google Scholar]
- 16.Schnall MD, Ikeda DM. Lesion Diagnosis Working Group report. J Magn Reson Imaging. 1999 Dec;10(6):982–990. [PubMed] [Google Scholar]
- 17.Ikeda DM, Baker DR, Daniel BL. Magnetic resonance imaging of breast cancer: clinical indications and breast MRI reporting system. J Magn Reson Imaging. 2000 Dec;12(6):975–983. doi: 10.1002/1522-2586(200012)12:6<975::aid-jmri24>3.0.co;2-y. Review. [DOI] [PubMed] [Google Scholar]
- 18.Morris EA. Breast MR imaging lexicon updated. Magn Reson Imaging Clin N Am. 2006 Aug;14(3):293–303. doi: 10.1016/j.mric.2006.07.001. v. [DOI] [PubMed] [Google Scholar]
- 19.Balleyguier C, Ayadi S, Van Nguyen K, et al. BIRADS classification in mammography. Eur J Radiol. 2007 Feb;61(2):192–194. doi: 10.1016/j.ejrad.2006.08.033. [DOI] [PubMed] [Google Scholar]
- 20.Ikeda DM, Hylton NM, Kinkel K, et al. Development, standardization, and testing of a lexicon for reporting contrast-enhanced breast magnetic resonance imaging studies. J Magn Reson Imaging. 2001 Jun;13(6):889–895. doi: 10.1002/jmri.1127. [DOI] [PubMed] [Google Scholar]
- 21.Schnall MD, Rosten S, Englander S, et al. A combined architectural and kinetic interpretation model for breast MR images. Acad Radiol. 2001 Jul;8(7):591–597. doi: 10.1016/S1076-6332(03)80683-9. [DOI] [PubMed] [Google Scholar]
- 22.Kinkel K, Helbich TH, Esserman LJ, et al. Dynamic high-spatial-resolution MR imaging of suspicious breast lesions: diagnostic criteria and interobserver variability. AJR Am J Roentgenol. 2000 Jul;175(1):35–43. doi: 10.2214/ajr.175.1.1750035. [DOI] [PubMed] [Google Scholar]
- 23.Nunes LW, Schnall MD, Orel SG. Update of breast MR imaging architectural interpretation model. Radiology. 2001 May;219(2):484–494. doi: 10.1148/radiology.219.2.r01ma44484. [DOI] [PubMed] [Google Scholar]
- 24.Liberman L, Morris EA, Lee MJ, et al. Breast lesions detected on MR imaging: features and positive predictive value. AJR Am J Roentgenol. 2002;179(1):171–178. doi: 10.2214/ajr.179.1.1790171. [DOI] [PubMed] [Google Scholar]
- 25.Criteria for significant risk investigations of magnetic resonance diagnostic devices July 14, 2003. [Accessed May 12];U.S. Department of Health and Human Services, Food and Drug Administration Document 793; Supersedes “guidance for magnetic resonance diagnostic devices – criteria for significant risk investigations” (9/29/1997) 2008 Available at ( http://www.fda.gov/cdrh/ode/guidance/793.html).
- 26.Kuhl CK. The current status of breast MR imaging. Part I. choice of technique, image interpretation, diagnostic accuracy, and transfer to clinical practice. Radiology. 2007 Aug;244(2):356–378. doi: 10.1148/radiol.2442051620. Review. [DOI] [PubMed] [Google Scholar]
- 27.Kuhl CK, Jost P, Morakkabati N, et al. Contrast-enhanced MR imaging of the breast at 3.0 and 1.5 T in the same patients: initial experience. Radiology. 2006 Jun;239(3):666–676. doi: 10.1148/radiol.2392050509. [DOI] [PubMed] [Google Scholar]
- 28.Kuhl CK, Kooijman H, Gieseke J, Schild HH. Effect of B1 inhomogeneity on breast MR imaging at 3.0 T. Radiology. 2007 Sep;244(3):929–930. doi: 10.1148/radiol.2443070266. [DOI] [PubMed] [Google Scholar]
- 29.Kuhl CK, Schild HH, Morakkabati N. Dynamic bilateral contrast-enhanced MR imaging of the breast: trade-off between spatial and temporal resolution. Radiology. 2005 Sep;236(3):789–800. doi: 10.1148/radiol.2363040811. [DOI] [PubMed] [Google Scholar]
- 30.Macura KJ, Ouwerkerk R, Jacobs MA, Bluemke DA. Patterns of enhancement on breast MR images: interpretation and imaging pitfalls. Radiographics. 2006 Nov–Dec;26(6):1719–1734. doi: 10.1148/rg.266065025. Review. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Kuhl CK, Mielcareck P, Klaschik S, et al. Dynamic breast MR imaging: are signal intensity time course data useful for differential diagnosis of enhancing lesions? Radiology. 1999 Apr;211(1):101–110. doi: 10.1148/radiology.211.1.r99ap38101. [DOI] [PubMed] [Google Scholar]
- 32.Kaiser WA. Breast magnetic resonance imaging: principles and techniques. Semin Roentgenol. 2007 Oct;42(4):228–235. doi: 10.1053/j.ro.2007.07.003. [DOI] [PubMed] [Google Scholar]
- 33.Wenkel E, Geppert C, Schulz-Wendtland R, et al. Diffusion weighted imaging in breast MRI: comparison of two different pulse sequences. Acad Radiol. 2007 Sep;14(9):1077–1083. doi: 10.1016/j.acra.2007.06.006. [DOI] [PubMed] [Google Scholar]
- 34.Yoshikawa MI, Ohsumi S, Sugata S, et al. Comparison of breast cancer detection by diffusion-weighted magnetic resonance imaging and mammography. Radiat Med. 2007 Jun;25(5):218–223. doi: 10.1007/s11604-007-0128-4. [DOI] [PubMed] [Google Scholar]
- 35.Park MJ, Cha ES, Kang BJ, et al. The role of diffusion-weighted imaging and the apparent diffusion coefficient (ADC) values for breast tumors. Korean J Radiol. 2007 Sep–Oct;8(5):390–396. doi: 10.3348/kjr.2007.8.5.390. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Sinha S, Lucas-Quesada FA, Sinha U, et al. In vivo diffusion-weighted MRI of the breast: potential for lesion characterization. J Magn Reson Imaging. 2002;15:693–704. doi: 10.1002/jmri.10116. [DOI] [PubMed] [Google Scholar]
- 37.Stejskal EO, Tanner JE. Spin diffusion measurements: spin echoes in the presence of a time dependent field gradient. J Chem Phys. 1965;42:288–292. [Google Scholar]
- 38.Woodhams R, Matsunaga K, Iwabuchi K, et al. Diffusion-weighted imaging of malignant breast tumors: the usefulness of apparent diffusion coefficient (ADC) value and ADC map for the detection of malignant breast tumors and evalution of cancer extension. J Comput Assist Tomogr. 2005;29:644–649. doi: 10.1097/01.rct.0000171913.74086.1b. [DOI] [PubMed] [Google Scholar]
- 39.Guo Y, Cai YQ, Cai ZL, et al. Differentiation of clinically benign and malignant breast lesions using diffusion-weighted imaging. J Magn Reson Imaging. 2002;16:172–178. doi: 10.1002/jmri.10140. [DOI] [PubMed] [Google Scholar]
- 40.Kinoshita T, Yashiro N, Ihara N, et al. Diffusion-weighted half-fourier single-shot turbo spin echo imaging in breasr tumors: differentiation of invasive ductal carcinoma from fibroadenoma. J Comput Assist Tomogr. 2002;26:1042–1046. doi: 10.1097/00004728-200211000-00033. [DOI] [PubMed] [Google Scholar]
- 41.Marini C, Iacconi C, Giannelli M, et al. Quantitative diffusion-weighted MR imaging in the differential diagnosis of breast lesion. Eur Radiol. 2007 Oct;17(10):2646–2655. doi: 10.1007/s00330-007-0621-2. [DOI] [PubMed] [Google Scholar]
- 42.Rubesova E, Grell AS, De Maertelaer V, et al. Quantitative diffusion imaging in breast cancer: a clinical prospective study. J Magn Reson Imaging. 2006 Aug;24(2):319–324. doi: 10.1002/jmri.20643. [DOI] [PubMed] [Google Scholar]
- 43.Kuhl CK. Concepts for differential diagnosis in breast MR imaging. Magn Reson Imaging Clin N Am. 2006 Aug;14(3):305–328. doi: 10.1016/j.mric.2006.07.002. Review. [DOI] [PubMed] [Google Scholar]
- 44.Müller-Schimpfle M, Ohmenhaüser K, Stoll P, et al. Menstrual cycle and age: influence on parenchymal contrast medium enhancement in MR imaging of the breast. Radiology. 1997 Apr;203(1):145–149. doi: 10.1148/radiology.203.1.9122383. [DOI] [PubMed] [Google Scholar]
- 45.Kuhl CK, Bieling HB, Gieseke J, et al. Healthy premenopausal breast parenchyma in dynamic contrast-enhanced MR imaging of the breast: normal contrast medium enhancement and cyclical-phase dependency. Radiology. 1997 Apr;203(1):137–144. doi: 10.1148/radiology.203.1.9122382. [DOI] [PubMed] [Google Scholar]
- 46.Morris EA. The Normal Breast. In: Morris EA, Liberman L, editors. Breast MRI Diagnosis and Intervention. 1st ed. Secaucus NJ: Springer-Verlag, Inc; 2005. pp. 23–44. [Google Scholar]
- 47.Buadu LD, Murakami J, Murayama S, et al. Breast lesions: correlation of contrast medium enhancement patterns on MR images with histopathologic findings and tumor angiogenesis. Radiology. 1996 Sep;200(3):639–649. doi: 10.1148/radiology.200.3.8756909. [DOI] [PubMed] [Google Scholar]
- 48.Yasumura K, Ogawa K, Yuasa Y, et al. Dynamic MRI and tumor angiogenesis of breast cancer. Nippon Igaku Hoshasen Gakkai Zasshi. 2000 Jun;60(7):379–388. [PubMed] [Google Scholar]
- 49.Hulka CA, Smith BL, Sgroi DC, et al. Benign and malignant breast lesions: differentiation with echo-planar MR imaging. Radiology. 1995 Oct;197(1):33–38. doi: 10.1148/radiology.197.1.7568850. [DOI] [PubMed] [Google Scholar]
- 50.Tuncbilek N, Unlu E, Karakas HM, et al. Evaluation of tumor angiogenesis with contrast-enhanced dynamic magnetic resonance mammography. Breast J. 2003 Sep–Oct;9(5):403–408. doi: 10.1046/j.1524-4741.2003.09508.x. [DOI] [PubMed] [Google Scholar]
- 51.Narisada H, Aoki T, Sasaguri T, et al. Correlation between numeric gadolinium-enhanced dynamic MRI ratios and prognostic factors and histologic type of breast carcinoma. AJR Am J Roentgenol. 2006 Aug;187(2):297–306. doi: 10.2214/AJR.05.0696. [DOI] [PubMed] [Google Scholar]
- 52.Teifke A, Behr O, Schmidt M, et al. Dynamic MR imaging of breast lesions: correlation with microvessel distribution pattern and histologic characteristics of prognosis. Radiology. 2006 May;239(2):351–360. doi: 10.1148/radiol.2392050205. [DOI] [PubMed] [Google Scholar]
- 53.Oshida K, Nagashima T, Ueda T, et al. Pharmacokinetic analysis of ductal carcinoma in situ of the breast using dynamic MR mammography. Eur Radiol. 2005 Jul;15(7):1353–1360. doi: 10.1007/s00330-005-2661-9. [DOI] [PubMed] [Google Scholar]
- 54.Tse GM, Chaiwun B, Wong KT, et al. Magnetic resonance imaging of breast lesions--a pathologic correlation. Breast Cancer Res Treat. 2007 May;103(1):1–10. doi: 10.1007/s10549-006-9352-3. [DOI] [PubMed] [Google Scholar]
- 55.Matsubayashi R, Matsuo Y, Edakuni G, et al. Breast masses with peripheral rim enhancement on dynamic contrast-enhanced MR images: correlation of MR findings with histologic features and expression of growth factors. Radiology. 2000 Dec;217(3):841–848. doi: 10.1148/radiology.217.3.r00dc07841. [DOI] [PubMed] [Google Scholar]
- 56.Turetschek K, Preda A, Floyd E, et al. MRI monitoring of tumor response following angiogenesis inhibition in an experimental human breast cancer model. Eur J Nucl Med Mol Imaging. 2003 Mar;30(3):448–455. doi: 10.1007/s00259-002-1000-5. [DOI] [PubMed] [Google Scholar]
- 57.Fournier LS, Novikov V, Lucidi V, et al. MR monitoring of cyclooxygenase-2 inhibition of angiogenesis in a human breast cancer model in rats. Radiology. 2007 Apr;243(1):105–111. doi: 10.1148/radiol.2431050658. [DOI] [PubMed] [Google Scholar]
- 58.Wilmes LJ, Pallavicini MG, Fleming LM, et al. AG-013736, a novel inhibitor of VEGF receptor tyrosine kinases, inhibits breast cancer growth and decreases vascular permeability as detected by dynamic contrast-enhanced magnetic resonance imaging. Magn Reson Imaging. 2007 Apr;25(3):319–327. doi: 10.1016/j.mri.2006.09.041. [DOI] [PubMed] [Google Scholar]
- 59.Schnall MD, Blume J, Bluemke DA, et al. Diagnostic Architectural and Dynamic Features at Breast MR Imaging: Multicenter Study. Radiology. 2006 Jan;238(1):42–53. doi: 10.1148/radiol.2381042117. [DOI] [PubMed] [Google Scholar]
- 60.Goto M, Ito H, Akazawa K, et al. Diagnosis of breast tumors by contrast-enhanced MR imaging: comparison between the diagnostic performance of dynamic enhancement patterns and morphologic features. J Magn Reson Imaging. 2007 Jan;25(1):104–112. doi: 10.1002/jmri.20812. [DOI] [PubMed] [Google Scholar]
- 61.Nunes LW, Schnall MD, Orel SG, et al. Breast MR imaging: interpretation model. Radiology. 1997 Mar;202(3):833–841. doi: 10.1148/radiology.202.3.9051042. [DOI] [PubMed] [Google Scholar]
- 62.Nunes LW, Schnall MD, Siegelman ES, et al. Diagnostic performance characteristics of architectural features revealed by high spatial-resolution MR imaging of the breast. AJR Am J Roentgenol. 1997 Aug;169(2):409–415. doi: 10.2214/ajr.169.2.9242744. [DOI] [PubMed] [Google Scholar]
- 63.Nunes LW, Schnall MD, Orel SG, et al. Correlation of lesion appearance and histologic findings for the nodes of a breast MR imaging interpretation model. Radiographics. 1999 Jan–Feb;19(1):79–92. doi: 10.1148/radiographics.19.1.g99ja0379. [DOI] [PubMed] [Google Scholar]
- 64.Tozaki M, Igarashi T, Matsushima S, Fukuda K. High-spatial-resolution MR imaging of focal breast masses: interpretation model based on kinetic and morphological parameters. Radiat Med. 2005 Feb;23(1):43–50. [PubMed] [Google Scholar]
- 65.Hochman MG, Orel SG, Powell CM, et al. Fibroadenomas: MR imaging appearances with radiologic-histopathologic correlation. Radiology. 1997 Jul;204(1):123–129. doi: 10.1148/radiology.204.1.9205233. [DOI] [PubMed] [Google Scholar]
- 66.Tozaki M, Igarashi T, Fukuda K. Positive and negative predictive values of BI-RADS-MRI descriptors for focal breast masses. Magn Reson Med Sci. 2006 Apr;5(1):7–15. doi: 10.2463/mrms.5.7. [DOI] [PubMed] [Google Scholar]
- 67.Orel SG. Staging of suspected breast cancer: effect of MR imaging and MR-guided biopsy. Radiology. 1995 Jul;196(1):115–122. doi: 10.1148/radiology.196.1.7784554. [DOI] [PubMed] [Google Scholar]
- 68.Chen JH, Agrawal G, Feig B, et al. Triple negative breast cancer: MR imaging features in 29 patients. Annals of Oncology. 2007 Dec;18(12):2042–2043. doi: 10.1093/annonc/mdm504. [DOI] [PubMed] [Google Scholar]
- 69.Agrawal G, Chen JH, Baik HM, et al. MR imaging features of breast cancer: a correlation study with HER-2 receptor. Annals of Oncology. 2007 Nov;18(11):1903–1904. doi: 10.1093/annonc/mdm477. [DOI] [PubMed] [Google Scholar]
- 70.Chen JH, Baik HM, Nalcioglu O, Su MY. Estrogen receptor and breast MR imaging features: a correlation study. JMRI. 2008;27:825–833. doi: 10.1002/jmri.21330. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Wurdinger S, Herzog AB, Fischer DR, et al. Differentiation of phyllodes breast tumors from fibroadenomas on MRI. AJR Am J Roentgenol. 2005 Nov;185(5):1317–1321. doi: 10.2214/AJR.04.1620. [DOI] [PubMed] [Google Scholar]
- 72.Onishi M, Furukawa A, Takahashi M, Murata K. A wide variety of dynamic contrast-enhanced MR appearances of breast cancer: Pathologic correlation study. Eur J Radiol. 2008 Feb;65(2):286–292. doi: 10.1016/j.ejrad.2007.04.003. [DOI] [PubMed] [Google Scholar]
- 73.Jinguji M, Kajiya Y, Kamimura K, et al. Rim enhancement of breast cancers on contrast-enhanced MR imaging: relationship with prognostic factors. Breast Cancer. 2006;13(1):64–73. doi: 10.2325/jbcs.13.64. [DOI] [PubMed] [Google Scholar]
- 74.Chen JH, Naclioglu O, Su MY. Fibrocystic change presenting as a focal lesion mimicking breast cancer. JMRI. doi: 10.1002/jmri.21455. In Press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Liberman L, Mason G, Morris EA, Dershaw DD. Does size matter? Positive predictive value of MRI-detected breast lesions as a function of lesion size. AJR Am J Roentgenol. 2006 Feb;186(2):426–430. doi: 10.2214/AJR.04.1707. [DOI] [PubMed] [Google Scholar]
- 76.Chen JH, Liu H, Baek HM, et al. MR imaging of fibrocystic change of the breast. Magnetic Resonance Imaging. doi: 10.1016/j.mri.2008.02.004. In Press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Liberman L, Morris EA, Dershaw DD, et al. Ductal enhancement on MR imaging of the breast. AJR Am J Roentgenol. 2003 Aug;181(2):519–525. doi: 10.2214/ajr.181.2.1810519. [DOI] [PubMed] [Google Scholar]
- 78.Van Goethem M, Schelfout K, Kersschot E, et al. Comparison of MRI features of different grades of DCIS and invasive carcinoma of the breast. JBR-BTR. 2005 Sep–Oct;88(5):225–232. doi: 10.1016/j.clinimag.2006.01.009. [DOI] [PubMed] [Google Scholar]
- 79.Menell JH, Morris EA, Dershaw DD, et al. Determination of the presence and extent of pure ductal carcinoma in situ by mammography and magnetic resonance imaging. Breast J. 2005 Nov–Dec;11(6):382–390. doi: 10.1111/j.1075-122X.2005.00121.x. [DOI] [PubMed] [Google Scholar]
- 80.Tozaki M, Fukuda K. High-spatial-resolution MRI of non-masslike breast lesions: interpretation model based on BI-RADS MRI descriptors. AJR Am J Roentgenol. 2006 Aug;187(2):330–337. doi: 10.2214/ajr.05.0998. [DOI] [PubMed] [Google Scholar]
- 81.Tozaki M, Igarashi T, Fukuda K. Breast MRI using the VIBE sequence: clustered ring enhancement in the differential diagnosis of lesions showing non-masslike enhancement. AJR Am J Roentgenol. 2006 Aug;187(2):313–321. doi: 10.2214/AJR.05.0881. [DOI] [PubMed] [Google Scholar]
- 82.Morakkabati-Spitz N, Leutner C, Schild H, et al. Diagnostic usefulness of segmental and linear enhancement in dynamic breast MRI. Eur Radiol. 2005 Sep;15(9):2010–2017. doi: 10.1007/s00330-005-2755-4. [DOI] [PubMed] [Google Scholar]
- 83.van den Bosch MA, Daniel BL, Mariano MN, et al. Magnetic resonance imaging characteristics of fibrocystic change of the breast. Invest Radiol. 2005 Jul;40(7):436–441. doi: 10.1097/01.rli.0000167123.26334.c8. [DOI] [PubMed] [Google Scholar]
- 84.Qayyum A, Birdwell RL, Daniel BL, et al. MR imaging features of infiltrating lobular carcinoma of the breast: histopathologic correlation. AJR Am J Roentgenol. 2002 May;178(5):1227–1232. doi: 10.2214/ajr.178.5.1781227. [DOI] [PubMed] [Google Scholar]
- 85.Capobianco G, Spaliviero B, Dessole S, et al. Paget's disease of the nipple diagnosed by MRI. Arch Gynecol Obstet. 2006 Aug;274(5):316–318. doi: 10.1007/s00404-006-0160-0. [DOI] [PubMed] [Google Scholar]
- 86.Frei KA, Bonel HM, Pelte MF, et al. Paget disease of the breast: findings at magnetic resonance imaging and histopathologic correlation. Invest Radiol. 2005 Jun;40(6):363–367. doi: 10.1097/01.rli.0000163742.40401.4e. [DOI] [PubMed] [Google Scholar]
- 87.Morris EA, Schwartz LH, Drotman MB, et al. Evaluation of pectoralis major muscle in patients with posterior breast tumors on breast MR images: early experience. Radiology. 2000 Jan;214(1):67–72. doi: 10.1148/radiology.214.1.r00ja1667. [DOI] [PubMed] [Google Scholar]
- 88.Egan RL, McSweeney MB. Intramammary lymph nodes. Cancer. 1983 May 15;51(10):1838–1842. doi: 10.1002/1097-0142(19830515)51:10<1838::aid-cncr2820511014>3.0.co;2-8. [DOI] [PubMed] [Google Scholar]
- 89.Stomper PC, Leibowich S, Meyer JE. The prevalence and distribution of well-circumbscribed nodules on screening mammography: analysis of 1500 mammograms. Breast Dis. 1991;4:197–203. [Google Scholar]
- 90.Svane G, Franzén S. Radiologic appearance of nonpalpable intramammary lymph nodes. Acta Radiol. 1993 Nov;34(6):577–580. [PubMed] [Google Scholar]
- 91.Memarsadeghi M, Riedl CC, Kaneider A, et al. Axillary lymph node metastases in patients with breast carcinomas: assessment with nonenhanced versus uspio-enhanced MR imaging. Radiology. 2006 Nov;241(2):367–377. doi: 10.1148/radiol.2412050693. [DOI] [PubMed] [Google Scholar]
- 92.Kuhl CK. Current status of breast MR imaging. Part 2. clinical applications. Radiology. 2007 Sep;244(3):672–691. doi: 10.1148/radiol.2443051661. Review. [DOI] [PubMed] [Google Scholar]
- 93.Bluemke DA, Gatsonis CA, Chen MH, et al. Magnetic resonance imaging of the breast prior to biopsy. JAMA. 2004 Dec 8;292(22):2735–2742. doi: 10.1001/jama.292.22.2735. [DOI] [PubMed] [Google Scholar]
- 94.Luciani A, Dao TH, Lapeyre M, et al. Simultaneous bilateral breast and high-resolution axillary MRI of patients with breast cancer: preliminary results. AJR Am J Roentgenol. 2004 Apr;182(4):1059–1067. doi: 10.2214/ajr.182.4.1821059. [DOI] [PubMed] [Google Scholar]
- 95.Michel SC, Keller TM, Frohlich JM, et al. Preoperative breast cancer staging: MR imaging of the axilla with ultrasmall superparamagnetic iron oxide enhancement. Radiology. 2002 Nov;225(2):527–536. doi: 10.1148/radiol.2252011605. [DOI] [PubMed] [Google Scholar]
- 96.Bluemke DA, Gatsonis CA, Chen MH, et al. Magnetic resonance imaging of the breast prior to biopsy. JAMA. 2004 Dec 8;292(22):2735–2742. doi: 10.1001/jama.292.22.2735. [DOI] [PubMed] [Google Scholar]
- 97.Szabo BK, Aspelin P, Wiberg MK, Bone B. Dynamic MR imaging of the breast. Analysis of kinetic and morphologic diagnostic criteria. Acta Radiol. 2003;44:379–386. doi: 10.1080/j.1600-0455.2003.00084.x. [DOI] [PubMed] [Google Scholar]
- 98.Orel S. Who should have breast magnetic resonance imaging evaluation? J Clin Oncol. 2008 Feb 10;26(5):703–711. doi: 10.1200/JCO.2007.14.3594. Review. [DOI] [PubMed] [Google Scholar]
- 99.Heywang-Köbrunner SH, Huynh AT, Viehweg P, et al. Prototype breast coil for MR-guided needle localization. J Comput Assist Tomogr. 1994 Nov–Dec;18(6):876–881. doi: 10.1097/00004728-199411000-00006. [DOI] [PubMed] [Google Scholar]
- 100.Orel SG, Schnall MD, Newman RW, et al. MR imaging-guided 9-gauge vacuum-assisted core-needle breast biopsy: initial experience. Radiology. 1994 Oct;193(1):97–102. doi: 10.1148/radiol.2381050050. [DOI] [PubMed] [Google Scholar]
- 101.Kuhl CK, Elevelt A, Leutner CC, et al. Interventional breast MR imaging: clinical use of a stereotactic localization and biopsy device. Radiology. 1997 Sep;204(3):667–675. doi: 10.1148/radiology.204.3.9280242. [DOI] [PubMed] [Google Scholar]
- 102.Liney GP, Tozer DJ, van Hulten HB, et al. Bilateral open breast coil and compatible intervention device. J Magn Reson Imaging. 2000 Dec;12(6):984–990. doi: 10.1002/1522-2586(200012)12:6<984::aid-jmri25>3.0.co;2-x. [DOI] [PubMed] [Google Scholar]
- 103.Daniel BL, Birdwell RL, Black JW, et al. Interactive MR-guided, 14-gauge core-needle biopsy of enhancing lesions in a breast phantom mode. Acad Radiol. 1997 Jul;4(7):508–512. doi: 10.1016/s1076-6332(97)80238-3. [DOI] [PubMed] [Google Scholar]
- 104.Daniel BL, Birdwell RL, Ikeda DM, et al. Breast lesion localization: a freehand, interactive MR imaging-guided technique. Radiology. 1998 May;207(2):455–463. doi: 10.1148/radiology.207.2.9577495. [DOI] [PubMed] [Google Scholar]
- 105.Heywang-Köbrunner SH, Heinig A, Schaumlöffel U, et al. MR-guided percutaneous excisional and incisional biopsy of breast lesions. Eur Radiol. 1999;9(8):1656–1665. doi: 10.1007/s003300050905. [DOI] [PubMed] [Google Scholar]
- 106.Perlet C, Heywang-Kobrunner SH, Heinig A, et al. Magnetic resonance-guided, vacuum-assisted breast biopsy: results from a European multicenter study of 538 lesions. Cancer. 2006 Mar 1;106(5):982–990. doi: 10.1002/cncr.21720. [DOI] [PubMed] [Google Scholar]
- 107.Tardivon AA, Athanasiou A, Thibault F, El Khoury C. Breast imaging and reporting data system (BIRADS) magnetic resonance imaging illustrated cases. Eur J Radiol. 2007 Feb;61(2):216–223. doi: 10.1016/j.ejrad.2006.08.037. [DOI] [PubMed] [Google Scholar]