

Abstract
Retroperitoneal cystic masses pose an important diagnostic and therapeutic challenge. Simple drainage, internal or external, is usually not sufficient. We report a case of a large symptomatic retroperitoneal cyst and its management.
Keywords: Retroperitoneal cyst, Management
Case report
A 37-year-old woman from Cameroon presented with abdominal pain in the right upper quadrant. Computed tomography revealed a 19 × 14 × 14 cm large cyst with important displacement of the liver and the right kidney (Fig. 1A, B). The cyst was in close contact with the inferiorvena cava. The largely calcified cyst wall measured 4–5mm in thickness and showed no contrast enhancement. The cyst had no septa and was filled with a homogeneous fluid with a density of 16 Hounsfield units. Gastroscopy showed no pathology. All laboratory tests were normal, including C-reactive protein, leukocyte count, livervalues, catecholamines and Echinococcus serology. Malaria infection was excluded. Past history revealed no previous surgery or trauma. The differential diagnosis included a liver cyst (e.g. simple liver cyst, sero-negative echinococcosis) as well as a cystic tumour of the right adrenalgland. At laparoscopy, the cyst was easily dissected from the liver and the right adrenal gland (Fig. 2). After draining 1400 ml of muddy brownish fluid, the cyst was completely removed through a 4-cm long infra-umbilical incision. On inspection, the cyst had a smooth outer surface and an inner surface covered with floe-like patchy calcifications (Fig. 3A, B). Frozen sections excluded malignancy. The amylase and lipase values of the extracted fluid were within the normal range. The operation was completed with a laparoscopically performed right adrenalectomy. Definitive histology showed a heavily calcified and fibrotic cyst wall without any epithelial lining. There was no liver, renal, adrenal ormalignant tissue. Cytology of the cyst content revealed notumour cells. Histology of the right adrenal gland was normal. The final diagnosis of a retroperitoneal non-neoplastic non-pancreatic pseudocyst was made. Aetiologically, the cyst most likely resulted from the cystic transformation of a post-traumatic or post-inflammatory retroperitoneal haematoma. The postoperative course was uneventful and the patient remained free of symptomsduring a 2-year follow-up period.
Figure 1.
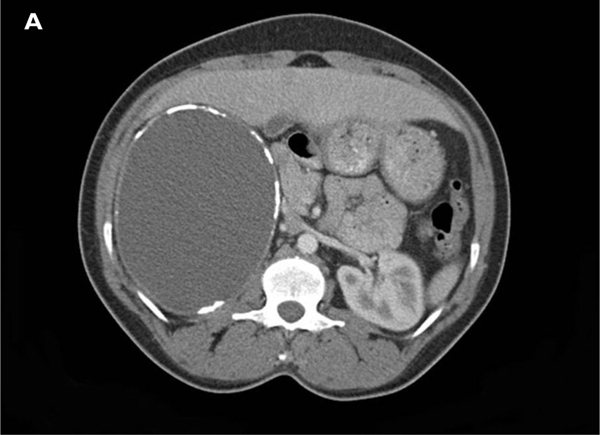
(A,B) CT scans of the retroperitoneal cyst withdisplacement of the liver and the right kidney.
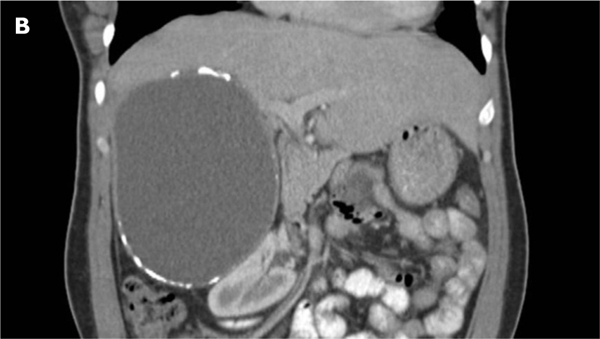
Figure 2.
View during laparoscopy: cyst (left) and liver (right).
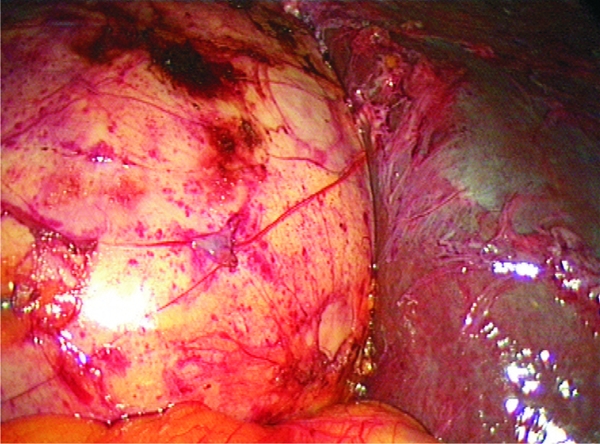
Figure 3.
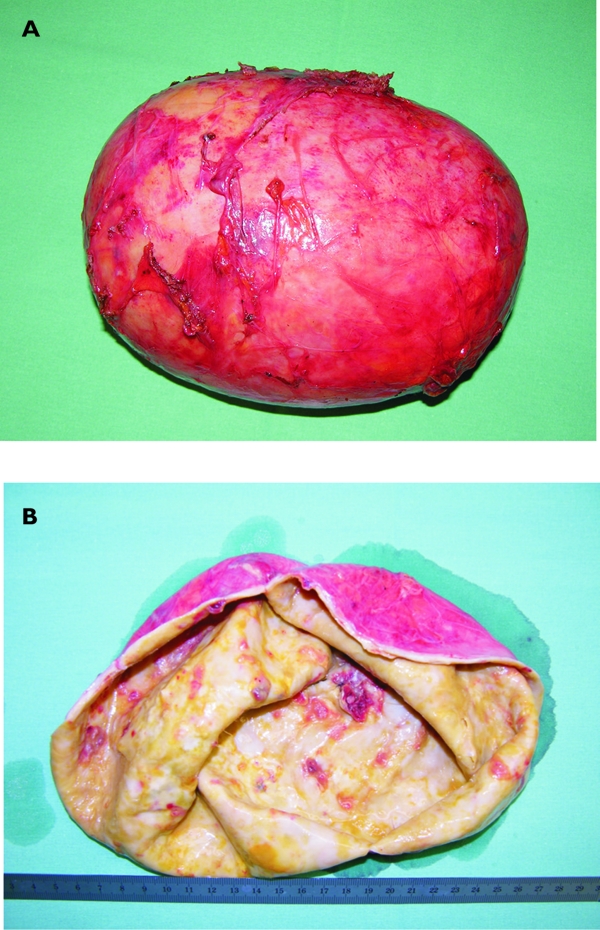
(A,B) Extracted cyst, refilled with water and cut open.
Discussion
Retroperitoneal cystic masses pose an important diagnostic and therapeutic challenge to the treating physician.1–3 The diagnostic work-up includes careful history taking, broad laboratory investigations and, particularly, computed tomography (CT) as well as magnetic resonance imaging (MRI). This approach will help to limit the number of potential diagnoses which otherwise would include a large variety of neoplastic lesions (cystic lymphangioma, mucinous cystadenoma, cystic teratoma, cystic mesothelioma, müllerian cyst,epidermoid cyst, tailgut cyst, bronchogenic cyst, cysticchange in solid neoplasms, pseudomyxoma retroperitonei) and non-neoplastic lesions (pancreaticpseudocyst, non-pancreatic pseudocyst, lymphocoele, urinoma, haematoma).1
Despite the use of the whole diagnostic armamentarium, many cystic lesions cannot be accurately classified. The decision to proceed with surgery is then determined by the presence of symptoms, the concern about future complications (e.g. rupture, infection) and the possibility of malignant change. It is also often driven by the patient's and the surgeon's desire to establish a definite diagnosis,thereby ending a psychologically extremely uncomfortable state of diagnostic uncertainty.
The transabdominal laparoscopic approach is the method of choice providing excellent overview, allowing anatomical evaluation and judgement of resectability, whereas retroperitoneoscopic surgery is limited to small lesions clearly located within the retroperitoneum. Complete excision of the cystic lesion, if feasible, ispreferred over simple fenestration or marsupialisation. An analysis of the cyst content (e.g. chemistry, bacteriology, cytology) and a histology of the cyst wall arealways mandatory. The use of intra-operative frozen sections is advisable, especially if only a partial resection of the cyst is performed.
References
- 1.Yang DM, Jung DH, Kim H, Kang JH, Kim SH, et al. Retroperitoneal cystic masses: CT, clinical, and pathological findingsand literature review. Radiographics. 2004;24:1353–65. doi: 10.1148/rg.245045017. [DOI] [PubMed] [Google Scholar]
- 2.Ros PR, Olmsted WW, Moser RP, Dachman AH, Hjermstad BH. Mesenteric and omental cysts: histologic classification with imagingcorrelation. Radiology. 1987;164:327–32. doi: 10.1148/radiology.164.2.3299483. [DOI] [PubMed] [Google Scholar]
- 3.Martin R, Sanz E, de Vicente E, Ortega P, Labrador E, et al. Differential diagnosis of asymptomatic retroperitoneal cystic lesion: anew case of retroperitoneal bronchogenic cyst. Eur Radiol. 2002;12:949–50. doi: 10.1007/s003300101119. [DOI] [PubMed] [Google Scholar]