

Abstract
Purpose
The purpose of this study was to identify relationships between medical, functional, economic, oral health, social, religious, and psychological factors and under-eating in homebound older adults. The focus of the study was on identifying potentially modifiable factors amenable to social and behavioral interventions.
Design and Methods
A total of 230 homebound older adults who were currently receiving home health services participated in interviews in their homes using a questionnaire to assess eating behaviors and factors that could possibly affect those eating behaviors. Interviewers measured height and weight, and participants completed three 24-hr dietary recalls.
Results
The mean age of participants was 79.1 years. The sample comprised 78% women and 38% African Americans. We found that 70% of participants were under-eating, defined as not consuming enough calories to maintain their current body weight. Participants who were at higher risk of under-eating included men, those receiving either infrequent care or very frequent care by a caregiver, those who had been hospitalized prior to receipt of home health services, and those with a higher body mass index.
Implications
Findings from the study have implications for both practice and policy. Experts must develop evidence-based interventions targeted at under-eating in this particularly vulnerable and growing population of homebound older adults. This study provides an initial foundation for the development of targeted evidence-based behavioral nutritional interventions that are noninvasive and cost effective.
Keywords: Under-eating, Undernutrition, Nutrition policy
Undernutrition in older adults is a well-recognized and serious problem with significant health, economic, and social consequences (DiMaria-Glalili & Amella, 2005; Olde-Rikkert & Riguad, 2003; Wellman & Johnson, 2004). Older adults who are confined to their homes for any number of reasons, including geographic isolation, lack of transportation, functional limitations, or medical conditions, may be at increased risk for experiencing undernutrition. Those who are homebound because of a medical problem and who are receiving formal home health services, about half of whom have been recently hospitalized, may be at even greater risk for experiencing undernutrition because of their already compromised health status (Payette, 2005).
The sequelae of undernutrition in older adults include increased mortality (Payette, Coulombe, Boutier, & Gray-Donald, 1999), functional decline or frailty (Bartali et al., 2006), higher rates of adverse complications from other health conditions (MacIntosh, Morley, & Chapman, 2000), decreased quality of life (Vailas, Nitzke, Becker, & Gast, 1998), and increased health care utilization and costs (Janssen, Shepard, Katzmarzyk, & Roubenoff, 2004; Payette, Coulombe, Boutier, & Gray-Donald, 2000). The consequences of undernutrition in homebound older adults may be especially severe, as inadequate caloric intake may affect the course of illness or, in some instances, be made worse by illness or treatment (Institute of Medicine, 2001).
Numerous researchers have reported on the myriad factors associated with inadequate caloric intake in the general population of older adults, the majority of whom are not homebound. These include reduced social support, cognitive impairment, poor mental health, poverty, lack of access to community resources, low religiosity, poor health, functional impairment, medication usage, and poor oral health (for overall reviews, see Bales & Ritchie, 2005; Davis & Randall, 1989; Elsner, 2002; Wellman & Johnson, 2004). Homebound older adults are likely to experience many of these problems concomitantly, thus compounding their likelihood for experiencing undernutrition. However, despite the growing numbers of homebound older adults, research on this population remains sparse. This is in large part due to the unique ethical and practical challenges involved in studying homebound older adults (Locher, Bronstein, Ritchie, Robinson, & Williams, 2006).
Previous research that has examined prevalence and correlates of poor nutritional intake in homebound older adults has found that inadequate caloric intake is very common (i.e., 71%–93% of individuals; Millen et al., 2001; Millen Posner, Smigelski, & Krachenfels, 1987; Payette, Gray-Donald, Cyr, & Boutier, 1995; Sharkey et al., 2002) and is associated with greater burden of disease, stress, poor appetite, poor vision (Payette et al., 1995), female gender, African American ethnicity, low income, low level of education, skipping breakfast (Sharkey et al., 2002), and multimorbidity (Sharkey, 2003).
Research conducted by the investigative teams of Sharkey and Payette is exceptional in that it has examined multiple factors that simultaneously could affect eating behavior; but these research teams relied upon subsamples of homebound older adults who were already receiving nutritional support within the community—either home-delivered meals or “home help services” (that may have included food preparation services). There is a compelling need to comprehensively assess the full spectrum of factors associated with under-eating in the growing population of homebound older adults—not just in those few who are already receiving food services.
In 2004, 2.8 million older adults received Medicare home health service, and this number is expected to rise (Medicare Payment Advisory Commission, 2006). Fewer older persons with functional impairment are entering nursing homes, and more are choosing to remain in the community (National Center for Health Statistics, 2006). In this population, weight loss has been shown to predict institutionalization and mortality (Payette et al., 2000; Thomas, 2005). Rising health care costs and consumer preferences for aging in place call attention to the need for a better understanding of factors that may contribute to undernutrition in this homebound population and the consequences of undernutrition in order to develop interventions that may prevent costly and unnecessary institutionalization.
The present study was informed by a conceptual model that takes into account the multiple and interrelated factors that may simultaneously contribute to under-eating among homebound older adults (see Figure 1). These factors include medical, functional, economic, oral health, social, religious, and psychological factors. This model draws upon a large body of empirical research that has identified risk factors for undernutrition among older adults in general, and it is being developed for understanding undernutrition in homebound older adults specifically.
Figure 1.
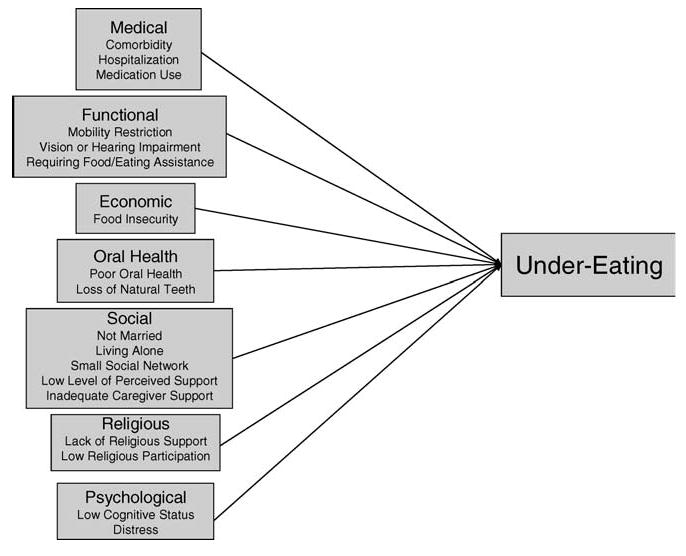
Conceptual model of under-eating.
Particularly relevant to the homebound population are risk factors related to acute or chronic illness and comorbidity, which are common among older adults who have been hospitalized (Sharkey, 2003). Illness and medications associated with their treatment can interfere either with one's desire or ability to eat. Depending upon the level of disability, functional impairments (e.g., mobility restriction, vision loss, or hearing impairment) may further interfere with the ability to purchase, prepare, or eat meals, making persons without physical assistance more vulnerable to undernutrition (Sharkey, 2002). Poverty is a major economic risk factor for poor nutritional intake in older adults when people with limited incomes are not able to afford the food they need or, in the case of many homebound individuals, cannot pay to have food delivered (Lee & Frongillo, 2001). Even when food is available, poor oral health—which leads to difficulty chewing, missing teeth, or oral pain—is especially common among the homebound and may reduce nutrient intake by interfering with the ability to eat (Sahyoun, Lin, & Krall, 2003).
In homebound older adults who are disabled and dependent on others for acquiring, preparing, or consuming their food, social factors assume particular importance. A large body of literature has demonstrated the positive nutritional benefits conferred to older adults who possess adequate social networks and support systems (Davis, Murphy, Neuhaus, Gee, & Quiroga, 2000; Locher, Ritchie, et al., 2005; McIntosh, Shifflett, & Picou, 1989). Additionally, the role of social support may be influenced by gender roles and recent widowhood (McDonald, Quandt, Arcury, Bell, & Vitolins, 2000; Quandt, McDonald, Arcury, Bell, & Vitolins, 2000). For example, older widowers (who have not been socialized to take care of their own nutritional needs) and older widows (who no longer have a spouse to prepare meals for) may be at risk for undernutrition. Various dimensions of religion and spirituality influence nutritional behavior among older adults and may affect the homebound through beliefs about health and lifestyle, or through the social support of being embedded in a religious network system (Locher, Ritchie, et al., 2005; McIntosh & Schifflett, 1984).
Research has also shown that psychological factors, including cognitive impairment and depression, contribute to older adults' experiencing poor eating behaviors and reduced intake (Elsner, 2002; Johnson & Fisher, 2004). Common nutritional problems among older adults with cognitive impairment include forgetting to eat, not knowing how to prepare meals, and simply refusing to eat. Depression is associated with reduced caloric intake among all age groups but may be experienced especially by homebound older adults who experience many changes and losses over a short period of time in the latter years of their life course.
The purpose of this study was to use this multifactorial conceptual model to examine the relationships between under-eating and these potential correlates in a sample of homebound older adults receiving home health care. The focus was on identifying factors that are potentially modifiable by social or behavioral interventions.
Methods
Sample
Participants in this study were 238 homebound older adults receiving home health services because of a recent acute illness or an exacerbation of a chronic condition. To be eligible for receipt of home health services, participants had to be homebound according to Medicare's definition of homebound status:
[An] individual [who] has a condition … that restricts [one's] ability to leave his or her home except with the assistance of another individual or the aid of a supportive devise … or [who] has a condition such that leaving his or her home is medically contraindicated.[42 U.S.C. '1395n(a)(2)(F)] (Center for Medicare Advocacy, Inc., Home Health Care)
Additionally, in order to be eligible for the study participants had to be community dwelling (i.e., residing in their own or someone else's private residence), be able to communicate or have a caregiver who was able to communicate in English, be free of significant cognitive impairment (if living alone, Mini-Mental State Examination Score [MMSE] ≥ 24; if caregiver present, MMSE ≥ 15), be free of terminal illness, not be tube-fed, and not be dependent on a ventilator. We recruited participants from area home health agencies (n = 146), a university-affiliated geriatric medicine outpatient clinic (n = 60), a university-affiliated inpatient rehabilitation facility (n = 27), and area churches (n = 5). All referring agencies were aware of inclusion and exclusion criteria. The University of Alabama at Birmingham Institutional Review Board reviewed and approved the study protocol.
Design
Interviewers visited participants in their homes and administered a questionnaire consisting of items related to medical, functional, economic, oral health, social, religious, and psychological factors that could potentially affect eating behaviors. Interviewers obtained measurements of height and weight from all participants who were able to stand (55% of participants) using a portable digital scale and vertical ruler. For those participants who were unable to stand, self-report of height and weight was obtained. Self-report was based on participant (73%) or caregiver (27%) response. Self-report did not vary according to body mass index [BMI] category (underweight: 44%, normal weight: 40%, overweight: 44%, Class I obesity: 63%, Class II obesity: 56%, and Class III obesity: 46%; Pearson χ2 = 4.872, p = .328).
Also during this visit, participants completed a 24-hr dietary recall while in the home using standard protocols (Witschi, 1990). The 24-hr recall collected all intake, including nutritional supplements. The interviewer inspected refrigerators and kitchen storage spaces to better determine foods actually eaten by participants and the materials in which they were prepared or consumed (i.e., bowls, cups, spoons, etc.). In most instances a caregiver was present during the interview and was able, if necessary, to supplement information provided by the participant. Interviewers contacted participants by telephone two more times over the next 2 weeks to obtain two additional 24-hr dietary recalls, one of which was for a weekend day.
Interviewers were trained in the 24-hr recall using standards consistent with those of the University of Minnesota, where Julie L. Locher and Christine S. Ritchie received formal training. The interviewers conducted recalls using standardized probing questions, two-dimensional food models to estimate portion size, and a multiple-pass methodology.
Measurement
The dependent variable was under-eating, defined as not consuming enough calories to maintain current body weight. We derived this measure by subtracting a participant's estimated energy requirements from their mean daily caloric intake. We calculated estimated energy requirements based upon a formula established by the Institute of Medicine (Panel on Macronutrients, Panel on the Definition of Dietary Fiber, Subcommittee on Upper Reference Levels of Nutrients, Subcommittee on Interpretation and Uses of Dietary Reference Intakes, and Standing Committee on the Scientific Evaluation of Dietary Reference Intakes, 2005) that takes into account height, weight, age, gender, and physical activity level. For women, the estimated energy requirement formula was as follows:
| (1) |
for men, the formula was as follows:
| (2) |
where age was measured in years, weight in kilograms, and height in meters, and a physical activity coefficient of 1 indicated sedentary.
We based the mean daily caloric intake upon the average of the three 24-hr dietary recalls that were collected on all participants and analyzed using Nutrition Data System for Research Software Version 4.05, developed by the Nutrition Coordinating Center, University of Minnesota, Minneapolis, Food and Nutrient Database 33, released July 2002 (Schakel, Sievert, & Buzzard, 1988).
Independent variables included several potential correlates of under-eating, including medical, functional, economic, oral health, social, religious, and psychological factors. We selected all measures, with the exception of items from the Outcome and Assessment Information Set (OASIS; described in “Social Factors”), based upon their psychometric properties, use in older populations, and particular relevance to the research question.
Medical Factors
Medical factors included comorbidities, medications, and hospitalization within the past 6 months. We used the Charlson Comorbidity Index Questionnaire to document comorbid conditions (Charlson, Pompei, Ales, & MacKenzie, 1987; Katz, Chang, Sangha, Fossel, & Bates, 1996). While in the home, the interviewer assessed total medications being taken, total prescription medications being taken, and total nonprescription medications being taken through visual inspection. The interviewer also determined hospitalization by asking participants whether they had been hospitalized prior to their receipt of home health services within the past 6 months (yes, no).
Functional Factors
We assessed functional status generally in terms of mobility restriction and vision or hearing impairment, and specifically in terms of requiring assistance for eating meals, preparing meals, and/or purchasing food. Mobility restriction was measured by a single item indicating whether participants were bed- or chairbound; were able to get out of bed or chair, but do not go out; or go out. Three questions from the OASIS questionnaire assessed participants' physical needs for food and eating assistance, including whether they could independently feed themselves, plan and prepare meals, and shop for their own food.
Economic Factors
We measured economic well-being specific to food and eating using the U.S. Department of Agriculture Abbreviated Six-Item Subset of the U.S. Household Food Security Survey Module Food Security Scale (Anderson, 1990; Bickel, Nord, Price, Hamilton, & Cook, 2000). We categorized participants according to whether the household experienced food security (all members of household having access at all times to enough food for an active healthy life), food insecurity (having limited or uncertain availability of nutritious and safe foods, or limited or uncertain ability to acquire those foods in a socially acceptable way), or hunger (resulting from not being able to afford food).
Oral Health Factors
We assessed oral health status using a modified version of the Oral Health-Related Quality of Life measure (Kressin, 1997) and a physical count of total number of natural teeth.
Social Factors
We used marital status (married or not married), living arrangement (living alone or living with someone), social network size, perceived social support, and caregiver support to assess social factors. We assessed social network size and perceived social support using the Medical Outcomes Study Social Support Survey, which consists of 20 items (Sherbourne & Stewart, 1991). One item assesses total number of close friends and relatives, and 19 five-point Likert items form four subscales: Tangible Support, Affectionate Support, Positive Social Interaction, and Emotional/Informational Support. The interviewer assessed caregiver support by asking participants who provides social support, who is the person who provides lead responsibility for support, and how often support is provided. We obtained these items from OASIS (www.cms.hhs.gov/OASIS/), a comprehensive assessment for home care patients required by Medicare to measure patient outcomes for purposes of outcome-based quality improvements.
Religious Factors
We assessed religiosity and spirituality across three domains using items from the Multidimensional Measurement of Religiousness/Spirituality for Use in Health Research (Fetzer Institute/National Institute on Aging Working Group, 1999). These included Religious Support (both anticipated support and negative interaction with congregation), Private Religious Practices, and Organizational Religiousness (including frequency of organized religious activity).
Psychological Factors
We assessed cognitive status using the MMSE (Folstein, Folstein, McHugh, & Fanjiang, 2001) and measured depression using a scale developed by Mirowsky and Ross (1989). The scale is a modification of the Center for Epidemiological Studies–Depression scale.
Control Variables
We assessed age, gender, ethnicity, and highest level of education by self-report. Additionally, we calculated BMI as weight (in kg) divided by height (in m2) and categorized it according to the National Heart, Lung, and Blood Institute (1998) clinical guidelines for underweight (BMI < 18.5), normal weight (BMI = 18.5–24.9), overweight (BMI = 25.0–29.9), Class I obesity (BMI = 30.0–34.9), Class II obesity (BMI = 35.0–39.9), and Extreme/Class III obesity (BMI > 40).
Statistical Analyses
We used descriptive statistics to characterize the sample. We used chi-square analysis or one-way analyses of variance, where appropriate, to test bivariate associations between the independent variables and under-eating. We performed a binary logistic regression to identify independent factors associated with under-eating. We included in the regression model all variables that reached the p ≤ .05 level of significance in the bivariate analyses.
Results
Of the 238 participants enrolled in the study, 8 participants did not complete the baseline interview and three 24-hr dietary recalls, resulting in a final sample size of 230 participants. Tables 1 and 2 present baseline characteristics of the study sample. The mean age of study participants was 79.1 years. There were 107 White women, 74 African American women, 35 White men, and 14 African American men in the study. No participants reported Hispanic ethnicity. BMIs ranged from 12.7 to 65.2. Although 38.3% of participants had a normal BMI, 7.8% were underweight, 25.2% were overweight, and the rest were obese (Class I, 10.4%; Class II, 9.1%; and Class III, 9.1%). Overall, 70% of participants were under-eating. Table 2 reports on daily caloric intake, estimated energy requirement, and caloric deficiency by BMI category.
Table 1. Baseline Characteristics of the Study Sample (N = 230).
| Variable | M (SD, Range) or % |
|---|---|
| Demographic | |
| Age | 79.1 (8.6, 60–99) |
| Female (%) | 78.7 |
| African American (%) | 38.3 |
| Highest level of education completed (%) | |
| None | 5.7 |
| Elementary or middle school | 32.1 |
| High school, technical, or junior college | 48.3 |
| College or beyond | 13.9 |
| Medical | |
| Charlson Comorbidity Index Questionnaire | 3.56 (2.68, 0–12) |
| Hospitalization prior to home health use (%) | 54.8 |
| Total all medications | 9.6 (4.5, 1–29) |
| Functional (%) | |
| Bed- or chairbound | 21.3 |
| Able to feed self meals and snacks independently | 80.0 |
| Able to plan and prepare light meals or reheat delivered meals | 53.5 |
| Able to shop | 5.7 |
| Normal vision | 83.5 |
| No hearing impairment | 82.2 |
| Economic (%) | |
| Food insecurea | 7.8 |
| Oral Health | |
| Oral Health-Related Quality of Life | 1.17 (1.17, 0–9) |
| Social | |
| Married (%) | 29.6 |
| Lives alone (%) | 31.7 |
| Social network size/number of close friends and relatives | 5.8 (4.0, 1–25) |
| Medical Outcomes Study Social Support Survey | 4.26 (0.91, 1.5–5) |
| Tangible Support Subscale | 4.44 (0.85, 1.25–5) |
| Who takes lead responsibility for providing or managing care (%) | |
| Self | 36.5 |
| No single person | 9.6 |
| Spouse or significant other | 16.5 |
| Daughter | 23.5 |
| Son | 7.8 |
| Other family member | 5.7 |
| How often support is provided by primary caregiver (%) | |
| Several times during day and night | 41.7 |
| Once daily | 13.9 |
| One to three times per week | 7.8 |
| Provides own care | 36.5 |
| Receipt of home-delivered meals | 5.2 |
| Religious | |
| Religious Support Scale | 6.49 (2.35, 4–16) |
| Private Religious Practices Scale | 3.99 (2.52, 2–11) |
| Organizational religiousness (%) | |
| More than once a week or every week | 8.7 |
| Once or twice a month or every month or so | 26.1 |
| Once or twice a year | 18.3 |
| Never | 46.5 |
| Psychological | |
| Mini-Mental State Examination | 26.68 (3.70, 15–30) |
| Depression | 2.80 (1.79, 0–6.29) |
Notes: SD = standard deviation.
According to the U.S. Department of Agriculture U.S. Household Food Security Survey Module Food Security Scale.
Table 2. Daily Caloric Intake, Estimated Energy Requirement (EER), and Caloric Deficiency.
| Variable | M (SD) | Min | Max |
|---|---|---|---|
| Daily caloric intake | |||
| Underweight | 1,573 (378) | 1,005 | 2,273 |
| Normal weight | 1,538 (549) | 638 | 3,006 |
| Overweight | 1,504 (402) | 685 | 2,336 |
| Obese Class I | 1,488 (442) | 861 | 2,356 |
| Obese Class II | 1,438 (547) | 230 | 2,485 |
| Obese Class III | 1,344 (364) | 754 | 1,972 |
| All participants | 1,500 (476) | 230 | 3,006 |
| EER | |||
| Underweight | 1,420 (191) | 1,204 | 1,978 |
| Normal weight | 1,653 (272) | 1,281 | 2,344 |
| Overweight | 1,819 (311) | 1,451 | 2,543 |
| Obese Class I | 1,940 (368) | 1,538 | 2,851 |
| Obese Class II | 2,021 (256) | 1,637 | 2,851 |
| Obese Class III | 2,267 (448) | 1,743 | 3,850 |
| All participants | 1,798 (371) | 1,204 | 3,850 |
| EER minus daily caloric intake | |||
| Underweight | 174 (367) | −434 | 841 |
| Normal weight | −115 (568) | −1,312 | 1,230 |
| Overweight | −314 (491) | −1,538 | 570 |
| Obese Class I | −452 (536) | −1,284 | 659 |
| Obese Class II | −584 (583) | −1,620 | 849 |
| Obese Class III | −923 (448) | −2,208 | −111 |
| All participants | −297 (587) | −2,208 | 1,230 |
Note: SD = standard deviation.
Table 3 presents results of the statistically significant bivariate relationships between the independent variables and under-eating. Under-eating was associated with several variables, including younger age, male gender, African American ethnicity, lower level of education, being hospitalized prior to receipt of home health services, lower Tangible Support Subscale score, not having a daughter or other female family member as the primary caregiver, not having care provided once daily, engaging in more private religious practices, and higher BMI.
Table 3. Factors Associated With Under-Eating in Bivariate Models.
| M or % | ||
|---|---|---|
| Variable | Under-Eating | Not Under-Eating |
| Demographic | ||
| Age | 78.34 | 80.80 |
| Gender (%) | ||
| Female | 66.1 | 33.9 |
| Male | 83.7 | 16.3 |
| Ethnicity (%) | ||
| African American | 79.3 | 20.7 |
| White | 64.1 | 35.9 |
| Highest level of education completed (%) | ||
| None | 69.2 | 30.8 |
| Elementary school | 70.0 | 30.0 |
| Middle school | 68.3 | 31.7 |
| High school | 78.7 | 21.3 |
| Technical or junior college | 70.6 | 29.5 |
| College | 39.1 | 60.9 |
| Graduate or professional | 66.7 | 33.3 |
| Medical | ||
| Hospitalization prior to home health use (%) | ||
| Yes | 75.2 | 24.8 |
| No | 63.5 | 36.5 |
| Social | ||
| Medical Outcomes Study Social Support | ||
| Survey/Tangible Support Subscale | 4.34 | 4.64 |
| Who takes responsibility for providing care (%) | ||
| Self | 71.4 | 28.6 |
| No single person | 86.4 | 13.6 |
| Spouse or significant other | 81.6 | 18.4 |
| Daughter | 52.8 | 47.2 |
| Son | 77.8 | 22.2 |
| Other family member | 61.5 | 38.5 |
| Paid help | 0.0 | 100.0 |
| How often is support provided by caregiver (%) | ||
| Several times during day and night | 74.7 | 25.3 |
| Once daily | 40.6 | 59.4 |
| One to three times per week | 88.9 | 11.1 |
| Every week or more often | 78.6 | 21.4 |
| Once or twice a month | 64.5 | 35.5 |
| Every month or so | 82.1 | 17.9 |
| Once or twice a year | 76.2 | 23.8 |
| Never | 65.4 | 34.6 |
| Religious | ||
| Private Religious Practices Scale | 3.7 | 4.7 |
| Body mass index (%) | ||
| Underweight | 29.4 | 70.6 |
| Normal weight | 61.4 | 38.6 |
| Overweight | 74.1 | 25.9 |
| Obese Class I | 79.2 | 20.8 |
| Obese Class II | 85.7 | 14.3 |
| Obese Class III | 100.0 | 0.0 |
Note: All are significant at p ≤ .05.
Because primary caregiver and frequency of care were significantly related to one another (p < .001), we chose to include in the binary logistic regression model only the frequency with which the primary caregiver provided support. Of note, a daughter was the most frequent provider of care for persons who were receiving care either several times during the day and night or once daily.
Table 4 presents the results of the model. The findings revealed that the odds of under-eating were greater for men compared with women; for those receiving infrequent care (one to three times per week) compared with daily or more frequent care; and for those receiving frequent care several times during the day and night compared with those receiving care once daily. Additionally, odds of under-eating were higher for those who had been hospitalized prior to receipt of home health services compared with those who had not been, and for all BMI categories compared with those who were underweight.
Table 4. Logistic Regression Model for Under-Eating.
| Variable | Odds Ratio | b | χ2 | p | 95% Confidence Interval |
|---|---|---|---|---|---|
| Age | 1.001 | 0.001 | 0.002 | .961 | 0.959–1.045 |
| Education | 0.854 | −0.157 | 1.323 | .250 | 0.654–1.117 |
| Male gender | 4.022 | 1.392 | 8.056 | .005 | 1.538–10.516 |
| African American ethnicity | 1.560 | 0.445 | 1.192 | .275 | 0.702–3.469 |
| Frequency of carea | |||||
| Once daily | 0.287 | −1.247 | 5.677 | .017 | 0.103–0.802 |
| One to three times per week | 6.688 | 1.900 | 4.064 | .044 | 1.054–42.421 |
| Self provides care | 0.901 | −0.105 | 0.067 | .796 | 0.407–1.991 |
| Private Religious Practices Scale | 0.889 | −0.117 | 2.493 | .114 | 0.769–1.029 |
| Prior hospitalization | 2.081 | 0.733 | 4.050 | .044 | 1.019–4.248 |
| Body mass index categoryb | |||||
| Normal weight | 5.810 | 1.760 | 6.303 | .012 | 1.471–22.950 |
| Overweight | 9.773 | 2.280 | 10.032 | .002 | 2.384–40.060 |
| Obese Class I | 10.423 | 2.344 | 7.744 | .005 | 2.000–54.321 |
| Obese Class II and III | 48.069 | 3.873 | 18.662 | .000 | 8.295–278.566 |
Several times during day and night is the reference.
Underweight is the reference.
Discussion
Seventy percent of homebound older adults in our study were not consuming enough calories to maintain their current body weight. Other studies have reported similarly high rates of inadequate nutrient intake in this population (Millen et al., 2001; Millen Posner et al., 1987; Payette et al., 1995; Sharkey et al., 2002). Many of the reasons for under-eating may be responsive to intervention (Payette, 2005; Payette & Shatenstein, 2005).
Participants who reported receiving care once daily were less likely to under-eat compared with those who received care either more or less often. Most of the care that was provided once daily was provided by either daughters or other female relatives. Participants who were receiving care more frequently may have been under-eating for health-related reasons. This explanation, however, was not borne out in our bivariate analyses examining either medical or functional factors. Another plausible explanation relates to the health and functional well-being of the caregiver, who in many instances was the spouse. Oftentimes, the spousal caregiver was as sick or dependent as the participant.
Most of the once-daily support that was provided to participants was related to delivery or preparation of a meal. In many instances, this involved caregivers who did not live in the same household, most frequently daughters, actually sitting down and eating meals together with the care recipient. Previous work using detailed dietary records of this sample indicated that the presence of others during meals, and not the presence of others in the household, is a significant predictor of caloric intake (Locher, Robinson, Roth, Ritchie, & Burgio, 2005). McIntosh and colleagues (1989) similarly found that having either companionship at mealtime or help from relatives or friends in preparing meals, but not marital status, was associated with greater caloric intake. Although having someone present in the household does increase the natural opportunities for dining together, it does not mean that household members are doing so; frequently, they are not. Intake may be increased because the duration of the meal is increased due to social facilitation, care recipients may want to please caregivers, or caregivers may monitor or assist with eating (de Castro & Stroebele, 2002).
These findings support the recommendation that caregivers (including family members, volunteers, or paid help), whether inside or outside the home, simply sit down and eat with the person who is at risk for under-eating. Unfortunately, many homebound older persons may not have a caregiver who is in close enough proximity to make this a practical option (MetLife Mature Market Institute, 2004). In fact, despite having some type of support in the community, 36.5% of participants reported that they assume day-to-day primary care for themselves. Homebound older adults, particularly those who live alone, those who do not have a caregiver who lives nearby, and those who are unable to travel, may be able to take advantage of technologies that allow them to engage in some form of “virtual family dining”—whether it is the telephone, a Web-cam, or some other more sophisticated device (Babwin, 2006).
Our research also found that persons who were hospitalized prior to receiving home health services were more likely to under-eat than those who were not hospitalized. This supports the findings of Sullivan, Liu, Roberson, Bopp, and Rees (2004) related to weight loss and mortality being associated with a recent hospitalization. Several factors may explain this association, including the likelihood that persons who were recently hospitalized may be sicker and/or more frail than those who were not. This may be true, but, similar to the association between under-eating and frequency of receipt of care, such an explanation should be evident in relationships between under-eating and medical or functional variables, and we did not find these relationships in our bivariate analyses.
Another plausible explanation is suggested by the findings of Xia and McCutcheon (2006) from Australian hospitals and Kayser-Jones (1997) from nursing homes. These researchers reported that many older adults do not receive needed assistance during meals, disruptions occur frequently, social interaction is neglected, and the eating environment and food are either unpleasant or unfamiliar. Thus, social disruption of routine and “normal” eating habits often occurs during hospitalization and may result in a failure to resume normal eating patterns upon return to home. Previous research has demonstrated the effect that aging has on body energy regulation, such that older adults are especially vulnerable to periods of under-eating—regardless of the circumstances(s) for that under-eating (MacIntosh et al., 2000). One influential experimental study of healthy men found that older participants in contrast to younger ones did not resume prior normal eating habits and did not regain weight they had lost following a period of voluntary under-eating (Roberts et al., 1994).
These findings suggest that interventions designed to increase caloric intake be targeted to hospitalized older adults and include post-discharge planning and subsequent case management. The majority of older adults (96%) receive their primary health insurance from Medicare. The Institute of Medicine (2001) report The Role of Nutrition in Maintaining Health in the Nation's Elderly concluded that because of Medicare's emphasis on acute care and its use of a prospective payment system for both hospital stays and home health care, many patients who may be in need of nutritional services either do not receive them or receive inadequate services. The Administration on Aging and Meals on Wheels Association of America are currently supporting six demonstration projects that focus on connecting older adults who are being discharged from the hospital into the community to nutrition services that are available to them (www.connecttowellness.org/).
A major provision of the Medicare Prescription Drug, Improvement, and Modernization Act of 2003 authorized the establishment of a Chronic Care Improvement Program (now called Medicare Health Support; www.cms.hhs.gov/CCIP/). The goal of the program is to develop individualized, goal-oriented care management plans for beneficiaries with chronic illnesses, including those who are homebound. One particular area of care management includes “self care education for the beneficiary (through approaches such as medical nutrition therapy) and education for primary caregivers and family members” delivered by a registered dietician or nutrition professional (Smith, 2004, p. 735). It is the intent of the law that such nutrition care plans be grounded in evidence-based guidelines. Evidence-based guidelines involve a conscious effort to use the best available research findings in making decisions regarding delivery of health services; they are important generally in behavioral health practices for older adults and, specifically, for those involving nutritional behaviors (Levkoff, Chen, Fisher, & McIntyre, 2006; Sahyoun, Pratt, & Anderson, 2004). Unfortunately, such evidence-based guidelines for treating undernutrition in older adults are virtually nonexistent, and there is little time to establish such guidelines because the program is expected to be fully implemented in 2009.
In the present study, men were much more likely to be under-eating than women. Previous work has similarly demonstrated that community-dwelling older men, especially those who are living alone, widowed, and/or African American, are at increased risk for undernutrition (Locher, Ritchie, et al., 2005; McDonald et al., 2000). Many older men were not socialized to be responsible for food-related activities. Older men are also less likely to participate actively in social networks, such as religious organizations, that might offer nutritional support. Men's knowledge of and experiences with food and eating are quite different than those of women, and these differences may be most deleterious to men when they are sick and when they are old and alone. In contrast, other researchers have found older women, including those who are homebound, to be at greater nutritional risk—especially those who are socially isolated, without transportation, and with limited finances (Sharkey et al., 2002). Homebound older adults, including those who are homebound because of health-related reasons, are a heterogeneous group, and experts must take these differences into account when developing programs. Specifically, where appropriate, experts should take gender and ethnic differences into account in designing and implementing programs (Sharkey & Schoenberg, 2005).
Last, we found that the higher a participant's BMI, the greater the odds of under-eating. This finding highlights the paradoxical observation that it is possible to be both overnourished based upon one measure of nutritional status (i.e., BMI) and undernourished based upon another measure (i.e., caloric intake). Overweight and obese older adults face a significant threat of developing sarcopenic obesity, particularly when they lose weight because of the onset of acute or chronic illness (Roubenoff, 2004; Villareal, Banks, Sienerc, Sinacore, & Klein, 2004). When older adults lose weight through decreased caloric intake and without the benefit of weight-bearing exercise, they are at increased risk for losing lean muscle mass as opposed to fat. Loss of lean muscle mass in this population could contribute to significant functional decline. As pointed out by Roubenoff, overweight and obese older adults who lose weight, particularly lean muscle mass, do not represent the stereotypical frail elder, but they do represent an important and growing public health threat that will be associated with tremendous health care needs and costs.
This study was limited by its relatively small sample size and its reliance on measures of self-report for dietary intake and, for some participants, height and weight. Use of self-report measures, particularly for overweight or obese participants, may have led to overestimates of under-eating in our sample. Future studies might include doubly labeled water or other techniques that measure energy expenditure as a means to validate self-report of under-eating in this population (Schoeller, 1999; St-Onge, Mignault, Allison, & Rabasa-Lhoret, 2007; Trabuisi & Schoeller, 2001). An additional limitation of our study is that we did not include any measures of body composition or fluid status. Therefore, we do not know the relative contributions of fat, muscle, or fluid to overall weight. Future studies might assess these measures as well.
Despite these shortcomings, we were able to identify factors associated with under-eating and the fact that a significant proportion of homebound older adults were not consuming enough calories to maintain their current body weight. What the implications of under-eating are for this population and, particularly, for those who are overweight or obese are not well known. Sharkey (2004) found that homebound men and women with poor nutrient intake, regardless of BMI, have the lowest level of lower extremity physical performance. Recent reports from the University of Alabama at Birmingham Longitudinal Study of Aging have found that unintentional weight loss, but not intentional weight loss, predicts declines in function and life space mobility and mortality across all BMI groups (Locher et al., 2007; Ritchie et al., 2008). These findings by Sharkey and investigators from the University of Alabama at Birmingham suggest that prevention of unintentional weight loss, including for those who are overweight or obese, may be beneficial in the prevention or restoration of function disability. Future studies, including our own ongoing longitudinal follow-up of this sample, might investigate further the effects of under-eating across all BMI categories on weight loss, health outcomes, and health service utilization.
Other investigators have similarly identified potentially modifiable risk factors for undernutrition and opportunities for intervention in homebound older adults (Millen et al., 2001; Millen Posner et al., 1987; Payette et al., 1995; Sharkey et al., 2002). As noted by several authors, it is important that interventions targeted at under-eating in this particularly vulnerable and growing population of homebound older adults be developed that are based on careful observational findings and that are consistent with what is appropriate for this population (Alibhai, Greenwood, & Payette, 2005; DiMaria-Glalili & Amella, 2005; Olde-Rikkert & Riguad, 2003; Well-man & Johnson, 2004). The current study provides an initial foundation for the development of evidence-based interventions for homebound older adults at risk for under-eating.
Acknowledgments
This work was supported by Grant K01 AG00994 from the National Institute on Aging (“Eating Behaviors in Homebound Older Adults”) to Julie L. Locher. Additional support was provided by Public Health Service Research Grant M01-RR00032 from the National Center for Research Resources to the University of Alabama at Birmingham Pittman General Clinical Research Center.
We thank especially Alacare Home Health and Hospice, HomeCare Plus, the William Clifford and Margaret Spain McDonald Clinic, and Drs. Andrew S. Duxbury and Victor W. Mark for referral of study participants. We also thank Drs. Melissa M. Galvin, Douglas C. Heimburger, Mark E. LaGory, and Laura I. Vailas for mentoring activities associated with this K-Award. Last, we thank J. Lynn Shanks and J. Lisa Harvey for interviewing and collecting data and Dr. Jeannine C. Lawrence for assisting with the management of the Nutrition Data System for Research data.
References
- Alibhai SMH, Greenwood C, Payette H. An approach to the management of unintentional weight loss in elderly people. Canadian Medical Association Journal. 2005;172:773–780. doi: 10.1503/cmaj.1031527. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Anderson SA. Core indicators of nutritional state for difficult-to-sample populations. Journal of Nutrition. 1990;120:1557–1600. doi: 10.1093/jn/120.suppl_11.1555. [DOI] [PubMed] [Google Scholar]
- Babwin D. Company develops virtual meal technology. 2006 Retrieved April 6, 2007, from www.usatoday.com/tech/news/techinnovations/2006-12-25-virtual-dinner_x.htm.
- Bales CW, Ritchie CS. Nutritional needs and assessment during the life cycle: The elderly. In: Shils ME, editor. Modern nutrition in health and disease. 10th. Philadelphia: Lippincott Williams & Wilkins; 2005. pp. 843–858. [Google Scholar]
- Bartali B, Frongillo EA, Bandinelli S, Lauretani F, Semba RD, Fried LP, et al. Low nutrient intake is an essential component of frailty in older persons. Journal of Gerontology: Medical Sciences. 2006;61A:589–593. doi: 10.1093/gerona/61.6.589. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bickel G, Nord M, Price C, Hamilton W, Cook J. Measuring food security in the United States: Guide to measuring household food security, rev 2000. Washington, DC: U.S. Department of Agriculture Office of Analysis, Nutrition, and Evaluation; 2000. [Google Scholar]
- Center for Medicare Advocacy, Inc. Home Health Care. Retrieved March 26, 2008 from http://www.medicareadvocacy.org/FAQ_HomeHealth.htm.
- Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. Journal of Chronic Disease. 1987;40:373–383. doi: 10.1016/0021-9681(87)90171-8. [DOI] [PubMed] [Google Scholar]
- Davis MA, Murphy SP, Neuhaus JM, Gee L, Quiroga SS. Living arrangements affect dietary quality for US adults aged 50 years and older: NHANES III 1988–1994. Journal of Nutrition. 2000;130:2256–2264. doi: 10.1093/jn/130.9.2256. [DOI] [PubMed] [Google Scholar]
- Davis MA, Randall E. Social change and food habits of the elderly. In: Riley MW, Hess BB, Bonds K, editors. Aging in society: Selected reviews of recent research. Hillsdale, NJ: Erlbaum; 1989. pp. 1199–1217. [Google Scholar]
- de Castro JM, Stroebele N. Food intake in the real world: Implications for nutrition and aging. In: Thomas D, editor. Undernutrition in older adults: Clinics in geriatric medicine. Philadelphia: W. B. Saunders; 2002. pp. 685–697. [DOI] [PubMed] [Google Scholar]
- DiMaria-Glalili RA, Amella E. Nutrition in older adults: Interventions and assessment can help curb the growing threat of malnutrition. American Journal of Nursing. 2005;105:40–50. doi: 10.1097/00000446-200503000-00020. [DOI] [PubMed] [Google Scholar]
- Elsner RJF. Changes in eating behavior during the aging process. Eating Behaviors. 2002;3:15–43. doi: 10.1016/s1471-0153(01)00041-1. [DOI] [PubMed] [Google Scholar]
- Fetzer Institute/National Institute on Aging Working Group. Multidimensional Measurement of Religiousness/Spirituality for Use in Health Research: A report of the Fetzer Institute/National Institute on Aging Working Group. Kalamazoo, MI: Fetzer Institute; 1999. [Google Scholar]
- Folstein MF, Folstein SE, McHugh PR, Fanjiang G. Mini-Mental State Examination user's guide. Odessa, FL: Psychological Assessment Resources; 2001. [Google Scholar]
- Institute of Medicine, Committee on Nutritional Services for Medicare Beneficiaries. The role of nutrition in maintaining health in the nation's elderly: Interventions and assessments can help beneficiaries. Washington, DC: National Academy Press; 2001. [Google Scholar]
- Janssen I, Shepard DS, Katzmarzyk PT, Roubenoff R. The healthcare costs of sarcopenia in the United States. Journal of the American Geriatrics Society. 2004;52:80–85. doi: 10.1111/j.1532-5415.2004.52014.x. [DOI] [PubMed] [Google Scholar]
- Johnson MA, Fisher JG. Eating and appetite: Common problems and practical remedies. Generations. 2004;28(3):11–17. [Google Scholar]
- Katz JN, Chang LC, Sangha O, Fossel AH, Bates DW. Can comorbidity be measured by questionnaire rather than medical record review? Medical Care. 1996;34:73–84. doi: 10.1097/00005650-199601000-00006. [DOI] [PubMed] [Google Scholar]
- Kayser-Jones J. Inadequate staffing at mealtime: Implications for nursing and health policy. Journal of Gerontological Nursing. 1997;23(8):14–21. doi: 10.3928/0098-9134-19970801-07. [DOI] [PubMed] [Google Scholar]
- Kressin NR. The Oral Health-Related Quality of Life Measure (OHQOL) In: Slade GD, editor. Measuring oral health and quality of life. Chapel Hill: University of North Carolina Press; 1997. pp. 113–119. [Google Scholar]
- Lee JS, Frongillo EA. Nutritional and health consequences are associated with food insecurity among US elderly persons. Journal of Nutrition. 2001;131:1503–1509. doi: 10.1093/jn/131.5.1503. [DOI] [PubMed] [Google Scholar]
- Levkoff SE, Chen H, Fisher JE, McIntyre JS. Evidence-based behavioral health practices for older adults. New York: Springer; 2006. [Google Scholar]
- Locher JL, Bronstein J, Ritchie CS, Robinson CO, Williams C. Ethical issues involving research conducted in the home with homebound older adults: Therapeutic misconception and role conflict. The Gerontologist. 2006;4:160–164. doi: 10.1093/geront/46.2.160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Locher JL, Ritchie CS, Roth DL, Baker PS, Bodner EV, Allman RM. Social isolation, support, and capital and nutritional risk in an older sample: Ethnic and gender differences. Social Science & Medicine. 2005;60:747–761. doi: 10.1016/j.socscimed.2004.06.023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Locher JL, Robinson CO, Roth DL, Ritchie CS, Burgio KL. The effect of the presence of others on caloric intake in homebound older adults. Journal of Gerontology: Medical Sciences. 2005;60A:1475–1478. doi: 10.1093/gerona/60.11.1475. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Locher JL, Roth DL, Ritchie CS, Cox K, Sawyer P, Bodner EV, et al. Body mass index, weight loss, and mortality in community-dwelling older adults. Journal of Gerontology: Medical Sciences. 2007;62(12):1389–92. doi: 10.1093/gerona/62.12.1389. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MacIntosh C, Morley JE, Chapman IM. The anorexia of aging. Nutrition. 2000;16:983–995. doi: 10.1016/s0899-9007(00)00405-6. [DOI] [PubMed] [Google Scholar]
- McDonald J, Quandt SA, Arcury TA, Bell RA, Vitolins MZ. Nutritional self-management strategies of rural widowers. The Gerontologist. 2000;40:480–491. doi: 10.1093/geront/40.4.480. [DOI] [PubMed] [Google Scholar]
- McIntosh WA, Shifflett PA, Picou SJ. Social support, stressful events, strain, dietary intake, and the elderly. Medical Care. 1989;27:140–153. doi: 10.1097/00005650-198902000-00005. [DOI] [PubMed] [Google Scholar]
- Medicare Payment Advisory Commission. Report to the Congress: Medicare payment policy. 2006 March; Retrieved September 26, 2006 from www.cms.hhs.gov/CCIP/
- MetLife Mature Market Institute. Miles away: The MetLife Study of Long-Distance Caregiving. 2004 Retrieved March 1, 2007 from www.caregiving.org/data/milesaway.pdf.
- Millen BE, Silliman RA, Cantey-Kiser J, Copenhafer DL, Ewart CV, Ritchie CS, et al. Nutritional risk in an urban homebound older population: The Nutrition and Healthy Aging Project. Journal of Nutrition Health and Aging. 2001;5:269–277. [PubMed] [Google Scholar]
- Millen Posner BE, Smigelski CG, Krachenfels MM. Dietary characteristics and nutrient intake in an urban homebound population. Journal of the American Dietetic Association. 1987;87:452–456. [PubMed] [Google Scholar]
- Mirowsky J, Ross CE. Social causes of psychological distress. New York: Aldine de Gruyter; 1989. [Google Scholar]
- Health, United States, 2006 with chartbook on trends in the health of Americans. National Center for Health Statistics; Washington, DC: U.S. Government Printing Office; 2006. [PubMed] [Google Scholar]
- National Heart, Lung, and Blood Institute in cooperation with the National Institute on Diabetes and Digestive and Kidney Diseases. Clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults: The evidence report. 1998 (National Institutes of Health Publication No. 98-4083). Retrieved July 20, 2006 from www.nhlbi.nih.gov/guidelines/obesity/ob_gdlns.pdf.
- Olde-Rikkert GM, Riguad AS. Malnutrition research: High time to change the menu. Age and Ageing. 2003;32:241–243. doi: 10.1093/ageing/32.3.241. [DOI] [PubMed] [Google Scholar]
- U.S. Department of Health and Human Services, Centers for Medicare & Medicaid Services; Outcome and Assessment Information Set [data set] Retrieved July 18, 2006 from www.cms.hhs.gov/OASIS/ [Google Scholar]
- Panel on Macronutrients, Panel on the Definition of Dietary Fiber, Subcommittee on Upper Reference Levels of Nutrients, Subcommittee on Interpretation and Uses of Dietary Reference Intakes, and Standing Committee on the Scientific Evaluation of Dietary Reference Intakes. Dietary reference intake for energy, carbohydrate, fiber, fat, fatty acids, cholesterol, protein, and amino acids (macronutrients) Institute of Medicine of the National Academies. Washington, DC: The National Academies Press; 2005. Retrieved July 20, 2006 from www.nap.edu/catalog/10490.html. [Google Scholar]
- Payette H. Nutrition as a determinant of functional autonomy and quality of life in aging: A research program. Canadian Journal of Physiology and Pharmacology. 2005;83:1061–1070. doi: 10.1139/y05-086. [DOI] [PubMed] [Google Scholar]
- Payette H, Coulombe C, Boutier V, Gray-Donald K. Weight loss and mortality among free-living frail elders: A prospective study. Journal of Gerontology: Medical Sciences. 1999;54A:M440–M445. doi: 10.1093/gerona/54.9.m440. [DOI] [PubMed] [Google Scholar]
- Payette H, Coulombe C, Boutier V, Gray-Donald K. Nutrition risk factors for institutionalization in a free-living functionally dependent elderly population. Journal of Clinical Epidemiology. 2000;53:579–587. doi: 10.1016/s0895-4356(99)00186-9. [DOI] [PubMed] [Google Scholar]
- Payette H, Gray-Donald K, Cyr R, Boutier V. Predictors of dietary intake in a functionally dependent elderly population in the community. American Journal of Public Health. 1995;85:677–683. doi: 10.2105/ajph.85.5.677. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Payette H, Shatenstein B. Determinants of healthy eating in community-dwelling elderly people. Canadian Journal of Public Health. 2005;96(Suppl 3):27–31. [PubMed] [Google Scholar]
- Quandt SA, McDonald J, Arcury TA, Bell RA, Vitolins MZ. Nutritional self-management of elderly widows in rural communities. The Gerontologist. 2000;40:86–96. doi: 10.1093/geront/40.1.86. [DOI] [PubMed] [Google Scholar]
- Ritchie CS, Locher JL, Roth DL, McVie T, Sawyer P, Allman R. Unintentional weight loss predicts decline in ADL function and life space mobility over four years among community dwelling older adults. Journal of Gerontology: Medical Sciences. 2008;63(1):67–75. doi: 10.1093/gerona/63.1.67. [DOI] [PubMed] [Google Scholar]
- Roberts SB, Fuss P, Heyman MB, Evans WJ, Tsay R, Rasmussen H, et al. Control of food intake in older men. Journal of the American Medical Association. 1994;272:1601–1606. doi: 10.1001/jama.1994.03520200057036. [DOI] [PubMed] [Google Scholar]
- Roubenoff R. Sarcopenic obesity: The confluence of two epidemics. Obesity Research. 2004;12:887–888. doi: 10.1038/oby.2004.107. [DOI] [PubMed] [Google Scholar]
- Sahyoun NR, Lin C, Krall E. The nutritional status of the older adult is associated with dentition status. Journal of the American Dietetic Association. 2003;103:61–66. doi: 10.1053/jada.2003.50003. [DOI] [PubMed] [Google Scholar]
- Sahyoun NR, Pratt CA, Anderson A. Evaluating nutrition interventions for older adults: A proposed framework. Journal of the American Dietetic Association. 2004;104:58–69. doi: 10.1016/j.jada.2003.10.013. [DOI] [PubMed] [Google Scholar]
- Schakel S, Sievert YA, Buzzard IM. Sources of data for developing and maintaining a nutrient database. Journal of the American Dietetic Association. 1988;88:1268–1271. [PubMed] [Google Scholar]
- Schoeller DA. Recent advances from application of doubly labeled water to measurement of human energy expenditure. Journal of Nutrition. 1999;129:1765–1768. doi: 10.1093/jn/129.10.1765. [DOI] [PubMed] [Google Scholar]
- Sharkey JR. The interrelationship of nutritional risk factors, indicators of nutritional risk, and severity of disability among home-delivered meal participants. The Gerontologist. 2002;42:373–380. doi: 10.1093/geront/42.3.373. [DOI] [PubMed] [Google Scholar]
- Sharkey JR. Risk and presence of food insufficiency are associated with low nutrient intakes and multimorbidity among homebound older women who receive home-delivered meals. Journal of Nutrition. 2003;133:3485–3491. doi: 10.1093/jn/133.11.3485. [DOI] [PubMed] [Google Scholar]
- Sharkey JR. The influence of nutritional health on physical function: A critical relationship for homebound older adults. Generations. 2004;28(3):34–38. [Google Scholar]
- Sharkey JR, Branch L, Zohoori N, Giuliani C, Busby-Whitehead J, Haines PS. Inadequate nutrient intakes among homebound elderly and their correlation with individual characteristics and health-related factors. American Journal of Clinical Nutrition. 2002;76:1535–1545. doi: 10.1093/ajcn/76.6.1435. [DOI] [PubMed] [Google Scholar]
- Sharkey JR, Schoenberg NE. Prospective study of black–white differences in food insufficiency among homebound elders. Journal of Aging and Health. 2005;17:507–527. doi: 10.1177/0898264305279009. [DOI] [PubMed] [Google Scholar]
- Sherbourne CD, Stewart AL. The MOS Social Support Survey. Social Science & Medicine. 1991;32:705–714. doi: 10.1016/0277-9536(91)90150-b. [DOI] [PubMed] [Google Scholar]
- Smith R. Medicare reform: What it means to the future of dietetics. Journal of the American Dietetic Association. 2004;104:734–735. doi: 10.1016/j.jada.2004.03.008. [DOI] [PubMed] [Google Scholar]
- St-Onge M, Mignault D, Allison DB, Rabasa-Lhoret R. Evaluation of a portable device to measure daily energy expenditure in free-living adults. American Journal of Clinical Nutrition. 2007;85:742–749. doi: 10.1093/ajcn/85.3.742. [DOI] [PubMed] [Google Scholar]
- Sullivan DH, Liu L, Roberson PK, Bopp MM, Rees JS. Body weight change and mortality in a cohort of elderly patients recently discharged from the hospital. Journal of the American Geriatrics Society. 2004;52:1696–1701. doi: 10.1111/j.1532-5415.2004.52463.x. [DOI] [PubMed] [Google Scholar]
- Thomas DR. Weight loss in older adults. Reviews in Endocrine & Metabolic Disorders. 2005;6:129–136. doi: 10.1007/s11154-005-6725-6. [DOI] [PubMed] [Google Scholar]
- Trabuisi J, Schoeller DA. Evaluation of dietary assessment instruments against doubly labeled water, a biomarker of habitual energy intake. American Journal of Physiology: Endocrinology and Metabolism. 2001;281:E891–E899. doi: 10.1152/ajpendo.2001.281.5.E891. [DOI] [PubMed] [Google Scholar]
- Vailas L, Nitzke SA, Becker M, Gast J. Risk indicators for malnutrition are associated inversely with quality of life in participants in meal programs for older adults. Journal of the American Dietetic Association. 1998;98:548–553. doi: 10.1016/S0002-8223(98)00123-0. [DOI] [PubMed] [Google Scholar]
- Villareal D, Banks M, Sienerc C, Sinacore D, Klein S. Physical frailty and body composition in obese elderly men and women. Obesity Research. 2004;12:553–557. doi: 10.1038/oby.2004.111. [DOI] [PubMed] [Google Scholar]
- Wellman NS, Johnson MA. Food and nutrition for healthier aging. Generations. 2004;28(3) [Google Scholar]
- Witschi JC. Short-term recall and recording methods. In: Willett W, editor. Nutritional epidemiology. New York: Oxford University Press; 1990. pp. 663–671. [Google Scholar]
- Xia C, McCutcheon H. Mealtime in hospital—Who does what? Journal of Clinical Nursing. 2006;15:1221–1227. doi: 10.1111/j.1365-2702.2006.01425.x. [DOI] [PubMed] [Google Scholar]