

Abstract
Background:
Total pancreatectomy (TP) is performed for various indications. Historically, morbidity and mortality have been high. Recent series reporting improved peri-operative mortality have renewed interest in TP. We performed a national review of TP including indication, patient/hospital characteristics, complications and peri-operative mortality.
Methods:
The Nationwide Inpatient Sample (NIS) was queried to identify TPs performed during 1998 to 2006. Univariate analyses were used to compare patient/hospital characteristics. Multivariable logistic regression was performed to identify predictors of in-hospital mortality. Post-operative complications/disposition were assessed.
Results:
From 1998 to 2006, 4013 weighted patient-discharges occurred for TP. Fifty-three per cent were male; mean age 58 years. Indication: neoplastic disease 67.8%. Post-operative complications occurred in 28%. Univariate analyses: TPs increased significantly (1998, n= 384 vs. 2006 n= 494, P < 0.01). 77.1% of TPs occurred in teaching hospitals (P < 0.0001), 86.4% in hospitals performing <five pancreatectomies/year (P < 0.0001). In-patient mortality was 8.5% with a significant decrease (12.4% 1998–2000 vs. 5.9% 2002–2006, P < 0.01). Multivariable analyses: advanced age [referent ≤50 years; ≥70 Adjusted odds ratio (AOR) 3.4, 95% confidence interval (CI) 1.33–8.67], select patient comorbidities and year (referent = 2004–2006; 1998–2000 AOR 2.70; 95% CI 1.41–5.14) independently predicted in-patient mortality whereas hospital surgical volume did not.
Discussion:
TP is increasingly performed nationwide with a concomitant decrease in peri-operative mortality. Patient characteristics, rather than hospital volume, predicted increased mortality.
Introduction
Total pancreatectomy (TP) was first described by Rockey in 19431 and its popularity increased during the 1960s with the prospect of improving oncological outcomes and decreasing morbidity from anastomotic leaks.2 However, subsequent studies demonstrated TP did not improve Ro resections and had peri-operative mortality similar to or higher than classic Whipple resections.3,4 Furthermore, TP was complicated by permanent pancreatic endocrine and exocrine deficiencies.5 This led to surgeons largely abandoning TP and no longer considering TP as a viable option for pancreatic disease.
Recently, TP is being revisited as single institution series report improved per-operative mortality and long-term survival for TP to be similar to classic Whipple resections.6 Major advances in the management of the post-operative apancreatic state have improved post-operative morbidity associated with TP.7,8 Clinical indications for TP are increasingly reported in the literature. Concern regarding the extent of ductal disease for intraductal papillary mucinous neoplasms (IPMNs) has led some surgeons to advocate TP for surgical management.9 After TP, intractable pain associated with chronic pancreatitis refractory to conservative management has been reported to improve in 80% of patients.10 Multifocal metastatic renal cell carcinoma has been treated with removal of the entire gland through TP.11
With these recent findings, we sought to perform a current national review of TP including indications, patient/hospital characteristics, major post-operative complications and in-hospital mortality.
Methods
Database
The Nationwide Inpatient Sample (NIS) was queried between the years 1998 to 2006 for patient discharges for TP [International Classification of Diseases, 9th revision, clinical modification (ICD-9-CM) procedure code 52.6].12 Patients undergoing TP with a concurrent diagnosis of traumatic injury during the same hospital stay were excluded from further analyses. The NIS is the largest national all-payer hospital inpatient care database in the United States. Data exists for approximately 8 million hospital discharges per year from a stratified sample of 20% of non-federal US community hospitals (n= 1045 in 2006) from participating states (n= 38 in 2006), including academic and specialty hospitals. The NIS is supported by the Healthcare Cost and Utilization Project and contains all-payer discharge information for 100% of patient discharges from participating hospitals. It contains hospital level information obtained from a direct link to the American Hospital Association's annual survey of hospitals, which includes hospital type (teaching/nonteaching) and geographic region (Northeast, West, South, Midwest as defined by the US Census Bureau). A weighting strategy is implemented by the NIS to allow population-based estimates to be drawn at the national level. Sampled hospitals are given appropriate weights based on the number of hospitals they represent in the database for a given year.13 All statistical analyses were performed based on these survey weights; therefore, all data provided in the results represent weighted frequencies.
Patient and hospital characteristics
Patient demographics including age at admission, sex and race were collected. Race information was excluded from multivariable analyses because of the high rate of missing values. Patients were assigned a Charlson comorbidity score,14 based on ICD-9-CM diagnoses, according to the methods described by Deyo et al.15 In addition, independent patient comorbidities were evaluated in analyses from previously established comorbidity software for use with national datasets (congestive heart failure, chronic lung disease, valvular heart disease, renal failure, diabetes mellitus, liver disease and obesity).16
Indication for TP was determined by primary diagnoses codes (ICD-9-CM). Indications were categorized as neoplastic disease, pancreatitis, pancreatic cystic disease and other/unspecified (categorical ICD-9 codes listed in Appendix 1). Major post-operative complications were defined by specific diagnoses with codes based on their validation as true complications rather than comorbidities by the methods described by Lawthers et al.17 These were defined as secondary diagnoses of post-operative infection (except wound and pneumonia), acute myocardial infarction (MI), aspiration pneumonia, deep venous thrombosis (DVT), pulmonary embolism (PE), post-operative pulmonary compromise, post-operative gastrointestinal haemorrhage, reopening of a surgical site and procedure-related lacerations or perforations. A complete listing of ICD-9-CM codes used may be found in Appendix 1. Post-operative length of stay (LOS) was calculated by subtracting the number of days from admission to the first operation from the total length of stay.
Annual hospital surgical volume for pancreatectomy utilized methods described by McPhee et al.18 Low volume hospitals were defined as performing fewer then five pancreatic resections/year, and medium/high volume hospitals were defined as performing ≥five pancreatic resections/year.
Statistical analysis
All data were analysed through the advanced survey procedures available in SAS version 9.1 (SAS Institute, Cary, NC, USA). Univariate analyses of categorical variables were performed using Rao-Scott chi-square tests, with a P-value < 0.05 considered statistically significant. Trend analyses were performed using the Mantel–Haentszel chi-square test. Multivariable logistic regression was used to determine independent predictors of in-patient mortality.
Results
Patient and hospital demographics
During the sampled time frame of 1998–2006, 4013 weighted patient-discharges (n= 813 unweighted) were identified for patients who underwent TP. Patient and hospital demographics of the cohort are shown in Table 1. The mean age of patients was 58 years [95% confidence interval (CI) 57–60]. The majority of the cohort was White (58.8%, n= 2360), followed by non-Whites (18.1%, n= 726). Race information was missing for 23.1% (n= 927) of the cohort and race was then excluded from any further analyses. Similar numbers of males and females underwent TP (male 52.9%, n= 2124 vs. females 47.1% n= 1889, P= 0.14). The majority of patients undergoing TP had comorbidities as evidenced by an elevated Charlson score (Charlson score 2, 20%, n= 804, Charlson score ≥3 45.3%, n= 1817, P < 0.01). The majority of TPs were performed for neoplastic disease (67.8%, n= 2719), followed by pancreatitis (19.2%, n= 770), other/unspecified pancreatic disease (10.6%, n= 425) and pancreatic cystic disease (2.5%, n= 99) (P < 0.0001).
Table 1.
Patient and hospital characteristics for total pancreatectomy including univariate analyses, Nationwide Inpatient Sample (NIS) 1998–2006
| Weighted number (%) | P-value | |
|---|---|---|
| Total (n= 813) | 4013 (100) | |
| Age (years) | <0.0001 | |
| Mean [SEM] | 58.4 [0.77] | |
| <50 | 1080 (26.9) | |
| 50–69 | 1863 (46.4) | |
| >70 | 1070 (26.7) | |
| Sex | 0.14 | |
| Male | 2124 (52.9) | |
| Female | 1889 (47.1) | |
| Race | <0.0001 | |
| White | 2360 (58.8) | |
| Non-White | 726 (18.1) | |
| Other | 927 (23.1) | |
| Insurance status | <0.0001 | |
| Medicare | 1612 (40.2) | |
| Private/HMO | 1817 (45.3) | |
| Medicaid/self-pay | 419 (10.4) | |
| No charge/other | 165 (4.1) | |
| Teaching status | <0.0001 | |
| Teaching | 3088 (77.1) | |
| Non-teaching | 925 (22.9) | |
| Hospital volume | <0.0001 | |
| <five resections/year | 3467 (86.4) | |
| ≥five resections/year | 546 (13.6) | |
| Year | <0.01 | |
| 98–00 | 1240 (30.9) | |
| 01–03 | 1378 (34.4) | |
| 04–06 | 1395 (34.7) | |
| Charlson score | <0.0001 | |
| 0 | 894 (22.3) | |
| 1 | 498 (12.4) | |
| 2 | 804 (20.0) | |
| ≥ 3 | 1817 (45.3) | |
| Indication | <0.0001 | |
| Neoplastic disease | 2719 (67.8) | |
| Pancreatitis | 770 (19.1) | |
| Cyst/benign | 99 (2.5) | |
| Other/unspecified | 425 (10.6) |
SEM, standard error of mean.
TP was more likely to be performed in a teaching hospital (77.1%, n= 3088) than a non-teaching hospital (22.9%, n= 916). The majority of TPs (86.4%, n= 3467) were performed at institutions performing fewer than five pancreatic resections per year (P < 0.0001). Nationwide utilization of TP increased significantly over the time period studied with 384 TPs performed in 1998 and 494 performed in 2006 (P < 0.01 trend analysis) (Fig. 1).
Figure 1.
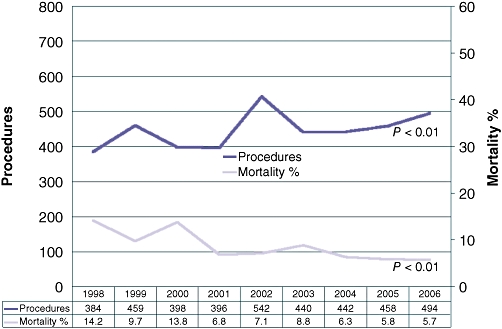
Annual volume and in-hospital mortality for total pancreatectomy, Nationwide Inpatient Sample (NIS) 1998–2006
Post-operative complications and patient disposition
Major in-hospital complications occurred in 28% (n= 1136) of patients who underwent TP (Fig. 2). Pulmonary compromise (12%, n= 485), gastrointestinal (GI) haemorrhage (4.2%, n= 168) and DVT/ PE (3.7%, n= 149) were the most frequent complications (Fig. 2).
Figure 2.
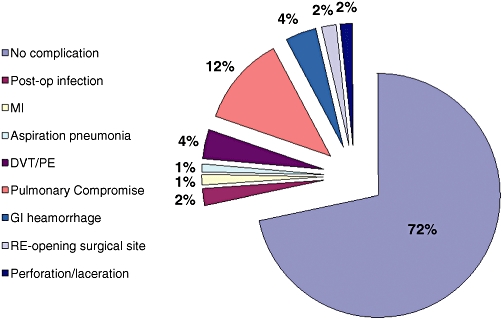
Major in-hospital complications after total pancreatectomy. MI, myocardial infraction; DVT, deep vein thrombosis; PE, pulmonary embolism; GI, gastrointestinal; MI = Myocardial Infarction; DVT = Deep Venous Thrombosis; PE = Pulmonary Embolism; GI = Gastrointestinal
Mean LOS was 16.6 days (95% CI 15.3–17.8) for patients undergoing TP. After TP, the majority of patients were discharged home (56%, n= 2236) with an additional 23% (n= 939) discharged home with visiting nurse services. A smaller percentage (12%, n= 487) were discharged to either a short-term rehabilitation centre or skilled nursing facility (Fig. 3).
Figure 3.
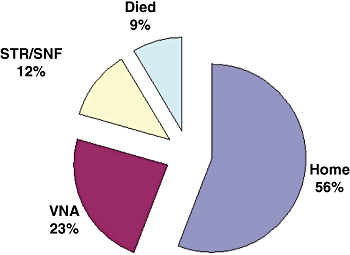
Patient disposition after total pancreatectomy. STR, short-term rehabilitation; SNF, skilled nursing facility; VNA, visiting nurse
Univariate analyses of mortality
Over the years studied, the overall in-patient mortality rate for TP was 8.5% as shown in Table 2. In-patient mortality significantly decreased over time with in-patient mortality in 1998 of 14.2% which declined to 5.7% in 2006 (trend P < 0.01) (Fig. 1). Advanced age was associated with increased in-patient mortality (≥70 years, 12.6%, n= 135, vs. 50–69 years, 8.2%, n= 153, vs. <50 years, 4.8%, n= 52, P < 0.05). Comorbidities were associated with increased mortality risk (Charlson score 0, 6.1%, n= 55 vs. Charlson score ≥3, 9.7%, n= 175, P < 0.01). Indication for TP was not associated with an increased risk of mortality (P= 0.80).
Table 2.
Univariate analyses of in-patient mortality for total pancreatectomy, Nationwide Inpatient Sample (NIS) 1998–2006
| Weighted number | Mortality rate (%) | P-value | |
|---|---|---|---|
| Total (n= 813) | 340 | 8.5 | |
| Age (years) | <0.05 | ||
| <50 | 52 | 4.8 | |
| 50–69 | 153 | 8.2 | |
| >70 | 135 | 12.6 | |
| Gender | 0.22 | ||
| Male | 169 | 8.0 | |
| Female | 171 | 9.1 | |
| Race | 0.15 | ||
| White | 194 | 8.2 | |
| Non-White | 54 | 7.5 | |
| Other | 92 | 10 | |
| Insurance status | <0.0001 | ||
| Medicare | 174 | 10.9 | |
| Private/HMO | 108 | 5.9 | |
| Medicaid/self-pay/other | 58 | 9.9 | |
| Teaching status | 0.37 | ||
| Teaching | 255 | 8.3 | |
| Non-teaching | 85 | 9.2 | |
| Hospital volume | <0.01 | ||
| <five resections/year | 312 | 9.0 | |
| ≥five resections/year | 28 | 5.2 | |
| Year | <0.01 | ||
| 98–00 | 154 | 12.4 | |
| 01–03 | 103 | 7.6 | |
| 04–06 | 83 | 5.9 | |
| Charlson score | <0.01 | ||
| 0 | 55 | 6.1 | |
| 1 | 51 | 10.4 | |
| 2 | 59 | 7.4 | |
| 3 or more | 175 | 9.7 | |
| Indication | 0.80 | ||
| Neoplastic disease | 229 | 8.4 | |
| Benign disease | 111 | 8.7 |
In-patient mortality was similar for TP performed at both teaching and non-teaching hospitals (8.3%, n= 255 vs. 9.2%, n= 85, P= 0.37). Hospital volume of pancreatic resection correlated significantly with peri-operative mortality on univariate analyses. Among hospitals performing fewer than five pancreatic resections annually, in-patient mortality for TP was 9% (n= 312). In comparison, in-patient mortality was 5.2% (n= 28) for hospitals performing ≥five pancreatic resections annually (P < 0.01).
Multivariable analyses
Using a multivariable logistic regression model, independent predictors of in-hospital mortality were evaluated. Significant factors identified on univariate analyses and those with biological plausibility were incorporated into the model with results demonstrated in Table 3. Patient characteristics including advanced age (referent ≤50 years; ≥70 years, AOR 3.40, 95% CI 1.33–8.67) and the presence congestive heart failure (CHF) (referent = no CHF; AOR 3.39, 95% CI 1.26–9.11), liver disease (referent = no liver disease; AOR 6.80, 95% CI 2.72–17.02) or renal failure (referent = no renal failure; AOR 4.52; 95% CI 1.47–13.89) were independently predictive of increased in-patient mortality. During 1998 to 2000, patients undergoing TP had a 2.7-fold increased risk (95% CI 1.41–5.14) of peri-operative mortality when compared with TPs performed during the more recent time period of 2004–2006. Neither hospital teaching status nor hospital volume of pancreatic resections was independently associated with peri-operative mortality for TP on multivariate analyses.
Table 3.
Logistic regression of in-hospital mortality for total pancreatectomy, Nationwide Inpatient Sample (NIS) 1998–2006
| AOR | 95% CI | |
|---|---|---|
| Patient gender | ||
| Male | Referent | |
| Female | 1.09 | 0.65–1.82 |
| Age groups (years) | ||
| <50 | Referent | |
| 50–69 | 2.25 | 0.93–5.43 |
| ≥70 | 3.40 | 1.33–8.67 |
| Year group | ||
| 1998–2000 | 2.70 | 1.41–5.14 |
| 2001–2003 | 1.67 | 0.82–3.38 |
| 2004–2006 | Referent | |
| Comorbidities | Referent = none | |
| Diabetes | 0.60 | 0.29–1.06 |
| Chronic lung disease | 0.82 | 0.35–1.95 |
| Congestive heart failure | 3.39 | 1.26–9.11 |
| Valvular heart disease | 2.02 | 0.47–8.79 |
| Liver disease | 6.80 | 2.72–17.02 |
| Renal failure | 4.52 | 1.47–13.89 |
| Obesity | 0.71 | 0.08–6.67 |
| Hospital volume | ||
| <five resections/year | 1.96 | 0.54–7.11 |
| ≥five resections/year | Referent | |
| Teaching status | ||
| Teaching | Referent | |
| Non-teaching | 0.85 | 0.46–1.56 |
| Indication | ||
| Neoplastic disease | Referent | |
| Pancreatitis | 1.50 | 0.70–3.24 |
| Cyst/benign | 0.92 | 0.17–5.00 |
| Other/unspecified | 1.36 | 0.46–3.99 |
AOR, adjusted odds ratio; CI, confidence interval.
Discussion
We performed a national review of total pancreatectomy performed for neoplastic and benign indications. We found a significant increase in the number of TPs performed annually from 1998–2006 with a concomitant decrease in peri-operative mortality. Patient characteristics including advanced age and the presence of select comorbid conditions (congestive heart failure, liver disease and renal disease) independently predicted in-patient mortality. Indication for TP and hospital characteristics including annual resection volume and teaching status, were not independently associated with perioperative mortality. TP was associated with significant morbidity with major in-hospital complications occurring in nearly 30% of patients.
Historically, operative mortality for TP has been high, with single-institution rates greater than 20%.19,20 Prohibitive mortality coupled with significant morbidity managing the apancreatic state, led some surgeons to argue against the use of TP.21 However, recent single-institution series have reported lower peri-operative mortality rates for TP ranging from 3% to 6.1%.6,7,22,23 Our overall national rate of 8.5% for peri-operative mortality is slightly higher, although when reviewing the most recent years included in our study (2004–2006), we found peri-operative mortality to be 5.7–6.3%. Consistent with our findings, McPhee et al. reported decreasing perioperative mortality associated with TP in a national review of all types of pancreatectomy performed for neoplastic disease.18
Post-operative surgical morbidity associated with TP remains high with complication rates ranging from 36% to 54% in single-institution series.6,22,23 In our cohort, 28% developed a major post-operative complication during their hospital stay. This number is likely underestimated, as we utilized a set of validated complication codes, therefore limiting the number of complications evaluated. Despite the relatively high complication rate, nearly 80% of patients were discharged home after TP (with/without visiting nurse services).
The call for regionalization of complex, high mortality-rate procedures to large, high-volume centres has been well described in the literature.24,25 We found high volume hospitals (≥five pancreatic resections/year) to be associated with improved survival for TP on univariate analyses. However, after adjustment for additional covariates in multivariable analyses, high volume hospitals were no longer protective against peri-operative mortality. Individual patient factors, namely advanced age (>70 years) and the presence of comorbid conditions, were predictive of increased mortality. This suggests that careful patient selection may be more prognostic for in-patient mortality than absolute hospital surgical volume. The majority of TPs were performed at institutions performing fewer than five resections per year.
While our study demonstrates the recent national trends for TP, its limitations must be acknowledged. The NIS is an administrative database and therefore lacks certain clinical information including patient-level factors (pre-operative performance status and laboratory values), operative data (blood loss and transfusions), and long-term follow-up/re-admission information. Racial demographic information was largely missing necessitating removal of race from multivariable analyses. The NIS provides information on individual hospital admissions, allowing for evaluation of in-hospital mortality. This may reflect a lower rate when compared with studies utilizing 30-day mortality rates. We evaluated post-operative complications using a validated set of ICD-9 codes,17 however, the true complication rate may have been underestimated. Long-term outcomes of managing the post-operative apancreatic state were not available for evaluation. However, despite these limitations, the NIS provides a mechanism to study national trends of procedures, diagnoses and outcomes including in-patient mortality.
Indications for TP are being re-visited as the peri-operative mortality rate has become more acceptable. Concern regarding the extent of ductal disease for IPMN has led to the inclusion of TP in the armamentarium of surgical options.9,26,27 Intractable pain associated with chronic pancreatitis refractory to medical management, has been shown to significantly improve after TP.10,28,29 Additionally, TP may serve a role in diseases likely affecting the entire gland including familial pancreatic adenocarcinoma, neuroendocrine tumours,26 and metastatic disease.11 Management of the diabetic state after TP has been improved with the availability of long-acting insulin and continuous subcutaneous insulin pumps.30 Pancreatic enzyme replacement has assisted in the treatment of the acquired exocrine deficiency after TP.
With expanding indications and improved post-operative treatment strategies, TP is increasingly performed nationwide. While in-hospital morbidity remains substantial, TP is a viable option for specific indications with acceptable in-patient mortality. Careful patient selection and pre-operative counselling may further improve patient outcomes for TP. Additional studies including patient-level data, operative information, quality of life and long-term survival are warranted to provide a fuller understanding of the specific predictors of outcome after TP.
Appendix 1
| ICD-9-CM diagnoses | |
|---|---|
| Indication | |
| Neoplastic disease | 157.1, 157.2, 157.3, 157.0, 157.4, 157.8, 157.9, 156.2, 156.1, 152.0, 197.8, 151.8, 196.2, 197.4, 197.6, 153.7, 194.0, 156, 156.0, 156.8, 230.9, 235.5, 239.0, 211.6, 235.3, 211.5, 230, 230.2, 230.7, 230.8, 230.9, 235.2, 235.3, 235.4, 235.5, 239.9, 211, 211.1, 211.2, 211.6, 211.7, 211.8, 211.9, 239, 239.8, 239.9, 158.0, 189.0, 202.82, 151.4, 153.3, 159.9 |
| Pancreatitis | 577.0, 577.1, 576.1 |
| Cystic disease | 577.2 |
| Complications | |
| Post-operative infection | 000.45, 320.00–320.99, 510.0, 510.9, 513.1, 519.2, 590.10–590.11, 590.80, 683 |
| Myocardial infarction | 410.00–410.91 |
| Aspiration pneumonia | 507.0 |
| Deep venous thrombosis/pulmonary embolism | 415.1, 451.11, 451.19, 451.2, 451.81, 453.8 |
| Pulmonary compromise | 514, 518.4, 518.5, 518.81, 518.82 |
| Gastrointestinal haemorrhage | 530.82, 531.00–531.21, 531.40–531.41, 531.60–531.61, 532.00–532.21, 532.40–532.41, 533.60–533.61, 534.00–534.21, 534.40–534.41, 534.60–534.61, 535.01, 535.11, 535.21, 535.31, 353.41, 535.51, 535.61, 578.9 |
| Reopening surgical site | 01.23, 03.03, 06.02, 34.09, 35.95, 39.49, 54.12, 54.61 |
| Procedure-related perforation or laceration | 530.4, 569.83, 575.4, 29.51, 31.61, 33.41, 33.43, 42.82, 44.61, 46.71, 46.75, 48.71, 50.61, 51.91, 55.81, 56.82, 57.81, 58.41, 69.41 |
Conflicts of interest
None declared.
References
- 1.Rockey EW. Total pancreatectomy for carcinoma: case report. Ann Surg. 1943;118:603–611. doi: 10.1097/00000658-194310000-00008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.ReMine WH, Priestley JT, Judd ES, King JN. Total pancreatectomy. Ann Surg. 1970;172:595–604. doi: 10.1097/00000658-197010000-00006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Sarr MG, Behrns KE, van Heerden JA. Total pancreatectomy. An objective analysis of its use in pancreatic cancer. Hepatogastroenterology. 1993;40:418–421. [PubMed] [Google Scholar]
- 4.Grace PA, Pitt HA, Tompkins RK, DenBesten L, Longmire WP., Jr Decreased morbidity and mortality after pancreatoduodenectomy. Am J Surg. 1986;151:141–149. doi: 10.1016/0002-9610(86)90024-3. [DOI] [PubMed] [Google Scholar]
- 5.Dresler CM, Fortner JG, McDermott K, Bajorunas DR. Metabolic consequences of (regional) total pancreatectomy. Ann Surg. 1991;214:131–140. doi: 10.1097/00000658-199108000-00007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Muller MW, Friess H, Kleeff J, Dahmen R, Wagner M, Hinz U, et al. Is there still a role for total pancreatectomy? Ann Surg. 2007;246:966–974. doi: 10.1097/SLA.0b013e31815c2ca3. [DOI] [PubMed] [Google Scholar]
- 7.Billings BJ, Christein JD, Harmsen WS, Harrington JR, Chari ST, Que FG, et al. Quality-of-life after total pancreatectomy: is it really that bad on long-term follow-up? J Gastrointest Surg. 2005;9:1059–1066. doi: 10.1016/j.gassur.2005.05.014. [DOI] [PubMed] [Google Scholar]
- 8.The Diabetes Control and Complications Trial Research Group. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med. 1993;329:977–986. doi: 10.1056/NEJM199309303291401. [DOI] [PubMed] [Google Scholar]
- 9.Cuillerier E, Cellier C, Palazzo L, Deviere J, Wind P, Rickaert F, et al. Outcome after surgical resection of intraductal papillary and mucinous tumors of the pancreas. Am J Gastroenterol. 2000;95:441–445. doi: 10.1111/j.1572-0241.2000.01764.x. [DOI] [PubMed] [Google Scholar]
- 10.Linehan IP, Lambert MA, Brown DC, Kurtz AB, Cotton PB, Russell RC. Total pancreatectomy for chronic pancreatitis. Gut. 1988;29:358–365. doi: 10.1136/gut.29.3.358. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Wente MN, Kleeff J, Esposito I, Hartel M, Muller MW, Frohlich BE, et al. Renal cancer cell metastasis into the pancreas: a single-center experience and overview of the literature. Pancreas. 2005;30:218–222. doi: 10.1097/01.mpa.0000153337.58105.47. [DOI] [PubMed] [Google Scholar]
- 12.CDC. International Classification of Diseases, 9th Revision, Clinical Modification. Salt Lake City, UT: Medicode Publications; 2001. [Google Scholar]
- 13.Project HCUP. Overview of the Nationwide Inpatient Sample (NIS) cited 15 September 2008]. http://www.hcup-us.ahrq.gov/nisoverview.jsp.
- 14.Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40:373–383. doi: 10.1016/0021-9681(87)90171-8. [DOI] [PubMed] [Google Scholar]
- 15.Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J Clin Epidemiol. 1992;45:613–619. doi: 10.1016/0895-4356(92)90133-8. [DOI] [PubMed] [Google Scholar]
- 16.Elixhauser A, Steiner C, Harris DR, Coffey RM. Comorbidity measures for use with administrative data. Med Care. 1998;36:8–27. doi: 10.1097/00005650-199801000-00004. [DOI] [PubMed] [Google Scholar]
- 17.Lawthers AG, McCarthy EP, Davis RB, Peterson LE, Palmer RH, Iezzoni LI. Identification of in-hospital complications from claims data. Is it valid? Med Care. 2000;38:785–795. doi: 10.1097/00005650-200008000-00003. [DOI] [PubMed] [Google Scholar]
- 18.McPhee JT, Hill JS, Whalen GF, Zayaruzny M, Litwin DE, Sullivan ME, et al. Perioperative mortality for pancreatectomy: a national perspective. Ann Surg. 2007;246:246–253. doi: 10.1097/01.sla.0000259993.17350.3a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Cooperman AM, Herter FP, Marboe CA, Helmreich ZV, Perzin KH. Pancreatoduodenal resection and total pnacreatectomy – an institutional review. Surgery. 1981;90:707–712. [PubMed] [Google Scholar]
- 20.Ihse I, Anderson H, Andren S. Total pancreatectomy for cancer of the pancreas: is it appropriate? World J Surg. 1996;20:288–293. doi: 10.1007/s002689900046. [DOI] [PubMed] [Google Scholar]
- 21.Brooks JR. Where are we with pancreas transplantation? Surgery. 1989;106:935–945. [PubMed] [Google Scholar]
- 22.Schmidt CM, Glant J, Winter JM, Kennard J, Dixon J, Zhao Q, et al. Total pancreatectomy (R0 resection) improves survival over subtotal pancreatectomy in isolated neck margin positive pancreatic adenocarcinoma. Surgery. 2007;142:572–578. doi: 10.1016/j.surg.2007.07.016. [DOI] [PubMed] [Google Scholar]
- 23.Karpoff HM, Klimstra DS, Brennan MF, Conlon KC. Results of total pancreatectomy for adenocarcinoma of the pancreas. Arch Surg. 2001;136:44–47. doi: 10.1001/archsurg.136.1.44. [DOI] [PubMed] [Google Scholar]
- 24.Dimick JB, Cowan JA, Jr, Colletti LM, Upchurch GR., Jr Hospital teaching status and outcomes of complex surgical procedures in the United States. Arch Surg. 2004;139:137–141. doi: 10.1001/archsurg.139.2.137. [DOI] [PubMed] [Google Scholar]
- 25.Finlayson EV, Goodney PP, Birkmeyer JD. Hospital volume and operative mortality in cancer surgery: a national study. Arch Surg. 2003;138:721–725. doi: 10.1001/archsurg.138.7.721. [DOI] [PubMed] [Google Scholar]
- 26.Heidt DG, Burant C, Simeone DM. Total pancreatectomy: indications, operative technique, and postoperative sequelae. J Gastrointest Surg. 2007;11:209–216. doi: 10.1007/s11605-006-0025-7. [DOI] [PubMed] [Google Scholar]
- 27.Bendix Holme J, Jacobsen N, Rokkjaer M, Kruse A. Total pancreatectomy in six patients with intraductal papillary mucinous tumour of the pancreas: the treatment of choice. HPB (Oxford) 2001;3:257–262. doi: 10.1080/136518201753335539. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Cooper MJ, Williamson RC, Benjamin IS, Carter DC, Cuschieri A, Linehan IP, et al. Total pancreatectomy for chronic pancreatitis. Br J Surg. 1987;74:912–915. doi: 10.1002/bjs.1800741013. [DOI] [PubMed] [Google Scholar]
- 29.Alexakis N, Ghaneh P, Connor S, Raraty M, Sutton R, Neoptolemos JP. Duodenum- and spleen-preserving total pancreatectomy for end-stage chronic pancreatitis. Br J Surg. 2003;90:1401–1408. doi: 10.1002/bjs.4324. [DOI] [PubMed] [Google Scholar]
- 30.Radermecker RP, Scheen AJ. Continuous subcutaneous insulin infusion with short-acting insulin analogues or human regular insulin: efficacy, safety, quality of life, and cost-effectiveness. Diabetes Metab Res Rev. 2004;20:178–188. doi: 10.1002/dmrr.447. [DOI] [PubMed] [Google Scholar]