

Abstract
Background
Individuals with medial knee osteoarthritis often present with varus knee alignment and ambulate with increased knee adduction moments. Understanding the factors that relate to the knee adduction moment in healthy individuals may provide insight into the development of this disease. Thus, this study aimed to examine the relationships of both static and dynamic lower extremity measures with the knee adduction moment. We hypothesized that the dynamic measures would be more closely related to this moment.
Methods
Arch height index, hip abduction strength and two static measures of knee alignment were recorded for 37 young asymptomatic knees that varied from normal to varus-aligned. Overground gait analyses were also performed. Correlation coefficients were used to assess the relationships between the static and dynamic variables to the knee adduction moment. Hierarchical regression analyses were then conducted using the static measures, the dynamic measures, and the static and dynamic measures together.
Results
Among the static measures, the tibial mechanical axis and the distance between the medial knee joint lines were correlated with the knee adduction moment. The best predictive static model (R2 = 0.53) included only the tibial mechanical axis. Among the dynamic variables, knee adduction and rearfoot eversion angles were correlated with the knee adduction moment. Knee adduction and rearfoot eversion, together, were the best dynamic model (R2=0.53). The static and dynamic measures together created the strongest of the three models (R2 = 0.59).
Conclusions
These results suggest that dynamic measures slightly enhance the predictive strength of static measures when explaining variation in the knee adduction moment.
Introduction
Knee osteoarthritis (OA) is among the most common and disabling medical conditions of the elderly (Guccione, 1994). The prevalence of symptomatic knee OA is estimated at 12.1% for adults aged greater than 60 years, and the lifetime incidence risk is nearly 1 in 2 persons (Dillon et al., 2006; Murphy et al., 2008). Of the joint compartments, the medial tibiofemoral compartment is most commonly affected (Dearborn et al, 1996). Varus knee alignment is commonly associated with medial knee OA. Varus alignment has been shown to quadruple the risk of disease progression in individuals with existing medial knee OA (Sharma et al., 2001). Further, varus knee alignment doubles the risk of developing OA in individuals with otherwise healthy knees (Brouwer et al., 2007). These studies suggest that varus alignment is associated with increased medial knee loading, which, in turn, contributes to the development of OA.
The knee external adduction moment (KEAM) has become an important variable of interest in the study of knee OA. It is often used as a surrogate measure for medial knee loading, as measuring in vivo knee loads is difficult (Andriacchi, 1994). The KEAM has been related to increased medial tibial bone mineral density (Hurwitz et al., 1998; Wada et al., 2001; Bennell et al., 2008), decreased medial tibial plateau cartilage volume (Jackson et al., 2004), increased medial knee contact forces (Zhao et al., 2007, Mundermann et al., 2008), and consequently to medial knee OA disease progression (Miyazaki et al., 2002).
Static measures that represent frontal plane alignment may be correlated with the KEAM. Two clinical measures, tibial mechanical axis (TMA) and the distance between the medial knee joint lines (DMJL), have been found to correlate well with radiographic knee alignment (Hinman et al., 2006). Knee malalignment may result in compensatory alignments distally. With greater varus knee alignment, the calcaneus is naturally in a more varus alignment at footstrike. Thus, the rearfoot (and possibly the midfoot) may undergo increased pronation to help get the foot plantigrade. Interestingly, these motions may help to reduce the KEAM by indirectly moving the knee medially. Proximally, greater knee varus may also be associated with greater hip abduction. This may potentially decrease the relative eccentric demand on the hip abductors during single-limb stance and lead to weakness. Previous authors have suggested such a relationship between hip strength and the KEAM (Chang et al., 2004)
As the KEAM is a dynamic measure, however, it may be more strongly correlated to frontal plane dynamic movement patterns than to static measures. Surprisingly, the relationships of the KEAM to lower extremity joint kinematics have not been evaluated. Due to increased varus knee alignment, greater knee adduction is likely present during stance. In addition, increased foot pronation may be indicated by increased rearfoot eversion during gait. Finally, greater hip abduction (or less movement into hip adduction) may be seen with increasing varus knee alignment.
Therefore, the objective of this study was to examine the relationships of selected static and dynamic measures of the lower extremity with the KEAM. We hypothesized that the static measures of TMA and DMJL would be positively associated with the KEAM. In addition, we expected that arch flattening between sitting and standing would be inversely associated with the KEAM. Finally, weak hip abductors were expected to be associated with greater KEAM. For the dynamic measures, we expected that hip abduction, knee adduction and rearfoot eversion joint angles would be positively associated with the peak KEAM. We also expected that some combination of the dynamic measures would provide a more robust predictive model of the KEAM than the static measures. However, ultimately, we expected that the most robust model would likely include both static and dynamic measures.
Methods
SUBJECTS
Thirty-seven subjects (32 males), who were part of a study investigating gait patterns in varus and normally-aligned knees, were included in this study. The varus individuals were recruited initially and gender matched with the normally aligned individuals. It has been reported that males are generally more varus-aligned than females (Tillman et al., 2005) thus accounting for this gender bias. All subjects were between 18–35 years of age and were recruited from a university environment. Individuals were excluded if they reported current or previous ligamentous, meniscal, chondral, patellofemoral or bony pathology at the knee. All subjects also completed the Sports and Recreational Activities subscale of the Knee Injury and Osteoarthritis Outcome Score Knee Survey (KOOS-SR) (Roos et al., 1998). Answers to the items were based on the previous week, and were indicated using a Likert scoring system (0–4). A score of 0 indicated no symptom during the activity, and a score of 4 indicated extreme symptoms or difficulty. The five activities were squatting, running, jumping, twisting/pivoting and kneeling. Individuals who scored greater than 2/20 for the subscale were excluded from the study.
Knee alignment was measured in those who met the initial inclusion criteria. Knee alignment was determined using measurement of TMA with respect to vertical (Figure 1). For this measure, individuals stood in tandem stance with their weight evenly distributed between both feet while maintaining full knee extension. Using a caliper-inclinometer device (Isomed, Portland, OR, USA), the proximal arm was placed at the most prominent aspect of the tibial tuberosity. The distal arm was placed at the center of the palpable depression over the neck of the talus. The measure was then recorded to the nearest degree. To qualify, the TMA value had to exceed 7° from vertical in the varus direction. The limb with the greater TMA was the test limb. This value is 0.5 standard deviations below a mean of TMA values of 30 healthy individuals (mean age 26.5, SD 6.1 years, mean TMA 8.0°, SD 1.9°) collected in our laboratory. This resulted in the inclusion of subjects with normal to varus alignment of the knee.
Figure 1.

Clinical measurement of tibial mechanical axis with a caliper-inclinometer device using procedures modified from Hinman and colleagues (2006).
STATIC MEASURES
Prior to conducting the investigation, the within-tester reliability of the static measurements was assessed for the single investigator. Measurements were taken three times on five pilot subjects according to the previously described methods. Subjects were repositioned between tests, and greater than 2 minutes separated the trials. Intraclass correlation coefficients (model 3,1) ranged from 0.83 to 0.97 (Table 1).
Table 1.
Reliability of clinical measures performed in this study
| Measurement | Reliability Coefficient (ICC 3,1) |
|---|---|
| Tibial Mechanical Axis | 0.93 |
| Hip External Rotation Range of Motion | 0.92 |
| Hip Extension Range of Motion | 0.83 |
| Hip Abduction Strength | 0.91 |
| Distance b/n Medial Knee Joint Lines | 0.95 |
| Arch Height Index | 0.93 |
Two static measures of frontal plane knee alignment were assessed. The first was TMA relative to vertical, as described for the screening of subjects. It should be noted that Hinman and colleagues recorded their measure in natural stance. Our modification was implemented to minimize the between-subject variability of the measurement position. The second measure was DMJL, again taken in tandem stance. The joint lines were identified using palpation. Then, sliding calipers, marked in 1-millimeter increments, was used to measure the distance (Hinman et al., 2006). The value was recorded to the nearest millimeter.
The arch height index measurement system was used to assess medial arch characteristics (Butler et al., 2008). The arch height index is the ratio of the arch height (measured at 50% foot length) to the truncated foot length (measured from the heel to the first metatarsophalangeal joint (Williams et al, 2000) (Figure 2). The measure was first taken with the subject in sitting with their hips and knees at 90 degrees of flexion and their feet resting on the floor. The measure was then repeated with the subject standing with weight equally distributed on both feet. The difference in the measure between sitting and standing was calculated and was used as the measure of midfoot pronation (or arch flattening) with weight bearing.
Figure 2.
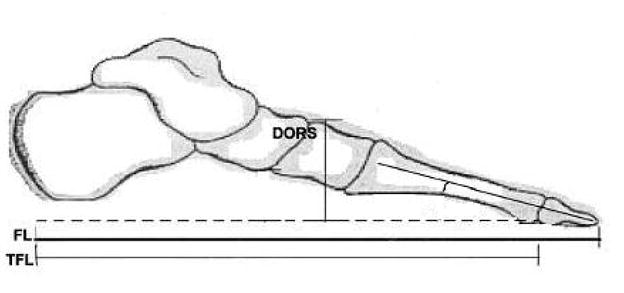
Schematic representation of landmarks used in determining arch height index. FL=foot length, TFL=truncated foot length, DORS=dorsum height. Adapted from Williams et al., 2000, with permission.
For hip abduction strength, peak isometric force was measured using a hand-held dynamometer (Lafayette Instruments, Lafayette, IN, USA). The force range of the dynamometer was from 0 to 199.9 kg. Straps were used to stabilize the subject and eliminate the influence of tester strength. Subjects were instructed to lie on the contralateral side to the test limb, with the test limb toward the ceiling (Bohannon, 1997). The dynamometer was placed on the lateral thigh, one inch proximal to the knee joint line. Pillows were placed between the legs such that both hips were in 0° of abduction, and the thigh of the test limb was horizontal. The dynamometer was secured to the leg with a strap wrapped around the leg and under the plinth. The subjects were instructed to raise their top leg up towards the ceiling with maximal effort. Two practice and three experimental trials were performed for five seconds with at least 15 seconds of rest between trials. The force measurements were multiplied by the length of the thigh to obtain a torque value, and then normalized to body weight. The mean normalized peak torque of the three trials was analyzed.
DYNAMIC MEASURES
In order to obtain dynamic measures, retroreflective markers were attached to the pelvis, thigh, shank and foot. Anatomical markers were placed over the iliac crests, greater trochanters, medial and lateral femoral condyles, and the medial and lateral tibial plateaus. They were also positioned over medial and lateral malleoli, the first and fifth metatarsal heads, and the tip of the standardized lab shoe (Air Pegasus, Nike, Beaverton, OR, USA). Tracking markers were positioned as a cluster of 3 on the rearfoot of the shoe, a cluster of 4 on the posterior shank, and a cluster of 4 on the lateral thigh. Individual tracking markers were placed on the anterior superior iliac spines and the L5-S1 interspinous space. The shank and thigh markers were adhered to rigid shells that were affixed to the subjects with Velcro using elastic straps.
The subjects then entered a calibrated volume to prepare for the dynamic trials. The approximate dimensions of the capture volume were 0.92 X 0.92 X 1.22 m. The camera calibration residual errors from the eight cameras were held below 0.6 mm (VICON, Oxford Metrics, UK). First, a standing calibration trial was collected. Next, a hip motion trial was collected to functionally determine the hip joint center (Hicks & Richards, 2005). The anatomical markers were then removed, leaving the tracking markers for the walking trials.
Dynamic data were then captured for level walking. Five usable trials were collected. Subjects walked at a controlled walking speed of 1.46 m/s (SD 0.04 m/s). The marker data were collected at 120 Hz, and filtered offline using a fourth-order, zero lag, low-pass Butterworth filter with a cut-off frequency of 8 Hz. Kinetic data from the force platform were collected at 1080 Hz (BERTEC Corp., Worthington, OH, USA), and low-pass filtered at 50 Hz. These low pass filter cut-off frequencies retained at least 95% of the power of each signal (Antonsson & Mann, 1985).
Finally, post-processing to calculate the data of interest was conducted. Visual3D software (Version 3.91, C-Motion Inc, Rockville, MD, USA) was used to calculate kinematic and kinetic time series data. All lower extremity segments were modeled as conical frustra, with inertial parameters estimated from established anthropometric data (Dempster et al., 1959). Joint kinematics were calculated using an X-Y-Z Euler rotation sequence, equivalent to the Joint Coordinate System (Grood & Suntay, 1983). Joint kinetic data were calculated using three-dimensional inverse dynamics, and the external joint moment data were normalized to body mass and height. Custom-written software programs (LabView 8.2, National Instruments, Austin, TX, USA) extracted the kinematic data at the rearfoot, knee and hip at the time of peak KEAM.
STATISTICAL ANALYSIS
Data were analyzed using SPSS version 15.0 (SPSS Inc, Chicago, IL, USA). Means and standard deviations of the variables of interest were calculated. Pearson’s correlation coefficients and Spearman’s rank correlation coefficients were used to examine bivariate relationships among the KEAM and the variables of interest. We then used stepwise multiple linear regressions (penter ≤ 0.05, premove ≥ 0.10) to create three separate models explaining variation in the peak KEAM. The first regression model used the static measures as independent variables. The second model used the dynamic variables. The final model used the static and dynamic correlates as independent variables. The stepwise multiple linear regression approach was chosen as a conservative approach, considering limitations in sample size. An alpha level of 0.05 was used for all tests.
Results
Overall, the subjects in the cohort were young, fit, and asymptomatic (Table 2). The TMA values ranged from 7–13° in the varus direction, where 13° was approximately 2.5 standard deviations from our normative database mean.
Table 2.
Subject demographics
| Mean (SD) | |
|---|---|
| Age (years) | 23.6 (4.0) |
| Height (m) | 1.78 (0.09) |
| Weight (kg) | 76.9 (18.0) |
| Tibial Mechanical Axis | 9.9 (2.0) |
| KOOS-SR score | 0.2 (0.5) |
The primary variable of interest was the peak KEAM. On average, the peak KEAM occurred at 22% of stance, with a magnitude of 0.34 (SD 0.07) Nm/kgm. At the time of peak KEAM, the rearfoot was slightly dorsiflexed, everted, and abducted (Table 3). The knee was flexed, adducted and slightly externally rotated, and the hip was flexed, adducted, and slightly internally rotated.
Table 3.
Means (SD), correlation coefficients to peak KEAM, and correlation p-values for independent variables in this study
| Static Variable | Mean (SD) | r | p-value |
|---|---|---|---|
| Sit-to-Stand Δ in Arch Height Index | 0.020 (0.011) | 0.09 | 0.30 |
| Hip Abduction Strength (kg*m/BW) | 0.12 (0.02) | 0.20 | 0.12 |
| Distance b/n Medial Knee Joint Lines (mm) | 42.8 (24.2) | 0.64 | <0.001 |
| Tibial Mechanical Axis (°) | 9.9 (2.0) | 0.74 | <0.001 |
| Dynamic Variable (angle (°) at peak KEAM) | Mean (SD) | r | p-value |
| Ankle Frontal Plane (+ inversion) | −4.2 (2.7) | −0.60 | < 0.001 |
| Knee Frontal Plane (+ adduction) | 2.4 (4.6) | 0.68 | < 0.001 |
| Hip Frontal Plane (+ adduction) | 7.8 (2.6) | −0.14 | 0.20 |
The correlations between the static measures and the peak KEAM are presented in Table 3. There were significant positive correlations for TMA (r = 0.74) and DMJL (r = 0.64). There were no other significant relationships to the KEAM. In the final model of the stepwise multiple regression, TMA alone explained 53 percent of the variance in the peak KEAM (Table 4). No other static variable significantly increased the predictive strength of the model.
Table 4.
Final regression models for predicting the peak KEAM
| Dynamic predictor(s) | Adjusted R2 | R2 change | F change p-value | Model p-value |
|---|---|---|---|---|
| Frontal plane knee angle | 0.467 | --- | --- | <0.001 |
| Frontal plane knee angle + Frontal plane ankle angle | 0.533 | 0.066 | 0.036 | <0.001 |
| Static predictor(s) | Adjusted R2 | R2 change | F change p-value | Model p-value |
|---|---|---|---|---|
| Tibial mechanical axis | 0.532 | --- | --- | <0.001 |
| Static + Dynamic predictor(s) | Adjusted R2 | R2 change | F change p-value | Model p-value |
|---|---|---|---|---|
| Tibial mechanical axis | 0.532 | --- | --- | <0.001 |
| Tibial mechanical axis + Frontal plane knee angle | 0.591 | 0.059 | 0.019 | <0.001 |
For the dynamic measures, knee adduction angle was significantly correlated with the peak KEAM (r = 0.68). A significant correlation was also found for rearfoot eversion angle (r = 0.59). Hip adduction was weakly correlated to the peak KEAM. In the stepwise regression, knee adduction and rearfoot eversion angle significantly contributed to the model in the presence of each other (R2 = 0.53) (Table 4).
The final model combined all static and dynamic variables as predictors of variation in the peak KEAM. As a result, TMA and knee adduction angle were retained by the stepwise regression (R2 = 0.59). The remaining variables did not contribute to the final model.
The assumptions for regression analyses were reviewed following the analysis. The variance inflation ratio was between 1.00 and 2.00 depending on the model, suggesting the assumptions of no multicollinearity were met. Residual plot analysis did not reveal non-linearity or heteroscedasticity. Finally, inspection of the histogram and normal probability plots suggested the model residuals were normally distributed.
Discussion
The primary objective of this study was to investigate the relationships between static and dynamic measures of the lower extremity with dynamic knee joint loading. The KEAM magnitudes and waveforms were in line with previous works (Butler et al., 2009; Hurwitz et al., 2002). We expected frontal plane kinematics to be more closely related to the KEAM than the static clinical measures. The knee adduction and rearfoot eversion angle together created the strongest dynamic model to predict the KEAM. For the static measures, TMA alone was the best predictor of the KEAM. Surprisingly, both the static and dynamic measures explained similar amounts of variation in the peak KEAM.
The static variables with the strongest correlations to the KEAM were TMA and the DMJL. These two measures have been reported to be valid alternatives to radiographic knee alignment (Hinman et al., 2006). Not surprisingly, the correlation coefficient between these two measures (r = 0.81) was high in this study. However, DMJL demonstrated a slightly weaker correlation to the KEAM (r = 0.64) than TMA (r = 0.74). This may be a result of the distance measure being influenced by the alignment of both legs. The TMA, however, is a measure of the limb from which the KEAM was measured, which may explain the stronger relationship.
Isometric hip abduction strength was not correlated to the KEAM. Previously, Chang and colleagues (2004) found that a greater internal hip abduction moment, generated by the lateral hip muscles, was associated with a decreased risk for medial knee OA disease progression. However, they used an older OA population, which may have had weaker hip muscles. Thus, the requisite force production to sustain typical gait patterns may have been closer to maximal in these individuals, which may have increased the correlation between strength and moment. However, for a healthy individual, peak force production is not required of the lateral hip musculature during walking. Further exploration of our own data demonstrated no relationship between isometric hip strength and the peak frontal plane hip moment (r = 0.08). This lack of a relationship supports the findings of Fosang and Baker (2006), who suggested hip moments and strength are not strongly associated.
In terms of dynamics, knee adduction angle was significantly correlated with the KEAM, as expected. Similar findings have been noted in the medial knee OA population (Teixeira & Olney, 1996). However, we were surprised that this correlation was not stronger than that of TMA (a static measure) with KEAM. These results suggest that either measure could be equivocally used to predict medial knee loading. However, based on the moderate correlations, neither of these measures of frontal plane knee alignment completely account for the KEAM seen in these individuals. Other factors, such as muscle co-contraction of the medial hamstrings and medial gastrocnemius that increase compressive loads on the medial compartment, could contribute to this variance.
We believe that the significant correlation between rearfoot eversion and the KEAM is indicative of a compensatory mechanism. With an inclined tibia, as seen with varus knee alignment, the foot must evert to become plantigrade during stance. This motion may also provide a means to reduce medial joint loading, as increasing eversion with laterally wedged foot orthoses has been shown to reduce the KEAM (Butler et al., in press). Increased midfoot pronation might accomplish the same goal. However, arch flattening during sit-to-stand did not correlate well to the KEAM. If this measure could been taken during walking, excursions might be greater, potentially resulting in a stronger relationship with the KEAM.
The stepwise regression analysis using the static measures revealed that TMA alone was the best predictive model for determining variation in the KEAM (R2 = 0.53). Despite a high correlation with the KEAM, DMJL added very little unique predictive strength beyond that of TMA. This is likely because the measures were strongly correlated (r = 0.81). Thus, while either measure alone would suffice as a predictor of the KEAM, TMA would be the measure of choice.
During walking, knee adduction and rearfoot eversion together were moderately predictive of variation in the peak KEAM (R2 = 0.53). In the model, rearfoot eversion accounted for an additional 7% of the explained variation. As stated previously, this likely represents the compensatory mechanism of rearfoot eversion associated with varus alignment. On the other hand, knee adduction relates directly to the greater varus knee alignment and, consequently greater KEAM magnitude. The amount of variance explained by the dynamic model (53%) was the same as for the static model (53%). These findings suggest that TMA is as predictive of the KEAM as knee adduction during gait. As the latter requires collection of motion analysis data, the simple clinical measure of TMA might be preferred.
Finally, the combined model was found to be the most highly predictive of the models (R2 = 0.59). As all static and dynamic variables were entered into the stepwise regression, it is notable that the final model retained both a static and a dynamic predictor. In the model, knee adduction angle accounted for another 6% of the variation in the KEAM, in addition to TMA alone. This improvement in the model suggests that a dynamic measure of knee alignment can provide additional information about medial knee loading, beyond that of a static measure. However, it should be noted that the model improvement was modest, reinforcing the utility of TMA as a predictor of the KEAM.
Conclusions
In summary, understanding factors that influence dynamic knee joint loading in healthy knees may help us to identify risk factors that lead to OA. This, in turn, can lead to successful preventative strategies. Of the static and dynamic measures, TMA and knee adduction angle during gait, respectively, were the most predictive of medial knee joint loading. Comparatively, the static and dynamic models were equally predictive of the KEAM. The combination of TMA and knee adduction during gait together created the most robust model. These are important findings, as they suggest both that simple clinical tools can be used to predict knee joint loading, but that a dynamic assessment provides further improvement.
Acknowledgments
This study was supported by the Foundation for Physical Therapy, and National Institutes of Health shared instrumentation grant 1 S10 RR022396-01.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Contributor Information
Joaquin A. Barrios, 326 McKinly Lab, University of Delaware, Newark, DE 19716, USA, 302-831-4646, 301-831-4234 (fax), joaquin@udel.edu.
Jill S. Higginson, 201A Spencer Lab, University of Delaware, Newark, DE 19716, USA, 302-831-6622, higginson@udel.edu.
Todd D. Royer, 144 Rust Ice Arena, 541 South College Avenue, University of Delaware, Newark, DE 19716, USA, 302-831-4351, royer@udel.edu.
Irene S. Davis, 305 McKinly Lab, University of Delaware, Newark, DE 19716, USA, 302-831-4263, mcclay@udel.edu.
References (alphabetized)
- Andriacchi TP. Dynamics of knee malalignment. Orthop Clin North Am. 1994;25:395–403. [PubMed] [Google Scholar]
- Antonsson EK, Mann RW. The frequency content of gait. J Biomech. 1985;18(1):39–47. doi: 10.1016/0021-9290(85)90043-0. [DOI] [PubMed] [Google Scholar]
- Bennell KL, Creaby MW, Wrigley TV, Hunter DJ. Tibial subchondral trabecular volumetric bone density in medial knee joint osteoarthritis using peripheral quantitative computed tomography technology. Arthritis Rheum. 2008;58:2776–2785. doi: 10.1002/art.23795. [DOI] [PubMed] [Google Scholar]
- Bohannon R. Reference values for extremity muscle strength obtained by hand-held dynamometry from adults aged 20 to 79. Arch Phys Med Rehabil. 1997;78:26–31. doi: 10.1016/s0003-9993(97)90005-8. [DOI] [PubMed] [Google Scholar]
- Brouwer GM, van Tol AW, Bergink AP, Belo JN, Bernsen RMD, Reijman M, Pols HAP, Bierma-Zeinstra SMA. Association between valgus and varus alignment and the development and progression of radiographic osteoarthritis of the knee. Arthritis Rheum. 2007;56:1204–1211. doi: 10.1002/art.22515. [DOI] [PubMed] [Google Scholar]
- Butler RJ, Hillstrom H, Jong J, Richards CJ, Davis IS. Arch height index measurement system: establishment of reliability and normative values. J Am Podiatr Med Assoc. 2008;98:102–106. doi: 10.7547/0980102. [DOI] [PubMed] [Google Scholar]
- Butler RJ, Barrios JA, Royer T, Davis IS. Effect of laterally wedged foot orthoses on rearfoot and hip mechanics in patients with medial knee osteoarthritis. Prosthet Orthot Int. 2009;33:107–116. doi: 10.1080/03093640802613237. [DOI] [PubMed] [Google Scholar]
- Chang A, Hayes K, Dunlop D, Hurwitz D, Song J, Cahue S, Genge R, Sharma L. Thrust during ambulation and the progression of knee osteoarthritis. Arthritis Rheum. 2005;50:3897–3903. doi: 10.1002/art.20657. [DOI] [PubMed] [Google Scholar]
- Dearborn JT, Eakin CL, Skinne HB. Medial compartment arthrosis of the knee. Am J Orthop. 1996;25:18–26. [PubMed] [Google Scholar]
- Dempster WT, Gabel WC, Felts WJ. The anthropometry of the manual work space for the seated subject. Am J Phys Anthropol. 1959;17:289–317. doi: 10.1002/ajpa.1330170405. [DOI] [PubMed] [Google Scholar]
- Dillon CF, Rasch EK, Gu Q, Hirsch R. Prevalence of knee osteoarthritis in the United States: Arthritis data from the third National Health and Nutrition Survery 1991–94. J Rheumatol. 2006;33:2271–2279. [PubMed] [Google Scholar]
- Fosang A, Baker R. A method for comparing manual muscle strength measurements with joint moments during walking. Gait Post. 2006;24:406–411. doi: 10.1016/j.gaitpost.2005.09.015. [DOI] [PubMed] [Google Scholar]
- Grood ES, Suntay WJ. A joint coordinate system for the clinical description of three-dimensional motions: application to the knee. J Biomech Eng. 1983;105(2):136–144. doi: 10.1115/1.3138397. [DOI] [PubMed] [Google Scholar]
- Guccione AA, Felson DT, Anderson JJ, Anthony JM, Zhang YQ, Wilson PWF, Kellyhayes M, Wolf PA, Kreger BE, Kannel WB. The effects of specific medial conditions on the functional limitations of elders in the Framingham study. Am J Pub Health. 1994;84:351–358. doi: 10.2105/ajph.84.3.351. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hicks JL, Richards JG. Clinical applicability of using spherical fitting to find hip joint centers. Gait Post. 2005;22:138–145. doi: 10.1016/j.gaitpost.2004.08.004. [DOI] [PubMed] [Google Scholar]
- Hinman RS, May RL, Crossley KM. Is there an alternative to the full-length radiograph for determining knee joint alignment in osteoarthritis? Arthritis Rheum. 2006;55:306–313. doi: 10.1002/art.21836. [DOI] [PubMed] [Google Scholar]
- Hurwitz DE, Sumner DR, Andriacchi TP, Sugar DA. Dynamic knee loads during gait predict proximal tibial bone distribution. J Biomech. 1998;31:423–430. doi: 10.1016/s0021-9290(98)00028-1. [DOI] [PubMed] [Google Scholar]
- Jackson BD, Teichtahl AJ, Morris ME, Wluka AE, Davis SR, Cicuttini FM. The effect of the knee adduction moment on tibial cartilage and bone size in healthy women. Rhuematology. 2004;43:311–314. doi: 10.1093/rheumatology/keh002. [DOI] [PubMed] [Google Scholar]
- Miyazaki T, Wada M, Kawahara H, Sato M, Baba H, Shimada S. Dynamic load at baseline can predict radiographic disease progression in medial compartment knee osteoarthritis. Ann Rheum Dis. 2002;61:617–622. doi: 10.1136/ard.61.7.617. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mundermann A, Dyrby CO, D’Lima DD, Colwell CW, Jr, Andriacchi TP. In vivo knee loading characteristics during activities of daily living as measured by an instrumented total knee replacement. J Orthop Res. 2008;26:1167–1172. doi: 10.1002/jor.20655. [DOI] [PubMed] [Google Scholar]
- Murphy L, Schwartz TA, Helmick CG, Renner JB, Tudor G, Koch G, Dragomir A, Kalsbeek WD, Luta G, Jordan JM. Lifetime risk of symptomatic knee osteoarthritis. Arthritis Rheum. 2008;59:1207–1213. doi: 10.1002/art.24021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roos EM, Roos HP, Lohmander LS, Ekdahl C, Beynnon BD. Knee Injury and Osteoarthritis Outcome Score (KOOS) -- development of a self-administered outcome measure. J Orthop Sports Phys Ther. 1998;28:88–96. doi: 10.2519/jospt.1998.28.2.88. [DOI] [PubMed] [Google Scholar]
- Sharma L, Song J, Felson DT, Cahue S, Shamiyeh E, Dunlop DD. The role of knee alignment in disease progression and functional decline in knee osteoarthritis. J Am Med Assoc. 2001;286:188–195. doi: 10.1001/jama.286.2.188. [DOI] [PubMed] [Google Scholar]
- Tamari K, Tinley P, Aoyagi K. Gender and age-related differences in axial alignment of the lower limb among healthy Japanese volunteers. J Jpn Phys Ther Assoc. 2003;6:25–34. doi: 10.1298/jjpta.6.25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Teixeira LF, Olney SJ. Relationship between alignment and kinematic and kinetic measures of the knee of osteoarthritic elderly subjects in level walking. Clin Biomech. 1996;11:126–134. doi: 10.1016/0268-0033(95)00057-7. [DOI] [PubMed] [Google Scholar]
- Tillman MD, Bauer JA, Cauraugh JH, Trimble MH. Differences in lower extremity alignment between males and females—potential predisposing factors for knee injury. J Sports Med Phys Fitness. 2005;45:355–359. [PubMed] [Google Scholar]
- Wada M, Maezawa Y, Baba H, Shimada S, Sasaki S, Nose Y. Relationships among bone mineral densities, static alignment and dynamic load in patients with medial compartment knee osteoarthritis. Rheumatology. 2001;40:499–505. doi: 10.1093/rheumatology/40.5.499. [DOI] [PubMed] [Google Scholar]
- Williams DS, McClay IS. Measurements used to characterize the foot and the medial longitudinal arch: reliability and validity. Phys Ther. 2000;80:864–871. [PubMed] [Google Scholar]
- Zhao D, Banks SA, Mitchell KH, D’Lima DD, Colwell CW, Fregly BJ. Correlation between the knee adduction torque and medial contact force for a variety of gait patterns. J Orthop Res. 2007;25:789–797. doi: 10.1002/jor.20379. [DOI] [PubMed] [Google Scholar]