

Abstract
Introduction:
Asthmatic inflammation is responsible for vital features of the disease, including bronchial hyperresponsiveness (BHR). At present we do not have precise markers for monitoring asthmatic inflammation. C-reactive protein (CRP), a marker of systemic inflammation, seemed to be a factor which could also reflect the level of asthmatic inflammation expressed by BHR. Therefore the relationship between CRP concentration and BHR was evaluated.
Materials and Methods:
One hundred and two patients entered the study. A skin prick test with a broad spectrum of common aeroallergens as well as baseline spirometry and a histamine bronchoprovocation test were performed in each subject. Blood samples for high-sensitivity CRP (hsCRP) measurement were taken before the bronchial challenge tests.
Results:
Serum hsCRP concentrations ranged from 0.20 to 14.5 mg/l (median: 1.2 mg/l, 25–75% quartiles: 0.6–2.4). Positive skin prick tests were found in 26 subjects. Bronchial hyperresponsiveness was confirmed in 42 patients (first subgroup), while 60 subjects did not demonstrate BHR (second subgroup). Among the patients with BHR, asthma was diagnosed in 33 cases and Corrao syndrome in 9. In both subgroups, serum hsCRP concentrations had similar levels (median: 1.4 mg/l, 25–75% quartiles: 0.8–2.4 and median: 0.9 mg/l, 25–75% quartiles: 0.5–2.8, respectively; p=0.297). There was no statistically significant correlation (r= −0.163, p=0.302) between serum hsCRP concentration and the level of BHR expressed as the 20% provocative concentration for histamine. In addition, hsCRP serum concentration, after adjustment for age, atopy, body mass index, and gender, was not a significant predictor of positive histamine bronchoprovocation test results (p=0.22, OR=0.86, 95% CI).
Conclusions:
Serum hsCRP concentration is not a good marker of BHR, which is mainly dependent on asthmatic inflammation and is measured during bronchial challenge with histamine. This finding is important for interpreting and discussing results obtained from epidemiological and population-based studies on relationships between either CRP concentration and BHR or local and systemic inflammation.
Keywords: asthmatic inflammation, asthma, Corrao syndrome, BHR, high-sensitivity CRP, systemic inflammation
Introduction
Bronchial hyperresponsiveness (BHR) is a crucial attribute of asthma. It is due to chronic asthmatic inflammation and may reflect the level of the inflammatory process [16]. Direct airway challenge with histamine or metacholine discloses BHR, expressed as the 20% provocative concentration (PC20) value, and is also used for assessing the potential anti-inflammatory effects of treatment with new agents. However, using PC20 for histamine which reflects the BHR level, though priceless in the diagnosis of asthma, is not valuable in monitoring asthmatic inflammation. Airway challenge with histamine is accompanied by discomfort to the patient and sometimes produces life-threatening situations; moreover, it is expensive and time consuming for medical staff. Other means of assessing airway inflammation in asthma, such as the evaluation of many markers in induced sputum (cytokines, eosinophils) [6, 22], bronchoalveolar lavage [5, 10], or exhaled air (NO, CO) [13, 16, 18], share the same inconveniences as the determination of BHR. On the other hand, convincing data show that bronchial asthma treatment developed on the basis of inflammatory premises is more effective than treatment which considers the classical British Thoracic Society recommendations [6].
Recent publications suggest that C-reactive protein (CRP) could be taken into consideration as a simple, cheap, and reliable marker for monitoring asthmatic inflammation [8, 9, 17]. If this hypothesis was true, there should be a noticeable interrelationship between CRP and some BHR indices such as direct airway challenges results. Theoretically, CRP should not exist in a healthy organism, but even minimal exciting factors including age, body mass index (BMI), gender, smoking and variability of blood pressure in normotensive patients may either trigger or bias trace amount of CRP production [1]. Therefore, a CRP concentration of <5 mg/l is accepted as the normal value. The normal median concentration of CRP is 0.8 mg/l, with 90% of apparently healthy individuals having a value less than 3 mg/l and 99% less than 12 mg/l. It is produced by the liver at a higher concentration when the organism is challenged by a significant inflammatory stimulus, such as endotoxins from the membranes of Gram-negative bacteria inhaled into the bronchial tree of asthmatic patients [14]. It is well known that CRP increases during infection and autoimmune disturbances [20]. Much attention has been focused lately on CRP in cardiovascular diseases, such as chronic heart failure [26], ischemic heart disease [12], arrhythmia [2], and atherosclerosis [27]. Especially interesting are publications pointing to CRP as a marker which may have prognostic value in ischemic heart attack [3] and irregularity of rhythm [11].
The main question concerns the relationships between local asthmatic inflammation, mediated by Th2 CD4+ lymphocytes, and systemic inflammation, which depends on Th1 CD4+ lymphocytes. At present, very little is known about this, but it must be realized that such relationships, even complex ones, exist and one segment of the immune response influences another, also resulting in CRP production [25]. Interesting experimental data suggest that CRP may inhibit local inflammatory effects and also protect against Th2-mediated reactions [21]. Being aware of these relationships, as well as the circumstances, we developed this study using a purely clinical model to determine whether CRP may be a marker of asthmatic inflammation, expressed by BHR, and thus be useful in monitoring this process and predicting asthma severity and exacerbation.
Materials and Methods
Study participants
The study group consisted of 102 patients, 29 male and 73 female aged 16–74 years (average: 38.9±14.8 years), who were admitted to our department with the suspicion of asthma or Corrao syndrome. All subjects enrolled in the study were free of any medication for at least two weeks before the trial and were steroid naive and nonsmokers. Precise clinical evaluation allowed exclusion of chronic inflammatory and systemic diseases, particularly those of pulmonary, cardiovascular, or autoimmune origin. Anamnesis and detailed physical examination did not reveal any abnormalities, and particularly blood pressure and heart rate were within the normal ranges. X-ray images of the nasal sinuses and chest as well as computed tomography, performed in some cases, did not display changes in the upper and lower airways and lungs. Any uncertainty in a diagnosis was explained by means of bronchoscopy. Electrocardiography tracings and echocardiography did not demonstrate heart rhythm disturbances, heart failure, or pulmonary hypertension. There were no disturbances in erythrocyte sedimentation rate, blood cell count, the concentrations of glucose, uric acid, or blood lipids, and the partial pressure of blood gases. In particular cases, serologic evaluation was undertaken to evaluate rheumatoid factor and anti-DNA antibodies, which were negative. Detailed demographic data and spirometric values are shown in Table 1. The study was approved by the local ethics committee (Wrocław Medical University, decision No. KB-396/2005).
Table 1.
Demographic data, spirometric values, and hsCRP serum concentrations in the entire sample and subgroups with and without BHR
| Age (years) χ¯±SD | Male/female n | Weight (kg) χ¯±SD | Height (cm) χ¯±SD | FVC (%) χ¯±SD | FEV1 (%) χ¯±SD | BMI χ¯±SD | CRP (mg/l) Me 25–75% | PC20 (mg/ml) χ¯±SD | |
|---|---|---|---|---|---|---|---|---|---|
| Demographic data, spirometric, and CRP values: entire sample (n=102) | 38.9±14.8 | 29/73 | 70.7±13.6 | 166.6±10.2 | 102.0±13.1 | 102.5±14.8 | 25.4±4.4 0.6−2.4 | 1.2 | 7.1±6.7 |
| Positive test result (n=42) | 44.8±15.6 | 8/34 | 70.2±11.0 | 164.2±7.9 | 101.0±13.3 | 101.3±14.6 | 26.1±4.5 | 1.4 0.8−2.4 | 7.1±6.7 |
| Negative test result (n=60) | 34.8±12.8 | 21/39 | 71.1±15.3 | 168.3±11.2 | 102.7±13.1 | 103.3±15.0 | 24.9±4.3 | 0.9 0.5−2.8 | |
| p=0.0006* | p=0.125** | p=0.769* | p=0.047* | p=0.526* | p=0.503* | p=0.184* | p=0.297*** |
* Calculated by Student's t-test, ** calculated by χ¯-squared-test, *** calculated by Mann-Withney U-test.
χ¯-Arithmetic mean, SD-standard deviation, Me-median, 25–75% quartiles.
Study design
In each subject a skin prick test with a broad spectrum of common aeroallergens as well as baseline spirometry and a histamine bronchoprovocation test were performed. Blood samples for high-sensitivity CRP (hsCRP) measurement were taken from the subjects before the challenge test with histamine. For measurements of pulmonary functions, an Alfa spirometer (Vitalograf) was used. Each spirometric parameter was recorded in triplicate and the best value of the lung function test was taken for further analysis. ACCS criteria were used for estimating predicted values. BHR was determined by the histamine bronchoprovocation test according to the European Respiratory Society guidelines [19]. The tidal breathing method was used. Histamine was administered through a de Vilbis nebulizer in progressive concentrations of 0.125, 0.250, 0.5, 1, 2, 4, 8, and 16 mg/ml. The test was stopped when FEV1 had fallen by 20% or more. A positive histamine test was defined as a decrease in FEV1 of at least 20%, and then the results were expressed as the PC20. Serum hsCRP concentrations were determined by an immunoturbidimetric assay with amplification of latex molecules on an Integra 400 analyzer (Roche).
Statistical analysis
Data were statistically analyzed with Statistica software version 6.0 (SN:AXXP412B401322AR14). To compare factors between groups, the Student's t-test, the Mann-Whitney test, and the χ-squared test were used. The interrelationship between serum hsCRP concentrations and PC20 values was assessed by Spearman’s rank correlation coefficient; p values <0.05 were considered significant.
Results
Serum CRP concentrations in the entire sample ranged from 0.20 to 14.5 mg/l, (median: 1.2 mg/l, 25–75% quartiles: 0.6–2.4; Table 1). Positive skin-prick tests with allergen expressing one of the features of atopy were found in 26 subjects.
Among the 102 participants, 42 had positive histamine bronchoprovocation test results (first subgroup) and 60 patients (second subgroup) did not present BHR (Table 1). Among the patients with BHR, asthma was diagnosed in 33 cases and its variant, characterized by coughing (Corrao syndrome), in 9 participants of this subgroup. There were no significant differences between the two subgroups in both baseline spirometric parameters and gender distribution. The patients with BHR were significantly older than those with negative bronchoprovocation results (44.8±15.6 and 34.8±12.8 years, respectively; p=0.0006).
In both subgroups, serum CRP concentrations were on a similar level (median: 1.4 mg/l, 25–75% quartiles: 0.8–2.4 and median: 0.9 mg/l, 25–75% quartiles: 0.5–2.8; p=0.297; Fig. 1). There was no statistically significant correlation (r= −0.163, p=0.302) between serum CRP concentration and the level of BHR, expressed as the PC20 value (Fig. 2).
Fig. 1.
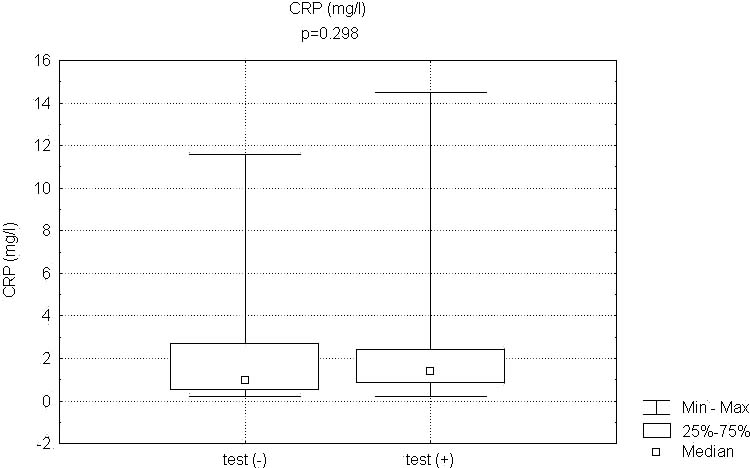
CRP serum concentration in patients with negative (n=60) and positive (n=42) bronchoprovocation test results.
Fig. 2.
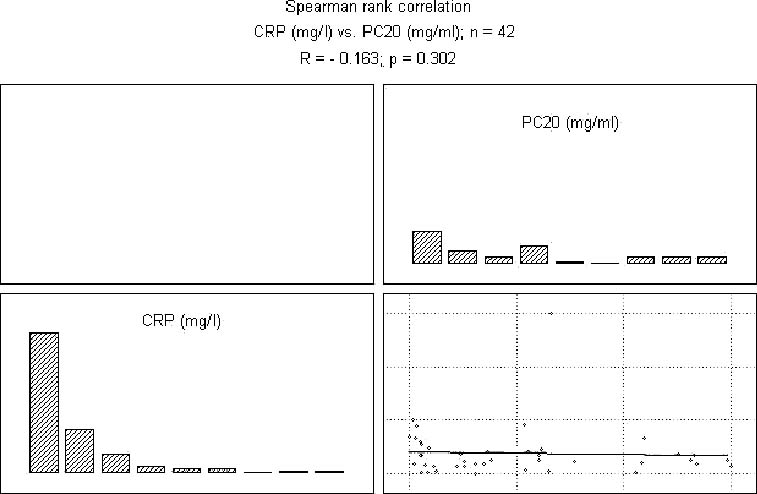
Spearman's rank correlation between CRP serum concentration and histamine PC20 value in patients with positive bronchoprovocation test result (n=42).
Logistic regression analysis showed that hsCRP serum concentration after adjustment for age, atopy, BMI, and gender cannot be considered a significant predictor of positive histamine bronchoprovocation test results (p=0.22, OR=0.86; 95% CI).
Discussion
The test data of this study definitely indicate that the serum concentration of hsCRP is not associated with asthmatic inflammation expressed by BHR and cannot be taken into consideration as a marker of the local inflammatory process in either atopic or non-atopic asthma. Multivariate analyses showed that this result was also independent of potential confounding factors such as age, BMI, and gender. The validity of these results are based on a purely clinical experiment and, to our knowledge, this is the first such attempt to evaluate the usefulness of measuring CRP concentration in monitoring asthmatic inflammation. The importance of our test data increases in light of a few very interesting publications, mainly of an epidemiological nature [17] and population-based studies [8, 9], which could suggest the possibility that serum CRP concentration may reflect the level of bronchial inflammation in asthma, so it could be a simple, cheap, and easy to perform test for a clinical evaluation of the disease.
Among these studies is an elegant work on a population-based study by Kony et al. [9] which revealed an association between a higher frequency of BHR and higher CRP levels in study participants which could reflect local inflammation within the bronchi. In our study, hsCRP concentration in serum did not differ in patients with and without BHR (Table 1, Fig. 1). In addition, no significant correlation was found between hsCRP and BHR (Fig. 2). All these data, seemingly contradictory, may arise from a fascinating and unknown link between local and systemic inflammation in asthma, which was also emphasized by the authors of that article. The methodology used in our study excluded events of systemic inflammation in the study participants; thus we can conclude that increasing CRP concentration does not depend on asthmatic inflammation in this link. This does not mean that sensitive systemic inflammation markers other than CRP, such as serum amyloid-A and plasma fibrinogen, could be significantly associated with asthma prevalence, as shown in a study by Jousilahti et al. [8]. However, the authors demonstrated these results in a population-based study, which is a correct pattern to show relationships between systemic inflammation markers and asthma prevalence, but it does not seem to be a good model to display linkage between asthmatic and systemic inflammation.
Other interesting data were developed as a multicenter epidemiological study by Ólafsdottir et al. [17], who revealed that hsCRP concentration increases in patients with non-allergic asthma, but not in allergic asthma. The study demonstrated, however, no significant relationships between CRP, atopy, and BHR, which is as yet an indispensable feature of non-allergic asthma as well. The lack of association between CRP and BHR is in accordance with our observation; however, we did not show any significant difference when comparing atopic and non-atopic subjects (Table 1). An epidemiological study can show many valuable relationships concerning hsCRP concentration and respiratory symptoms, non-allergic asthma, and atopy, but under these circumstances, that many clinical and inflammatory factors may change the natural history of asthma. Besides BMI, smoking, age, and gender, these relationships may arise from atherosclerosis [27], many cardiovascular abnormalities [2, 12, 26], or hidden inflammatory processes which may coexist with asthma in a population-based study. Non-allergic asthma, which has the same immune pathological basis as the allergic type of the disease, substantially differs from allergic asthma at the origin of the inflammatory process [15], which probably depends on bacteria [7], viral infection [24], unknown allergen [4], or auto-allergen [23]. Systemic inflammation could thus be a reason for the CRP concentration increase in non-allergic asthma.
The study by Szalai et al. [21] was of special interest to us as it suggested that an increase in CRP concentration may accompany the acute phase of allergic inflammation. This phenomenon may occur as a secondary reaction connected with a CRP ability to stimulate the expression of anti-inflammatory cytokine-10, which down-regulates the activity of the Th2 lymphocyte population. This observation may be an inspiration to develop a study on the significance of CRP concentration as a marker of allergic asthma exacerbation. Our study results clearly showed that hsCRP serum concentration in asthma did not correlate with BHR which, in turn, indirectly suggests its poor relationship with asthmatic inflammation. It should also be underlined that all our patients represented a subpopulation of newly diagnosed asthma without any significant concomitant diseases. Therefore we speculate that the increase in CRP concentration reported among a proportion of asthmatics in epidemiological and population-based studies might result from other conditions coexisting with chronic asthma.
References
- 1.Abramson J. L., Lewis C., Murrah N. V., Anderson G. T. and Vaccarino V. (2006): Relation of C-reactive protein and tumor necrosis factor-alpha to ambulatory blood pressure variability in healthy adults. Am. J. Cardiol., 98, 649–652. [DOI] [PMC free article] [PubMed]
- 2.Anderson J. L., Allen Maycock C. A., Lappe D. L., Crandall B. G., Horne B. D., Bair T. L., Morris S. R., Li Q. and Muhlestein J. B. (2004): Frequency of elevation of C-reactive protein in atrial fibrillation. Am. J. Cardiol., 94, 1255–1259. [DOI] [PubMed]
- 3.Bazzino O., Ferreiros E. R., Pizarro R. and Corrado G. (2001): C-reactive protein and the stress tests for the risk stratification of patients recovering from unstable angina pectoris. Am. J. Cardiol., 87, 1235–1239. [DOI] [PubMed]
- 4.Bottcher M. F., Bjurstrom J., Mai X. M., Nilsson L. and Jenmalm M. C. (2003): Allergen-induced cytokine secretion in atopic and non-atopic asthmatic children. Pediatr. Allergy Immunol., 14, 345–350. [DOI] [PubMed]
- 5.Fal A. M., Dobek R., Liebhart J., Panaszek B. and Małolepszy J. (2004): Complex assessment of differential cell count in bronchoalveolar lavage fluid as a distinction criterion between asthma and chronic obstructive pulmonary disease. Adv. Clin. Exp. Med., 13, 67–71.
- 6.Green R. H., Brightling C. E., McKenna S., Hargadon B., Parker D., Bradding P., Wardlaw A. J. and Paword I. D. (2002): Asthma exacerbations and sputum eosinophil counts: a randomised controlled trial. Lancet, 360, 1715–1721. [DOI] [PubMed]
- 7.Herz U., Ruckert R., Wollenhaupt K., Tschernig T., Neuhaus-Steinmetz U., Pabst R. and Renz H. (1999): Airway exposure to bacterial superantigen (SEB) induces lymphocyte-dependent airway inflammation associated with increased airway responsiveness — a model for non-allergic asthma. Eur. J. Immunol., 29, 1021–1031. [DOI] [PubMed]
- 8.Jousilahti P., Salomaa V., Hakala K., Rasi V., Vahtera E. and Palosuo T. (2002): The association of sensitive systemic inflammation markers with bronchial asthma. Ann. Allergy Asthma Immunol., 89, 381–385. [DOI] [PubMed]
- 9.Kony S., Zureik M., Driss F., Neukirch C., Leynaert B. and Neukirch F. (2004): Association of bronchial hyperresponsiveness and lung function with C-reactive protein (CRP): a population based study. Thorax, 59, 892–896. [DOI] [PMC free article] [PubMed]
- 10.Liebhart J., Cembrzynska-Nowak M., Bienkowska M., Liebhart E., Dobek R., Zaczyńska E., Panaszek B., Obojski A. and Małolepszy J. (2002): Relevance of the selected cytokine release (TNF-alpha, IL-6, IFN-gamma, and IFN-alpha) to the exacerbation of bronchial asthma from airway mycotic infections. Predominant role of IFN-alpha? J. Investig. Allergol. Clin. Immunol., 12, 182–191. [PubMed]
- 11.Lo B., Fijnheer R., Nierich A. P., Bruins P. and Kalkman C. J. (2005): C-reactive protein is a risk indicator for atrial fibrillation after myocardial revascularization. Ann. Thorac. Surg., 79, 1530–1535. [DOI] [PubMed]
- 12.Lowe G. D., Sweetnam P. M., Yarnell J. W., Rumley A., Rumley C., Bainton D. and Ben-Shlomo Y. (2004): C-reactive protein, fibrin D-dimer, and risk of ischemic heart disease: the Caerphilly and Speedwell studies. Arterioscler. Thromb. Vasc. Biol., 24, 1957–1962. [DOI] [PubMed]
- 13.Maskey-Warzęchowska M., Przybyłski T. and Hildebrand K. (2004): The influence of asthma and COPD exacerbation on exhaled nitric oxide (FENO). Pneumonol. Alergol. Pol., 72, 181–186. [PubMed]
- 14.Michel O., Ginanni R., Le Bon B., Content J., Duchateau J. and Sergysels R. (1992): Inflammatory response to acute inhalation of endotoxin in asthmatic patients. Am. Rev. Respir. Dis., 146, 352–357. [DOI] [PubMed]
- 15.Nieves A., Magnan A., Boniface S., Proudhon H., Lanteaume A., Romanet S., Vervolet D. and Godard P. (2005): Phenotypes of asthma revisited upon the presence of atopy. Respir. Med., 99, 347–354. [DOI] [PubMed]
- 16.Nogami H., Shoji S. and Nishima S. (2003): Exhaled nitric oxide as a simple assessment of airway hyperresponsiveness in bronchial asthma and chronic cough patients. J. Asthma, 40, 653–659. [DOI] [PubMed]
- 17.Ólafsdottir I. S., Gislason T., Thjodleifsson B., Olafsson Í., Gislason D., Jögi R. and Janson C. (2005): C reactive protein levels are increased in non-allergic but not in allergic asthma: a multicentre epidemiological study. Thorax, 60, 451–454 [DOI] [PMC free article] [PubMed]
- 18.Ramirez M., Garcia-Rio F., Vinas A., Prados C., Pino J. M. and Villamor J. (2004): Relationship between exhaled carbon monoxide and airway hyperresponsiveness in asthmatic patients. J. Asthma, 41, 109–116. [DOI] [PubMed]
- 19.Sterk P. J., Fabbri L. M., Quanjer P. H., Cockroft D. W., O'Byrne P. M., Anderson S. D., Juniper E. F. and Malo J. L. (1993): Standardized challenge testing with pharmacological physical and sensitizing stimuli in adults. Report working party standardization of lung function tests. European Community for Steal and Coal. Official statement of the European Respiratory Society. Eur. Respir. J., 6(suppl.), 1653–1683. [PubMed]
- 20.Szalai A. J. (2004): C-reactive protein (CRP) and autoimmune disease: facts and conjectures. Clin. Dev. Immunol., 11, 221–226. [DOI] [PMC free article] [PubMed]
- 21.Szalai A. J., Nataf S., Hu X. Z. and Barnum S. R. (2002): Experimental allergic encephalomyelitis is inhibited in transgenic mice expressing human C-reactive protein. J. Immunol., 168, 5792–5797. [DOI] [PubMed]
- 22.Taha R. A., Laberge S., Hamid Q. and Olivenstein R. (2001): Increased expression of the chemoattractant cytokines eotaxin, monocyte chemotactic protein-4, and interleukin-16 in induced sputum in asthmatic patients. Chest, 120, 595–601. [DOI] [PubMed]
- 23.Tedeschi A., Comi A.L., Lorini M., Tosini C. and Miadonna A. (2005): Autologous serum skin test reactivity in patients with non-allergic asthma. Clin. Exp. Allergy, 35, 849–853. [DOI] [PubMed]
- 24.Trigg C. J., Nicholson K. G., Wang J. H., Ireland D. C., Jordan S., Duddle J. M., Hamilton S. and Davies R. J. (1996): Bronchial inflammation and the common cold: a comparison of atopic and non-atopic individuals. Clin. Exp. Allergy, 26, 665–676. [DOI] [PMC free article] [PubMed]
- 25.Weidinger S., Klopp N., Rummler L., Wagenpfeil S., Baurecht H. J., Gauger A., Darsow U., Jakob T., Ollert M., Behrendt H., Wichmann H. E., Ring J. and Illig T. (2005): Association of CARD15 polymorphisms with atopy-related traits in a population-based cohort of Caucasian adults. Clin. Exp. Allergy, 35, 866–872. [DOI] [PubMed]
- 26.Yin W. H., Chen J. W., Jen H. L., Chiang M. C., Huang W. P., Feng A. N., Young M. S. and Lin S. J. (2004): Independent prognostic value of elevated high-sensitivity C-reactive protein in chronic heart failure. Am. Heart J., 147, 931–938. [DOI] [PubMed]
- 27.Zureik M., Kony S., Neukirch C., Courbon D., Leynaert B., Vervloet D., Ducimetiere P. and Neukirch F. (2004): Bronchial responsiveness to methacholine is associated with increased common carotid intima-media thickness in men. Arterioscler. Thromb. Vasc. Biol., 24, 1098–1103. [DOI] [PubMed]