

Abstract
Maltreatment places children at risk for psychiatric morbidity, especially conduct problems. However, not all maltreated children develop conduct problems. We tested whether the effect of physical maltreatment on risk for conduct problems was strongest among those who were at high genetic risk for these problems using data from the E-risk Study, a representative cohort of 1,116 5-year-old British twin pairs and their families. Children's conduct problems were ascertained via parent and teacher interviews. Physical maltreatment was ascertained via parent report. Children's genetic risk for conduct problems was estimated as a function of their co-twin's conduct disorder status and the pair's zygosity. The effect of maltreatment on risk for conduct problems was strongest among those at high genetic risk. The experience of maltreatment was associated with an increase of 2% in the probability of a conduct disorder diagnosis among children at low genetic risk for conduct disorder but an increase of 24% among children at high genetic risk. Prediction of behavioral pathology can attain greater accuracy if both pathogenic environments and genetic risk are ascertained. Certain genotypes may promote resistance to trauma. Physically maltreated children whose first-degree relatives engage in antisocial behavior warrant priority for therapeutic intervention.
Maltreatment poses severe risks to children's health and development and is increasingly coming to the attention of primary care clinicians and other community professionals (Cicchetti & Manly, 2001; Sedlak & Broadhurst, 1996). A major consequence of maltreatment in early childhood is antisocial behavior (Dodge, Bates, & Pettit, 1990; Lansford, Dodge, Pettit, Bates, Crozier, & Kaplow, 2002; Smith & Thornberry, 1995; Widom, 1989; Widom & Maxfield, 2001). Such early-onset antisocial behavior is, in turn, associated with life-long and pervasive mental (Moffitt, Caspi, Harrington, & Milne, 2002), physical (Farrington, 1995), economic (Caspi, Wright, Moffitt, & Silva, 1998), and interpersonal (Moffitt et al., 2002) problems that create an enormous public-health burden (Potter & Mercy, 1997).
However, not all maltreated children develop conduct problems (Widom, 1997), and some maltreated children exhibit adaptive functioning (Cicchetti, Rogosch, Lynch, & Holt, 1993) that is still evident in adulthood (McGloin & Widom, 2001). Very little systematic evidence is available to explain why children show such marked variation in their response to maltreatment. Such variability would be observed if there were genetically influenced individual differences in susceptibility to environmental experiences like maltreatment, a concept referred to as “gene–environment interaction” (GxE; Kendler & Eaves, 1986; Rutter & Silberg, 2002). The GxE concept is familiar to clinicians as the “host–pathogen interaction” in a patient's vulnerability or resistance to disease (Evans & Relling, 1999; Hill, 1999) and to developmentalists as the “diathesis–stress” interaction in an individual's vulnerability or resistance to pathogenic experiences (Monroe & Simons, 1991). In this article, we test the hypothesis that children's conduct problems emerge when genetically vulnerable children encounter family environments in which they are maltreated. That many children are not at genetic risk for conduct problems may explain, in part, why the experience of maltreatment does not always result in the development of conduct problems.
To analyze GxE with real precision, one must specify both the environmental risk and the genotype. Although twin studies of antisocial behavior have shown that genetic factors influence early-emerging conduct problems (Arseneault, Moffitt, Caspi, Taylor, Rijsdijk, Jaffee, Ablow, & Measelle, 2003; van den Oord, Verhulst, & Boomsma, 1996; van der Valk, Verhulst, Neale, & Boomsma, 1998), functional genes for these problems have yet to be reliably identified. There are some promising candidates (Rowe, 2001), and one study has reported that a monoamine oxidase A (MAOA) polymorphism is associated with severe antisocial behavior in the presence of childhood maltreatment in a New Zealand sample of males (Caspi, McClay, Moffitt, Mill, Martin, Craig, Taylor, & Poulton, 2002). However, for a complex trait like antisocial behavior, genetic risk is likely to involve multiple genes (Plomin & Crabbe, 2000) that interact with experiences such as maltreatment to influence children's development.
If, as is currently the case, the actual, multiple genes are unknown, data from monozygotic (MZ) and dizygotic (DZ) twin pairs can be used to study the interplay between genetic and environmental risks. The goal of the current study was to determine whether children's genetic risk for conduct disorder exacerbated the effect of physical maltreatment on their conduct problems and we used the twin design to test this hypothesis.
When data are collected on twins, a child's genetic risk for disorder can be estimated as a function of his or her co-twin's diagnostic status and the pair's zygosity (Andrieu & Goldstein, 1998; Kendler & Kessler, 1995; Ottman, 1994). These analyses are premised on the testable assumption that the disorder of interest is heritable, meaning that evidence is required to establish that genes partly account for individual differences in the disorder. Because MZ twins share 100% of their genes, it can be inferred that a child's genetic risk for the disorder is high if his or her MZ co-twin has a diagnosis of disorder and low if his or her MZ co-twin does not have a diagnosis of disorder. That is, if a disorder is genetically influenced and a child's MZ co-twin is diagnosed with the disorder, then that child must share all of the susceptibility genes for disorder. In contrast, DZ twins share only half their genes, on average. Thus, if a child's DZ co-twin has a diagnosis of disorder, then the child's genetic risk of disorder is high, but not as high as for MZ twins because the child may not share the susceptibility genes with his or her co-twin. If a child's DZ co-twin does not have a diagnosis of disorder, then that child's genetic risk for disorder is low, but not as low as for MZ twins because the child may have inherited susceptibility genes for disorder while his or her co-twin did not. Therefore, MZ and DZ twins can be placed along a continuum of genetic risk as a function of their co-twins' diagnostic status. A child's genetic risk is highest if his or her co-twin has a diagnosis of disorder and the pair are MZ and a child's genetic risk is lowest if his or her co-twin does not have a diagnosis of disorder and the pair are MZ. DZ twins' genetic risk falls intermediate to these two groups.
In assessing the interplay between genetic risk for conduct problems and physical maltreatment, we examined correlations and interactions between genetic risk for conduct problems and physical maltreatment. Evidence for a gene–environment (GE) correlation would be observed if those at higher levels of genetic risk were more likely to be maltreated. Evidence of GxE would be observed if the effect of physical maltreatment on conduct problems varied as a function of genetic risk (Kendler & Eaves, 1986).
Method
The Environmental Risk (E-Risk) Study sample
Participants are members of the E-Risk Longitudinal Twin Study, which investigates how genetic and environmental factors shape children's development. The study follows an epidemiological sample of families with young twins who were interviewed in the home when the twins were ages 5 and 7 years. The E-Risk sampling frame was two consecutive birth cohorts (1994 and 1995) in the Twins' Early Development Study, a birth register of twins born in England and Wales (Trouton, Spinath, & Plomin, 2002). The full register is administered by the government's Office of National Statistics, which invited parents of all twins born in 1994 and 1995 to enroll. Of the 15,906 twin pairs born in these 2 years, 71% joined the register. Our sampling frame excluded opposite-sex twin pairs and began with the 73% of register families who had same-sex twins.
The E-Risk Study sought a sample size of 1,100 families to allow for attrition in future years of the longitudinal study while retaining statistical power. An initial list of families was drawn from the register to target for home visits, with a 10% oversample to allow for non-participation. The probability sample was drawn using a high-risk stratification strategy. High-risk families were those in which the mother had her first birth when she was 20 years of age or younger. We used this sampling (a) to replace high risk families who were selectively lost to the register via nonresponse, and (b) to ensure sufficient base rates of problem behaviors given the low base rates expected for 5-year-old children. Early first childbearing was used as the risk-stratification variable because it was recorded for virtually all families in the register, it is relatively free of measurement error, and it is a known risk factor for children's problem behaviors (Maynard, 1997; Moffitt & E-Risk Study Team, 2002). The sampling strategy resulted in a final sample in which two-thirds of study mothers accurately represented all mothers in the general population (ages 15–48 years) in England and Wales in 1994–1995 (estimates derived from the General Household Survey; Bennett, Jarvis, Rowlands, Singleton, & Haselden, 1996). The other one-third of study mothers (younger only) constituted a 160% oversample of mothers who were at high risk based on their young age at first birth (ages 15–20 years). To provide unbiased statistical estimates that could be generalized to the population of British families with children born in the 1990s, we corrected the data reported in this article with weighting to represent the proportion of maternal ages in that population (Bennett et al., 1996).
Of the 1,203 eligible families, 1,116 (93%) participated in home-visit assessments when the twins were 5 years old, forming the base sample for the study. Four percent of families refused and 3% were lost to tracing or could not be reached after many attempts. With parents' permission, questionnaires were mailed to the children's teachers, and teachers returned questionnaires for 94% of cohort children. Written informed consent was obtained from mothers. The E-Risk Study has received ethical approval from the Maudsley Hospital Ethics Committee.
Zygosity was determined with a standard zygosity questionnaire, which has been shown to have 95% accuracy (Price, Freeman, Craig, Petrill, Ebersole, & Polmin, 2000). Ambiguous cases were zygosity-typed using DNA. The sample includes 56% MZ and 44% DZ twin pairs. Gender is evenly distributed within zygosity (49% male).
Data were collected within 120 days of the twins' fifth birthday. Research workers visited each home for 2.5–3 hr in teams of two. While one interviewed the mother, the other tested the twins in sequence in a different part of the house. Families were given shopping vouchers for their participation, and children were given books and stickers. All research workers had university degrees in behavioral science, and experience in psychology, anthropology, or nursing. Each research worker completed a formal 15-day training program on either the mother interview protocol or the child assessment protocol, to attain certification to a rigorous reliability standard.
Measures
Physical maltreatment was assessed separately for each twin by interviewing mothers with the standardized clinical interview protocol from the Multisite Child Development Project (Dodge et al., 1990; Dodge, Pettit, Bates, & Valente, 1995; Lansford et al., 2002). We interviewed mothers instead of ascertaining cases from Child Protective Service registers for three reasons. First, official record data identify only a small proportion of cases, which may be a biased, unrepresentative subset (Walsh, McMillan, & Jamieson, 2002; Widom, 1988). Second, because of time delays in detection, investigation, and legal proceedings against perpetrators, official record data sources tend not to record children as confirmed cases until older ages and the children in our sample were 5-year-olds. Third, searching child protection records for this sample would have required parental consent, placing record data at the same potential risk of parental concealment as mothers' reports.
The interview protocol was designed by Dodge and colleagues (1990, 1995; Lansford et al., 2002) to enhance mothers' comfort with reporting valid physical maltreatment information, while also meeting researchers' legal and ethical responsibilities for reporting. Under the UK Children Act (Department of Health, 1989), our responsibility was to secure intervention if maltreatment was current and ongoing. At the start of the interview about discipline and physical maltreatment, the interviewer explained to the mother that if she reported maltreatment that had occurred in the child's first 4 years and was not ongoing, that information could remain confidential. However, if she reported maltreatment that occurred in the year prior to the interview and the risk to the child was ongoing, the Study would be under legal obligation to assist the family to get help. Thus, when mothers gave informed consent to proceed with the interview they understood that a report of recent, ongoing maltreatment would constitute a request for help (if the maltreatment was not already known to authorities). The interview did not ask directly about the timing of incidents, and therefore mothers who wished to report maltreatment while avoiding intervention could have opted to describe maltreatment as happening in the past. There was a need to intervene on behalf of 15 families. We found that almost all current cases of maltreatment were already known to government home health visitors, the family's general practitioner, or child protection teams, although very few of the cases had been officially registered.
The protocol included standardized probe questions such as, “When (name) was a toddler, do you remember any time when s/he was disciplined severely enough that s/he may have been hurt?” and “Did you worry that you or someone else (such as a babysitter, a relative or a neighbor) may have harmed or hurt (name) during those years?” (1% of mothers declined to answer the questions). Because these questions followed an interview on normative disciplinary practices (including questions about corporal punishment), mothers understood that these questions about harm did not refer to ordinary spanking or slapping. Mothers were not asked specifically about neglect, psychological abuse, or sexual abuse (although several cases of sexual abuse were reported in response to our questions about harm). So that mothers might feel more willing to report that a child had been maltreated, questions were carefully worded to avoid implying that the mother was the perpetrator. In cases where mothers reported any maltreatment, interviewers probed mothers for details about the incident and recorded notes. Interviewers coded the likelihood that the child had been maltreated based on the mothers' narrative. This classification showed intercoder agreement on 90% of ratings (κ = .56) in our sample and in the Child Development Project (Dodge, Pettit, & Bates, 1994; Dodge et al., 1995). The 10% of codes that disagreed tended to reflect uncertainty about whether physical maltreatment was “probable” or “definite.” Based on the mother's report of the severity of discipline, her concern that someone else might have harmed the child, and the interviewer's rating of the likelihood that the child had been maltreated, children were coded as having not been, possibly been, or definitely been physically maltreated. Examples of possible maltreatment in our sample (N = 273 children) included instances where the mother reported that she smacked the child harder than intended and left a mark or bruise, or cases where social services were contacted by schools, neighbors, and/or family members out of concern that the child was being physically maltreated. Examples of definite maltreatment included children who were beaten by a teenaged step-sibling, punished by being burnt with matches or thrown against doors, had injuries (e.g., fractures or dislocations) from neglectful or abusive care, or were formally registered with a social services child protection team. The prevalence of such definite, serious maltreatment as defined in this sample was 1.5% (N = 34 children). For the purposes of our analyses, the physical maltreatment variable was recoded into a dichotomous variable representing children who experienced no maltreatment (unweighted, the prevalence was 86%; weighted to represent the population it was 88%) versus a combined group of children who experienced possible or definite physical maltreatment (unweighted, the prevalence was 14%; weighted to represent the population it was 12%). The prevalence of physical maltreatment was similar among MZ (11%) and DZ (14%) twins. Our combined prevalence of 12% resembles the 15% prevalence estimate reported by Dodge and colleagues (Dodge et al., 1990) whose measurement protocol we used. Our prevalence rate of 1.5% for definite physical maltreatment is consistent with physical abuse estimates of 1.5 and 2.6% from population surveys in North America (Bland & Orn, 1986; Egami, Ford, Greenfield, & Crum, 1996).
The physical maltreatment interview protocol has (a) good concurrent validity as evidenced by correlations above .60 with mothers' reports of their child-directed aggression using the Conflict Tactic Scales (Dodge et al., 1990; Straus & Gelles, 1988); (b) good interreporter reliability as evidenced by a correlation of .60 between mothers' and fathers' reports in 396 couples (Dodge et al., 1995); and (c) good predictive validity as evidenced by significant 12-year prediction from preschool maltreatment to outcomes in Grade 11, including increased violence, school absenteeism, anxiety and depressive symptoms, and posttraumatic stress disorder symptoms, controlling for a variety of social and family risk factors (Lansford et al., 2002).
The same set of questions about physical maltreatment was asked individually about each twin, and the interviews about each twin were separated by 1.5 hr of questions on other topics. In those families in which at least one twin was maltreated, both twins suffered physical maltreatment in 63% of cases and only one twin suffered maltreatment in 37% of cases.
Children's conduct problems were assessed with the Achenbach family of instruments (Achenbach, 1991a, 1991b). The Aggression and Delinquency Scales were supplemented with the American Psychiatric Association (APA) Diagnostic and Statistical Manual of Mental Disorders—4th Edition (DSM-IV; APA, 1994) items assessing conduct and oppositional defiant disorder. Mother and teacher reports of conduct problems correlated .29 (p ≤ .001), which is typical of interrater agreement about behavioral problems (Achenbach, McConaughy, & Howell, 1987). Mother and teacher reports of children's conduct problems were summed. Scores ranged from 0 to 130 (M = 21.17, SD = 16.27). The internal consistency of the combined score was .94.
Child conduct disorder
To assess child conduct problems in the clinical range, we derived diagnoses of conduct disorder on the basis of the above mentioned mothers' and teachers' reports. Fourteen of 15 DSM-IV (APA, 1994) symptoms of conduct disorder were assessed (forced sex was age inappropriate), covering fighting, bullying, lying, stealing, cruelty to people or animals, vandalism, and rule violations. A child was considered to have a given symptom if either the mother or the teacher scored the symptom as being very true or often true of the child over the past 6 months. We counted a symptom as present if there was evidence of it from either source, following evidence that this approach enhances diagnostic validity (Bird, Gould, & Staghezza, 1992; Piacentini, Cohen, & Cohen, 1992). Symptom counts ranged from 0 to 11 (M = 0.47, SD = 1.20). Consistent with DSM-IV criteria, children with three or more symptoms were assigned a diagnosis of conduct disorder (unweighted, the prevalence of conduct disorder in the sample was 8.5%; weighted to represent the population, it was 6.6%). Within this group, a smaller number of children had five or more symptoms and met criteria for severe conduct disorder (unweighted prevalence = 3.4%, weighted to represent the population, it was 2.5%).
Genetic risk was computed by selecting one twin from each twin pair as the “target twin” and the second twin as the “co-twin.” Each twin pair was represented in the data set twice, first with the elder twin as the target and the younger twin as the co-twin, and second with the younger twin as the target and the elder twin as the co-twin. A continuum of genetic risk was computed as a function of zygosity and the co-twin's conduct disorder status. This method has been used to estimate the combined effects of genetic risk for depression and negative life events on risk for major depressive disorder (Kendler & Kessler, 1995). The co-twin's conduct disorder status combined with information on the pair's zygosity provides a good index of genetic risk because several twin studies have shown that the heritability of young children's conduct problems is moderate to high in magnitude (see Arseneault et al., 2003). Combining information on the co-twin's conduct disorder status with information on the pair's zygosity, the target twin's genetic risk was highest if his or her MZ co-twin had a diagnosis of conduct disorder (5%; n = 104). The target twin's genetic risk was lower if his or her DZ co-twin had a diagnosis of conduct disorder (4%; n = 85). The target twin's genetic risk was lower still if his or her DZ co-twin did not have a diagnosis of conduct disorder (40%; n = 903). Finally, the target twin's genetic risk was lowest if his or her MZ co-twin did not have a diagnosis of conduct disorder (51%; n = 1140). Genetic risk was coded on a 0–3 ordinal scale, with 0 representing lowest risk and 3 representing highest risk.
Results
Because our twin study included two children from each family, observations of children's behavior were nonindependent. As such, we analyzed the data using standard regression techniques but with all tests based on the sandwich or Huber/White variance estimator (Rogers, 1993; Williams, 2000), a method available in STATA 7.0. (StataCorp, 2001). Application of this technique adjusts estimated standard errors and therefore accounts for the dependence in the data due to analyzing sets of twins. Although all of the estimates in this results section were statistically penalized to correct for the nonindependence of observations from children in the same family, we reran all analyses, selecting one child at random as the target twin from each twin pair. The results reported below were unchanged (available upon request).
Establishing the validity of the genetic risk index
Heritability of children's conduct problems
For the logic of our genetic risk index, it was important to demonstrate that individual differences in diagnoses of conduct disorder among the young children in this sample were genetically influenced. Supporting this assumption, Table 1 shows that twin correlations for the conduct problems scale and for diagnoses of conduct disorder were approximately twice as high among MZ compared to DZ twins. Maximum likelihood estimation techniques were used to decompose the variance in the children's conduct problems and diagnoses of conduct disorder into that which could be accounted for by latent additive genetic (A), shared environmental (C), and nonshared environmental (E) factors (Neale & Cardon, 1992) and to test whether genetic influences on children's conduct problems and diagnoses of conduct disorder were statistically significant. The goal of fitting different structural equations to twin data is to account for the observed covariance structure using the most parsimonious number of parameters. To compare the fit of different models, we used two model-selection statistics. The first was the chi-square goodness of fit statistic. Large values indicate poor model fit to the observed covariance structure. When two models are nested (i.e., identical with the exception of constraints placed on the submodel), the difference in fit between them can be evaluated with the chi-square difference, using as its degrees of freedom (df) the df difference from the two models. When the chi-square difference is not statistically significant, the more parsimonious model is selected, as the test indicates that the constrained model fits equally well with the data. The second model-selection statistic was the root mean square error of approximation, which is an index of the model discrepancy, per degree of freedom, from the observed covariance structure (MacCallum, Browne, & Sugawara, 1996). Values less than 0.05 indicate close fit and values less than 0.08 indicate fair fit to the data (Browne & Cudeck, 1993).
Table 1. Conduct problem mean scores, standard deviations, and correlations as a function of zygosity and estimates of genetic and environmental influences on conduct problems.
| MZ | DZ | Correlations | Population Variance Attributable | RMSEA | χ2 (df) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | MZ | DZ | A | C | E | ||||||||
| Conduct problem scale scores | ||||||||||||||||
| Full ACE model | 21.28 | 16.86 | 21.05 | 15.56 | .75*** | .30*** | 0.72 | 0.60–0.75 | 0.00 | 0.00–0.11 | 0.28 | 0.25–0.32 | 0.070 | 9.56 (3) | ||
| A = 0 | — | 0.56 | 0.52–0.61 | 0.44 | 0.39–0.48 | 0.232 | 99.80 (4) | 90.24*** | ||||||||
| Proportion | ||||||||||||||||
| Conduct disorder | ||||||||||||||||
| Full ACE model | 6.3% | 7.1% | .54a,*** | .27a,*** | 0.58 | 0.19–0.90 | 0.25 | 0.00–0.59 | 0.17 | 0.10–0.28 | 0.00 | 0.56 (3) | ||||
| A = 0 | — | 0.72 | 0.62–0.80 | 0.28 | 0.20–0.38 | 0.041 | 9.58 (4) | 9.02*** | ||||||||
Note: A, additive genetic factors; C, shared environmental factors; E, nonshared environmental factors or measurement error; RMSEA, root mean square error of approximation; , χ2 difference statistic.
Phi coefficient, estimated as a square root (χ2/N).
p ≤ .001.
Table 1 presents the results of the maximum likelihood models of genetic and environmental influences on children's conduct problems. The first row presents the results of the full model in which all genetic and environmental influences on children's continuously distributed conduct problems were estimated. The model shows that genetic factors accounted for 72% of the variance, with shared and nonshared environmental factors accounting for the remainder. In the second row of the table, we tested whether genetic influences on children's conduct problems were significant by comparing the fit of the full model to a model in which the genetic effect was hypothesized to be zero. The fit of the reduced model in which genetic factors were hypothesized to have no effect on children's conduct problems was significantly worse than the fit of the full model, , p ≤ .001. Thus, genetic factors do account for significant variation in children's continuously distributed conduct problems. The third and fourth rows of Table 1 present parallel results for children's diagnosed conduct disorder. As shown in the third row, genetic factors accounted for 58% of the variation in children's diagnosed conduct disorders, with shared and nonshared environmental factors accounting for the remainder. The fourth row presents the model in which the effect of genetic factors was hypothesized to be zero. The reduced model fit significantly worse than the full model, , p ≤ .001, indicating that genetic effects on children's diagnosed conduct disorder were statistically significant. Thus, both conduct problem phenotypes are highly heritable in 5-year-old children and these estimates are consistent with estimates from other samples of young children, as reviewed by Arseneault and colleagues (2003).
Zygosity differences in exposure to maltreatment
For the logic of our genetic risk index, it was important to ensure that zygosity differences in exposure to maltreatment could not account for observed differences among the genetic risk groups on our outcome measures. MZ and DZ twins did not differ in the odds of having been physically maltreated (odds ratio [OR] = 1.27; 95% confidence interval [CI] = 0.90–1.80). There was little indication that MZ twins' greater genetic similarity made them more concordant than DZ twins for exposure to maltreatment. The pairwise concordance calculates the proportion of pairs in which both twins were physically maltreated using the formula C/(C + D), where C is the number of concordant pairs and D is the number of discordant pairs (i.e., pairs in which only one twin was maltreated). The pairwise concordance for MZ twins was 66% and the pairwise concordance for DZ twins was 60%. Other work with our sample has established that physical maltreatment is an environmental risk factor that is largely uncorrelated with genetic factors (Jaffee, Caspi, Moffitt, & Taylor, 2004). Among the children who were maltreated, the proportion who experienced definite maltreatment was 13% if their MZ co-twin did not have a diagnosis of conduct disorder (lowest risk) and also 13% if their MZ co-twin did have a diagnosis of conduct disorder (highest risk). Thus, the severity of maltreatment among children who were physically maltreated was similar across high and low genetic risk.
Zygosity differences in conduct problems
For the logic of the genetic risk index, it was also important to ensure that zygosity differences in the prevalence of conduct problems could not account for observed differences among the genetic risk groups on our outcome measures. Recall that the two highest genetic risk groups comprise MZ and DZ twin pairs in which the co-twin has a diagnosis of conduct disorder. The two lowest genetic risk groups comprise MZ and DZ pairs in which the co-twin does not have a diagnosis of conduct disorder. If, for example, conduct disorder was more prevalent among MZ than DZ twins, the two highest genetic risk groups would disproportionately comprise MZ twin pairs (because more MZ than DZ co-twins would have a diagnosis of conduct disorder). The two lowest genetic risk groups would disproportionately comprise DZ twin pairs (because more DZ than MZ co-twins would lack a diagnosis of conduct disorder). As a result, any zygosity differences on the outcome might be mistakenly interpreted as differences among the genetic risk groups. Ordinary least squares (OLS) regression analyses showed that MZ and DZ twins did not differ on the mean number of conduct problems reported by their mothers and teachers (b = −.22, β = −.007, SE = 0.88, p = .80; Table 1). Logistic regression analyses showed that MZ and DZ twins did not differ in the odds of having a conduct disorder diagnosis (OR = 1.14; 95% CI = 0.77–1.68). Having shown that conduct problems are heritable and that MZ and DZ twins have similar levels of conduct problems and exposure to physical maltreatment, we have established the legitimacy of the genetic risk index.
Testing GE interplay
To determine whether genetic risk for conduct problems was significantly associated with having been maltreated, GE correlations were estimated using point biserial correlations and chi-square tests (Table 2). We found a small GE correlation: genetic risk for conduct disorder was weakly related to physical maltreatment (r = .15, p ≤ .001). A logistic regression analysis revealed that the effect of genetic risk on physical maltreatment did not differ as a function of sex (OR = 0.97, SE = 0.20, p = .89).
Table 2. Percentage and number of physically maltreated children by genetic risk.
| Maltreated | |
|---|---|
| Highest risk: MZ co-twin has diagnosis of CD | 34.6% (n = 36) |
| High risk: DZ co-twin has diagnosis of CD | 24.7% (n = 21) |
| Low risk: DZ co-twin does not have diagnosis of CD | 14.2% (n = 128) |
| Lowest risk: MZ co-twin does not have diagnosis of CD | 10.7% (n = 122) |
Note: CD, conduct disorder.
χ2 (3) = 46.39, p ≤ .001.
We also found evidence of GxE. To assess GxE on children's continuously distributed conduct problems, we conducted an OLS regression analysis in which physical maltreatment and genetic risk were entered at the first step and the interaction between physical maltreatment and genetic risk was entered at the second step. The OLS regression analysis of continuously distributed conduct problems showed that having been maltreated (b = 7.33, β = .15, SE = 1.24, p ≤ .001), and high genetic risk (b = 6.21, β = .27, SE = 0.73, p ≤ .001), were both associated with elevated levels of conduct problems. In addition, the inter action between genetic risk and physical maltreatment was significant (b = 4.32, β = .11, SE = 1.61, p ≤ .01).1 Figure 1a shows that the effect of having been maltreated on conduct problems was stronger at high levels of genetic risk than at low levels of genetic risk. Figure 1b and 1c demonstrates the Genetic Risk × Physical Maltreatment interaction using mother and teacher reports of children's conduct problems, respectively, as the dependent variables in the model.
Figure 1.
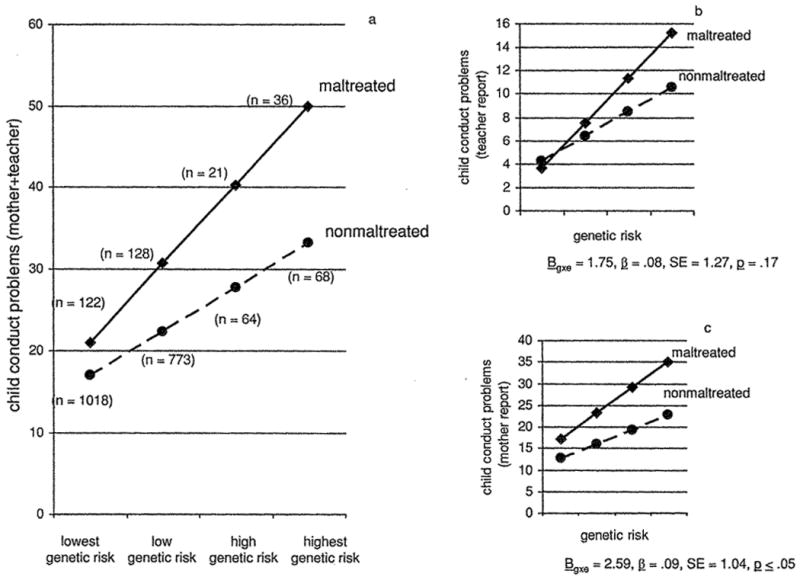
Child conduct problems as a function of genetic risk and physical maltreatment.
We examined whether the GxE interaction was different for boys and girls by testing the three-way interaction between genetic risk, physical maltreatment, and sex (after testing all main effects and two-way interactions in a hierarchical regression analysis). The Genetic Risk × Maltreatment interaction did not differ for boys and girls (b = 4.23, β = .09, SE = 3.00, p = .16).
The Genetic Risk × Maltreatment interaction clearly showed that physical maltreatment exacerbated the effect of genetic risk on children's conduct problem symptoms. We next tested whether the GxE effect would extend to children's diagnosable conduct disorder. To assess GxE on children's conduct disorder, we conducted a logistic regression analysis in which physical maltreatment and genetic risk were entered at the first step and the interaction between physical maltreatment and genetic risk was entered at the second step. The dependent variable is the natural logarithm of the odds (or log odds) of a conduct disorder diagnosis. Of interest is the probability that an individual with given genetic risk and experience of physical maltreatment will have a diagnosis of conduct disorder. The probability of being diagnosed with conduct disorder is a function of the log odds where
where P is the probability, CD is conduct disorder, x represents predictors such as genetic risk and physical maltreatment, and B is the effects of the predictors (DeMaris, 1993). Although the logistic model is additive in the scale of the log odds, the effect of a given predictor variable (e.g., genetic risk) on the probability of some outcome (e.g., a conduct disorder diagnosis) is not constant across different levels of genetic risk, and is also a function of all other predictors in the model (DeMaris, 1993). Thus, the main effects in a logistic regression model will automatically capture ordinal interactions wherein the magnitude of the effect of a predictor variable like genetic risk will differ over high versus low levels of genetic risk and as a function of other predictors, such as physical maltreatment. When the dependent variable is scaled in terms of the probability of a conduct disorder diagnosis, the formal interaction term in the logistic model tests for disordinal (i.e., crossover) interactions or for a greater than expected degree of ordinal interaction. We note that a disordinal interaction was not predicted and would not be consistent with the diathesis stress model.
The logistic regression analysis showed that having been maltreated (OR = 2.22; 95% CI = 1.53–3.21, p ≤ .001), and high genetic risk (OR = 3.67; 95% CI = 2.76–4.88, p ≤ .001), both increased the odds of a diagnosis of conduct disorder. In the scale of the log odds, the Genetic Risk × Physical Maltreatment interaction was not significant (OR = 1.12; 95% CI = 0.65–1.94, p = .68).2 However, our interest is not in the odds of a conduct disorder diagnosis, but rather in the probability of a diagnosis given a particular level of genetic risk and experience of physical maltreatment. Figure 2 plots the predicted probability of a conduct disorder diagnosis as a function of genetic risk and physical maltreatment. At the lowest level of genetic risk, physical maltreatment was associated with an increase of 1.6% in the probability of a conduct disorder diagnosis (from 1.9 to 3.5%). At the highest level of genetic risk, physical maltreatment was associated with an increase of 23.5% in the probability of a conduct disorder diagnosis (from 46.1 to 69.6%).3
Figure 2.
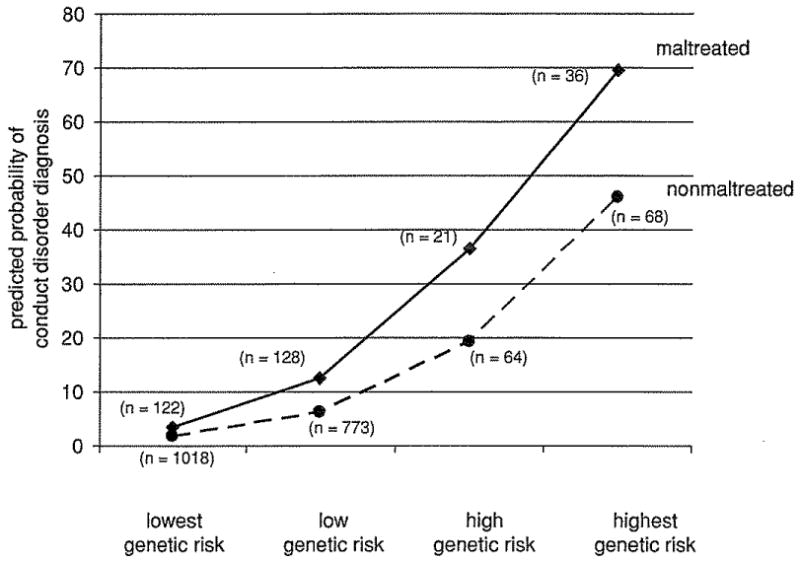
The predicted probability of a conduct disorder diagnosis as a function of genetic risk and physical maltreatment.
Discussion
Conduct problems, particularly those emerging in early childhood, are linked to a range of adverse outcomes in adolescence and young adulthood (Moffitt et al., 2002). Our findings showed that such early-onset conduct problems were most likely to emerge when genetically vulnerable children were maltreated. The Genetic Risk × Physical Maltreatment interaction was associated with a clear and significant elevation in conduct problem symptoms. However, evidence was somewhat weaker that Gene × Environment interactions predicted conduct problems severe enough to meet diagnostic criteria, although the same pattern of results obtained regardless of whether the conduct problem scale or the diagnosis was the focus of analysis. Because power was modest to detect interaction effects on small diagnostic groups, we nevertheless found it illustrative to present the findings with respect to the conduct disorder diagnosis.
Physical maltreatment was only weakly associated with conduct problems among children who were at low genetic risk for conduct disorder, suggesting the protective role of genotype on children's risk for conduct problems. This finding is consistent with evidence from a New Zealand cohort of adults showing that a genotype conferring high levels of MAOA activity protects men with a childhood history of maltreatment from developing antisocial problems in adulthood (Caspi et al., 2002), and that a childhood history of maltreatment did not predict risk for depression among individuals who had the long version of the serotonin transporter gene (5-HTTLPR; Caspi, Sugden, Moffitt, Taylor, Craig, Harrington, McClay, Mill, Martin, Braithwaite, & Poulton, 2003). We parallel those findings in our UK cohort of 5-year-old children, extending the results to account for the possibility that many genes will be involved in the development of conduct problems. These findings of gene–environment interplay suggest that purely environmental etiological theories of children's conduct problems are incomplete, as are deterministic genetic accounts. Prediction of behavioral pathology can attain greater accuracy if both pathogenic environments and genetic risk are ascertained.
It is not likely that genes code directly for aggression or conduct problems. Rather, high-versus low-risk genotypes may moderate the effects of physical maltreatment by influencing those factors that have been implicated in the link between maltreatment and child conduct problems, such as neuroendocrine functioning (Cicchetti & Rogosch, 2001; De Bellis, 2001), cognitive processing (Dodge et al., 1995; McGee, Wolfe, & Olson, 2001) and emotion recognition (Pollak, Cicchetti, Hornung, & Reed, 2000; Pollak & Sinha, 2002). The present study, documenting a GxE interaction, suggests that some genotypes may increase children's sensitivity to environmental adversities such as physical maltreatment, whereas other genotypes may promote children's resistance to trauma. This study and others (Bennett, Lesch, Heils, Long, Lorenz, Shoaf, Champoux, Suomi, Linnoila, & Higley, 2002; Caspi et al., 2002, 2003; Suomi, 2002) suggest that genes may not influence behavior disorders directly, but, in some complex disorders, genes may act to influence people's susceptibility or resistance to stressful environmental experiences. If this reconceptualization of the role of genes is correct, then the search for the specific genes related to multifactorial behaviors like conduct problems will be aided by testing for GE interplay rather than assuming a direct gene–disorder correspondence (Hamer, 2002). As an aid to the interpretation of GxE findings, researchers will need to ensure that the environmental risk in question is not genetically mediated. That is, putative environmental risk factors may be associated with a given outcome because heritable characteristics of the child provoke an environmental response, or because the parents who provide a child's rearing environment are the same ones who provide the child's genotype. When genes and environments are highly correlated, what researchers identify as a GxE interaction may in fact represent a gene–gene interaction, where the putative environmental risk is, in fact, a marker for genetic risk. Other work in our sample has established that the effect of physical maltreatment on children's conduct problems is not strongly genetically mediated (Jaffee et al., 2004). Thus, we can be confident that our findings represent a true GxE interaction.
Limitations
This study has a number of limitations. First, without a measured genotype we cannot be certain that each child who was assumed to be at high genetic risk for conduct disorder was, in fact, so. Moreover, because children in the sample have not yet passed through the age of risk for conduct disorder, some children whose siblings will go on to earn a diagnosis may have been misclassified in the low genetic risk groups. However, such misclassification would have exerted a conservative influence on our findings by making it more difficult to detect differences as a function of high versus low genetic risk.
Second, because our group of physically maltreated children was small in numbers, it was not possible to compare subtypes of maltreatment or to compare groups according to severity, chronicity, perpetrator, or precise developmental period of maltreatment. Although all cases of maltreatment were necessarily confined to the infancy–toddlerhood and preschool years, the effects of genetic risk may be moderated by specific characteristics of maltreatment (Barnett, Manly, & Cicchetti, 1993). We could, however, assume that definite cases were relatively more severe cases and check whether definite versus possible maltreatment was distributed similarly across children in the higher versus lower genetic risk groups. As reported in the Results, the prevalence of definite maltreatment among children who were maltreated was identical (13%) in the highest and lowest genetic risk groups. A fuller picture of GE interplay in the context of maltreatment is likely to emerge when the dimensions of maltreatment can be operationalized with greater complexity (Cicchetti et al., 2001; Manly, Cicchetti, & Barnett, 1994; Manly, Kim, Rogosch, & Cicchetti, 2001).
Third, it is possible that some mothers, despite our best efforts to make it possible for them to report physical maltreatment, concealed maltreatment or did not report it because they were unaware that their child had been maltreated. Any underreporting should have exerted a conservative influence on our findings, however, by causing us to place physically maltreated children in the nonmaltreated group. Moreover, the fact that mothers reported on children's experience of maltreatment as well as children's conduct problems means that shared informant variance might have accounted, in part, for our findings of Gene × Environment interaction. However, we reduced the effects of shared informant variance by combining mothers' and teachers' reports of children's conduct problems and by demonstrating that the pattern of Gene × Environment interaction was similar when mother and teacher reports of child conduct problems were analyzed separately compared to when they were combined, although it must be noted that the Genetic Risk × Physical Maltreatment interaction failed to reach conventional significance levels when the teacher data alone were used.
Fourth, it is possible that data from twins will not generalize to singletons. However, the proportion of twins who were physically maltreated is similar to the prevalence in a US study of singletons that used the same method of ascertaining maltreatment (Dodge et al., 1994, 1995), and twins and singletons do not differ in mean levels of conduct problems (Simonoff, Pickles, Meyer, Silberg, Maes, Loeber, Rutter, Hewitt, & Eaves, 1997; van den Oord, Koot, Boomsma, Verhulst, & Orleveke, 1995).
Fifth, a clearer demonstration of GxE using a twin design would be one in which the twins were separated for adoption and reared apart. However, such separations are rare in the general population and adoption agencies screen prospective adopting parents carefully, making it highly unlikely that twins (or singletons) will experience physical maltreatment after adoption (Stoolmiller, 1999). The advantage of the adoption design with respect to detecting GxE is that it ensures the independence of genetic and environmental risk factors (the notable exception being when children's heritable characteristics provoke a response from the environment). Thus, it bears noting that our findings of GE interplay are consistent with findings from adoption studies showing that genes and environments interact to promote antisocial behavior, although these studies did not specifically measure maltreatment as an environmental risk factor (Cadoret, Cain, & Crowe, 1983; Cadoret, Yates, Troughton, Woodworth, & Stewart, 1995).
Sixth, in two-thirds of the families in which there was physical maltreatment, both twins were reported to have been maltreated. It is possible that in these twin pairs, the co-twin's conduct disorder (on which the genetic risk index is based) might have been caused by the experience of maltreatment and not, as the risk index assumes, by a genetic predisposition to conduct problems. An analysis of twin pairs who are discordant for the experience of maltreatment would be a stronger test of GxE, as it would ensure that if the target twin had been maltreated, the co-twin (on whom the genetic risk index is based) would not have been. Unfortunately, we did not have sufficient power to test for GxE using only discordant twin pairs, as the number of physically maltreated children whose co-twin was not maltreated was too small (from lowest to highest genetic risk, the n's were 28, 32, 5, and 4). However, the pattern of plotted results was consistent with those in Figure 1a.
Clinical relevance
Because genetic risk for conduct disorder predicts early-emerging conduct problems, particularly in conjunction with maltreatment, knowledge of a family history of antisocial behavior may be used to help understaffed and underresourced child protective services to prioritize cases within their heavy caseloads. An absence of any family history of antisocial behavior may be one indicator that a maltreated child is at relatively low risk for conduct problems. It remains possible, however, that these children will be at high risk for other adverse outcomes like anxiety or depression.
Early interventions show promise for preventing child conduct problems that arise, in part, from abusive experiences. For example, an evaluation of a nurse home-visitation program found that fewer children in the nurse-visited group were abused relative to comparison children (Olds, Eckenrode, Henderson, Kitzman, Powers, Cole, Sidora, Morris, Pettitt, & Luckey, 1997). Moreover, those children in the nurse-visited group who were abused did not have more conduct problems than their nonabused, nurse-visited peers because the intervention prevented abuse from becoming persistent (Eckenrode, Zielinski, Smith, Marcynyszyn, Henderson, Kitzman, Cole, Powers, & Olds, 2001). The current study suggests that nurse home-visitation programs might become most cost beneficial if aimed at children having one or more biological parents with a history of offending or antisocial personality disorder. Such parents are at increased risk of maltreating their children (Jaffee, in press). Although maltreatment increases children's risk for conduct problems beyond that associated with a parent's history of antisocial behavior (Jaffee et al., 2004), parents' antisocial behavior may serve as a marker for children's genetic risk and for families who should be targeted for inclusion in prevention programs. Although our findings suggest that maltreated children who are at the highest genetic risk will comprise a small fraction of maltreated children overall, knowledge of a family history of antisocial behavior will help to screen for children who are highly likely to develop severe conduct problems.
Acknowledgments
We are grateful to the Study mothers and fathers, the twins, and the twins' teachers for their participation. Our thanks to Robert Plomin for his contributions; to Thomas Achenbach for generous permission to adapt the CBCL; to Tom Price for comments on earlier drafts of this manuscript; to Hallmark Cards for their support; and to members of the E-Risk team for their dedication, hard work, and insights. The E-Risk Study is funded by Medical Research Council Grant G9806489. Terrie Moffitt is a Royal Society–Wolfson Research Merit Award holder.
Footnotes
The combined mother and teacher report of children's conduct problems was positively skewed. Although OLS regression estimates are robust to skew in the dependent variable when sample sizes are as large as ours (Lumley, Diehr, Emerson, & Chen, 2002), skew can result in the detection of spurious GxE interactions (Martin, 2000). To address this concern, the conduct problems distribution was normalized via a square root transformation (M = 4.27, SD = 1.71, skew = .35, kurtosis = 3.33). The Physical Maltreatment × Genetic Risk interaction remained a significant predictor of the normalized conduct problems distribution (b = .33, β = .08, SE = 0.13, p ≤ .05).
The reason for the nonsignificant interaction in the logistic regression model can be demonstrated by examining the odds ratios in the lowest and highest genetic risk groups. Having been maltreated increased the odds of a conduct disorder diagnosis by 2.24 times in the lowest genetic risk group (95% CI = 1.04–4.78; p ≤ .05) and by 4.27 times in the highest genetic risk group (95% CI = 1.41–12.89; p ≤ .05). The overlapping confidence intervals around these odds ratios suggest that they do not differ significantly.
The logistic regression model tests for interaction on the multiplicative scale for the binary variables (e.g., conduct disorder diagnosis). In addition to the logistic regression analysis, we reestimated the model testing for the interaction between genetic risk and physical maltreatment on an additive scale, using a risk difference model (binomial regression with identity link; Hardin & Hilbe, 2001). This analysis was performed using BINREG in Stata (StataCorp, 2001). The results indicated that the Genetic Risk × Maltreatment interaction was statistically significant (RD = .09, 95% CI = .04–.15), indicating that the difference in the rate of conduct disorder between the maltreated and nonmaltreated groups varied as a function of genetic risk. We also conducted an OLS regression analysis in which we regressed the conduct disorder diagnosis on physical maltreatment, genetic risk, and the Genetic Risk × Maltreatment interaction. This analysis yielded significant main effects of physical maltreatment (b = .07, β = .09, SE = 0.02, p ≤ .001), genetic risk (b = .12, β = .33, SE = 0.02, p ≤ .001), as well as a significant Maltreatment × Genetic Risk interaction (b = .11, β = .18, SE = 0.03, p ≤ .01). The use of OLS regression to analyze dichotomous outcomes is uncommon because the dependent variable is not normally distributed and because of concerns about heteroscedasticity. In fact, the assumption of OLS regression is that the dependent variable is normally distributed, conditional on the set of predictors. The normality of the regression coefficients is required to compute confidence intervals and inferential statistics (Lumley et al., 2002). Given the large sample size and the prevalence rate of conduct disorder in our sample, the Central Limit Theorem ensures that the regression coefficients will be normally distributed (Lumley et al., 2002). Although it is unlikely that the residuals are normally distributed around the regression line, the use of robust variance estimators (Rogers, 1993; Williams, 2000) addresses the bias associated with such heteroscedasticity.
References
- Achenbach TM. Manual for the Child Behavior Checklist/4–18 and 1991 profile. Burlington, VT: University of Vermont Department of Psychiatry; 1991a. [Google Scholar]
- Achenbach TM. Manual for the Teacher's Report Form and 1991 profile. Burlington, VT: University of Vermont Department of Psychiatry; 1991b. [Google Scholar]
- Achenbach TM, McConaughy SH, Howell CT. Child/adolescent behavioral and emotional problems: Implications of cross-informant correlations for situational specificity. Psychological Bulletin. 1987;101:213–232. [PubMed] [Google Scholar]
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 4th. Washington, DC: Author; 1994. [Google Scholar]
- Andrieu N, Goldstein AM. Epidemiologic and genetic approaches in the study of gene–environment interaction: An overview of available methods. Epidemiologic Reviews. 1998;20:137–147. doi: 10.1093/oxfordjournals.epirev.a017976. [DOI] [PubMed] [Google Scholar]
- Arseneault L, Moffitt TE, Caspi A, Taylor A, Rijsdijk FV, Jaffee SR, Ablow JC, Measelle JR. Strong genetic effects on cross-situational antisocial behavior among 5-year-old children according to mothers, teachers, examiner-observers, and twins' self-reports. Journal of Child Psychology and Psychiatry. 2003;44:832–848. doi: 10.1111/1469-7610.00168. [DOI] [PubMed] [Google Scholar]
- Barnett D, Manly JT, Cicchetti D. Defining child maltreatment: The interface between policy and research. In: Cicchetti D, Toth SL, editors. Child abuse, child development, and social policy. Norwood, NJ: Ablex; 1993. pp. 7–73. [Google Scholar]
- Bennett AJ, Lesch KP, Heils A, Long J, Lorenz J, Shoaf SE, Champoux M, Suomi SJ, Linnoila M, Higley JD. Early experience and serotonin transporter gene variation interact to influence primate CNS function. Molecular Psychiatry. 2002;7:118–122. doi: 10.1038/sj.mp.4000949. [DOI] [PubMed] [Google Scholar]
- Bennett N, Jarvis L, Rowlands O, Singleton N, Haselden L. Living in Britain: Results from the General Household Survey. London: HMSO; 1996. [Google Scholar]
- Bird HR, Gould MS, Staghezza B. Aggregating data from multiple informants in child psychiatry epidemiological research. Journal of the American Academy of Child and Adolescent Psychiatry. 1992;31:78–85. doi: 10.1097/00004583-199201000-00012. [DOI] [PubMed] [Google Scholar]
- Bland R, Orn H. Family violence and psychiatric disorder. Canadian Journal of Psychiatry. 1986;31:129–137. doi: 10.1177/070674378603100210. [DOI] [PubMed] [Google Scholar]
- Browne MW, Cudeck R. Alternative ways of assessing model fit. In: Bollen KA, Long JS, editors. Testing structural equation models. Newbury Park, CA: Sage; 1993. pp. 136–162. [Google Scholar]
- Cadoret RJ, Cain CA, Crowe RR. Evidence for gene–environment interaction in the development of adolescent antisocial behavior. Behavior Genetics. 1983;13:301–310. doi: 10.1007/BF01071875. [DOI] [PubMed] [Google Scholar]
- Cadoret RJ, Yates WR, Troughton E, Woodworth G, Stewart MA. Genetic–environmental interaction in the genesis of aggressivity and conduct disorders. Archives of General Psychiatry. 1995;52:916–924. doi: 10.1001/archpsyc.1995.03950230030006. [DOI] [PubMed] [Google Scholar]
- Caspi A, McClay J, Moffitt TE, Mill J, Martin J, Craig IW, Taylor A, Poulton R. Role of genotype in the cycle of violence in maltreated children. Science. 2002;297:851–854. doi: 10.1126/science.1072290. [DOI] [PubMed] [Google Scholar]
- Caspi A, Sugden K, Moffitt TE, Taylor A, Craig IW, Harrington H, McClay J, Mill J, Martin J, Braithwaite A, Poulton R. Influence of life stress on depression: Moderation by a polymorphism in the 5-HTT gene. Science. 2003;31:386–389. doi: 10.1126/science.1083968. [DOI] [PubMed] [Google Scholar]
- Caspi A, Wright BRE, Moffitt TE, Silva PA. Early failure in the labor market: Childhood and adolescent predictors of unemployment in the transition to adulthood. American Sociological Review. 1998;63:424–451. [Google Scholar]
- Cicchetti D, Manly JT. Operationalizing child maltreatment: Developmental processes and outcomes [Special Issue] Development and Psychopathology. 2001;13:1–1048. [PubMed] [Google Scholar]
- Cicchetti D, Rogosch FA. The impact of maltreatment and psychopathology on neuroendocrine functioning. Development and Psychopathology. 2001;13:783–804. [PubMed] [Google Scholar]
- Cicchetti D, Rogosch FA, Lynch M, Holt KD. Resilience in maltreated children: Processes leading to adaptive outcome. Development and Psychopathology. 1993;5:629–647. [Google Scholar]
- De Bellis MD. Developmental traumatology: The psychobiological development of maltreated children and its implications for research, treatment, and policy. Development and Psychopathology. 2001;13:539–564. doi: 10.1017/s0954579401003078. [DOI] [PubMed] [Google Scholar]
- DeMaris A. Odds versus probabilities in logit equations: A reply to Roncek. Social Forces. 1993;71:1057–1065. [Google Scholar]
- Department of Health. The Children Act. London: HMSO; 1989. [Google Scholar]
- Dodge KA, Bates JE, Pettit GS. Mechanisms in the cycle of violence. Science. 1990;250:1678–1683. doi: 10.1126/science.2270481. [DOI] [PubMed] [Google Scholar]
- Dodge KA, Pettit GS, Bates JE. Socialization mediators of the relation between socioeconomic status and child conduct problems. Child Development. 1994;65:649–665. [PubMed] [Google Scholar]
- Dodge KA, Pettit GS, Bates JE, Valente E. Social information-processing patterns partially mediate the effect of early physical abuse on later conduct problems. Journal of Abnormal Psychology. 1995;104:632–643. doi: 10.1037//0021-843x.104.4.632. [DOI] [PubMed] [Google Scholar]
- Eckenrode J, Zielinski D, Smith E, Marcynyszyn LA, Henderson CR, Jr, Kitzman H, Cole R, Powers J, Olds DL. Child maltreatment and the early onset of problem behaviors: Can a program of nurse home visitation break the link? Development and Psychopathology. 2001;13:873–890. [PubMed] [Google Scholar]
- Egami Y, Ford D, Greenfield S, Crum R. Psychiatric profile and sociodemographic characteristics of adults who report physically abusing or neglecting their children. American Journal of Psychiatry. 1996;153:921–925. doi: 10.1176/ajp.153.7.921. [DOI] [PubMed] [Google Scholar]
- Evans WE, Relling MV. Pharmacogenomics: Translating functional genomics into rational therapeutics. Science. 1999;286:487–491. doi: 10.1126/science.286.5439.487. [DOI] [PubMed] [Google Scholar]
- Farrington DP. Crime and physical health: Illnesses, injuries, accidents and offending in the Cambridge Study. Criminal Behaviour and Mental Health. 1995;5:278. [Google Scholar]
- Hamer D. Rethinking behavior genetics. Science. 2002;298:71–72. doi: 10.1126/science.1077582. [DOI] [PubMed] [Google Scholar]
- Hardin J, Hilbe J. Generalized linear models and extensions. College Station, TX: Stata Press; 2001. [Google Scholar]
- Hill AVS. Genetics and genomics of infectious disease susceptibility. British Medical Bulletin. 1999;55:401–413. doi: 10.1258/0007142991902457. [DOI] [PubMed] [Google Scholar]
- Jaffee SR. Family violence and parent psychopathology: Implications for children's socioemotional development and resilience. In: Goldstein S, Brooks R, editors. Handbook of resilience in children. New York: Kluwer; in press. [Google Scholar]
- Jaffee SR, Caspi A, Moffitt TE, Taylor A. Physical maltreatment victim to antisocial child: Evidence of an environmentally-mediated process. Journal of Abnormal Psychology. 2004;113:44–55. doi: 10.1037/0021-843X.113.1.44. [DOI] [PubMed] [Google Scholar]
- Kendler KS, Eaves LJ. Models for the joint effect of genotype and environment on liability to psychiatric illness. American Journal of Psychiatry. 1986;143:279–289. doi: 10.1176/ajp.143.3.279. [DOI] [PubMed] [Google Scholar]
- Kendler KS, Kessler RC. Stressful life events, genetic liability and onset of an episode of major depression in women. American Journal of Psychiatry. 1995;152:833–842. doi: 10.1176/ajp.152.6.833. [DOI] [PubMed] [Google Scholar]
- Lansford JE, Dodge KA, Pettit GS, Bates JE, Crozier J, Kaplow J. Long-term effects of early child physical maltreatment on psychological, behavioral, and academic problems in adolescence: A 12-year prospective study. Archives of Pediatrics and Adolescent Medicine. 2002;156:824–830. doi: 10.1001/archpedi.156.8.824. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lumley T, Diehr P, Emerson S, Chen L. The importance of the normality assumption in large public health data sets. American Review of Public Health. 2002;23:151–169. doi: 10.1146/annurev.publhealth.23.100901.140546. [DOI] [PubMed] [Google Scholar]
- MacCallum RC, Browne MW, Sugawara HM. Power analysis and determination of sample size for covariance structure modeling. Psychological Methods. 1996;1:130–149. [Google Scholar]
- Manly JT, Cicchetti D, Barnett D. The impact of maltreatment on child outcome: An exploration of dimensions within maltreatment. Development and Psychopathology. 1994;6:121–143. [Google Scholar]
- Manly JT, Kim JE, Rogosch FA, Cicchetti D. Dimensions of child maltreatment and children's adjustment: Contributions of developmental timing and subtype. Development and Psychopathology. 2001;13:759–782. [PubMed] [Google Scholar]
- Martin N. Gene–environment interaction and twin studies. In: Spector TD, Snieder H, Mac-Gregor AJ, editors. Advances in twin and sib-pair analysis. London: Greenwich Medical Media Ltd; 2000. pp. 143–150. [Google Scholar]
- Maynard RA. Kids having kids: Economic costs and social consequences of teen pregnancy. Washington, DC: Urban Institute Press; 1997. [Google Scholar]
- McGee R, Wolfe D, Olson J. Multiple maltreatment, attribution of blame, and adjustment among adolescents. Development and Psychopathology. 2001;13:827–846. [PubMed] [Google Scholar]
- McGloin JM, Widom CS. Resilience among abused and neglected children grown up. Development and Psychopathology. 2001;13:1021–1038. doi: 10.1017/s095457940100414x. [DOI] [PubMed] [Google Scholar]
- Moffitt TE, Caspi A, Harrington H, Milne BJ. Males on the life-course-persistent and adolescence-limited antisocial pathways: Follow-up at age 26 years. Development and Psychopathology. 2002;14:179–207. doi: 10.1017/s0954579402001104. [DOI] [PubMed] [Google Scholar]
- Moffitt TE, E-Risk Study Team Teen-aged mothers in contemporary Britain. Journal of Child Psychology and Psychiatry. 2002;43:727–742. doi: 10.1111/1469-7610.00082. [DOI] [PubMed] [Google Scholar]
- Monroe SM, Simons AD. Diathesis–stress theories in the context of life stress research: Implications for depressive disorders. Psychological Bulletin. 1991;110:406–425. doi: 10.1037/0033-2909.110.3.406. [DOI] [PubMed] [Google Scholar]
- Neale MC, Cardon LR. Methodology for genetic studies of twins and families. Dordrecht: Kluwer; 1992. [Google Scholar]
- Olds DL, Eckenrode J, Henderson CR, Jr, Kitzman H, Powers J, Cole R, Sidora K, Morris P, Pettitt LM, Luckey D. Long-term effects of home visitation on maternal life course and child abuse and neglect: 15-year follow-up of a randomized trial. Journal of the American Medical Association. 1997;278:637–643. [PubMed] [Google Scholar]
- Ottman R. Epidemiologic analysis of gene– environment interaction in twins. Genetic Epidemiology. 1994;11:75–86. doi: 10.1002/gepi.1370110108. [DOI] [PubMed] [Google Scholar]
- Piacentini JC, Cohen P, Cohen J. Combining discrepant diagnostic information from multiple sources: Are complex algorithms better than simple ones? Journal of Abnormal Child Psychology. 1992;20:51–63. doi: 10.1007/BF00927116. [DOI] [PubMed] [Google Scholar]
- Plomin R, Crabbe J. DNA. Psychological Bulletin. 2000;126:806–828. doi: 10.1037/0033-2909.126.6.806. [DOI] [PubMed] [Google Scholar]
- Pollak SD, Cicchetti D, Hornung K, Reed A. Recognizing emotion in faces: Developmental effects of child abuse and neglect. Developmental Psychology. 2000;36:679–688. doi: 10.1037/0012-1649.36.5.679. [DOI] [PubMed] [Google Scholar]
- Pollak SD, Sinha P. Effects of early experience on children's recognition of facial displays of emotion. Developmental Psychology. 2002;38:784–791. doi: 10.1037//0012-1649.38.5.784. [DOI] [PubMed] [Google Scholar]
- Potter LB, Mercy JA. Public health perspective on interpersonal violence among youths in the United States. In: Stoff DM, Breiling J, Maser JD, editors. Handbook of antisocial behavior. New York: Wiley; 1997. pp. 3–11. [Google Scholar]
- Price TS, Freeman B, Craig I, Petrill SA, Ebersole L, Plomin R. Infant zygosity can be assigned by parental report questionnaire data. Twin Research. 2000;3:129–133. doi: 10.1375/136905200320565391. [DOI] [PubMed] [Google Scholar]
- Rogers WH. Regression standard errors in clustered samples. Stata Technical Bulletin. 1993;13:19–23. [Google Scholar]
- Rowe DC. Biology and crime. Los Angeles: Roxbury; 2001. [Google Scholar]
- Rutter M, Silberg J. Gene–environment interplay in relation to emotional and behavioral disturbance. Annual Review of Psychology. 2002;53:463–490. doi: 10.1146/annurev.psych.53.100901.135223. [DOI] [PubMed] [Google Scholar]
- Sedlak AJ, Broadhurst DD. Executive summary of the third national incidence study of child abuse and neglect. 1996 Retrieved July 31, 2002 from http://www.calib.com/nccanch/pubs/statinfo/nis3.cfm#national.
- Simonoff E, Pickles A, Meyer JM, Silberg J, Maes HHM, Loeber R, Rutter M, Hewitt JK, Eaves LJ. The Virginia Twin Study of Adolescent Behavioral Development. Archives of General Psychiatry. 1997;54:801–808. doi: 10.1001/archpsyc.1997.01830210039004. [DOI] [PubMed] [Google Scholar]
- Smith C, Thornberry TP. The relationship between childhood maltreatment and adolescent involvement in delinquency. Criminology. 1995;33:451–481. [Google Scholar]
- StataCorp. Stata statistical software: Release 7.0. College Station, TX: Stata Corporation; 2001. [Google Scholar]
- Stoolmiller M. Implications of the restricted range of family environments for estimates of heritability and nonshared environment in behavior– genetic adoption studies. Psychological Bulletin. 1999;125:392–409. doi: 10.1037/0033-2909.125.4.392. [DOI] [PubMed] [Google Scholar]
- Straus MA, Gelles RJ. How violent are American families? Estimates from the National Family Violence Resurvey and other studies. In: Hotaling GT, Finkelhor D, editors. Family abuse and its consequences: New directions in research. Thousand Oaks, CA: Sage; 1988. pp. 14–36. [Google Scholar]
- Suomi SJ. Social and biological mechanisms underlying impulsive aggressiveness in rhesus monkeys. In: Lahey BB, Moffitt TE, Caspi A, editors. The causes of conduct disorder and serious juvenile delinquency. New York: Guilford Press; 2002. [Google Scholar]
- Trouton A, Spinath FM, Plomin R. Twins Early Development Study (TEDS): A multivariate, longitudinal genetic investigation of language, cognition, and behaviour problems in childhood. Twin Research. 2002;5:444–448. doi: 10.1375/136905202320906255. [DOI] [PubMed] [Google Scholar]
- van den Oord EJCG, Koot HM, Boomsma DI, Verhulst FC, Orleveke JF. A twin-singleton comparison of problem behaviour in 2–3 year olds. Journal of Child Psychology and Psychiatry. 1995;36:449–458. doi: 10.1111/j.1469-7610.1995.tb01302.x. [DOI] [PubMed] [Google Scholar]
- van den Oord EJCG, Verhulst FC, Boomsma DI. A genetic study of maternal and paternal ratings of problem behaviors in 3-year-old twins. Journal of Abnormal Psychology. 1996;105:349–357. doi: 10.1037//0021-843x.105.3.349. [DOI] [PubMed] [Google Scholar]
- van der Valk JC, Verhulst FC, Neale MC, Boomsma DI. Longitudinal genetic analysis of problem behaviors in biologically related and unrelated adoptees. Behavior Genetics. 1998;28:365–380. doi: 10.1023/a:1021621719059. [DOI] [PubMed] [Google Scholar]
- Walsh C, McMillan H, Jamieson E. The relationship between parental psychiatric disorder and child physical and sexual abuse: Findings from the Ontario Health Supplement. Child Abuse and Neglect. 2002;26:11–22. doi: 10.1016/s0145-2134(01)00308-8. [DOI] [PubMed] [Google Scholar]
- Widom CS. Sampling biases and implications for child abuse research. American Journal of Orthopsychiatry. 1988;58:260–270. doi: 10.1111/j.1939-0025.1988.tb01587.x. [DOI] [PubMed] [Google Scholar]
- Widom CS. The cycle of violence. Science. 1989;244:160–166. doi: 10.1126/science.2704995. [DOI] [PubMed] [Google Scholar]
- Widom CS. Child abuse, neglect, and witnessing violence. In: Stoff DM, Breiling J, Maser JD, editors. Handbook of antisocial behavior. New York: Wiley; 1997. pp. 159–170. [Google Scholar]
- Widom CS, Maxfield MG. An update on the “cycle of violence” (NCJ 184894) Washington, DC: National Institute of Justice; 2001. [Google Scholar]
- Williams RL. A note on robust variance estimation for cluster-correlated data. Biometrics. 2000;56:645–646. doi: 10.1111/j.0006-341x.2000.00645.x. [DOI] [PubMed] [Google Scholar]