

Abstract
Background
Arterial augmentation (AP) and the augmentation index (Aix) are surrogate parameters of arterial stiffness and are commonly used as predictors for cardiovascular risk. The aim of this study is to compare these parameters in diabetic subjects and nondiabetic cardiovascular risk subjects with healthy control subjects.
Methods
One hundred sixty-six nonsmoking subjects aged between 35 and 70 years were included in the study, which included 100 subjects with cardiovascular disease but not diabetes (mean age 62.73±8.75 years), 33 subjects with type 2 diabetes (66.58±2.69 years), and 33 healthy controls (51.89±8.91 years). In these subjects, arterial stiffness was measured by the difference between the second and the first systolic peak of the central pressure waveform, and the Aix was calculated as the percentage of Aix from pulse pressure.
Results
Arterial augmentation was increased in subjects with diabetes (DM) with 10.21±6.97 mm Hg and in subjects with cardiovascular disease but not diabetes (CV) with 10.74±5.29 mm Hg in comparison to healthy controls (C) with 6.59±3.97 mm Hg (p < 0.0005 DM vs C; p < 0.00005 CV vs C). Moreover, Aix was increased with 26.00±9.91% in CV subjects compared to healthy controls with 19.84±9.37% (p < 0.02 CV vs C). The augmentation index was increased with 21.12±11.21% in subjects with type 2 diabetes mellitus compared to controls, but failed to be statistically significant. There was no statistical significance in arterial augmentation or the augmentation index between CV and diabetic subjects.
Conclusion
The results of our study revealed a comparable increased augmentation index as a surrogate measure of arterial stiffness and arteriosclerosis in subjects with diabetes mellitus and in nondiabetic subjects with cardiovascular disease.
Keywords: augmentation, augmentation index, cardiovascular risk, diabetes mellitus type 2, pulse wave analysis
Introduction
Diabetes mellitus type 2 is associated with a higher risk of cardiovascular disease.1,2 Morbidity and mortality in hypertension and cardiovascular disease are related to structural and functional alterations of the arterial wall.3–5 Changes in the arterial wall can lead to increased arterial stiffness, which influences cardiovascular prognosis negatively.6 Pulse wave analysis (PWA) is a noninvasive and reproducible technique7–9 used to examine arterial elastic properties and has therefore been utilized in many clinical studies.10–12 An increased augmentation index (Aix) is associated with increased cardiovascular risk,13,14 and an increased augmentation index was reported in patients with either type 2 diabetes (DM) or impaired glucose tolerance.15 The aim of this study is to compare changes in the augmentation index in patients with DM and in nondiabetic cardiovascular risk patients with healthy controls.
Patients and Methods
One hundred sixty-six subjects (89 male and 77 female) aged between 35 and 70 years were included in the study: 100 subjects with increased cardiovascular risk but not diabetes, 33 subjects with type 2 diabetes, and 33 healthy controls. The clinical characteristics and demographical data of the different subject groups are given in Table 1. All subjects were nonsmokers. Type 2 diabetes mellitus was defined by American Diabetes Association criteria; increased cardiovascular risk was defined as having a current or past history of hypertension, coronary heart disease, myocardial infarction, or stroke, but not diabetes. Patients with heart failure were excluded from the study.
Table 1.
Characteristics of Patients with Diabetes Mellitus Type 2, Cardiovascular Risk Patients, and Healthy Controls
| Diabetes mellitus type 2 | Nondiabetic cardiovascular risk | Healthy subjects | |
|---|---|---|---|
| n | 33 | 100 | 33 |
| Age (years) | 66.58±2.69 | 62.73± 8.75 | 51.89± 8.91 |
| Gender (male/female) | 19/14 | 52/48 | 18/15 |
| Body mass index (kg/m2) | 33.12 | 29.86 | 26.24 |
Pulse Waveform Analysis
Arterial stiffness, which is predictive of vascular disease outcomes, can be measured by analysis of the arterial waveform to determine pulse waveform and augmentation index.16 In our study, arterial stiffness was assessed noninvasively with a commercially available SphygmoCor system (AtCorMedical, Australia) from the radial artery at the left wrist using applanation tonometry.
After 20 sequential waveforms were recorded, a validated generalized transfer function was used to generate the corresponding central aortic pressure waveform.17–19 On the generated central aortic pressure waveform, the merging curve of the incident and the reflected wave (the inflection point) was identified (Figure 1). The augmentation (AP) of the central aortic pressure is a manifestation of early wave reflection and is the boost of pressure from the first systolic shoulder to the systolic pressure peak.6 Augmentation is calculated as the difference between the second and the first systolic shoulder of the central pressure wave curve, and the augmentation index is expressed as the percentage of AP from total pulse pressure (Figure 1). Because Aix is influenced in an inverse and linear manner by heart rate, according to Wilkinson et al.,20 the Aix was normalized for a heart rate of 75 bpm (Aix@75). Higher values of Aix indicate increased wave reflection from periphery or earlier return of the reflected wave as a result of increased pulse wave velocity, which can be contributed to an increased arterial stiffness. Lower values for Aix indicate a good elasticity of the arterial wall.
Figure 1.
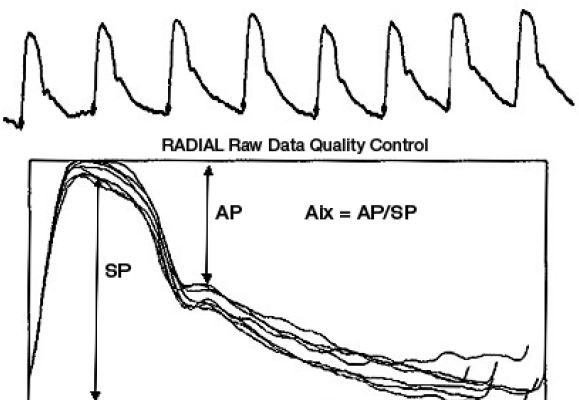
Pulse wave analysis: Calculation of augmentation (AP) and augmentation index (Aix) from superimposed sequential pulse (SP) waves.
All PWA recordings were performed on a subject lying in a quiet room after a rest of at least 5 minutes. Recordings were performed by one of two trained investigators.
Only high-quality recordings, controlled by internal quality definitions (in-device quality index >80%) and an acceptable curve by visual inspection, were included in the analysis.
Statistics
All results are presented as mean±1 SD and as the number/proportion of patients with a characteristic for categorical variables. Differences in mean values among the three groups were compared by using unpaired t tests. The Shapiro–Wilk test was used for the characterization of data distribution. All analyses were performed in exploratory and nonconfirmatory settings and all p values <0.05 are interpreted as significant.
Results
As shown in Figure 2, AP was increased both in patients with DM with 10.21±6.97 mm Hg and in cardiovascular risk patients without diabetes (CV) with 10.74±5.29 mm Hg compared to healthy controls (C) with 6.59±3.97 mm Hg (p < 0.0005 DM vs C; p < 0.00005 CV vs C).
Figure 2.
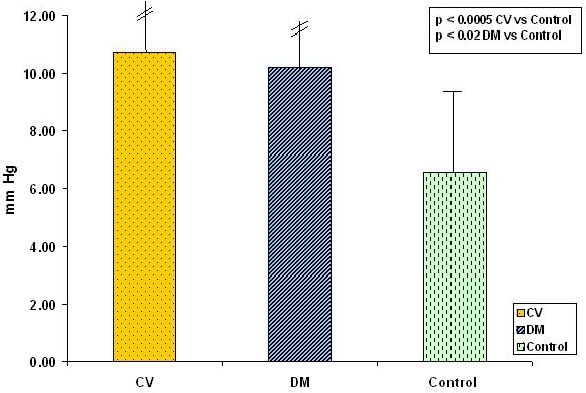
Augmentation in cardiovascular risk patients (CV), patients with diabetes mellitus type 2 (DM), and healthy controls.
The augmentation index in CV subjects (26.00±9.91%) compared to healthy controls (19.84±9.37%) was increased significantly (p < 0.02 CV vs C). The augmentation index was also increased in patients with DM (21.12±11.21%), but failed statistical significance (p = 0.5) (Figure 3).
Figure 3.

Augmentation index (Aix@75) in cardiovascular risk patients (CV), patients with diabetes mellitus type 2 (DM), and healthy controls.
No difference was found between cardiovascular risk patients and diabetic patients, neither in AP (p = 0.56) nor in Aix (p = 0.2).
Discussion
The main finding of our study is that subjects with type 2 diabetes have a comparable increased arterial stiffness (compared to healthy controls) as subjects with increased cardiovascular risk and no diabetes. In the Hoorn study, an increased augmentation index in patients with type 2 diabetes mellitus was found to be independent of other potential confounders, such as age, sex, or mean arterial blood pressure.15 Moreover, an increased pulse pressure, measured noninvasively by PWA, was associated with increased cardiovascular mortality in these patients.21 Even in patients with an impaired glucose tolerance, the augmentation index was higher compared to healthy controls.15 These findings demonstrate the destructive effect of metabolic disturbances on the vascular wall even in subjects not already defined as having diabetes. The relationship between measured arterial stiffness and type 2 diabetes and cardiovascular disease suggests that impairment in glucose metabolism or reduced vascular insulin sensitivity might cause functional and/or anatomical changes in the arterial wall. These changes might be due to alterations in elastin and collagen fibers caused by glycation of proteins and formation of advanced glycation end products.22 Other studies have revealed an independent association between an increased augmentation index as a marker for arterial stiffness and the presence and severity of coronary heart disease.13,14 Findings of the aforementioned studies confounded our results of increased arterial stiffness measured by PWA in patients with diabetes mellitus type 2 and in subjects with increased cardiovascular risk but without diabetes. There was no significant difference between patients with diabetes and cardiovascular diseases, suggesting that diabetes mellitus type 2 causes similar changes in arterial elasticity as cardiovascular diseases. This finding is in accordance with epidemiological studies showing a comparable risk for cardiovascular end points such as myocardial infarction and stroke in patients with type 2 diabetes compared with patients suffering from coronary artery disease.23 The same method has been used previously in type 2 diabetic patients15 and in type 1 diabetes.24 The main topic of our study was to compare this method in diabetic and nondiabetic patients at cardiovascular risk, whereas in the cited paper of Schram et al.,15 patients with diabetes type 2 or impaired glucose tolerance were investigated.
There are some limitations of our study. The healthy controls were slightly younger than the cardiovascular and diabetic patients. Although it is generally supposed that arterial stiffness increases with increasing age, a previous study did not detect age as a confounder for the augmentation index in patients with diabetes or cardiovascular risk.13 Moreover, the CV subjects received vasodilating drugs such as nitrates, angiotensin-converting enzyme inhibitors, and calcium channel blockers to a greater extent than the other groups did; these drugs all decreased the augmentation index.24
If these drugs had been withdrawn, then the difference in AP or Aix between CV patients and controls might have been even more pronounced. In conclusion, arterial stiffness in type 2 diabetic patients is increased comparable to that in patients with cardiovascular disease who do not have diabetes. Our findings of a comparable restriction in arterial elasticity in type 2 diabetic subjects and nondiabetic cardiovascular risk subjects highlight the significance of early metabolic alterations in the pathophysiology of arteriosclerosis. This noninvasive measurement of augmentation or the augmentation index would be a valuable tool for risk characterization in these patient populations because these measures appear to be surrogate measures of atherosclerosis.
Abbreviations
- AP
augmentation
- Aix
augmentation index
- PWA
pulse wave analysis
References
- 1.Pyorala K, Laakso M, Uusitupa M. Diabetes and atherosclerosis: an epidemiologic view. Diabetes Metab Rev. 1987 Apr;3(2):463–524. doi: 10.1002/dmr.5610030206. [DOI] [PubMed] [Google Scholar]
- 2.de Vegt F, Dekker JM, Ruhe HG, Stehouwer CD, Nijpels G, Bouter LM, Heine RJ. Hyperglycemia is associated with all-cause and cardiovascular mortality in the Hoorn population: the Hoorn study. Diabetologica. 1999 Aug;42(8):926–931. doi: 10.1007/s001250051249. [DOI] [PubMed] [Google Scholar]
- 3.Asmar R, Benetos A, London G, Hugue C, Weiss Y, Topouchian J. Aortic distensibility in normotensive, untreated and treated hypertensive patients. Blood Press. 1995 Jan;4(1):48–54. doi: 10.3109/08037059509077567. [DOI] [PubMed] [Google Scholar]
- 4.O'Rourke M. Mechanical principles in arterial disease. Hypertension. 1995 Jul;26(1):2–9. doi: 10.1161/01.hyp.26.1.2. [DOI] [PubMed] [Google Scholar]
- 5.Nichols WW, O'Rourke MF. McDonalds blood flow in arteries: theoretical, experimental and clinical principles. 4th ed. London: Edward Arnold; 1998. [Google Scholar]
- 6.O'Rourke MF, Mancia G. Arterial stiffness. J Hypertens. 1999 Jan;17(1):1–4. doi: 10.1097/00004872-199917010-00001. [DOI] [PubMed] [Google Scholar]
- 7.O'Rourke MF, Gallagher DE. Pulse wave analysis. J Hypertens Suppl. 1996 Dec;14(5):S147–S157. [PubMed] [Google Scholar]
- 8.Wilkinson IB, Cockcroft JR, Webb DJ. Pulse wave analysis and arterial stiffness. J Cardiovasc Pharmacol. 1998;32(Suppl 3):S33–S37. [PubMed] [Google Scholar]
- 9.Filipovsky J, Svobodova V, Pecen L. Reproducibility of radial pulse wave analysis in healthy subjects. J Hypertens. 2000 Aug;18(8):1033–1040. doi: 10.1097/00004872-200018080-00007. [DOI] [PubMed] [Google Scholar]
- 10.Wilkinson IB, MacCallum H, Rooijmans DF, Murray GD, Cockcroft JR, McKnight JA, Webb DJ. Increased augmentation index and systolic stress in type 1 diabetes. QJM. 2000 Jul;93(7):441–448. doi: 10.1093/qjmed/93.7.441. [DOI] [PubMed] [Google Scholar]
- 11.Smith JC, Page MD, John R, Wheeler MH, Cockcroft JR, Scanlon MF, Davies JS. Augmentation of central arterial pressure in mild primary hyperparathyroidism. J Clin Endocrinol Metab. 2000 Oct;85(10):3515–3519. doi: 10.1210/jcem.85.10.6880. [DOI] [PubMed] [Google Scholar]
- 12.Kohara K, Jiang Y, Igase M, Hiwada K. Effect of reflection of arterial pressure on carotid circulation in essential hypertension. Am J Hypertens. 1999 Oct;12(10 Pt 1):1015–1020. doi: 10.1016/s0895-7061(99)00091-6. [DOI] [PubMed] [Google Scholar]
- 13.Nürnberger J, Keflioglu-Scheiber A, Opazo Saez AM, Wenzel RR, Philipp T, Schäfers RF. Augmentation index is associated with cardiovascular risk. J Hypertens. 2002 Dec;20(12):2407–2414. doi: 10.1097/00004872-200212000-00020. [DOI] [PubMed] [Google Scholar]
- 14.Weber T, Auer J, O'Rourke MF, Kvas E, Lassnig E, Berent R, Eber B. Arterial stiffness, wave reflections and the risk of coronary artery disease. Circulation. 2004 Jan 20;109(2):184–189. doi: 10.1161/01.CIR.0000105767.94169.E3. [DOI] [PubMed] [Google Scholar]
- 15.Schram MT, Henry RM, van Djik RA, Kostense PJ, Dekker JM, Nijpels G, Heine RJ, Bouter LM, Westerhof N, Stehouwer CDA. Increased central artery stiffness in impaired glucose metabolism and type 2 diabetes. Hypertension. 2004 Feb;43(2):176–181. doi: 10.1161/01.HYP.0000111829.46090.92. [DOI] [PubMed] [Google Scholar]
- 16.Haffner SM, Lehto S, Ronnemaa T, Pyorala K, Laakso M. Mortality from coronary heart disease in subjects with type 2 diabetes and in nondiabetic subjects with and without prior myocardial infarction. N Engl J Med. 1998 Jul 23;339(4):229–234. doi: 10.1056/NEJM199807233390404. [DOI] [PubMed] [Google Scholar]
- 17.Chen CH, Nevo E, Fetics B, Pak PH, Yin FC, Maughan WL, Kass DA. Estimation of central aortic pressure waveform by mathematical transformation of radial tonometry pressure: validation of a generalized transfer function. Circulation. 1997 Apr 1;95(7):1827–1836. doi: 10.1161/01.cir.95.7.1827. [DOI] [PubMed] [Google Scholar]
- 18.Pauca AL, O'Rourke MF, Kon ND. Prospective evaluation of a method for estimating ascending aortic pressure from the radial arterial pressure waveform. Hypertension. 2001 Oct;38(4):932–937. doi: 10.1161/hy1001.096106. [DOI] [PubMed] [Google Scholar]
- 19.O'Rourke MF, Pauca A, Kon ND. Generation of ascending aortic from radial artery pressure waveform. J Am Coll Cardiol. 2002;39:177B. [Google Scholar]
- 20.Wilkinson IB, MacCullum H, Flint L, Cockcroft JR, Newby DE, Webb DJ. The influence of heart rate on augmentation index and central arterial pressure in humans. J Physiol. 2000 May 15;(525 Pt 1):263–270. doi: 10.1111/j.1469-7793.2000.t01-1-00263.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Schram MT, Kostense PJ, Van Dijk RA, Dekker JM, Nijpels G, Bouter LM, Heine RJ, Stehouwer CD. Diabetes pulse pressure and cardiovascular mortality: the Hoorn Study. J Hypertens. 2002 Sep;20(9):1743–1751. doi: 10.1097/00004872-200209000-00017. [DOI] [PubMed] [Google Scholar]
- 22.Henry RM, Kostense PJ, Spijkerman AM, Dekker JM, Nijpels G, Heine RJ, Kamp O, Westerhof N, Bouter LM, Stehouwer CD Hoorn Study. Arterial stiffness increases with deteriorating glucose tolerance status. The Hoorn study. Circulation. 2003 Apr 29;107(16):2089–2095. doi: 10.1161/01.CIR.0000065222.34933.FC. [DOI] [PubMed] [Google Scholar]
- 23.Karamanoglu M, O'Rourke MF, Avolio AP, Kelly RP. An analysis of the relationship between central aortic and peripheral upper limb pressure waves in man. Eur Heart J. 1993 Feb;14(2):160–167. doi: 10.1093/eurheartj/14.2.160. [DOI] [PubMed] [Google Scholar]
- 24.Westerbacka J, Uosukainen A, Mäkimattila S, Schlenzka A, Yki-Järvinen H. Hypertension. 2000 May;35(5):1043–1048. doi: 10.1161/01.hyp.35.5.1043. [DOI] [PubMed] [Google Scholar]
- 25.Nichols WW, Singh BM. Augmentation index as a measure of peripheral vascular disease state. Curr Opin Cardiol. 2002 Sep;17(5):543–551. doi: 10.1097/00001573-200209000-00016. [DOI] [PubMed] [Google Scholar]