

Abstract
Peer rejection and aggression in the early school years were examined for their relevance to early starting conduct problems. The sample of 657 boys and girls from 4 geographical locations was followed from 1st through 4th grades. Peer rejection in 1st grade added incrementally to the prediction of early starting conduct problems in 3rd and 4th grades, over and above the effects of aggression. Peer rejection and aggression in 1st grade were also associated with the impulsive and emotionally reactive behaviors found in older samples. Being rejected by peers subsequent to 1st grade marginally added to the prediction of early starting conduct problems in 3rd and 4th grades, controlling for 1st grade ADHD symptoms and aggression. Furthermore, peer rejection partially mediated the predictive relation between early ADHD symptoms and subsequent conduct problems. These results support the hypothesis that the experience of peer rejection in the early school years adds to the risk for early starting conduct problems.
Keywords: peer rejection, aggression, conduct disorder
The purpose of this paper was to address three questions relating to the role of early school-age peer rejection and aggression in the development of early starting conduct problems. First, does peer rejection in first grade independently predict subsequent conduct problems, over and above the effects of aggression? This question has been examined from middle childhood onward; it has not, however, been examined in the early school years. The second goal was to investigate the concurrent behavioral correlates of peer rejection and aggression in first grade in order to understand why aggressive children who are rejected by their peers might be at greater risk than were those who are not rejected. Third, we tested the hypothesis that peer rejection was not simply a marker for these related behavioral risk factors, but that the experience of being rejected by peers contributed incrementally to the prediction of later conduct problems. By addressing these questions in a sample of early school age boys and girls, we hoped to advance the understanding of the development of early starting conduct problems.
In the last decade, there has been a growing recognition of the independent contribution made by peer relations in forecasting subsequent conduct problems (Coie & Miller-Johnson, in press; Rudolph & Asher, 2000). Because peer rejection is correlated with aggression, Parker and Asher (1987) raised the important question of whether rejection added to the existing tendency toward conduct problems or simply indexed the developmental progression of early aggressive behavior. Prior to Parker and Asher's review, there were no studies in which the independent effects of both peer rejection and aggression were analyzed simultaneously. Instead, the correlates and outcomes of peer rejection were assessed without controlling for aggression. Consequently, it was unclear whether rejection, on its own, was a unique predictor of conduct problems or merely a marker for childhood aggression.
Since that time, there have been two sets of longitudinal studies that address Parker and Asher's question. Bierman, Smoot, and Aumiller (1993) investigated a small sample of Caucasian boys in first through fifth grades and compared concurrent functioning for males who were rejected only, aggressive only, rejected and aggressive, or neither rejected nor aggressive. They found that the combination of peer rejection and aggression was associated with a range of uncontrolled behavior problems, including elevated levels of physically aggressive, argumentative, inattentive, and disruptive behaviors and low levels of prosocial behaviors. In contrast, boys who were aggressive, but not rejected did not exhibit the same range and diversity of behavior problems, but rather showed elevations only in physical, instrumental, and goal-directed aggression. Boys who were rejected but not aggressive tended to be inattentive, passive, and socially awkward. In a 2-year follow-up, boys who were both rejected and aggressive continued to exhibit higher levels of aggressive and disruptive behaviors and prosocial deficits than did boys who were aggressive but not rejected (Bierman & Wargo, 1995).
In another study, Coie, Lochman, Terry, and Hyman (1992) and Coie, Terry, Lenox, Lochman, and Hyman (1995) followed a large, urban African American sample from third grade through adolescence. Follow-up data showed that both childhood aggression and peer rejection in third grade independently predicted externalizing problems in sixth grade (Coie et al., 1992). Furthermore, growth curve analyses showed that the combination of peer rejection and aggression predicted higher levels of externalizing behaviors among 10th-grade boys than did aggression or rejection alone. A slightly different pattern emerged for girls, as peer rejection led to higher parent ratings of externalizing problems, whereas aggression led to higher youth self-reports of externalizing problems (Coie et al., 1995). In the same sample, Miller-Johnson, Coie, Maumary-Gremaud, Lochman, and Terry (1999) extended the inquiry to examine specific types of conduct problems. Aggression predicted a wide array of offending behavior in males, including vandalism, robbery, felony theft, and minor assault. Most striking was that the combination of rejection and aggression in boys uniquely predicted acts of felony assault, demonstrating that the combination of childhood peer rejection and aggression was not only associated with increased risk for subsequent conduct problems, but also predicted the more serious forms of antisocial behavior.
These two longitudinal studies provide good evidence that peer rejection and aggression independently predict later conduct problems, and that these patterns can be detected reliably as early as third grade. What is less clear, however, is whether similar predictive patterns can be found earlier in childhood, in terms of the prognostic significance of these variables for the later school years. The Coie et al. (1992, 1995) and Miller-Johnson et al. (1999) studies began in third grade and followed children through adolescence. The Bierman et al. studies (1993, 1995) examined a mixed grade sample of first through fifth graders, but the total number of participants at follow-up was fairly small (N = 81), resulting in insufficient statistical power to detect age variations. This study fills in the missing steps between peer rejection and aggression in first grade and conduct problem outcomes in third and fourth grades, because it is at that age that we are able to predict forward into adolescence.
The current dataset also allowed us to study the contribution of concurrent behavior problems, including emotional reactivity, hyperactive–inattentive behaviors, and prosocial skill deficits, that are often associated with peer rejection to understand their predictive significance for later conduct problems. Although there is now good evidence that peer rejection is not simply a marker for related aggressive behavior, no attempts have been made to determine whether the behavioral factors that distinguish between rejected, aggressive children and nonrejected, aggressive children might account for the greater risk status of the former group. For example, rejected, aggressive children have been found to be more emotionally reactive and labile in their displays of aggression, in comparison with those children who are aggressive but not rejected. Bierman et al. (1993, 1995) found that although both rejected, aggressive and aggressive subgroups displayed high levels of aggression, the type of aggressive behavior differed across the two groups. Specifically, the aggressive behavior of rejected, aggressive children was more uncontrolled, argumentative, and disruptive and lasted for longer periods, whereas the aggressive behavior of the nonrejected subgroup was briefer and more goal-directed and instrumental.
These different types of aggression are similar to those found by Coie, Dodge, Terry, and Wright (1991) in their observational study of aggressive boys in experimentally organized play groups. The primary question was to understand differences between aggressive boys who were rejected and those who were not. Those boys who were both rejected and aggressive initiated a more reactive type of aggressive behavior that was characterized by angrier, more persistent displays of aggression. In addition, they tended to retaliate more often even when they initiated the aggression. These results, along with Bierman et al. (1993), suggest that peer rejection and aggression is associated with a more emotionally reactive, uncontrolled aggressive style.
These findings suggest a connection between the combination of peer rejection and aggression, and the impulsive and emotionally reactive behaviors that are symptomatic of attention deficit hyperactive disorder (ADHD). Hinshaw (1994) and Hinshaw and Melnick (1995) found strong ties between peer rejection and symptoms of ADHD. To illustrate, boys with ADHD were observed while interacting with unfamiliar peers in a camp setting. By the end of the 1st day of camp, the unfamiliar peers rejected boys with ADHD. The subgroup of children who were both aggressive and had ADHD were at especially high risk for being rejected by their peers (Erhardt & Hinshaw, 1994). Similarly, other researchers have documented increased risk for both social rejection and later conduct problems among children who are aggressive and hyperactive–inattentive compared with those who are aggressive only (Milich & Dodge, l984; Pope & Bierman, l999; Soussigan et al., l992). Thus, symptoms of ADHD appeared to contribute to the experience of being rejected and to the development of later conduct problems, over and above the effects of aggression alone.
Children who are rejected by their peers also display poorer social skills in comparison with other children. Spetter, LaGreca, Hogan, and Vaughn (1992) found that rejected children interacted less positively with other children and were more socially insensitive to others, for example, grabbing toys, talking meanly, and playing inappropriately. Bierman et al. (1993) found that rejected children tended to have poorer social skills. In addition, rejected children tended to expect more negative social outcomes and therefore may behave less competently in new situations (Hymel & Franke, 1985; Rabiner & Coie, 1989).
These findings suggest that early childhood peer rejection, combined with aggressiveness, may be associated with a more emotionally reactive, uncontrolled aggressive style, attentional deficits, and low levels of social competence. Most of the supporting research on childhood antecedents of peer rejection, however, has been conducted on older samples of children. In this study, we had the opportunity to investigate the concurrent correlates of rejection–aggression in an early school age sample.
The study of risk factors for conduct problems is not only an attempt to identify the earliest, primary determinants of antisocial behavior, but to identify processes that amplify or mediate the relation between early risk factors and subsequent conduct disorder. For example, it is plausible to reason that aggressive behavior and impulsivity may be strong predictors of peer rejection, as well as being antecedents of later conduct problems. This could mean that rejected, aggressive children are at greater risk for conduct problems than are aggressive children who are not rejected because of the contributing risk factor of impulsivity. However, it is also possible that once poorly skilled, hyperactive, aggressive children become rejected by peers, they are then subject to social experiences that also add to their risk for conduct problems. One example of this is provided by Dodge (1993). They found that being rejected increased children's tendencies to interpret peer motives in a hostile fashion, which in turn led to greater reactive aggression. The final question addressed in this study is whether, once we control for those child characteristics that contribute to being socially rejected (e.g., aggression, ADHD symptoms, prosocial skill deficits), the experience of peer rejection still adds incrementally to risk for early conduct problems.
In summary, the goal of this study was to fill in significant gaps in our understanding of how peer rejection and aggression in the early schools years are related to early starting antisocial behavior. We will first determine whether peer rejection in first grade independently predicts conduct problem outcomes in third and fourth grades, over and above the effects of aggression, because it is at that time we are able to predict further into adolescence. Second, we will explore the concurrent correlates of peer rejection and aggression in the early school years and evaluate relations between these behavior problems and later conduct problems. The final question is whether rejection is simply a marker for these related behavioral risk factors, namely, ADHD symptoms and aggression, or whether being rejected by peers contributes incrementally to the prediction of later conduct problems over and above these behavioral risk factors.
Method
Participants
Participants were part of a multisite longitudinal investigation of the development and prevention of conduct problems in children. Four sites were included in the study: Durham, NC; Nashville, TN; Seattle, WA, and rural central PA. Schools from high-risk communities were selected based on indicators of poverty and crime. Within each site, schools were matched based on poverty level, racial composition, and size and then randomly assigned to either intervention or control conditions. High-risk children were selected based on teacher and parent ratings completed at the end of the kindergarten year (see Conduct Problems Prevention Research Group [CPPRG], 1992, for more details).
As part of the study, 100 participants from each site were also included in a normative sample that was selected from the control schools. To form this representative sample, within each site, 10 children were selected from each decile of teacher ratings on the Authority-Acceptance scale of the Teacher Observation of Classroom Adaptation – Revised (TOCA-R; Werthamer-Larsson, Kellam, & Wheeler, 1991). The final normative sample consisted of 387 participants (50% male).5 Because control participants were also selected from schools not receiving the intervention, there was some overlap between the normative and the high-risk control group participants (N = 79). To include a large number of children at risk for subsequent conduct disorder, this study includes children from both the control and normative samples. A total of 657 children for whom sociometric data were available in first grade were included (57% male; 46% African American, 51% Caucasian, 3% other).
Procedures
Child self-report and parent ratings were obtained from face-to-face home interviews in the summer following first, third, and fourth grades. Two interviewers visited the home, and one interviewed the primary caregiver (usually the mother), whereas the other one interviewed the child. The interviewer read through all questionnaires and noted the caregiver's response. Parents were compensated financially for their time, and children received a prize.
Teacher ratings were obtained in the spring of the first-grade year. An interviewer visited the school and reviewed the rating measures with teachers. Teachers were compensated financially for their participation. Table I shows correlations across the different measures.
Table I.
Correlations
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. ADHD-PA | — | ||||||||||||||
| 2. ADHD-TE | .39*** | — | |||||||||||||
| 3. ADHD-PE | .29*** | .53*** | — | ||||||||||||
| 4. Agg-PE | .21*** | .41*** | .58*** | — | |||||||||||
| 5. Pro agg-PA | .40*** | .21*** | .17*** | .19*** | — | ||||||||||
| 6. Reac agg-PA | .37*** | .24*** | .21*** | .22*** | .58*** | — | |||||||||
| 7. Pro agg-TE | .27*** | .61*** | .33*** | .38*** | .23*** | .25*** | — | ||||||||
| 8. Reac agg-TE | .33*** | .74*** | .43*** | .41*** | .22*** | .28*** | .77*** | — | |||||||
| 9. Soc com-PA | −.49*** | −.27*** | −.30*** | −.24*** | −.36*** | −.50*** | −.11*** | −.32*** | — | ||||||
| 10. Soc com-TE | −.07 | −.17*** | −.11** | −.13** | .01 | −.02 | −.17** | −.23*** | .09* | — | |||||
| 11. Soc com-CH | −.12** | −.11** | −.11** | −.09* | −.03 | −.07 | −.01 | −.06 | .11** | .05 | — | ||||
| 12. Soc com-PE | −.24*** | −.34*** | −.29*** | −.20*** | −.13** | −.18*** | −.24*** | −.31*** | .26*** | .13*** | .14*** | — | |||
| 13. Soc pref-PE-g1 | −.28*** | −.43*** | −.54*** | −.43*** | −.19*** | −.27*** | −.27*** | −.40*** | .33*** | .15*** | .16*** | .62*** | — | ||
| 14. Soc pref-PE-g2/3 | −.29*** | −.38** | −.46*** | −.37*** | .16*** | −.26*** | −.25*** | −.35*** | .26*** | .08* | .15*** | .39*** | .55*** | — | |
| 15. Conduct probs-CH | .13** | .24*** | .19*** | .12** | .20*** | .17*** | .21*** | .23*** | −.17*** | −.00 | −.02 | −.10* | −.18*** | −.19*** | — |
| Mean | 1.13 | 1.17 | 0.37 | 0.29 | 1.92 | 5.78 | 0.86 | 1.77 | 13.59 | 2.71 | 0.69 | −0.22 | −0.31 | −0.26 | 0.24 |
| SD | 0.64 | 0.94 | 1.18 | 1.08 | 2.30 | 2.73 | 1.08 | 1.39 | 4.05 | 1.04 | 0.17 | 0.88 | 1.02 | 0.94 | 0.43 |
Note. CH = child self-report ratings; PA = parent ratings; PE = peer ratings; TE = teacher ratings; measures 1–13 are at Grade 1; measure 14 is the average of Grades 2 and 3; measure 15 is at Grade 4.
p < .05.
p < .01.
p < .001.
Sociometric peer surveys were collected in the spring of the first-, second-, and third-grade years. Students were interviewed individually at school in the spring of the first-, second-, and third-grade years. Each child received a list of students in their classroom and was asked to name children that they “liked most (LM)” and “liked least (LL).” They were also asked to nominate the children in their classroom who best fit a set of behavioral descriptors (described in the following sections).
Measures
Social Preference
Peer “like most” and “like least” nominations were used to assess social preference and rejected status in first, second, and third grades. During the sociometric interviews, children were allowed to nominate an unlimited number of peers of both genders in order to minimize ceiling effects and increase stability of measurement (Terry & Coie, 1991). Nominations were summed for each item, and scores were then standardized within the classroom to control for variability in classroom size. A continuous social preference score was calculated by taking the difference between standardized LM and LL ratings. Procedures established by Coie and Dodge (l983) were used to identify rejected or nonrejected status using a 0.75 SD cutoff (see Coie & Dodge, 1983, for more detailed scoring information).
Aggression
Peers, parents, and teachers provided ratings of aggression in first grade. Peers nominated classmates on aggression using the behavioral item “starts fights, says mean things and hits other kids.” Nominations were standardized within gender to have an equal proportion of aggressive males and females. For categorical peer ratings, students were classified as being either aggressive or nonaggressive using a standard score of 0.75 as the cutoff.
Parents and teachers rated six items that tapped reactive and proactive types of aggression (Dodge & Coie, 1987). Reactive aggression included aggressive retaliatory responses and attributional biases of hostile intent, whereas proactive aggression included instrumental, goal-directed aggressive behaviors. Items were rated on a 5-point scale (range: 0–4), and summed scores were used. This measure demonstrated good internal consistency for teacher ratings (α = .94 and .91, respectively) and for parent ratings (α = .71 and .75, respectively).
ADHD Symptoms
Peers, parents, and teachers provided ratings of ADHD symptoms at the end of the first-grade year. Peers nominated classmates in response to the question, “who gets out of their seat a lot, does strange things, makes a lot of noise, and bothers people who are trying to work?” Teachers and parents completed the ADHD Rating Scale (DuPaul, 1990), providing ratings on 14 items describing the DSM-III-R symptoms of ADHD. Each item was rated using a 4-point scale (range: 0–3). A mean score was used for analyses. Computed alphas revealed strong internal consistency for parent ratings (.91) and for teacher ratings (.96).
Social Competence
Peers, parents, teachers, and children provided ratings of social competence in first grade. Peers nominated classmates who fit the description “some kids are really good to have in your class because they cooperate, help others, and share; they let other kids have a turn.”
Parents completed the 12-item Social Competence Scale (SCS; CPPRG, 1998), which assesses child prosocial behaviors and emotion regulation (e.g., being friendly, understanding others, controlling temper in a disagreement). Items were rated on a 5-point scale, and a summed score was calculated (α = .87). Teachers completed the Social Health Profile (SHP; CPPRG, 1998). On this 9-item scale, teachers rated child prosocial behaviors and emotion regulation using a 6-point scale. A mean score was used (range: 0–5; α = .92).
Children completed the Social Problem-Solving measure (SPS; Dodge, Bates, & Pettit, 1990), which provided a child-based assessment of social competence. On this measure, children were shown eight drawings depicting social challenge situations (social entry; response to provocation) and asked what they could do or say to resolve the situation. For example, after a vignette of a child being pushed out of line, the child was asked what he or she could do to get a place back in line. The interviewer prompted for three responses. The interviewer immediately coded each response into one of seven categories: (a) aggressive (i.e., physical or verbal aggression or threats), (b) competent (i.e., socially appropriate way of handling the situation), (c) authority-punish (i.e., appeals to an authority figure to punish the provocateur), (d) authority-intervene (i.e., appeals to an authority figure to intervene on the child's behalf rather than to punish), (e) passive-inept (i.e., responses indicating a passive or nonassertive response to the situation), (f) irrelevant-other (i.e., nonsense responses or other responses that do not fit into any other category), and (g) unable to provide further responses. For each of the eight scenarios, a score was computed that indicated the proportion of responses that were coded as competent. Independent coder agreement was very high (κ = 0.91, p < .001). The internal consistency for the competence scale was also acceptable (α = .70). In previous studies, the measure has also shown strong internal consistency (α = .88) and temporal stability (4-year α = .79; Dodge, Pettit, Bates, & Valente, 1995).
Conduct Problems
When children were in the third grade, clinical diagnoses of conduct disorder (CD) and oppositional defiant disorder (ODD) were obtained from parent ratings on the Diagnostic Interview Schedule for Children (DISC; Costello, Edelbrock, Dulcan, Dalas, & Klaric, 1994). The DISC has evidenced moderate-to-good validity and reliability to evaluate child psychopathology in other samples (Schwab-Stone et al., 1996; Shaffer et al., 1996). Specifically, test-retest reliability (i.e., kappa values) was moderate for ODD/CD diagnoses (.56–.73). Concurrent validity (based on clinician symptom ratings) was also quite good for CD (kappa values greater than 0.70) and somewhat lower for ODD (κ = .56–.59). In this study, conduct problems were represented by a DISC diagnosis of either ODD or CD.
Children's self-reported conduct problems were obtained from the Things That You Have Done measure (CPPRG, 1998). Most of the items were from the National Youth Survey (NYS; Elliot, Huizinga, & Menard, 1989); additional items were written specifically for the project. The NYS was developed as part of a longitudinal study of conduct problems using a national probability sample of U.S. households of youth ages 11–17. The developers report test-retest reliabilities ranging from .7 to .9 and validation by follow-up interviews with parents and youth, comparisons with official arrest records and self-reported offenses, and examination of the pattern of associations between the self-report scales and predictor measures (Huizinga & Elliot, 1986). Children were asked how many times in the last year they had done a specific act. The Conduct Problems scale (16 items) was used as the outcome variable. The scales were re-coded using a log (x + 1) transformation because of skewness. In this sample, the internal consistency was .58 (alpha).
Attrition
Attrition occurred primarily because of child relocations to new schools that did not participate in the project. Of the initial sample of 657 children with first-grade data, the following data were available at subsequent grades: (a) parent diagnostic ratings of their children in third grade—573 (87%) participants; (b) child self-reports of conduct problems in fourth grade—569 (87%) of the original first-grade sample; and (c) sociometric ratings in second or third grades—576 (88%) of the original first-grade sample.
Attrition analyses compared first-grade functioning (i.e., peer ratings of aggression and social preference and gender) for participants with missing data at each of the three outcome points outlined above (i.e., third-grade parent ratings, fourth-grade child self-report ratings, and second/third peer sociometric ratings). These analyses revealed only a few scattered, but nonsystematic effects. Girls were more likely than boys to be missing DISC ratings, χ2(1) = 4.73, p < .05. Children who were missing self-reported conduct problems in fourth grade were less aggressive in first grade than those with fourth-grade self-reports, t(657) = −2.30, p < .05. In contrast, children with missing sociometric data in Grades 2 and 3 received lower social preference ratings in first grade than did those with sociometric data in Grades 2 and 3, t = −1.99, p < .05. Findings for other variables were not significant.
Results
First-Grade Peer Rejection and Aggression and Conduct Problem Outcomes
Table I shows the correlations across the various measures. First, we tested the hypothesis that peer rejection and aggression in first grade would independently predict parent-reported ODD/CD diagnoses in third grade and child-reported conduct problems in fourth grade.
To examine the prediction of third grade ODD/CD diagnoses (a dichotomous outcome), logistic regressions were computed, assessing the predictive contributions of gender, first-grade peer ratings of social preference and aggression, and their interactions. The peer nominated aggression score was used in this analysis. As shown in Table II, both social preference and aggression were significant independent predictors of the diagnostic outcome, overall model χ2(4) = 20.97, p < .01. Effects were nonsignificant for gender and for the interaction effects. The magnitude of these effects is illustrated by the odds ratios shown in Table II. For example, the odds ratio shows that as social preference scores increased by a standard deviation (i.e., less rejection by peers), the odds of receiving a diagnosis of ODD/CD decreased by .65. The odds ratios also indicate that as aggression scores increased by a standard deviation, the odds of receiving a ODD/CD diagnosis increased by 1.56.
Table II.
First-Grade Social Preference and Aggression and Conduct Problems in Third Grade
| Predictors | Wald χ2 | Odds ratio |
|---|---|---|
| Gender | 0.20 | 1.21 |
| Aggression | 6.04* | 1.56 |
| Social preference | 4.03* | 0.65 |
| Social preference * aggression | 1.60 | 1.19 |
p < .05.
Next, to examine the continuous outcome of fourth-grade child-reported conduct problems, multiple regression analyses were computed, with gender, first-grade social preference, first-grade peer-nominated aggression, and their interactions serving as predictors. As shown in Table III, results were consistent with the CD/ODD diagnostic outcomes. Namely, both social preference and aggression added unique variance to the prediction of self-reported conduct problems, overall model F(4, 568) = 8.20, p < .001, R2 = .06. Effects were nonsignificant for gender and for the interaction of social preference by aggression.6
Table III.
Grade 1 Social Preference and Rejection and ODD/CD in Grade 4
| β | t value | |
|---|---|---|
| Gender | 0.07 | 1.53 |
| Aggression | 0.14 | 2.35* |
| Social preference | −0.11 | −2.36* |
| Aggression * social preference | 0.05 | 0.34 |
p < .05.
Peer Rejection and Aggression in First Grade and Concurrent Functioning
Next, we explored the behavioral correlates of peer rejection in first grade as a way of understanding why both aggression and peer rejection contribute to the development of conduct problems. The general linear model (GLM; Cohen & Cohen, 1983) was used to determine whether differences on teacher- and parent-reports aggression and ADHD and teacher-, parent-, and child-reports of social competence emerged as a function of peer ratings of rejection, aggression (both defined categorically using a 0.75 cutoff), and gender. We also looked at the two- and three-way interactions of these variables (none of the three-way interactions were significant; hence, they are not reported). Table IV shows the pattern of group differences for concurrent functioning at first grade.
Table IV.
Peer Rejection and Aggression at Grade 1 and Concurrent Patterns of Group Differences
| AGGRESSION BY REJECTIONa | AGG vs NON-AGGa | REJ vs NON-REJa | UNIVARIATE F | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| NEITHER (n = 373) |
REJ ONLY (n = 88) |
AGG ONLY (n = 80) |
BOTH (n = 116) |
NON-AGG (n = 461) |
AGG (n = 196) |
NON-REJ (n = 453) |
REJ (n = 204) |
AGGR | REJ | AGGR* REJ | |
| ADHD | |||||||||||
| Parent | 0.98 | 1.24 | 1.24 | 1.38 | 1.03 | 1.32 | 1.03 | 1.32 | 8.71** | 10.33** | 0.95 |
| Teacher | 0.78 | 1.33 | 1.48 | 1.94 | 0.88 | 1.76 | 0.90 | 1.69 | 45.76*** | 37.90*** | 0.29 |
| Peer | −0.21 | 0.40 | 0.91 | 1.88 | −0.10 | 1.50 | −0.01 | 1.28 | 161.97*** | 83.74*** | 4.50 |
| AGGR | |||||||||||
| Proactive-Parent | 1.46 | 2.15 | 2.51 | 2.61 | 1.58 | 2.57 | 1.63 | 2.42 | 9.71** | 3.33+ | 1.84 |
| Proactive-Teacher | 0.51 | 0.81 | 1.50 | 1.58 | 0.56 | 1.55 | 0.67 | 1.26 | 61.63*** | 3.54+ | 1.12 |
| Reactive-Parent | 5.18 | 6.25 | 5.93 | 7.14 | 5.38 | 6.67 | 5.31 | 6.78 | 7.41** | 19.72*** | 0.09 |
| Reactive-Teacher | 1.16 | 1.96 | 2.56 | 2.85 | 1.31 | 2.74 | 1.39 | 2.48 | 62.86*** | 20.55*** | 4.58+ |
| Social comp | |||||||||||
| Parent | 14.72 | 12.30 | 12.78 | 11.68 | 14.29 | 12.11 | 14.39 | 11.93 | 6.91** | 20.98*** | 2.92+ |
| Teacher | 2.84 | 2.52 | 2.56 | 2.48 | 2.78 | 2.51 | 2.79 | 2.50 | 1.24 | 3.87* | 1.31 |
| Child | 0.72 | 0.65 | 0.68 | 0.65 | 0.70 | 0.66 | 0.71 | 0.65 | 0.03 | 7.46** | 1.35 |
| Peer | 0.05 | −0.60 | −0.29 | −0.72 | −0.07 | −0.55 | −0.01 | −0.67 | 1.98 | 43.09*** | 1.49 |
Tabled values represent means.
p < .10.
p < .05.
p < .01.
p < .001.
ADHD
Using the Wilks's lambda criterion, a significant multivariate main effect was obtained for aggression, F(3, 599) = 56.56, p < .001; rejection, F(3, 599) = 31.87, p < .001; and gender, F(4, 599) = 7.30, p < .001. Boys were described as exhibiting higher levels of aggression than did girls. The multivariate effect for the interaction of rejection and aggression was marginal, F(3, 599) = 2.3, p < .10; the univariate analyses showed the interaction to be significant for peer ratings of ADHD. All of the pairwise contrasts were significant. Children who were both rejected and aggressive scored highest on ADHD, followed by the aggressive-only group, the rejected-only group, and the nonproblem group.
Proactive and Reactive Aggression7
Multivariate main effects were significant for aggression, F(4, 604) = 18.79, p < .001; rejection, F(4, 604) = 10.11, p < .001; and gender, F(4, 604) = 3.13, p < .05. As expected, boys were reported to have higher levels of aggression. Univariate results for the proactive and reactive types of aggression showed different patterns of association with peer rejection and aggression. Not surprisingly, aggression was significantly associated with both proactive and reactive types of aggression. However, peer rejection showed highly significant associations with reactive aggression, but only a marginally significant relation with proactive aggression. The multivariate interaction of rejection and aggression evidenced a marginal effect, F(4, 604) = 2.24, p < .10.
Social Competence
Significant multivariate main effects were found for aggression, F(4, 603) = 11.62, p < .001; peer rejection, F(4, 603) = 17.68, p < .001; and gender, F(4, 603) = 15.52, p < .001; girls displayed higher levels of social competence. The multivariate interactions of gender with aggression, F(4, 603) = 3.67, p < .01, and rejection, F(4, 603) = 2.50, p < .05, were also significant.
The multivariate effect for aggression was qualified by the significant aggression by gender interaction effect for child social competence scores, and univariate analyses were run separately by gender. Social competence scores were lower for aggressive females than for nonaggressive females (mean scores for females—aggressive: 0.58; nonaggressive: 0.74), but social competence scores did not differ for males as a function of aggression (mean score for males: aggressive = 0.67; nonaggressive = 0.67). In addition, the multivariate effect for rejection was qualified by the significant interaction between gender and rejection for peer ratings of social competence. Analyses were run separately by gender, and rejected males and females both received significantly lower social competence scores. However, the degree of difference between the rejected and nonrejected groups was greater for females than that for males (mean scores for females: rejected = −0.64; nonrejected = 0.20; males: rejected = −0.68; nonrejected = −0.21).
Peer Rejection as a Mediator of the Effects of Aggression and ADHD on Conduct Problems
The final hypothesis was that the experience of rejection, subsequent to the assessment of behavioral factors that contribute to both rejection and later conduct problems, significantly predicts conduct problems with these earlier behavioral variables in the model. In addition, we explored the degree to which subsequent peer rejection (in Grades 2 and 3) might mediate the effects of early reactive, hyperactive, and low prosocial behaviors (in Grade 1) on the emergence of conduct problem behavior (in Grade 4).
Applying the strategy modeled after Baron and Kenny (1986), we examined these questions using structural equation modeling (SEM) analyses. First, we considered the direct effects of first-grade ADHD symptoms and aggression on fourth-grade conduct problems, individually and then in combination using structural equation modeling. Then we examined the direct relation between peer social preference assessed in Grades 2 and 3 and conduct problems in Grade 4 to determine if the putative mediator significantly predicted the outcome variable itself. Finally, we examined changes in the strength of paths from the Grade 1 behavioral variables to the Grade 4 outcome when Grade 2/3 social preference was inserted in the model as a potential mediator.8 Standardizing and averaging scores across data from multiple raters created composite scores for Grade 1 social competence, ADHD, and aggression. Social preference ratings were averaged across scores from second and third grades.
SEM with maximum likelihood estimation and Mplus software, Version 1.04 (Muthen & Muthen, 1998) was used to test the hypothesized mediation effects. All models were fully saturated; hence, no overall fit statistics are reported. Preliminary SEMs showed that social competence did not have a direct effect on later conduct problems; hence, it was dropped from subsequent models.
Our first equation tested the direct effects of aggression and ADHD in first grade on conduct problems ratings in fourth grade (see Fig. 1). As expected, aggression (β = 0.20, SE = 0.03, p < .001) and ADHD (β = 0.11, SE = 0.03, p < .001) in first grade significantly predicted later conduct problems. In the next model, we examined whether social preference mediated the effects of aggression and ADHD on conduct problems. As is also shown in Fig. 1 (see effects in parentheses), ADHD was strongly predictive of social preference (β = −0.49; SE = 0.04, p < .001). ADHD no longer predicted later conduct problems when social preference was included in the model (β = 0.06; SE = 0.03, ns). Aggression did not predict social preference (β = −0.04; SE = 0.06, ns). With social preference in the model, aggression continued to strongly predict later conduct problems (β = 0.20; SE = 0.03, p < .001). Furthermore, rejection continued to marginally predict conduct problems (β = −0.09; SE = 0.05, p < .10), even with ADHD and aggression in the model. We tested the significance of social preference as a mediator of ADHD and aggression in their effects on conduct problems by looking at the product of the two effects (i.e., the effect of the variable on the mediator and the effect of the mediator on the outcome variable), as outlined by Sobel (1982). Social preference marginally mediated the effect of ADHD on later conduct problems (z = 1.84, p < .07). Social preference did not mediate the effect of aggression on later conduct problems (z = 0.85, ns).
Fig. 1.
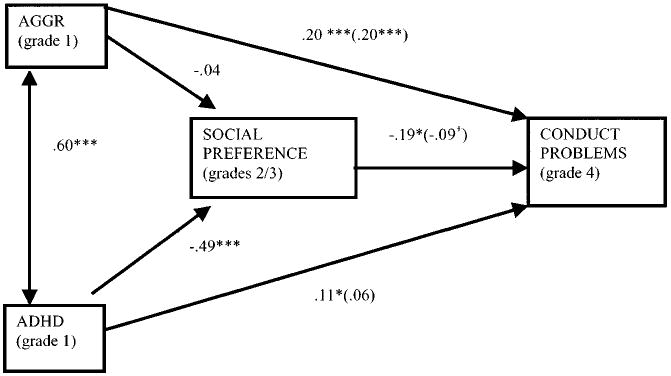
Mediation model: Social preference as potential mediator of effects of ADHD and aggression on conduct problems.
Discussion
The results of this investigation are the first to demonstrate the significance of both peer rejection and aggression in the early school years for the development of early starting conduct problems. The findings from this study support the hypothesis that peer rejection in first grade contributes to subsequent conduct problem behavior, independent of the effects of aggression, as has been found with rejection and aggression at older ages (Coie et al., 1992, 1995; Miller-Johnson et al., 1999; Patterson & Bank, 1989). Thus, these findings provide evidence for the prognostic significance of social rejection in the early school years, along with aggression, in terms of identifying and intervening with children at risk for early starting conduct problems.
The role played by problematic peer relations in foretelling negative outcomes has been discussed in several recent treatments of the development of psychopathology (Coie & Miller-Johnson, in press; Parker et al., 1995; Rudolph & Asher, 2000). Peer relationships provide a critical socialization milieu in which children gain social and behavioral competencies that are crucial for successful development. Conversely, rejected children can be subjected to negative experiences that shape their attitudes toward other people in a way that amplifies antisocial behaviors such as aggression or social withdrawal. They can also be excluded from mainstream social groups and shunted toward deviant peer groups that promote conduct problem behavior. Thus, the peer system can serve as a link between early maladaptive behavior patterns and subsequent psychopathology. Previous research has shown the prognostic significance of peer rejection in middle childhood as a predictor of later conduct problems, over and above the effects of aggression. However, support for the predictive role of very early peer relations for subsequent conduct problems has not previously been demonstrated. This study provides such support in several ways.
First, the study provides evidence that both social rejection by peers and aggression independently contribute to early starting conduct problems. As noted earlier, Parker and Asher (1987) raised the important question of whether peer rejection added incrementally to the prediction of conduct problems, after controlling for the effects for aggression. Our study builds on work in the last decade indicating unique effects for both rejection and aggression in predicting conduct problems (Bierman et al., 1993, 1995; Coie et al., 1992, 1995; Miller-Johnson et al., 1999) and extends these results to a younger sample. These findings add to previous research documenting the negative developmental impact of poor peer relations at school entry. For example, Ladd and colleagues (Ladd, Birch, & Buhs, 1999; Ladd, Kochenderfer, & Coleman, 1997) found that peer rejection in kindergarten led to negative attitudes toward school and self, and in addition, impaired future academic performance by decreasing child interest and participation in academic activities (effects apparent after controlling for cognitive maturity at school entry). Thus, the experience of being rejected by early school peers seems to add to a child's risk for behavioral and academic adjustment problems in the school context beyond the impact of child characteristics and capacities.
Second, this study revealed that the combination of peer rejection and aggression in first grade was associated with the same pattern of social and behavioral deficits as that found among older rejected, aggressive children. For example, it was the more dysregulated form of reactive aggression, rather the more controlled form of proactive–instrumental aggression that elicited rejection. Similarly, behavioral dysregulation, in the form of inattention and impulsiveness, characterized aggressive rejected children and distinguished them from aggressive nonrejected children. Finally, being rejected by peers in first grade was also related to lower ratings of social competence.
These findings on the social and behavioral correlates of rejected, aggressive children provide clues as to how the experience of peer rejection might contribute to their early starting conduct problems. Because these children are more impulsive and have problems sustaining attention, they are more likely to disrupt other children's activities in the classroom and during organized play. As a result, other children are likely to become irritated and upset with them, as well as to reject them socially. Because these rejected, aggressive children are more prone to anger themselves, as well as having fewer social skills for mediating peer distress, they may be more likely to get into escalating clashes with others, thus setting a pattern of greater interpersonal violence with peers. Add to this the feelings of resentment and suspicion that may arise in them as a result of being rejected and excluded by peers (Dodge, 1993), and it is easy to see how rejected, aggressive children become significantly more aggressive over time than their nonrejected counterparts.
There is a second explanation for the impact of early childhood peer rejection on conduct problem behavior, in addition to effects of rejection on the child's increased hostility and suspicion toward peers. Patterson, DeBaryshe, and Ramsey (1989) have theorized that rejection in later childhood can lead to associations with deviant peers in early adolescence because of the limited social choices available to rejected children, and they cite data from the Oregon Social Learning Center longitudinal study to support this hypothesis. Furthermore, Bagwell, Coie, Terry, and Lochman (2000) provide more recent evidence that rejection in middle childhood (age 10) is linked to concurrent membership in deviant peer groups. They found that nonrejected, aggressive boys were equally represented in these same fourth-grade deviant peer groups and appeared to be the leaders of these groups. Data on the centrality of membership also indicated that while the nonrejected aggressive children were the more central members of deviant peer groups, the rejected, aggressive children were more peripheral members of these groups. The fact that they are only peripheral group members may, in fact, make the rejected, aggressive children more susceptible to deviant peer influence than more central members because they feel they need to prove they belong. Thus, the deviant peer context of rejected, aggressive children may also promote or amplify conduct problem behaviors.
A third contribution of this study involves an examination of the developmental pathways linking early aggression and ADHD symptoms, social rejection, and the emergence of significant conduct problems in middle childhood. On the one hand, the findings suggest that a strong, direct connection between early aggressive behavior and later conduct problems is not affected by the presence of either concurrent ADHD symptoms or subsequent peer rejection, despite the strength of the relations between aggression and each of these other constructs. The relation between ADHD symptoms, peer rejection, and conduct problems appears to be more complex, however. Unlike aggression, neither of these constructs represents a form of conduct problem behavior, per se. ADHD symptoms may be irritating and disruptive to other people, but they do not necessarily entail conduct problems. Thus, the connection between ADHD symptoms and peer rejection and subsequent conduct problems requires some transitional explanation, to understand how either of them amplifies risk for serious conduct problems. The research literature on ADHD and CD clearly documents a high degree of co-morbidity, although it appears to be the impulsive and hyperactive components of ADHD that are mostly closely associated with CD rather than inattentiveness, by itself (Campbell, 2000). ADHD symptoms are strongly predictive of peer rejection, rather than the converse (Erhardt & Hinshaw, 1994; Pelham & Bender, 1982; Whalen & Henker, 1992), and so this causal relation seems well-established. By placing social preference in the model displayed in Fig. 1, the significance of the relation between conduct problems and ADHD symptoms shifted from significance to nonsignificance, and the relation between conduct problems and social preference shifted from significance to marginal significance. This fact makes it difficult to assert that social preference mediates all of the relation between ADHD symptoms and conduct problems, but it does suggest that that some partial mediation is taking place. Clearly, there are overlapping effects of these two variables on future conduct problems, even with aggression in the model, with some of this overlap taking the form of mediation by social preference.
These results suggest two important things about the role of peer rejection. First, although rejection in and of itself may be influenced by disruptive behaviors, such as aggression and ADHD, the experience of being socially rejected by peers has its own independent influence on antisocial behavior. Second, ADHD and aggression appeared to function differently in terms of how these variables were directly and indirectly associated with subsequent conduct problems. Specifically, with social preference in the model, aggression continued to directly predict conduct problems, and social preference did not mediate the association between aggression and later conduct problems. However, once social preference was included in the model, ADHD no longer directly predicted later conduct problems. Rather, ADHD appeared to have its influence on subsequent conduct problems through causing children to be rejected by peers. In other words, ADHD appears to have its effect, in part, through its negative social consequences on others.
These findings support a more complex conceptualization of the role of peer relations in forecasting maladaptive outcomes. Recent theorists have extended Sameroff's transactional model (Sameroff, 1975) to peer relations and have proposed that peer relations are part of a complex set of interactions between children and others in their environment (Coie, in press; Parker, Rubin, Price, & DeRoiser, 1995; Rudolph & Asher, 2000). Namely, there is a dynamic and reciprocal relation between a child's behavior and reactions to this behavior by others in that child's social world. In terms of peer rejection, certain behaviors (such as being impulsive and reactively aggressive) may lead to a child to become highly disliked by others. Other children may come to treat this child more negatively. The rejected child may become picked on by others or left out of activities and develop a reputation for not getting along with others. Rejected children may thus come to feel poorly about themselves and start to see themselves as “trouble makers.” They may seek out others like themselves and develop deviant peer affiliations that further amplify their tendencies toward antisocial behavior. Thus, the experience of being rejected by peers carries with it a set of experiences and consequences that contribute to subsequent conduct problems.
Our findings have two important implications for preventive interventions to reduce the risk for later conduct problems. First, in identifying children who are at high risk for later conduct problems, children's aggressive behavior is most commonly used and is readily identified. Results of this study suggest that peer rejection is another risk factor that might add profitably to the model to increase the sensitivity of identifying those at risk for later conduct problems. Second, an important component of preventive interventions would be to enhance prosocial skills and develop anger management abilities (Bierman, Greenberg, & Conduct Problems Prevention Research Group, 1997). Conversely, our results suggest that early treatment for ADHD symptoms might head off the negative consequences of peer rejection in children who also exhibit excessive aggressiveness.
There are several limitations to this study that should be acknowledged. The attrition analyses indicated that sociometric data at Grade 2 or 3 was disproportionately missing for children who had lower social preference scores in first grade. Because there is good evidence for the stability of social preference scores, this may have reduced the number of rejected children in the mediation analyses and served to attenuate the significance of social preference, either as a mediator of ADHD symptoms or as a predictor of fourth-grade conduct problems. Second, although this was a very large sample of children for this type of research question, the number of girls that fit the criteria for aggression, rejection, and ADHD symptoms may have been too small to yield significant interaction effects for gender in these analyses. Thus, even though we have discussed the results as holding true for children, in general, they may have greater application for boys.
In conclusion, the results of this study provide more support for considering the socialization effects of peers on the development of serious conduct problems. In particular, the findings provide some clarification of the connections between early ADHD symptoms and peer rejection, suggesting a causal link between the former and the latter, with the latter serving as a partial mediator of the relation between ADHD and conduct problems, at least in the early school years.
Footnotes
At one of the sites, a school dropped out in the 1st year of the study, and the normative sample was reduced to 87 children.
Results from analyzing continuous predictors were consistent with analyses using categorical predictors; namely, peer rejection and aggression defined categorically significantly predicted conduct problems and CD/ODD.
Interactions with gender were nonsignificant; therefore, these interactions were removed from the model and only main effects for gender were included.
We ran identical models, using second- or third-grade ratings of social preference. Results were consistent with those using the average of second- and third-grade ratings of social preference.
References
- Bagwell CL, Coie JD, Terry RA, Lochman JE. Peer clique participation and social status in preadolescence. Merrill-Palmer Quarterly. 2000;45:280–305. [Google Scholar]
- Baron RM, Kenny DA. The moderator–mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology. 1986;51:1173–1182. doi: 10.1037//0022-3514.51.6.1173. [DOI] [PubMed] [Google Scholar]
- Bierman KL, Smoot DL, Aumiller K. Characteristics of aggressive–rejected, aggressive (nonrejected), and rejected (nonaggressive) boys. Child Development. 1993;64:139–151. [PubMed] [Google Scholar]
- Bierman KL, Greenberg MT, Conduct Problems Prevention Research Group . Social skills training in the Fast Track program. In: Peters RD, McMahon RJ, editors. Preventing childhood disorders, substance abuse, and delinquency. Thousand Oaks, CA: Sage; 1997. pp. 65–89. [Google Scholar]
- Bierman KL, Wargo JB. Predicting the longitudinal course associated with aggressive–rejected, aggressive (nonrejected), and rejected (nonaggressive) status. Development and Psychopathology. 1995;7:669–682. [Google Scholar]
- Campbell SB. Attention-deficit/hyperactivity disorder: A developmental view. In: Sameroff AJ, Lewis M, Miller SM, editors. Handbook of developmental psychopathology. 2nd. New York: Kluwer; 2000. [Google Scholar]
- Cohen J, Cohen P. Applied multiple regression/correlation for the behavioral sciences. 2nd. Hillsdale, NJ: Erlbaum; 1983. [Google Scholar]
- Coie JD, Dodge KA. Continuities and changes in children's social status: A five-year longitudinal study. Merrill-Palmer Quarterly. 1983;29:261–282. [Google Scholar]
- Coie JD, Dodge KA, Terry R, Wright V. The role of aggression in peer relations: An analysis of aggression episodes in boys' play groups. Child Development. 1991;62:812–826. doi: 10.1111/j.1467-8624.1991.tb01571.x. [DOI] [PubMed] [Google Scholar]
- Coie JD, Lochman JE, Terry R, Hyman C. Predicting early adolescent disorder from childhood aggression and peer rejection. Journal of Consulting and Clinical Psychology. 1992;60:783–792. doi: 10.1037//0022-006x.60.5.783. [DOI] [PubMed] [Google Scholar]
- Coie JD. The impact of negative social experience on the development of antisocial behavior. In: Kupersmidt JB, Dodge KA, editors. Children's peer relations: From development to intervention to policy: A festschrift in honor of John D Coie. Washington, DC: American Psychological Association; in press. [Google Scholar]
- Coie J, Terry R, Lenox K, Lochman J, Hyman C. Childhood peer rejection and aggression as predictors of stable patterns of adolescent disorder. Development and Psychopathology. 1995;7:697–713. [Google Scholar]
- Conduct Problems Prevention Research Group. A developmental and clinical model for the prevention of conduct disorder: The FAST Track Program. Development and Psychopathology. 1992;4:509–527. [Google Scholar]
- Conduct Problems Prevention Research Group. Technical reports for the Fast Track assessment battery. 1998 Unpublished technical reports. [Google Scholar]
- Costello AJ, Edelbrock LS, Dulcan MK, Dalas R, Klaric SH. Report on the NIMH Diagnostic Interview for Children. Washington, DC: National Institute of Mental Health; 1994. [Google Scholar]
- Dodge KA. Social–cognitive mechanisms in the development of conduct disorder and depression. Annual Review of Psychology. 1993;44:559–584. doi: 10.1146/annurev.ps.44.020193.003015. [DOI] [PubMed] [Google Scholar]
- Dodge KA, Bates JE, Pettit GS. Mechanisms in the cycle of violence. Science. 1990;250:1678–1683. doi: 10.1126/science.2270481. [DOI] [PubMed] [Google Scholar]
- Dodge KA, Coie JD. Social-information-processing factors in reactive and proactive aggression in children's peer groups. Journal of Personality and Social Psychology. 1987;53:1146–1158. doi: 10.1037//0022-3514.53.6.1146. [DOI] [PubMed] [Google Scholar]
- Dodge KA, Pettit GS, Bates JE, Valente E. Social information-processing patterns partially mediate the effect of early physical abuse on later conduct problems. Journal of Abnormal Psychology. 1995;104:632–643. doi: 10.1037//0021-843x.104.4.632. [DOI] [PubMed] [Google Scholar]
- DuPaul GJ. The ADHD rating scale: Normative data, reliability and validity. The University of Massachusetts Medical Center; Worchester, MA: 1990. Unpublished manuscript. [Google Scholar]
- Elliot DS, Huizinga D, Ageton SS. Explaining delinquency and drug use. Newbury Park, CA: Sage; 1985. [Google Scholar]
- Elliot DS, Huizinga D, Menard S. Multiple problem youth: Delinquency, substance use, and mental health problems. New York: Springer; 1989. [Google Scholar]
- Erhardt D, Hinshaw SP. Initial sociometric impressions of attention-deficit hyperactivity disorder and comparison boys: Predictions from social behavior and from nonbehavioral variables. Journal of Consulting and Clinical Psychology. 1994;62:833–842. doi: 10.1037/0022-006X.62.4.833. [DOI] [PubMed] [Google Scholar]
- Hinshaw SP. Conduct disorder in childhood: Conceptualization, diagnosis, comorbidity, and risk status for antisocial functioning in adulthood. In: Fowles D, Sutter P, Goodman S, editors. Progress in experimental personality and psychopathology research Special focus on psychopathy and antisocial personality: A developmental perspective. New York: Springer; 1994. pp. 3–44. [PubMed] [Google Scholar]
- Hinshaw SP, Melnick S. Peer relationships in boys with attention-deficit hyperactivity disorder with and without comorbid aggression. Development and Psychopathology. 1995;7:627–647. [Google Scholar]
- Huizinga D, Elliott DS. Reassessing the reliability and validity of self-report delinquency measures. Journal of Quantitative Criminology. 1986;2:293–327. [Google Scholar]
- Hymel S, Franke S. Children's peer relations: Assessing self-perceptions. In: Schneider BH, Rubin KH, Ledingham JE, editors. Children's peer relations: Issues in assessment and intervention. New York: Springer; 1985. pp. 75–91. [Google Scholar]
- Ladd GW, Birch S, Buhs E. Children's social and scholastic lives in kindergarten: Related spheres of influence? Child Development. 1999;70:1373–1400. doi: 10.1111/1467-8624.00101. [DOI] [PubMed] [Google Scholar]
- Ladd GW, Kochenderfer BJ, Coleman CC. Classroom peer acceptance, friendship, and victimization: Distinct relational systems that contribute uniquely to children's school adjustment? Child Development. 1997;68:1181–1197. doi: 10.1111/j.1467-8624.1997.tb01993.x. [DOI] [PubMed] [Google Scholar]
- Milich R, Dodge KA. Social information processing in child psychiatric populations. Journal of Abnormal Child Psychology. 1984;12:471–490. doi: 10.1007/BF00910660. [DOI] [PubMed] [Google Scholar]
- Miller-Johnson S, Coie JD, Maumary-Gremaud A, Lochman J, Terry R. Peer rejection and aggression in childhood and severity and type of delinquency during adolescence among African American youth. Journal of Emotional and Behavioral Disorders. 1999;7:137–146. [Google Scholar]
- Muthen LK, Muthen BO. Mplus The comprehensive modeling program for applied researchers. User's guide. Los Angeles: Muthen & Muthen; 1998. [Google Scholar]
- Parker JG, Asher SR. Peer relations and later personal adjustment: Are low-accepted children at risk? Psychological Bulletin. 1987;102:357–389. doi: 10.1037//0033-2909.102.3.357. [DOI] [PubMed] [Google Scholar]
- Parker JG, Rubin KH, Price JM, DeRosier ME. Peer relationships, child development, and adjustment: A developmental psychopathology perspective. In: Cicchetti D, Cohen DJ, editors. Developmental psychopathology. Vol 2: Risk, disorder, and adaptation. New York: Wiley; 1995. pp. 96–161. [Google Scholar]
- Patterson GR, Bank CL. Some amplifying mechanisms for pathologic processes in families. In: Gunnar M, Thelen E, editors. Systems and development: Symposia on child psychology. Hillsdale, NJ: Erlbaum; 1989. pp. 167–210. [Google Scholar]
- Patterson G, Debaryshe B, Ramsey E. A developmental perspective on antisocial behavior. American Psychologist. 1989;44:329–335. doi: 10.1037//0003-066x.44.2.329. [DOI] [PubMed] [Google Scholar]
- Pelham W, Bender ME. Peer relations in hyperactive children: Description and treatment. In: Gadow K, Bialer I, editors. Advances in learning and behavioral disabilities. Vol. 1. Greenwich, CT: JAI Press; 1982. pp. 365–436. [Google Scholar]
- Pope AW, Bierman KL. Predicting adolescent peer problems and antisocial activities: The relative roles of aggression and dysregulation. Developmental Psychology. 1999;35:335–346. doi: 10.1037//0012-1649.35.2.335. [DOI] [PubMed] [Google Scholar]
- Rabiner D, Coie JD. The effect of expectancy inductions on rejected children's acceptance by unfamiliar peers. Developmental Psychology. 1989;25:450–457. [Google Scholar]
- Rudolph KD, Asher SR. Adaptation and maldadaptation in the peer system Developmental processes and outcomes. In: Sameroff AJ, Lewis M, Miller SZ, editors. Handbook of developmental psychopathology. New York: Kluwer; 2000. pp. 157–175. [Google Scholar]
- Sameroff AJ. Transactional models in early social relations. Human Development. 1975;18:65–79. [Google Scholar]
- Schwab-Stone ME, Shaffer D, Dulcan MK, Jensen PS, Fisher P, Bird HR, et al. Criterion validity of the NIMH diagnostic Interview Schedule for Children version 2.3 (DISC-2.3) Journal of the American Academy of Child and Adolescent Psychiatry. 1996;35:878–899. doi: 10.1097/00004583-199607000-00013. [DOI] [PubMed] [Google Scholar]
- Shaffer D, Fisher P, Dulcan MK, Davies M, Piacentini J, Schwab-Stone ME, et al. The NIMH Diagnostic Interview Schedule for Children version 2.3 (DISC 2.3): Description, acceptability, prevalence rates, and performance in the MECA study. Journal of the American Academy of Child and Adolescent Psychiatry. 1996;35:865–877. doi: 10.1097/00004583-199607000-00012. [DOI] [PubMed] [Google Scholar]
- Sobel ME. Asymptotic confidence intervals for indirect effects in structural equation models. In: Leinhart S, editor. Sociological methodology. San Francisco: Jossey-Bass; 1982. pp. 290–312. [Google Scholar]
- Soussignan R, Tremblay RE, Schaal B, Laurent D, Larivee S, Gagnon C, et al. Behavioural and cognitive characteristics of conduct disordered-hyperactive boys from age 6 to 11: A multiple informant perspective. Journal of Child Psychology and Psychiatry. 1992;33:1333–1346. doi: 10.1111/j.1469-7610.1992.tb00953.x. [DOI] [PubMed] [Google Scholar]
- Spetter DS, LaGreca AM, Hogan A, Vaughn S. Subgroups of rejected boys: Aggressive responses to peer conflict situations. Journal of Clinical Child Psychology. 1992;21:20–26. [Google Scholar]
- Terry R, Coie JD. A comparison of methods for defining sociometric status among children. Developmental Psychology. 1991;27:867–880. [Google Scholar]
- Werthamer-Larsson L, Kellam S, Wheeler L. Effect of first-grade classroom on shy behavior, aggressive behavior, and concentration problems. American Journal of Community Psychology. 1991;19:585–602. doi: 10.1007/BF00937993. [DOI] [PubMed] [Google Scholar]
- Whalen CK, Henker B. The social profile of attention-deficit hyperactivity disorder: Five fundamental facts. In: Weiss G, editor. Child and adolescent psychiatric clinics of North America: Attention-deficit hyperactivity disorder. Philadelphia: Lippincott; 1992. pp. 395–410. [Google Scholar]