

Abstract
Renal cell carcinoma is an uncommon type of cancer that rarely metastasizes to the brain. The prognosis after discovering brain metastasis has traditionally been dismal. We are presenting a case of renal cell carcinoma with multiple brain metastases that was successfully treated with multimodal therapy including a new type of medication.
Keywords: renal cell carcinoma, brain metastasis, sorafenib
Abstract
Das Nierenzellkarzinom ist eine Karzinomart, die selten in das Gehirn metastasiert. Die Prognose nach der Entdeckung der Hirnmetastasen ist gewöhnlich infaust. Wir stellen den Fall eines Nierenzellkarzinoms mit multiplen Hirnmetastasen vor, das mit einer multimodalen Therapie einschließlich eines neuen Wirkstoffes erfolgreich behandelt worden ist.
Successful treatment of a brain-metastasized renal cell carcinoma
In the United States, renal cell carcinoma (RCC) accounts for 2.6% of all cancers, more among men [1]. It rarely metastasizes to the brain with a median survival after the diagnosis of brain metastases of 10.7 months and the 1-year, 2-year, and 5-year survival rates are 48%, 30%, and 12%, respectively [2]. We are presenting a case of RCC with multiple brain metastases that responded to neurosurgical, radiation and new drug treatment.
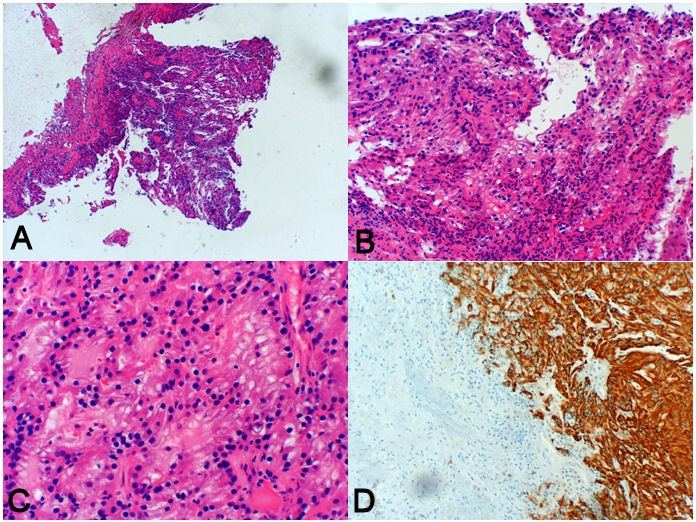
This patient was a 47 year old male who had a two-months history of numbness on his right side. MRI of the brain with and without contrast revealed multiple small enhancing lesions consistent with probable metastatic disease. The largest lesion was in the left parietal area (Figure 1 (Fig. 1)). Chest, abdomen and pelvis CT showed a 2.5×1.8 cm lesion in his left kidney (Figure 2 (Fig. 2)). The patient had no significant medical history other than an operation for a perforated ulcer 15 years ago. The patient admitted to smoking a pack and a half of cigarettes a day and drinking alcohol daily. There were no significant findings on physical exam. It was decided that the definitive treatment would depend on pathology and therefore surgery was undertaken. Pathology showed tubular structure (Figure 3A, Figure 3B, Figure 3C(Fig. 3)) with immunoreactivity to cytokeratin AE1/AE3 (Figure 3D (Fig. 3)) but negative for cytokeratin 7 and 20. The histologic features and immunoprofile was compatible with renal cell carcinoma. The patient then had 14 radiation seances to the brain; after that he was put on the new drug, sorafenib (approved by the U.S. Food and Drug Administration in December 2005). The tumor kidney was removed 11 months after metastasis resection. On his followup visit three years later the patient was neurologically intact. He was on phenytoin and sorafenib. The last MRI, 4 years after the initial surgery, looks stable without residual or recurrent tumor.
Figure 1. CT brain showing metastasis in the left parietal area.
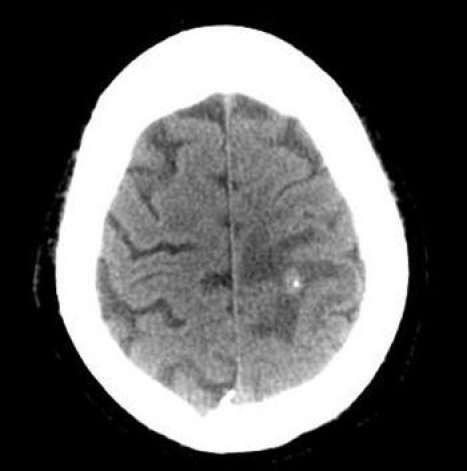
Figure 2. CT abdomen showing a tumor in the left kidney.

Figure 3. Pathologic view of brain metastasis A: ×4 magnification B: ×10 magnification C: Tubular structure (×20) D: Cytokeratin AE1/AE3 positivity (×10).
This is an illustrative case of a stage IV RCC tumor that was successfully treated with a multimodal combinatory approach. Nephrectomy, total or partial, is the first treatment for renal cancer. Metastectomy is usually reserved for single or limited lesions. In our case, the brain lesions were multiple. The largest one was not in the motor cortical region so it was deemed resectable. Whole brain therapy was used to clear microscopic tumor seedings. A new family of medications called tyrosine protein kinases inhibitors, namely sunitinib and sorafenib, has been shown to prolong survival in RCC patients by interfering with angiogenesis. The patient was put on sorafenib. There are few reports of renal cell brain metastases successfully treated with these agents [3], [4]. Sunitinib is now regarded as the first-line therapy for renal cell carcinoma while sorafenib is used in a second-line setting. Sorafenib has been shown to prevent the growth of tumors but, unlike sunitinib, not to reduce tumor size [5]. Further research is needed to establish the role of sunitinib and sorafenib in the treatment of brain metastases from renal cancer.
Notes
Conflicts of interest
None declared.
References
- 1.Cohen HT, McGovern FJ. Renal-cell carcinoma. N Engl J Med. 2005;353(23):2477–2490. doi: 10.1056/NEJMra043172. Available from: http://dx.doi.org/10.1056/NEJMra043172. [DOI] [PubMed] [Google Scholar]
- 2.Shuch B, La Rochelle JC, Klatte T, Riggs SB, Liu W, Kabbinavar FF, Pantuck AJ, Belldegrun AS. Brain metastasis from renal cell carcinoma: presentation, recurrence, and survival. Cancer. 2008;113(7):1641–1648. doi: 10.1002/cncr.23769. Available from: http://dx.doi.org/10.1002/cncr.23769. [DOI] [PubMed] [Google Scholar]
- 3.Valcamonico F, Ferrari V, Amoroso V, Rangoni G, Simoncini E, Marpicati P, Vassalli L, Grisanti S, Marini G. Long-lasting successful cerebral response with sorafenib in advanced renal cell carcinoma. J Neurooncol. 2009;91(1):47–50. doi: 10.1007/s11060-008-9676-4. Available from: http://dx.doi.org/10.1007/s11060-008-9676-4. [DOI] [PubMed] [Google Scholar]
- 4.Koutras AK, Krikelis D, Alexandrou N, Starakis I, Kalofonos HP. Brain metastasis in renal cell cancer responding to sunitinib. Anticancer Res. 2007;27(6C):4255–4257. [PubMed] [Google Scholar]
- 5.Hiles JJ, Kolesar JM. Role of sunitinib and sorafenib in the treatment of metastatic renal cell carcinoma. Am J Health Syst Pharm. 2008;65(2):123–131. doi: 10.2146/ajhp060661. Available from: http://dx.doi.org/10.2146/ajhp060661. [DOI] [PubMed] [Google Scholar]